
Abstract
Background
Physical morbidity is rife among patients with serious mental illness. When they are involuntarily hospitalized and even treated, they may still refuse treatment for physical illness leading clinicians to wonder about the ethics of coercing such treatments.
Research aim
This survey study explored psychiatric caregivers’ perceptions on whether compulsory treatment of physical illness is legal and whether it is justifiable in patients with serious mental illness and under what circumstances.
Research design
A questionnaire that included two case vignettes of an involuntarily hospitalized psychiatric patient with diabetes refusing treatment with insulin for various reasons. The cases differed in terms of diabetes severity. Participants answered questions regarding the appropriateness of involuntary treatment.
Participants and research context
Psychiatric medical doctors and nurses working in a mental health center. (N = 89, 50 female, ages 26–66).
Ethical considerations
The study was approved by the Medical Centre Institutional Review Board (IRB) and the University Ethics Committee. The respondents’ anonymity was kept. Participation was voluntary and consent was obtained.
Results
The severity of the patient’s medical condition and their reason for refusing treatment were associated with participants’ willingness to give insulin despite patient objection [(F(1, 87) = 49.41, p < .01; (F(1, 87) = 33.44, p < .01), respectively]. Participants were more inclined to support compulsory treatment if the patient’s refusal was “illness-oriented” (i.e. directly related to psychiatric illness). Participants presented diverse views regarding the perceived legality of compulsory treatment of physical illness in such situations (illegal 63.09%; legal 23.8%; 13% unsure). The majority (53.5%–55.3%) of those who thought it was illegal supported compulsory treatment in high-severity, illness-oriented refusal situations.
Conclusions
The severity of the medical condition and the reason for treatment refusal influence psychiatric caregivers’ willingness to provide compulsory treatment for physical illness in involuntary hospitalized psychiatric patients. Beyond the legal framework, ethical guidelines for these situations are warranted, while decisions should be made on a case-by-case basis.
Keywords
Introduction
Individuals who endanger themselves or others due to their mental state may be involuntarily hospitalized. 1 In many situations, this ensues patients lose their right to elective psychiatric treatment.2–4 While comorbidity with chronic physical illnesses is high in the psychiatric community,5–7 whether these individuals have the right to refuse concomitant treatment for physical ailments is unclear. Certainly, the distinction between a psychotic patient refusing treatment based on symptomatic delusions, or based on rational belief, may alter whether it can be administered ethically. Such a decision may be founded on the severity of the medical condition in question. Despite this, we did not find any previous studies exploring the attitudes of frontline healthcare professionals regarding this topic. In the context of Israeli law, involuntarily hospitalized psychiatric patients have the right to appeal medical treatment decisions. However, whether this clause applies to physical, as well as psychiatric treatments may rely on circumstance, as well as personal judgment. Our study seeks to clarify the ethical decision-making of medical doctors and nurses in Israel regarding compulsory treatment of physical illnesses in the involuntarily hospitalized psychiatric population.
Background
Psychiatric patients who endanger themselves or others due to serious mental illness may be involuntarily hospitalized. 1 In some countries, involuntary psychiatric hospitalization is legally limited to patients in psychotic states. In others, even non-psychotic severely depressed or suicidal patients may be involuntarily hospitalized. 8 Once hospitalized, in some jurisdictions, involuntarily hospitalized psychiatric patients (IHPPs) have the right to refuse psychiatric treatment.2,3 In others, compulsory psychiatric treatment for IHPP is not only legal but also expected. 4 Physical morbidity is rife in those with severe mental illness5–7 possibly due to unhealthy lifestyle, 9 the ramifications of psychiatric medication, 10 and inequalities in healthcare provision. 11 IHPP thus often require treatment for chronic physical illnesses. Hospitalizations may last weeks, months, or in extreme cases, years. When IHPP refuse treatment for physical ailments—for example, psychotic patients refusing insulin for diabetes, thereby endangering themselves with uncontrolled hyperglycemia—would it be appropriate to treat not only their psychosis, but also their diabetes involuntarily? The legality and justifiability of involuntary treatment of physical illness in IHPP may be unclear.
According to Israeli law, involuntary psychiatric hospitalization is legal when individuals with mental illness (usually interpreted by courts as acute psychotic states) are suffering due their illness from impaired reality testing or judgment and as a result endanger themselves or others. A depressed suicidal patient who is not acutely psychotic may not formally fulfill these legal criteria for involuntary hospitalization. Once an involuntary hospitalization order has been issued, the psychiatric patient holds the right to appeal the decision but has no legal right to refuse “medical treatment” if hospitalized. 4 Whether the legal term “medical treatment” includes physical conditions, or refers strictly to psychiatric ones, however, remains obscure. In the rare situation that an IHPP is rejecting medical treatment, there are three other laws which may be used to override their refusal. First, the legal competence and guardianship law 12 allows patient refusal to be overridden by court order if the treatment is necessary for preserving the patient’s physical or mental wellbeing. The court considers the treatment’s chances of improving life quality as well as any harmful consequences it might cause. Second, the Patients’ Rights Law 13 allows for urgent care provision if patients are unable to give informed consent in medical emergencies. Certain treatments (such as surgery, catheterization of blood vessels and chemotherapy) require the joint approval of three physicians. Third, hospital ethics committees may approve forcing a treatment that they have a reasonable cause to assume the patient will retroactively consent to in life-threatening conditions or where there is risk of developing severe, irreversible disability. 14
These laws, however, are often not applied in psychiatric hospital settings. In acute or life-threatening emergencies (i.e. suspected stroke), the psychiatric patient will be transferred to a general hospital for treatment. Furthermore, these laws do not seem appropriate for overriding refusal of non-life-threatening physical conditions such as chronic high blood pressure or diabetes.
