
Abstract
Background:
Ethical climate and moral distress have been shown to affect nurses’ ethical behaviour. Despite the many ethical issues in paediatric oncology nursing, research is still lacking in the field.
Research aim:
To investigate paediatric oncology nurses’ perceptions of ethical climate and moral distress.
Research design:
In this cross-sectional study, data were collected using Finnish translations of the Swedish Hospital Ethical Climate Survey–Shortened and the Swedish Moral Distress Scale–Revised. Data analysis includes descriptive statistics and non-parametric analyses.
Respondents and research context:
Ninety-three nurses, working at paediatric oncology centres in Finland, completed the survey.
Ethical considerations:
According to Finnish legislation, no ethical review was needed for this type of questionnaire study. Formal research approvals were obtained from all five hospitals. Return of the questionnaire was interpreted as consent to participate.
Results:
Ethical climate was perceived as positive. Although morally distressing situations were assessed as highly disturbing, in general they occurred quite rarely. The situations that did appear often reflected performing procedures on school-aged children who resist such treatment, inadequate staffing and lack of time. Perceptions of ethical climate and frequencies of morally distressing situations were inversely correlated.
Discussion:
Although the results echo the recurrent testimonies of busy work shifts, nurses could most often practise nursing the way they perceived as right. One possible explanation could be the competent and supportive co-workers, as peer support has been described as helpful in mitigating moral distress.
Conclusion:
Nurturing good collegial relationships and developing manageable workloads could reduce moral distress among nurses.
Introduction
Caring for sick children with life-threatening illnesses, such as cancer, exposes nurses to numerous ethical challenges. Despite good intentions to provide ethically good care, personal and professional moral values are challenged in clinical practice. This becomes apparent when paediatric nurses perform uncomfortable medical procedures that cause pain to children or when protective parents limit truth-telling. 1 Furthermore, conflicting perspectives on medical decisions may appear between parents, nurses and other healthcare professionals, which can easily cause disagreements about what is in the best interest of the child. 1 Nurses’ responses to ethical challenges are influenced by the ethical climate. 2
Ethical climate has attracted much attention due to its impact on nurses and on patient care. The interest in ethical climate was sparked by Victor and Cullen who described it as ‘the shared perceptions of what is ethically correct behaviour and how ethical issues should be handled’. 3 The concept was brought into healthcare by Olson, who developed an instrument to measure nurses’ perceptions of ethical climate. 4 According to a Swedish study, less than one-third of the paediatric nurses had a positive perception of their possibilities to practise ethically good care. 5 Other studies have suggested an association between ethical climate and other work-related factors such as job satisfaction and moral distress. 6
When dealing with things beyond their own control and not being able to do the right thing for their patients, nurses encounter discomfort and anguish. These feelings have been comprehended as moral distress since the 1980s when Jameton coined the term. 7 So far, moral distress in paediatric healthcare has been mostly studied among nurses working in paediatric and neonatal intensive care units. Nurses have identified issues anchored in end-of-life care and futile treatments as prominent causes of moral distress, together with unsafe staffing levels. 8,9 The few studies carried out exclusively in paediatric oncology care have suggested that incompetence of healthcare providers and poor communication are other common challenging issues. 10,11 Unattended, moral distress can lead to burnout, anger, sadness, frustration, intention to leave a clinical position, withdrawal from patients and diminished quality of patient care. 12,13
Prior research has found ethical climate and moral distress to be linked with each other. 6 This association has not yet been fully explored in paediatric oncology nursing, but mostly in adult care settings. 6 To fill the gap in current research, a multi-centre project was initiated to investigate ethical climate and moral distress in paediatric oncology care in Nordic countries. To study conditions and practices that influence nurses’ ethical behaviour can result in implications for clinical practice and further research.
Research aim and research questions
In this study, as a part of the multi-centre project in the Nordic countries,
10,14,15
we aimed to explore nurses’ experiences of the ethical climate and moral distress in Finnish paediatric oncology care. Our research questions were as follows: What are the nurses’ perceptions of the ethical climate at their workplace? What are the nurses’ perceptions of moral distress in different situations? Do perceptions of moral distress differ between nurses according to work experience in paediatric healthcare and to level of education? Are perceptions of the ethical climate correlated with levels of moral distress?
Research design
This descriptive, cross-sectional study was carried out in the framework of the Nordic Society for Paediatric Haematology and Oncology (NOPHO) and the Nordic Society of Paediatric Oncology Nurses (NOBOS).
Respondents and research context
We investigated nurses’ perceptions of the ethical climate and moral distress in Finnish paediatric oncology care. The study was conducted at the five paediatric oncology centres located at five University Hospitals in Finland.
The study was carried out in collaboration with the centres. After an initial contact with the head nurses, research permission was obtained from all of the hospitals. Each centre decided upon a suitable starting point. A local coordinator informed personnel about the study and performed the data collection. Altogether, 169 registered nurses, 32 physicians and 9 nursing assistants (n = 210) were invited to complete a pen-and-paper questionnaire. However, this article reports exclusively on registered nurses’ perceptions (n = 169). The five data collections were carried out between May 2019 and January 2020, and the collection periods varied between centres from 3 weeks to 3 months.
Instruments
The questionnaire included questions about the respondents’ demographic characteristics and the survey instruments.
The Swedish Hospital Ethical Climate Survey–Shortened (Swedish HECS-S) was translated into Finnish as described below. The original HECS was developed in the 1990s by Olson, 4 who organised the statements according to nurses’ interactions with other nurses (peers), physicians, patients, managers and the hospital. Later on, the instrument was shortened, and parallel versions were created for nurses, physicians and other professionals. 16,17 The second and the last author of this study coordinated the process of translating and adapting the Swedish HECS-S, 18 with the permission of Dr AB Hamric (email, 15 November 2014) and Dr L Olson (email, 29 May 2015). The Swedish HECS-S is a multi-professional tool intended to measure perceptions of nurses, physicians and nursing assistants, and therefore, the original term ‘peers’ targeting other nurses has been renamed ‘co-workers’ to cover all professions. 18 Consequently, the Swedish HECS-S assesses a dimension of relationships between co-workers rather than relationships to peers. All items are rated on a 5-point scale with labelled end points, ranging from 1 (hardly ever) to 5 (almost always). The higher scores imply more positive perceptions. While the Swedish HECS-S consists of 21 items, it was reduced to 18 items in the present analysis, due to irrelevance of three questions aimed at nursing assistants, as in two participating centres nursing staff consisted of registered nurses only.
The Swedish Moral Distress Scale–Revised (Swedish MDS-R) was translated into Finnish as described below. The original MDS was developed by Corley et al. to investigate moral distress among intensive care nurses. 19 It has since been shortened 16 and revised for other professions and settings. 20 The instrument has earned an extreme popularity in various healthcare settings and cultures. The items describe clinical situations and internal and external constraints 20 that healthcare providers may experience as disturbing: end-of-life care and quality of life, poor communication, staffing and material resources, hierarchies of decision-making and witnessing unethical behaviour. 21 The second and the last author of this study coordinated the process of translating and adapting the Swedish MDS-R et al, 15,22 with permission from Dr AB Hamric (email, 6 October 2014), for multi-professional use in paediatric oncology care. The Swedish MDS-R consists of 26 items whereof each is rated twice: first, how disturbing (intensity) the situation is assumed to be, and second, how often (frequency) the situation occurs. Items are scored on a 5-point scale with labelled end points: the intensity scores range from 0 (not at all) to 4 (very negatively), and the frequency scores range from 0 (never) to 4 (very often). The higher scores indicate higher moral distress levels.
Translation process and validity. Content validity of the Swedish versions of the HECS-S and the MDS-R had been assessed in preceding Swedish studies. 10,14,15 The Swedish HECS-S and the Swedish MDS-R were translated from Swedish to Finnish using a translation method described by Daniel et al. 23 with an aim to attain conceptual and content equivalence. The process involved two translations, one by the first author, who is a native Finnish speaker and fluent in Swedish, and another by a professional translator. These two translations were compared and converged during a group interview with three native Finnish speaking healthcare professionals working at a paediatric oncology centre in Sweden. Thereafter, face validity of the Finnish questionnaire was tested in six cognitive interviews with native Finnish-speaking healthcare professionals, using the Think Aloud technique. 24 Continual discussions were held between the authors, and some changes were made after comparing, when applicable, wording with an existing Finnish version of the original HECS, 25 after obtaining permission (email, R Suhonen, 19 December 2018). Translating the MDS-R from Swedish (a Germanic language) to Finnish (a Uralic language) provided linguistic challenges while attempting to maintain similar sentence structure.