Considerations regarding involuntary treatment of physical illness in IHPP
Coercion is a serious insult to patients and may be severely traumatizing. 15 Chronic medical conditions, however, which are not acute or immediately life-threatening, can have debilitating consequences if untreated. A diabetic patient, for example, with persistent hyperglycemia, risks future heart attacks, stroke, kidney failure, blindness, and limb amputation. When balanced with the trauma of coercion, is prevention of future disability enough reason to treat involuntarily? Furthermore, should medical staff be held liable for negligence if IHPP have suffered damage due to lack of treatment for physical illness? The low adherence to treatment for chronic medical illness in the general—not psychiatric—population makes this ethical dilemma even more complex. 16
Three main factors, among others, may influence whether IHPP should be treated for physical illness involuntarily. These include illness severity, reason for treatment refusal, and invasiveness of treatment.
Regarding illness severity, it may be assumed that patients in life-threatening emergency conditions requiring immediate medical help may be enforced to receive treatment. 17 Enforcing treatment in these extreme situations seems equally appropriate regarding IHPP. It is unclear, however, whether treatment for non-life-threatening chronic conditions should be involuntary, and if so, under what conditions.
Patients’ reasoning for refusing treatment may also justify compulsory intervention, as it reflects their ability to make genuinely autonomous decisions. Patients have the capacity to make autonomous decisions when they understand, retain, weigh information and communicate a rational choice18–20 in line with their values. 21 If a psychotic patient, for example, refuses insulin for diabetes due to a delusional belief that it is poisoned, her ability to understand the relevant information and rationally justify her decision is severely flawed. She thus lacks the capacity to refuse insulin. Arguably, her freedom to reject insulin should be hindered in favor of what she would have wanted had she not been psychotic. 22 What if that same patient, however, refuses insulin because injections are painful? This decision seems unwise, but if it is reflective of how she truly wants to live, it may be a genuinely authentic one that deserves respect.
The invasiveness of the intervention seems also to influence whether involuntary treatment is justified. Limb amputation for a gangrenous leg, for example, is more invasive and thus harder to justify than insulin injections for diabetes. Similarly, one-time interventions (e.g. vaccinations with no lasting effects) are less invasive than daily interventions (e.g. insulin shots). Practically, it may also be argued that if a patient is already physically restricted for receiving compulsory anti-psychotic injections, adding additional insulin injection to treat comorbid diabetes would not significantly restrict liberty more than anti-psychotics alone.
Research regarding involuntary treatment of physical illness in IHPP
Although the compulsory treatment for physical illness dilemma is prevalent in psychiatric wards’ everyday practice, ethical and legal guidance for dealing with it are scarce. There are a few studies on healthcare workers’ views on forced treatment of psychiatric illness. Various studies in Sweden23,24 and Ethiopia 25 found that psychiatrists support involuntary treatment for psychotic, dangerous and suicidal patients and those lacking insight more than mood disorder patients. A literature review found that healthcare workers perceive forced medication as ethically problematic but necessary. 26 Our literature review found no studies exploring the attitudes of those on the frontline, such as psychiatrists and nurses, regarding the compulsory treatment for physical illness in IHPP.
Presumably, in situations where there is an absence of clear guidelines, or whereby medical staff are not aware of existing guidelines, personal judgment may be heavily relied on when making treatment decisions. Given the lack of clear guidelines surrounding this subject in Israel, this study aims to explore psychiatric caregivers’ perceptions and moral reasoning on whether compulsory treatment of physical illness is justifiable in IHPP and if so, under what circumstances. Specifically, it focuses on whether the severity of patients’ medical condition or reason for treatment refusal influences attitudes on the topic.
Methods
Tools
A self-administered structured questionnaire was created to explore participants’ attitudes and knowledge regarding involuntary treatment of physical illness in IHPP. The questionnaire consisted of three sections: (a) Demographics (gender, age, religion, religiosity, occupation, seniority); (b) Two case vignettes followed by questions regarding the appropriateness of involuntary treatment. The vignettes described an involuntarily hospitalized psychiatric patient with diabetes who refuses treatment with insulin. The cases differed in terms of diabetes severity. One patient has moderately high blood sugar (HbA1c of 10% and fasting blood glucose 250 mg/dL) and risks future diabetic complications, such as heart attacks and stroke, if left untreated. These values were used as they are above the diagnostic threshold for diabetes according to the American Diabetes Association guidelines but are not severe enough to put the patient at risk of an acute diabetic emergency. 27
The other patient has severely high blood sugar (HbA1c 13.5% and a fasting blood glucose 450 mg/dL) and may enter a potentially life-threatening condition if not treated. It was emphasized that these severe high values approach, but do not reach the diagnostic threshold for a potentially lethal hyperosmolar hyperglycemic state, meaning the patient is in an urgent but not immediately life-threatening condition. 28
Following each vignette, subjects were asked whether they would enforce insulin treatment given five different reasons for refusal by the patient:
(1) A delusional belief that the patient does not have diabetes and the blood test is fake; (2) A delusional belief that the insulin is poisoned; (3) The patient is suicidal and believes high blood sugar will hasten death; (4) The patient finds injections unpleasant; (5) The patient prefers to control diabetes through strict diet.
The two vignettes and questions that followed were presented randomly to neutralize presenting bias. Participants rated their decision on a five-point Likert scale from 1 (totally disagree with compulsory insulin) to 5 (completely agree with compulsory insulin), with 3 being neutral. After participants answered all questions related to the first vignette they proceeded to the second one and were not allowed to change their answers.
Reasons 1, 2, and 3 were chosen as they are directly related to psychiatric illness, defined as “illness-oriented” reasons for refusing medication. Although reasons 1 and 2 are both delusional, reason 1 reflects lack of insight to the physical illness while reason 2 stems from paranoid thinking. Both options were included in order to examine whether participants would respond differently to different delusional content. Reason 3 is also illness-oriented; however, it is not delusional. It was thus included to see if participants respond differently to delusional (reasons 1–2) versus non-delusional (reason 3) illness-related reasoning.
Reasons 4 and 5 are not directly related to psychiatric illness and defined as “non-illness-oriented” reasons for refusing medication. Reason 4 reflects the patient’s basic negative attitude towards injections and reason 5 relates specifically to diabetes treatment. Both reasons may be interpreted as reflecting poor judgment, especially in the context of IHPP. They are not, however, delusional or directly related to an acute psychiatric condition. Reasons 4 and 5 were thus used to examine whether participants differentiate between illness-oriented and non-illness-oriented reasoning, and between two different types of non-illness-oriented reasoning.
Finally, section (c) consisted of two questions regarding legal knowledge about involuntary medication in IHPP, as follows: (1) “Does the law allow for forced psychiatric treatment in IHPP?”; (2) “Does the law allow for forced treatment of physical morbidity in IHPP?”
This section was presented after the vignettes to eliminate response bias.
Participants
Medical Doctors and Nurses working at a major Mental Health Centre in Israel were contacted via organizational email and WhatsApp and asked to participate in the study with a link. Data was collected over 17 days (08/15/21 to 09/03/21), using the online survey platform Qualtrics. Inclusion criteria were medical doctors and nurses who consented to participate in the study and completed the questionnaire online. Exclusion criteria were those who disagreed to participate or did not complete the questionnaire. 126 staff members entered the questionnaire link. Six did not consent to participate and 31 failed to complete the questionnaire. The final sample included 89 participants: 55 (61.8%) Medical Doctors (28 seniors and 27 residents, all of them psychiatrists) and 34 (38.2%) Nurses. 95.5% worked or still work in a closed psychiatric ward. 39 (43.8%) were males and 50 (56.2%) females. The mean age was 41 years, ranging from 26 to 66 years. Doctors (Mean age = 36) were overall younger than Nurses (Mean age = 49).
Ethical considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the Medical Centre IRB (reference BN-665-21) and the Ethics Committee of the University (reference 0003604-1). The respondents’ anonymity was kept (no identifying data collected). Informed consent was obtained via checking the agreement box in the digital consent form.
Data analysis
The SPSS statistical package, version 27 (IBM Corp., Armonk, NY) was used for the quantitative data analysis. Cronbach’s alpha measured the internal consistency of the questionnaire and subscales. A chi-square test examined the relationship between sociodemographic variables and research dependent variables. A comparative analysis compared doctors’ answers with that of nurses, using t-tests for independent samples. A multivariate factorial analysis (MANOVA) examined which variables influence the willingness of participants to treat the theoretical patients involuntarily. Variables included (1) severity of the patient’s medical condition (p < .01), (2) the reason for treatment refusal (p < .01) and (3) sociodemographic variables (occupation, level of religiosity and seniority).