Analysis
Data were analysed using IBM SPSS Statistics 25. Questionnaires with less than 10% missing answers were included in the analysis. To judge the reliability of the instruments, Cronbach’s alpha values were calculated. Frequencies and central tendencies were calculated to summarise the data. Categorical data were described as counts and percentages and ordinal data as means with standard deviations (SDs). The decision to present means was based on current praxis in the field, to enable comparisons between studies. Mean values per respondent were calculated for each scale, and the differences between groups were analysed with Mann–Whitney U-test. A Spearman’s rank-order correlation was run to evaluate the relationships between mean values. In all analyses, p < 0.05 was considered as statistically significant.
Ethical considerations
The study followed the ethical principles for conducting research. 26 The Finnish National Board of Research Integrity (email, P Louhiala, 28 February 2018) informed us of the Finnish legislation that does not require ethical review for questionnaire studies. Applications for research permissions were made to each hospital. All five University Hospitals reviewed and approved the study (50H116, 62/2019, 110/2019, HUS/284/2019, T08/014/19). Research applications included inter alia a description of data protection required by the EU General Data Protection Regulation (GDPR). A cover letter was attached to the questionnaires, explaining the purpose of the study and the voluntary nature of participation. Respondents were assured that all data would remain confidential. Formal signed consents were not obtained; instead, the returning of the questionnaire was interpreted as consent to participate.
Results
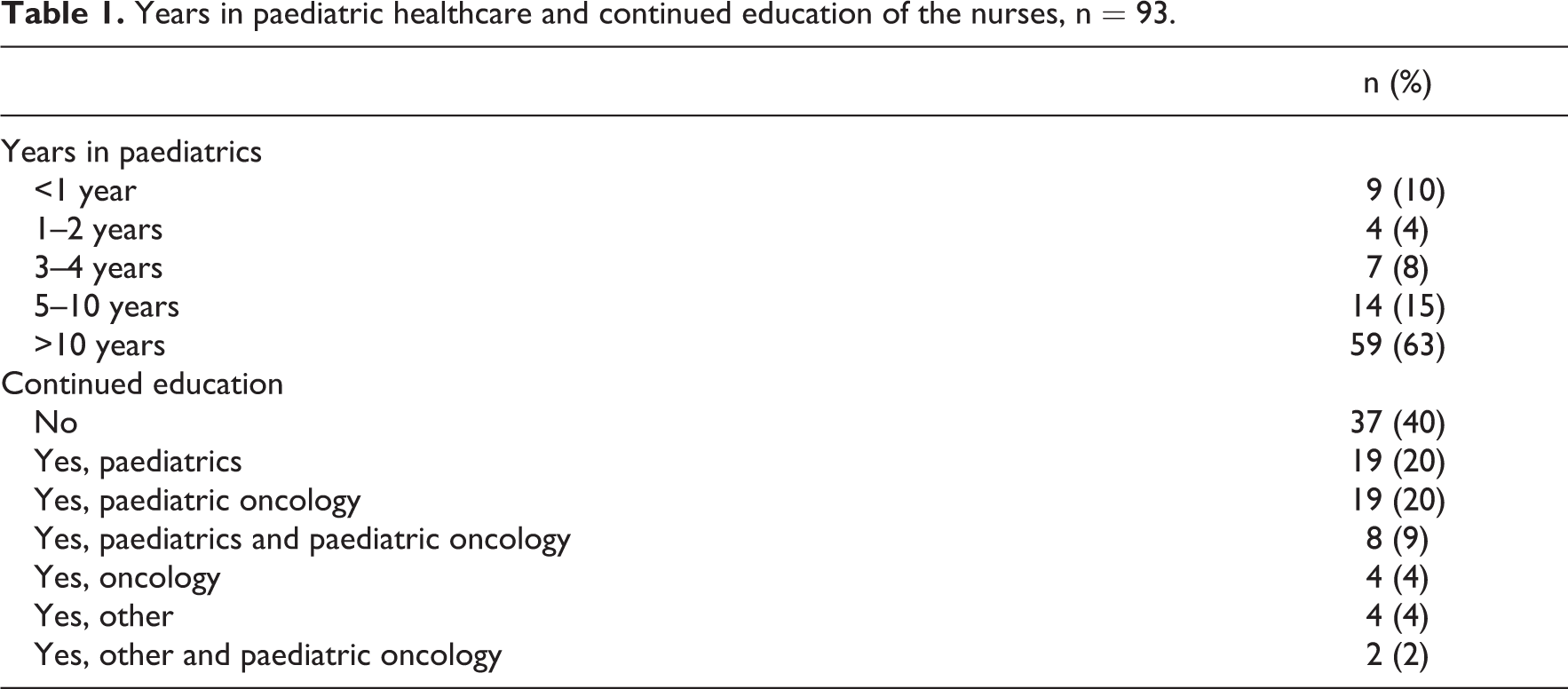
Altogether, 169 nurses who were on duty during the data collection periods received the questionnaire, and 96 (57 %) of them returned it. The response rate varied between centres from 32% to 83%. Three nurses were excluded from this study as they did not provide direct patient care, and thus, this study includes 93 nurses. However, one respondent had bypassed the HECS-S instrument and six other respondents had left more than 10% of the MDS-R questions unanswered, motivating their exclusion from the respective analysis. Thus, the total number of valid responses was 92 for the HECS-S and 87 for the MDS-R. Almost all nurses were females (n = 88; 95 %). As shown in Table 1, most nurses had worked in paediatrics for more than 5 years (n = 73; 79 %) and over half of the nurses had completed continued education (n = 56; 60 %).