Results
Severity of the medical condition
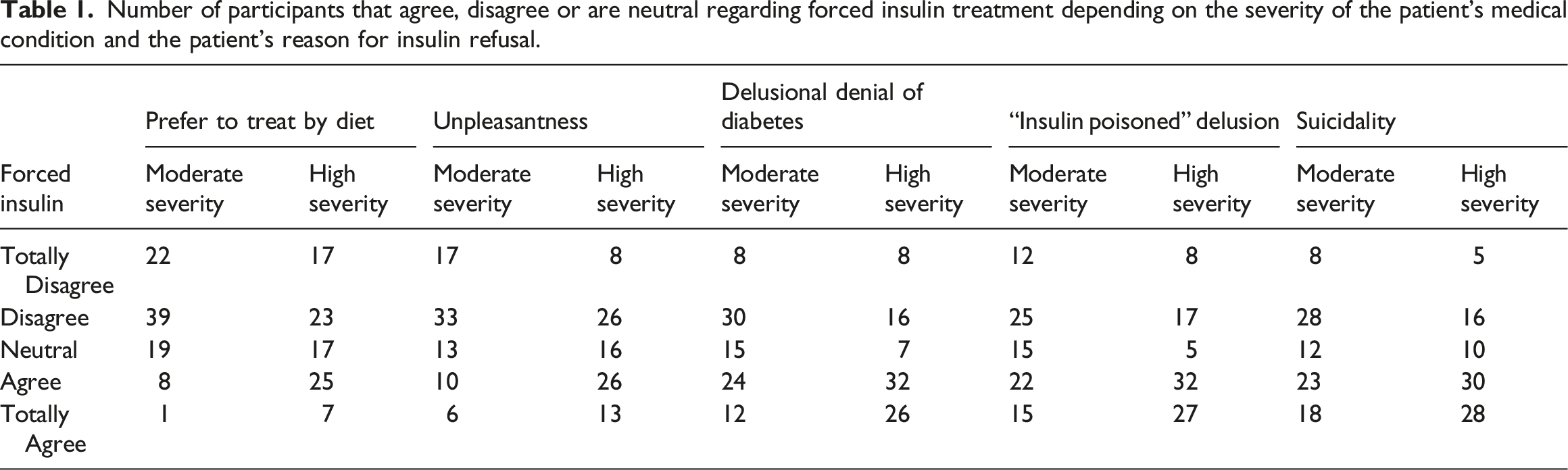
The severity of the patient’s medical condition was associated with participants’ willingness to give insulin despite patient objection (F(1, 87) = 49.41, p < .01) and was independent of the patient’s reason for refusing insulin. Namely, for any given reason for insulin refusal, a greater number of participants agreed or totally agreed with compulsory treatment for the patient in the high rather than moderate severity vignette. In parallel, for each reason for treatment refusal, a greater number of participants disagreed or totally disagreed with compulsory insulin for the patient in the moderate rather than high severity vignette (see Figure 1 and Table 1). Number of participants that totally agree (orange) and agree (blue) with compulsory insulin treatment against the severity of the patient’s medical condition and the patient’s reason for insulin refusal. Number of participants that agree, disagree or are neutral regarding forced insulin treatment depending on the severity of the patient’s medical condition and the patient’s reason for insulin refusal.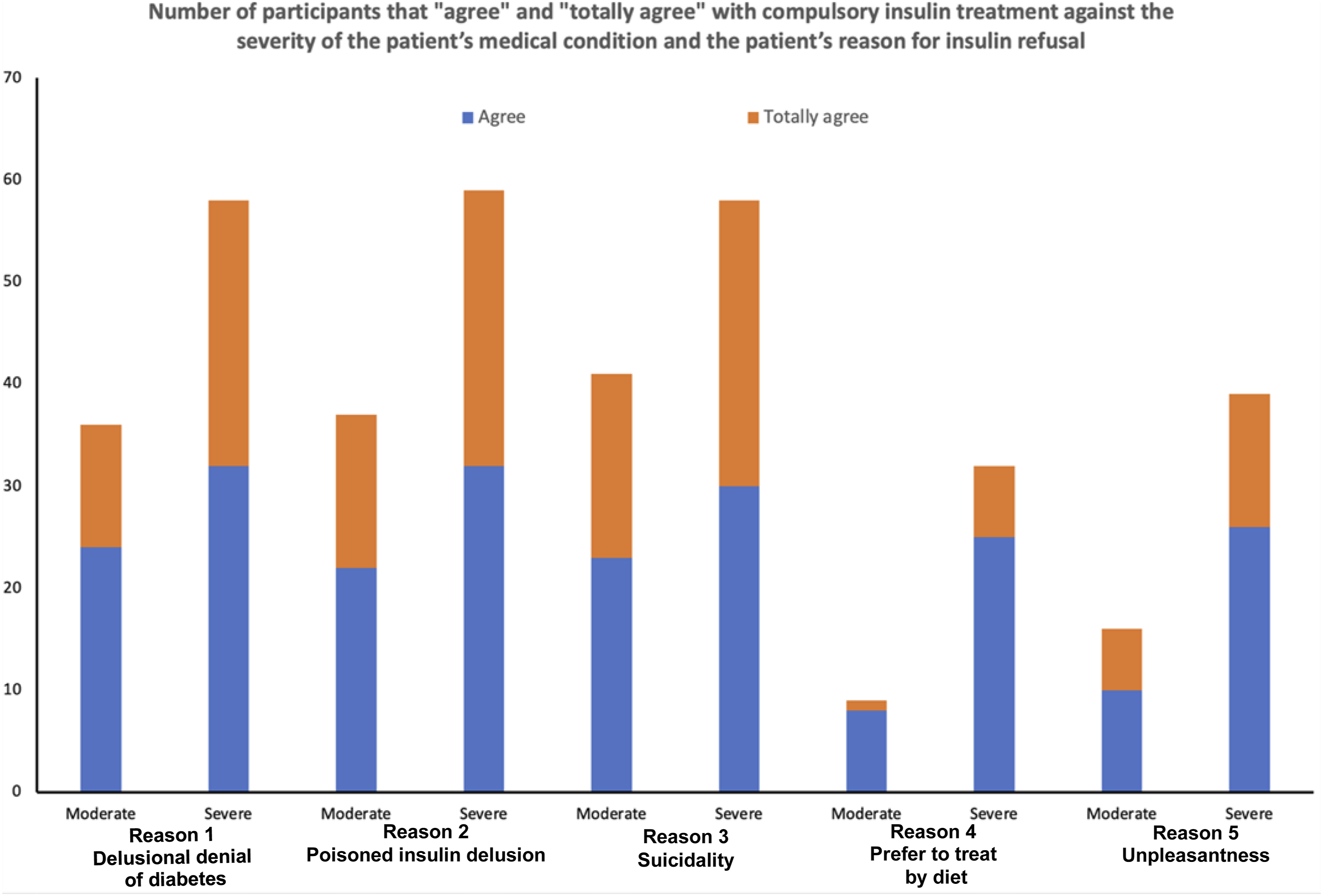
Participants’ answers to all five reasons for insulin refusal combined yielded a mean score of 2.78 for the moderate severity vignette and 3.35 for the high severity vignette. Since a score of 3 is neutral, participants tended to disagree with compulsory treatment for the patient in the moderate severity vignette (mean score <3) but tended to agree for the high severity vignette (mean score >3).