Years in paediatric healthcare and continued education of the nurses, n = 93.
Reliability of the instruments
A good internal consistency was confirmed with a Cronbach’s alpha of 0.842 for the Finnish HECS-S and a Cronbach’s alpha of 0.922 for the intensity scale and 0.862 for the frequency scale for the Finnish MDS-R.
Nurses’ perceptions of the ethical climate
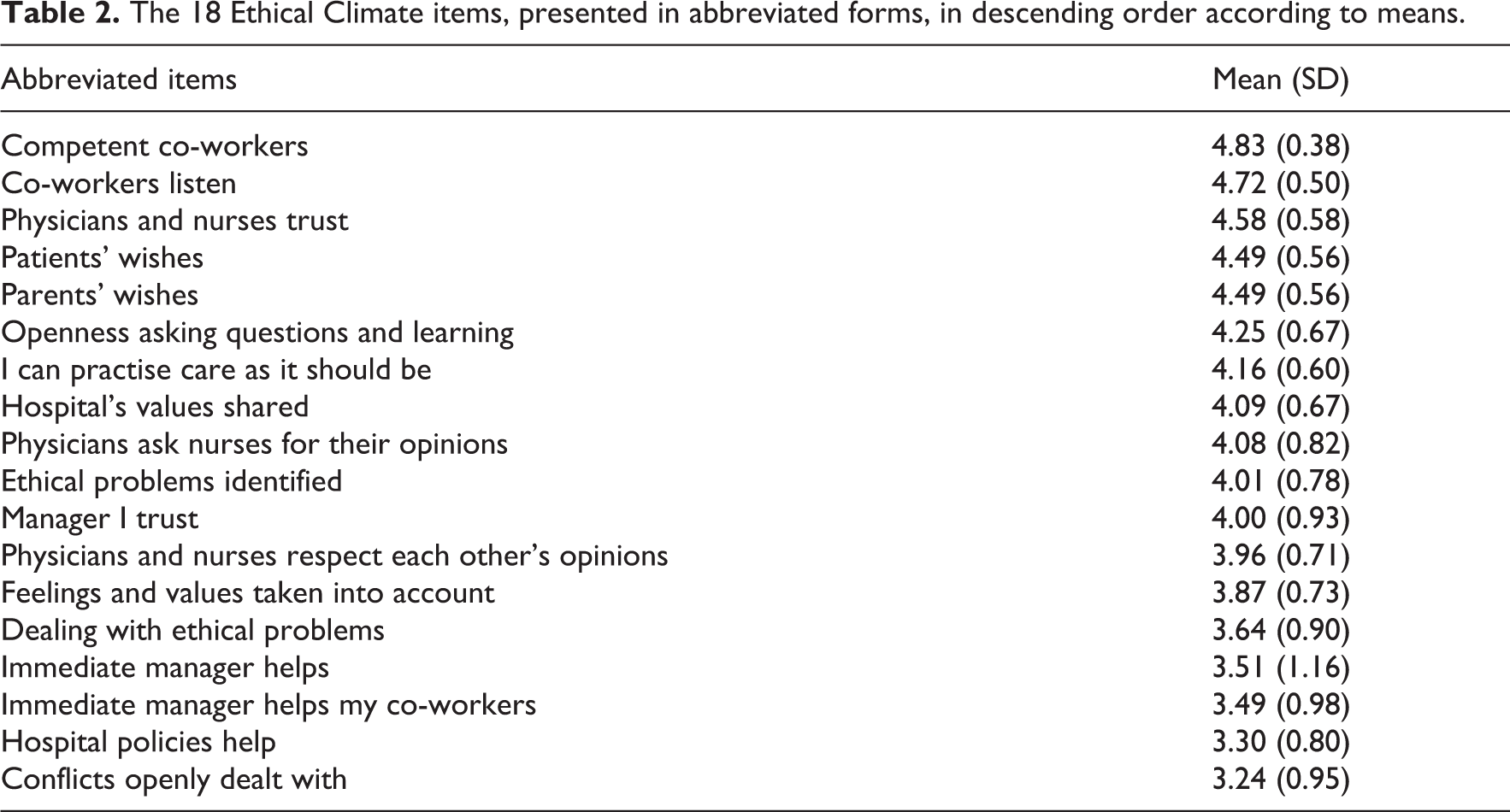
In general, nurses’ perceptions of the ethical climate were positive. The respondent mean for all 18 items, on a scale of 1 to 5, was 4.0 (SD, 0.4). None of the items had a mean score below the midpoint of 3. The highest scored items reflected relationships between co-workers and relations to patients and to parents. Perceptions of working with competent co-workers had the highest mean (4.8; SD, 0.4), as seen in Table 2. The items that reflected perceptions related to hospital policies and conflicts were scored lowest, but with a wider variation between individual nurses. Overall, items assessing relationships to managers were scored lower than items assessing relationships to co-workers.
The 18 Ethical Climate items, presented in abbreviated forms, in descending order according to means.