Reason for treatment refusal
The patient’s reason for refusing treatment was significantly associated with participants’ tendency to give insulin (F(1, 87) = 33.44, p < 0.01).
When reason for insulin refusal was “non-illness-oriented,” that is not directly related to psychiatric illness (i.e. preference to control diabetes through diet or disliking injections), participants tended to disagree with compulsory treatment (mean = 2.64).
When reason for insulin refusal was “illness-oriented,” however, (i.e. the delusional denial of diabetes, the poisoned insulin delusion or suicidal motivation), participants tended to agree with compulsory treatment (mean = 3.34). Additionally, when reason for refusal was non-illness-oriented, participants’ mean score was 2.96 (a tendency to disagree) for the high severity and 2.34 (a stronger tendency to disagree) for the moderate severity vignette. In parallel, when reason for refusal was illness-oriented participants’ mean score was 3.62 (tendency to agree) for the high severity and 3.07 (a lesser tendency to agree) for the moderate severity vignette (Figure 2). Participants’ mean scores regarding their willingness to provide compulsory treatment differentiated by illness severity and illness-oriented (delusional thinking and suicidality) versus non-illness-oriented (prefer to treat by diet, unpleasantness) reasons for refusal.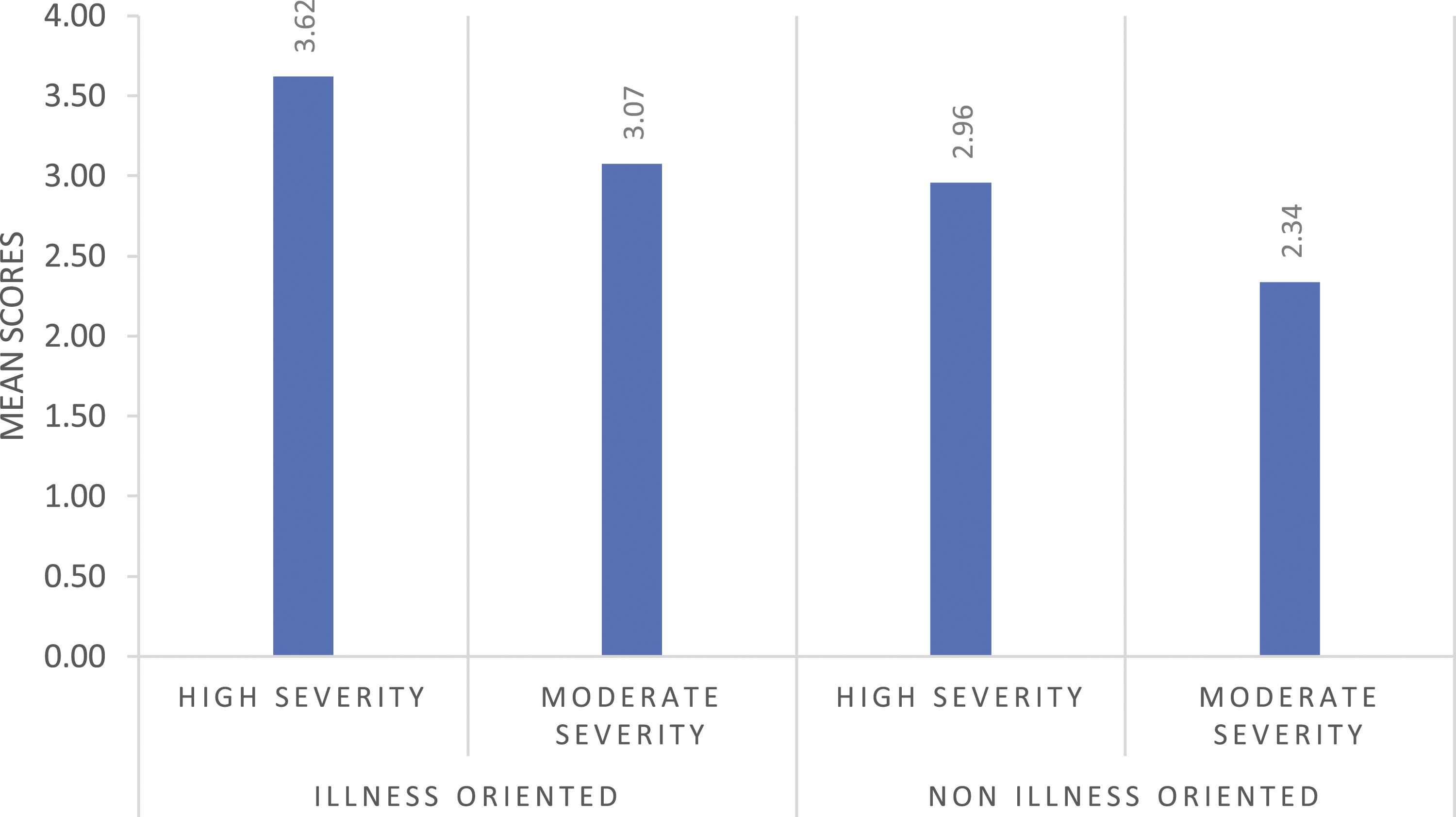
There were no significant differences in participants’ answers between different illness-oriented reasons for treatment refusal. This means that participants were just as likely to agree with compulsory treatment whether the patient’s reasoning was psychotic or not psychotic but suicidal.
Participants’ were least likely to agree with compulsory treatment if reason for refusal was based on the preference to treat diabetes by diet and most likely to agree with it if the patient was suicidal (Figure 3). Participants’ mean scores regarding their willingness to provide compulsory treatment, differentiated by both medical severity and reason for treatment refusal.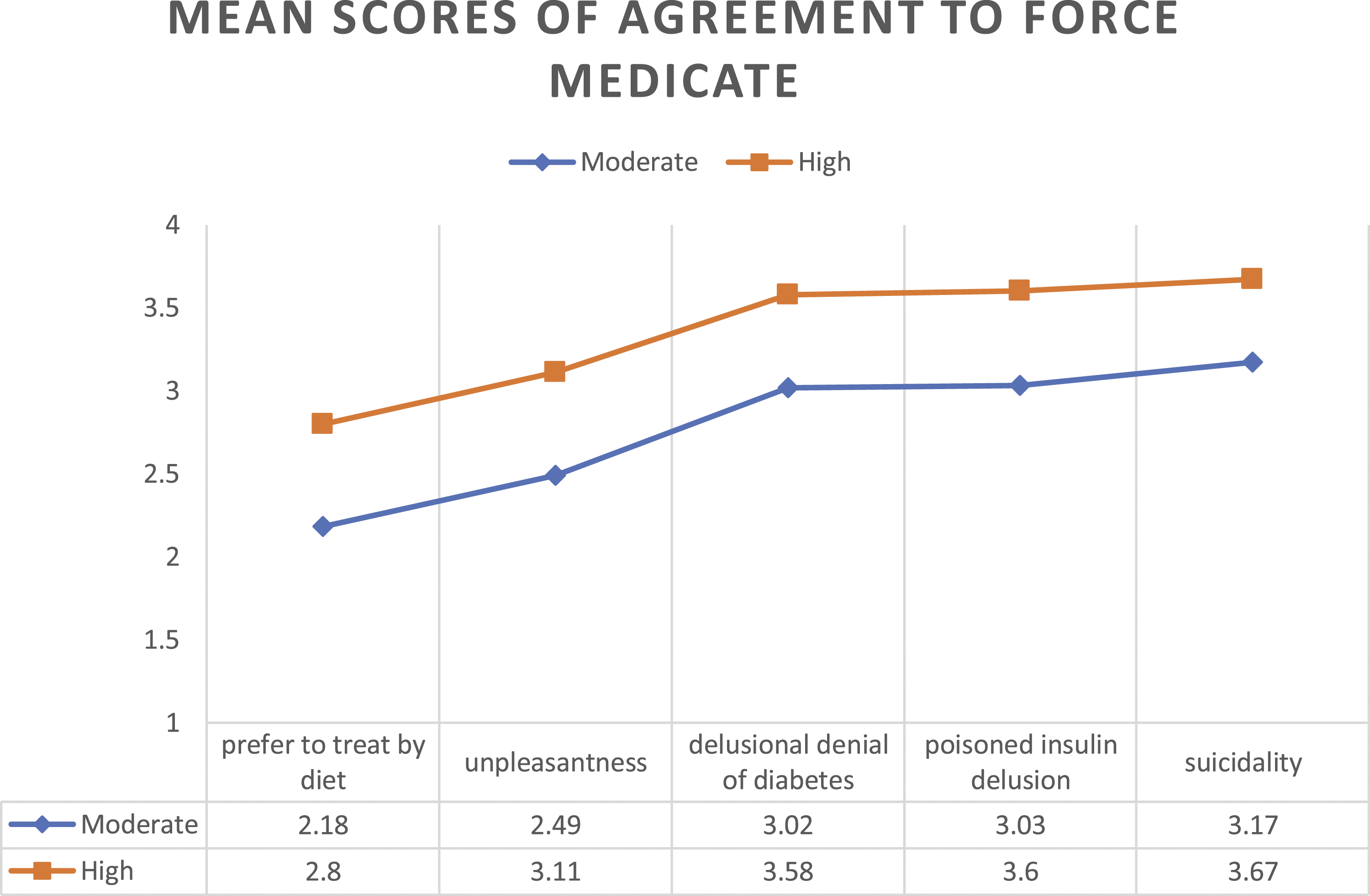
Sociodemographic variables
Occupation, religion, religiosity level, and professional seniority were not significantly correlated with willingness to provide compulsory medication. A significant association was found, however, between occupation and medical severity (F(1, 87) = 20.33, p < .01). Namely, for the high severity case, doctors tended to agree with compulsory medication (mean = 3.62) whilst nurses tended to disagree (mean = 2.96). The difference in doctors’ and nurses’ responses for this case was statistically significant (MD = 0.62, p = .008). For the moderate severity vignette, however, both doctors (mean = 2.61) and nurses (mean = 2.74) tended to disagree with compulsory medication. This difference was not statistically significant.