Nurses’ perceptions of moral distress
Perceived intensities
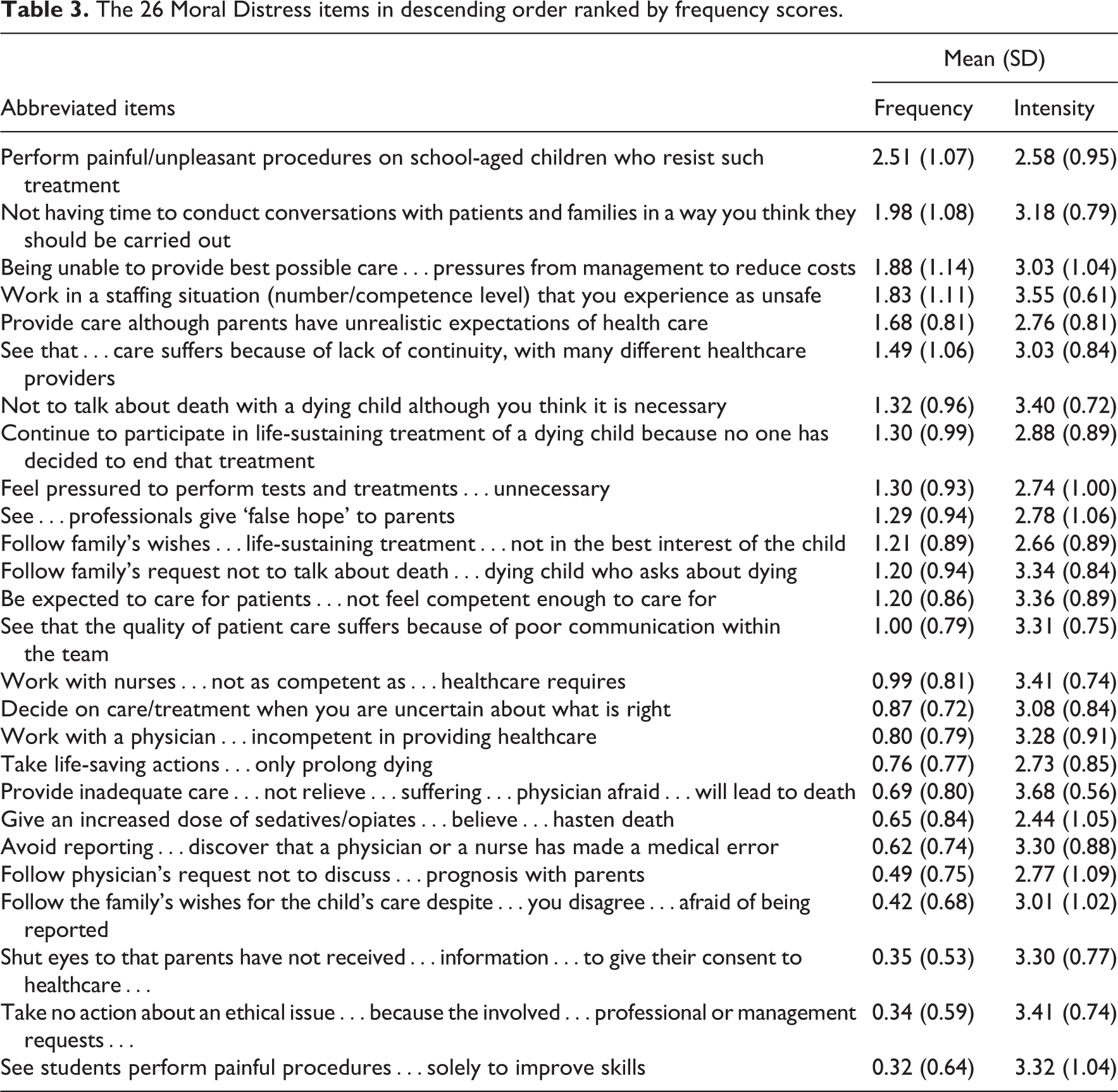
Overall, the disturbances of the situations described in the MDS-R were scored higher than the frequencies. Nurses assessed almost all scenarios as very disturbing; the respondent mean for intensities was 3.1 (SD, 0.5) on a scale of 0–4. All 26 items had a mean intensity score that exceeded the midpoint of 2.
Perceived frequencies
Many nurses perceived several situations described in the MDS-R as uncommon; 12 items out of 26 had a mean frequency score below 1 on a scale of 0–4. The situations that rarely or never occurred involved witnessing unethical behaviour, end-of-life care, hierarchies of decision-making, lack of competence and poor communication. The overall mean score for frequencies was 1.1 (SD, 0.4). The situation involving procedures on resistant school-aged children was the only item with a mean frequency score above the midpoint of 2 (mean, 2.5; SD, 1.1). Other situations, that were scored as moderately frequent, reflected lack of resources: unsafe staffing levels, shortage of time and cost reductions (Table 3).