Knowledge about the law and the willingness to treat by force
97.61% of participants held it was lawful to give forced psychiatric medication to IHPP. Only 23.8%, however, felt that forced treatment of physical conditions was lawful, whilst 63.09% felt it was illegal and 13.09% did not know.
A t test for independent samples comparing the mean differences of participants’ responses determined that responses were not influenced by perceptions about the legality of forced treatment of physical conditions (no statistically significant association). Among those who stated that forced treatment of physical conditions in IHPP was legal, however, the mean score was 3.35 (SD = 0.93), indicating a tendency to agree with compulsory treatment. For those who stated that it was illegal the mean score was 2.9 (SD = 0.99), indicating a tendency to disagree with compulsory treatment. Interestingly, the majority of the participants, who stated that forced treatment of physical conditions in IHPP is illegal, agreed or strongly agreed to compulsory treatment in the high severity vignette that involved illness-oriented refusal to treatment (poisoned insulin delusion 55.3%; delusional denial of diabetes 53.5%; suicidal ideation 53.5%). These respondents thus held that the patient should receive treatment despite it being perceived as illegal.
Discussion
This study focused on psychiatrists’ and nurses’ attitudes regarding compulsory treatment of physical illness in IHPP. Specifically, the authors tested whether the severity of a patients’ medical condition or their reason for treatment refusal would influence participants’ willingness to provide compulsory treatment.
The results confirmed the authors’ hypothesis that both severity of medical condition and reason for treatment refusal were associated with participants’ willingness to provide compulsory treatment. More specifically, if the reason for refusing treatment was illness-oriented, or if the medical condition was severe enough, participants favored compulsory treatment.
Compulsory treatment restricts patient liberty, which can be defined as “the absence of obstacles.” 29 Liberty is seen as highly valuable 29 and ruthlessly defended even at the price of self-harm. 30 The ethical justification for compulsory treatment in situations such as in this study, however, is based on the duty to protect patients from harming themselves. Participants’ views may thus implicitly reflect an agreement with Berlin’s famous distinction between positive and negative liberty. 31 Liberty, as Berlin describes it, is not only a freedom from external coercion (negative liberty), but also the ability to make genuinely authentic decisions, that are in line with one’s core values (positive liberty).
When IHPP refuse insulin for diabetes because of an illness-oriented reason, their refusal is arguably not a rational decision that reflects authentic personal values. Their freedom to refuse treatment (negative liberty) may thus be justifiably restricted temporarily. This idea was reflected in our study results: participants most strongly opposed compulsory treatment for moderate severity, non-illness–oriented refusal cases and most strongly favored compulsory treatment for high severity, illness-oriented refusal cases (Figure 2). It is possible that participants felt that when treatment refusal leads to grave consequences, or was influenced by mental illness, the refusal did not stem from authentic personal values, thus justifying the restriction of negative liberty. It is important to note, however, that a more accurate understanding of the participants’ reasoning requires a more detailed exploration which is beyond the scope of this study.
The idea that IHPP’s decision-making capacity regarding treatment may be distorted is supported by various studies. One study, for example, revealed that the majority of hospitalized schizophrenia patients lacked formal capacity regarding treatment decisions when delusional or lacking insight. 32 Others found that most patients who are forcibly hospitalized and given psychiatric treatment retrospectively agreed with it once stabilized.33,34
This study also found that within the category of illness-oriented reasons for insulin refusal, participants were just as likely to endorse compulsory treatment whether the refusal was psychotic in origin, or non-psychotic but related to suicidality. This is significant, as according to Israeli law, the types of mental illness warranting involuntary hospitalization are usually restricted to psychotic ones. It was thus reasonable to expect that our Israeli participants’ views would reflect the legal distinction between psychotic and non-psychotic conditions. Nevertheless, participants’ responses were more in accordance with legal approaches that do not require psychotic symptoms as necessary for involuntary hospitalization. It remains questionable as to whether this moral intuition, consciously or non-consciously, influences participants’ everyday decision-making regarding involuntary hospitalization and if so, to what extent patients’ who are suicidal but not psychotic are involuntary hospitalized.
Furthermore, the severity of the patient’s medical condition was associated with participants’ willingness to give insulin regardless of reason for insulin refusal (Figure 1). This suggests there is an implicit consequentialist moral intuition to restrict patient liberty and autonomy based on the expected results of not receiving treatment. In situations where foreseeable danger is clear and immediate, there is less tolerance to patient refusal, at least it the context of IHPP.