The 26 Moral Distress items in descending order ranked by frequency scores.
Differences according to work experience in paediatrics and education
Overall, nurses with more than 5 years of work experience in paediatric healthcare assessed situations as significantly (U = 874, p = 0.008) more frequent (mean, 1.2; SD, 0.4) than nurses with less than 5 years of experience (mean, 0.8; SD, 0.4). The perceptions of intensities averaged 3.1 (SD, 0.5) in both groups. Perceptions did not differ significantly between nurses with basic education and nurses with continued education.
Correlation between the ethical climate and moral distress
There was a moderate, negative correlation between the perceptions of ethical climate and moral distress frequencies (r = −0.435, n = 86, p < 0.001). No significant correlation was found between the perceptions of ethical climate and moral distress intensity scores (r = 0.032, n = 86, p = 0.769). The pattern that shows differences between centres can be seen in Table 4.
The ethical climate and moral distress intensity and frequency for each centre.
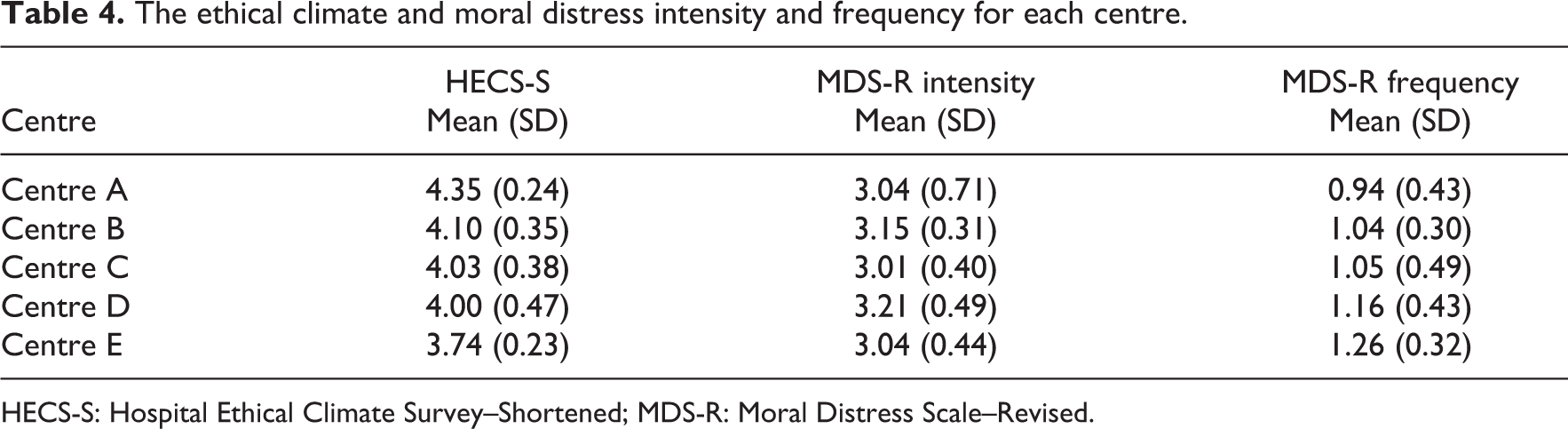
HECS-S: Hospital Ethical Climate Survey–Shortened; MDS-R: Moral Distress Scale–Revised.
Discussion
In this study, we surveyed nurses working in Finnish paediatric oncology care and explored their perceptions of ethical climate and moral distress. Overall, the perceptions of the ethical climate in paediatric oncology centres were positive, and the majority perceived that they most often could practise nursing the way they believed it should be practised. Clinical situations generating moral distress were perceived as quite uncommon, but highly disturbing. An association between ethical climate and frequencies of morally distressing situations was identified.
Nurses in this study shared a positive view on ethical climate. Even in previous studies, perceptions of ethical climate have been mostly positive, according to Koskenvuori et al. 6 As a part of our current project, ethical climate had already been investigated in paediatric oncology care in Sweden. 14 Those results suggested positive perceptions in general, but they also revealed that physicians had more positive perceptions than nurses. Compared to nurses in Sweden, Finnish nurses perceived the ethical climate as slightly more positive. The most favourable perceptions reflected relationships to co-workers, and in particular their competence. This probably mirrors the lengthy clinical experience most nurses possessed. Although cross-sectional studies must be interpreted with caution, it could be argued that promoting collegiality and retaining skilled nurses may help to build a positive ethical climate. In any case, medical knowledge and nursing skills need to be kept up to date, and thus, ongoing learning activities are needed to nurture the professional development of nurses. 27
In accordance with prior findings, 9,14 nurses perceived that conflicts were not always openly dealt with at their workplaces. This tendency may partly depend on how the expression ‘openly dealt with’ has been interpreted, as some concerns might require privacy. Conflicts involving unprofessional confrontations in front of others have been characterised as destructive. 28 Even though conflicts were not always openly dealt with, our results suggest that conflicts were more often dealt with than avoided. This is coherent with Johansen and Cadmus 29 who reported that only one out of four nurses used an avoidant conflict management style.
The hospital policies were not always found helpful in difficult patient care situations. This perception is in line with previous studies. 9,14,30 One possible explanation to this moderate perception could be that complex healthcare situations often require other resources than policies alone. Facilitated ethics discussions and clinical ethics support services can aid care teams to clarify complex ethical problems. 31 Winter et al. 32 found paediatric ethics consultations as rare, but when requested, they most often concerned issues related to non-beneficial treatments. According to Leland et al., 33 many paediatric ethics consultations involve provider moral distress. Fortunately, nurses consider formal ethics support as helpful in resolving moral distress. 34
We found that disagreements on end-of-life care as a root cause of moral distress were not quite as prominent in paediatric oncology units as those reported in critical care settings. 8,21 Although grief and loss are unavoidable in paediatric oncology nursing, 35 not all emotionally distressing situations generate moral distress. It is also important to bear in mind that even if paediatric oncology nurses’ experiences of end-of-life care include poor communication, limited truth-telling and cultural obstacles, 36 moral distress is not inevitable in all end-of-life care. It is possible that qualitative research methods would better capture experiences of moral distress in end-of-life care, and further studies using interview methodology are needed to develop a full picture on the topic. However, morally distressing situations during this vulnerable time should never be overlooked or belittled, as nurses assessed them as highly distressing if or when they occur, and their impact on nurses can be adverse and long-lasting.