Participants’ diverse views regarding the legality of compulsory treatment of physical illness is another remarkable finding. As abovementioned, under Israeli law, IHPP may be given “medical treatment” against their will. The meaning of “medical treatment,” however, is ambiguous. In the absence of clear legal guidelines, it is unsurprising that 13% of participants were unsure about the legality of compulsory treatment of physical illness in IHPP. The majority (63.09%), however, thought it illegal, whist a significant minority (23.8%) thought it legal. Arguably, the clinical practice of our participants is influenced by these diverse perceptions. Treatment refusal of physical illness by IHPP may thus be resolved differently based on the differing views of the treating medical staff. This potential reality highlights the need to establish clear guidelines regarding the appropriate mode of action in such situations.
The gap between what most participants believe the law requires and what they think the standard of care should be is another disturbing as well as surprising finding. 63.09% held that compulsory treatment for physical illness in IHPP is illegal. Despite this, the majority of these same participants supported compulsory treatment for patients in the high severity vignette whose reason for refusal was illness-oriented. This finding calls for attention in multiple directions. First, it may reflect caregivers’ mistrust in the legal system or in the solutions it provides to complex clinical situations. In parallel, from the legal system perspective, the willingness of caregivers to disobey—at least in theory—the perceived legal requirement, is alarming. This likely further increases the mutual mistrust between mental health caregivers and the legal system. Our study may thus reflect a tension that has already been suggested to have existed between the legal system and mental health caregivers. 35
In addition, it is important to mention that our subjects were doctors and nurses who likely confront this dilemma quite frequently. The disparity between their perception of what they should do legally and are inclined to do based on personal moral intuition may lead to moral distress. 36 Educational and supportive interventions may thus be needed to minimize the moral distress associated with treatment refusal. In addition, on-site supervision may be required to minimize potential deviations from institutional guidelines in such situations, given the high likelihood that at least some caregivers have strong opinions regarding this topic.
Finally, there was a statistically significant difference between doctors’ and nurses’ views regarding the patient in the high severity vignette: doctors tended to agree with compulsory medication (mean = 3.62) whilst nurses tended to disagree (mean = 2.96). The treatment of IHPP may be highly intense. Disagreements between doctors and nurses and the lack of clear guidelines regarding treatment refusals for medical illness may add unnecessary stress to this already stressful situation and negatively affect the quality and outcomes of treatment. Having clear guidelines may thus minimize disagreements and improve the quality of care.
Limitations
This study has some shortcomings related to the inherent limitations of survey research.
First, there is a potential selection bias, as only participants interested in sharing their views were included. Moreover, our survey was distributed via organizational email and WhatsApp, meaning the loss of participants who felt uncomfortable using an electronic interface, or cooperating with a research initiative perceived as coming from their employer.
Second, self-reported data can often be biased. 37 Third, this survey was administered to medical staff working in a specific medical center in Israel, that is, only one site. The inferences, interpretations and generalizability of the findings of this study may thus be limited. This is especially relevant to a study related to ethical and legal issues, which may be influenced by cultural context. Finally, limitations exist in attempting to predict caregivers’ “real life” behavior based on their attitudes in a theoretical survey. 38
Future research should aim to study the attitudes surrounding this topic in other countries, professions, medical situations, patients and families. Other factors (besides severity of the medical condition and reason for treatment refusal) that may influence decisions around compulsory treatment of physical illness can also be explored. Empirical studies focusing on what doctors and nurses do in practice and the outcomes of their practice may also add important information. Finally, whether caregivers who confront our study’s dilemma experience moral distress, and if so, how they deal with it and what could address it, may be the subject of future studies.
Furthermore, a legal-philosophical inquiry into the normative-prescriptive dimensions of this topic may be added to this descriptive, empirical study, namely, what should be the appropriate way to resolve the treatment refusal of physical illness in IHPP.
Additionally, in situations where there is a consensus that compulsory treatment for medical illness is appropriate, given the unique context of IHPP, the following ethical dilemma may arise: What is the most appropriate way to provide the refused treatment? Should patients be informed they are about to receive it in addition to their compulsory psychiatric treatment? Or should this information be omitted to minimize the conflict between patient and medical staff due to the additional coercion of forced medical treatment? In other words, given the minimal “extra” coercion involved in the provision of the medical treatment, is deception by omission ethically appropriate in this situation?39–41 As the deception-by-omission dilemma vividly illustrates, the resolution of one dilemma may open the door to another.
Conclusion
This study is unique as it is the first to explore psychiatric caregivers’ perceptions on compulsory treatment of physical illness in IHPP. The ethical dilemmas experienced by health professionals facing this issue are complex and need to be further discussed in order to create clearer guidelines. This study expands the ethical and legal discussion regarding coercion of psychiatric patients.
The unique therapeutic arena of severe mental illness raises challenging ethical and practical dilemmas. It is thus crucial that healthcare providers are familiar with these complex ethical challenges, are informed and equipped with appropriate solutions (e.g. guidelines) and will continuously search for the most respectful environment for their patients. The voice of psychiatric patients should be heard, 42 including those who are involuntarily hospitalized. Decisions regarding compulsory treatment of IHPP should be made based on a case-by-case basis and the relevant factors influencing each case should be considered, including the severity of the patient’s medical condition and their specific reason for treatment refusal.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.