The situations our study identified as major sources of moral distress in paediatric oncology nursing reflected performing procedures on school-aged children who resist such treatment, nurses’ lack of time and inadequate staffing levels. Our results describe lack of resources, compared to prior findings, 9,10 and unfortunately, they mirror the worldwide situation in nursing with heavy workloads and nursing shortages. 37 Recently, Hopia and Heino-Tolonen 38 described that busy work shifts caused concerns among paediatric oncology nurses, as a lack of time stopped them from supporting families in a way they felt was needed. Similarly, Newman et al. 39 reported that failing to provide compassionate, high-quality care escalated moral distress among paediatric oncology nurses. How to balance a healthy work environment with challenging ethical issues and financial cut-backs is a puzzle, but nurturing an ethical climate and collegiality may help to withstand moral distress. Sharing troublesome experiences with peers helps nurses to endure moral distress, 40 and evidently, communication and collaboration correlate not only with reduced levels of moral distress but also with improved quality of care. 39
Uncomfortable procedures against children’s will, and the potential infringement on children’s autonomy, presents an ethical challenge in paediatric nursing care. 1 Physical restraint of small children is perceived to be quite common and distressing. 41 According to the nurses in our study and earlier findings from Sweden, 15 even older children resist treatments quite often, but compared to the Swedish results, nurses in Finland did not find these situations quite as disturbing as nurses in Sweden did. This item was added in the Swedish MDS-R, 15 and the high scores show its relevance in paediatric nursing studies. Although our results do not reveal reasons for resisting and unwillingness among school-aged children, Bray et al. 42 have shown that children value detailed information about the planed procedure and the individual coping strategies they can use. Thus, it should be considered whether improved dialogue and preparations could prevent some of these situations.
Prior studies have reported conflicting results on moral distress and its relation to nurses’ education and work experience. 43 These relationships have been studied by many scholars without proof of significant associations, 44,45 while some have observed that nurses with longer experience report higher levels of moral distress. 46 Our results indicate a link between years in nursing and frequencies of distressing situations. This could be explained by the rarity of the situations: apparently it will take some time before novice nurses have experienced the situations described in the MDS-R. However, neither nurses’ level of education nor years in paediatric healthcare affected the level of disturbance. Maybe the repetitive exposure to distressing situations over time is not solely disadvantageous. According to Helmers et al., 34 it can broaden the understanding of different ways of dealing with ethical dilemmas, leading to a wider perspective on ethical issues that in turn can be helpful in diminishing experiences of moral distress.
Our study supports the proposed relationship between ethical climate and moral distress. 44,47,48 However, we found this relationship significant only when comparing to moral distress frequencies. This pattern can be clearly noticed by comparing centres: the more positive the ethical climate, the less frequent the experiences of distressing situations. Whether it is an absence of distressing situations that contributes to more positive perceptions of ethical climate, or the other way around, remains uncertain, as the methodological limitations of cross-sectional, correlational studies make it difficult to draw conclusions on causality.
The main limitation of this study is the low response rate. Despite the diligent participation in some centres and the reminders sent by the local coordinators during data collection periods, the overall response rate remained low. Since we did not gather identifying information in the form of nurses’ names or ages, or length of work experience in paediatric oncology, it was not possible to identify the non-responders. Another limitation is the geographic context. Some perceptions are sensitive to social and cultural influences, and therefore, the findings might not be generalizable to other countries.
Conclusion
Taken together, paediatric oncology nurses share a positive view of the ethical climate and especially of their co-workers’ competence and support. Morally distressing situations described in the MDS-R are, in general, more disturbing than frequent. Lack of time and inadequate staffing levels continue to be among the most frequent, morally distressing situations. These findings highlight the importance of good collegial relationships and suggest that continued efforts are needed to secure manageable workloads for the nurses to reduce moral distress. Finally, this study adds to a growing body of evidence that indicates a negative correlation between ethical climate and moral distress. Since this study is cross-sectional, it is not possible to explain the causality. Therefore, further studies are needed to better understand this association and to provide suggestions on how to best apply this knowledge in paediatric oncology nursing.
Footnotes
Acknowledgements
We thank all healthcare professionals who contributed to the translation process of the survey instruments. We also thank all local contributors in Finland who provided general support or carried out data collections: Kristian Juusola, Johanna Viitanen, Maarit Tuomela, Anna-Kaisa Myllynen, Anne Rajatammi, Mervi Taskinen and Tarja Heino-Tolonen. Also, we express our gratitude to the nursing leadership at each hospital who kindly supported our study. A very special thank you to all participating nurses who made this study possible.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors received financial support from the Doctoral School in Health Care Sciences at Karolinska Institutet (HK18) and the Swedish Childhood Cancer Fund (grant numbers PR2017-0123; TJ2017-0011). The funders did not have any role in the study design, data collection, analysis, interpretation or writing of the manuscript.