
Abstract
Background:
The law and literature about children’s consent generally assume that patients aged under-18 cannot consent until around 12 years, and cannot refuse recommended surgery. Children deemed pre-competent do not have automatic rights to information or to protection from unwanted interventions. However, the observed practitioners tend to inform young children s, respect their consent or refusal, and help them to “want” to have the surgery. Refusal of heart transplantation by 6-year-olds is accepted.
Research question:
What are possible reasons to explain the differences between theories and practices about the ages when children begin to be informed about elective heart surgery, and when their consent or refusal begins to be respected?
Research design, participants and context:
Research methods included reviews of related healthcare, law and ethics literature; observations and conversations with staff and families in two London hospitals; audio-recorded semi-structured interviews with a purposive sample of 45 healthcare professionals and related experts; interviews and a survey with parents and children aged 6- to 15-years having elective surgery (not reported in this paper); meetings with an interdisciplinary advisory group; thematic analysis of qualitative data and co-authorship of papers with participants.
Ethical considerations:
Approval was granted by four research ethics committees/authorities. All interviewees gave their informed written consent.
Findings:
Interviewees explained their views and experiences about children’s ages of competence to understand and consent or refuse, analysed by their differing emphases on informed, signified or voluntary consent.
Discussion:
Differing views about children’s competence to understand and consent are associated with emphases on consent as an intellectual, practical and/or emotional process.
Introduction
Standards in the law and literature concerning children’s consent or refusal, summarized in the background section, differ from actual respectful practices in two London paediatric cardiology departments. After reporting the methods, this paper explores possible reasons for the contrast in the approaches to children’s consent. Thematic analysis of professionals’ interviews shows attention not mainly to informed consent, as in the literature, but also to signified and voluntary consent. The findings sections are divided between these three aspects of consent, which are then discussed. The conclusion considers their significance for healthcare practice, research and teaching.
Background
There are clear differences between theories in the law and mainstream literature about children’s consent versus recently observed practices in two paediatric cardiac departments. Practitioners were observed to spend much time and effort on informing young children, responding to their resistance and refusal, and helping them to understand and ‘want’ the cardiac surgery. However, systematic reviews report that ‘shared decision-making is rarely implemented in paediatric practice’. 1 Some reviews of consent to children’s surgery report only parents’ experiences and exclude children. 2 The many meanings and methods of assent remain uncertain, and children’s dissent is largely ignored. 3 It is widely assumed that legal minors cannot consent until they are around 12 years, and may not refuse recommended major treatment. 4 Children who are deemed non-competent lack the automatic legal rights that protect most adult patients: to be informed and listened to, and not to be deceived or coerced. In 1998, a judge ordered that a 15 -year-old should be given a heart transplant against her will, showing that ‘the legal and ethical position on young people and consent is complicated and confused’. 5
In contrast to assent, consent includes the choice to refuse, and has been clearly defined for decades. 6 Though developed for medical research, the definitions of consent also apply to medical treatment and detailed definitions are considered in the Findings section. Numerous national and international professional healthcare guidelines emphasize the importance of consent as ‘essential’, though usually relying on parents’ consent. 7 Most of the literature review is in the findings section, in order to show how an original three versions of consent analysis of the literature produces new findings, and to compare closely the main views in the literature with those in the hospitals.
Research question
What are possible reasons to explain the wide differences between published theories and actual practices about the ages when children can begin to be informed about elective heart surgery, and when their consent or refusal begins to be respected?
Research design, participants and research context
Research methods included reviews about children’s consent in the law, ethics and healthcare literature. During October 2019 to February 2020, there were ethnographic observations in two London paediatric cardiology departments in the wards, clinics and multidisciplinary meetings, and audio-recorded, semi-structured interviews, conducted with 45 healthcare professionals and related experts. 8 The purposive multidisciplinary sample was interviewed once for about an hour in private face-to-face sessions October 2019 to February 2020, and then by phone between March 2020 and April 2021 Semi-structured question guides, based on previous research, 9 asked about interviewees’ views and experiences concerning children’s heart surgery. The main questions considered in this paper concern the ages when interviewees consider children should begin to be informed about heart surgery, and when their consent or refusal should begin to be respected.
Encrypted interview recordings were professionally transcribed and then anonymized. Research with children aged 6- to 15 years having elective heart surgery and their parents was to be central to the project, but was much reduced because of COVID-19 when elective surgery was cancelled. This work is reported elsewhere. There were meetings with the interdisciplinary advisory group. Thematic data analysis was informed by the sociology of childhood studies where children are viewed as social agents with rights, in contrast to age-based developmental psychology. 10 Grounded theory informed the repeated reading of the literature and research notes and transcripts to discover themes 11 and attend to authors′ and interviewees′ emphasis on, or neglect of, three differing aspects of consent.
Ethical considerations
Approval was granted by NHS HRA Research Ethics Committee (19/LO/0073), Hampstead Research Ethics Committee (ID 248332), and the Institute of Education University College London Research Ethics Committee (REC1188) in February 2019, and by the HRA-Confidentiality Advisory Group (19/CAG/0148) in September 2019. All interviewees gave their informed written consent and are anonymized. No patients were involved for this paper.
Findings
During data analysis, gradually, different emphases on the three traditional major meanings of consent were noted. The consent law and literature highlight informed consent, central to law and the Declaration of Helsinki 12 : detailed intellectual understanding of the nature and purpose of the intervention, risks, benefits and alternatives. There is brief attention to signified consent when a legally authorized person signs the consent form. However, practitioners were very involved with practical signified consent, in children’s active cooperation or resistance. This is hardly mentioned in the literature, which also says little on voluntary consent in practitioner-patient relationships. Voluntary consent is essential and involves patients’ emotions of willing agreement and not feeling coerced, 8 when trust and courage overcome fear and doubt. The findings are shown grouped into these three aspects of consent.
Specialties of the 45 interviewees: members of the paediatric cardiac teams and related experts.
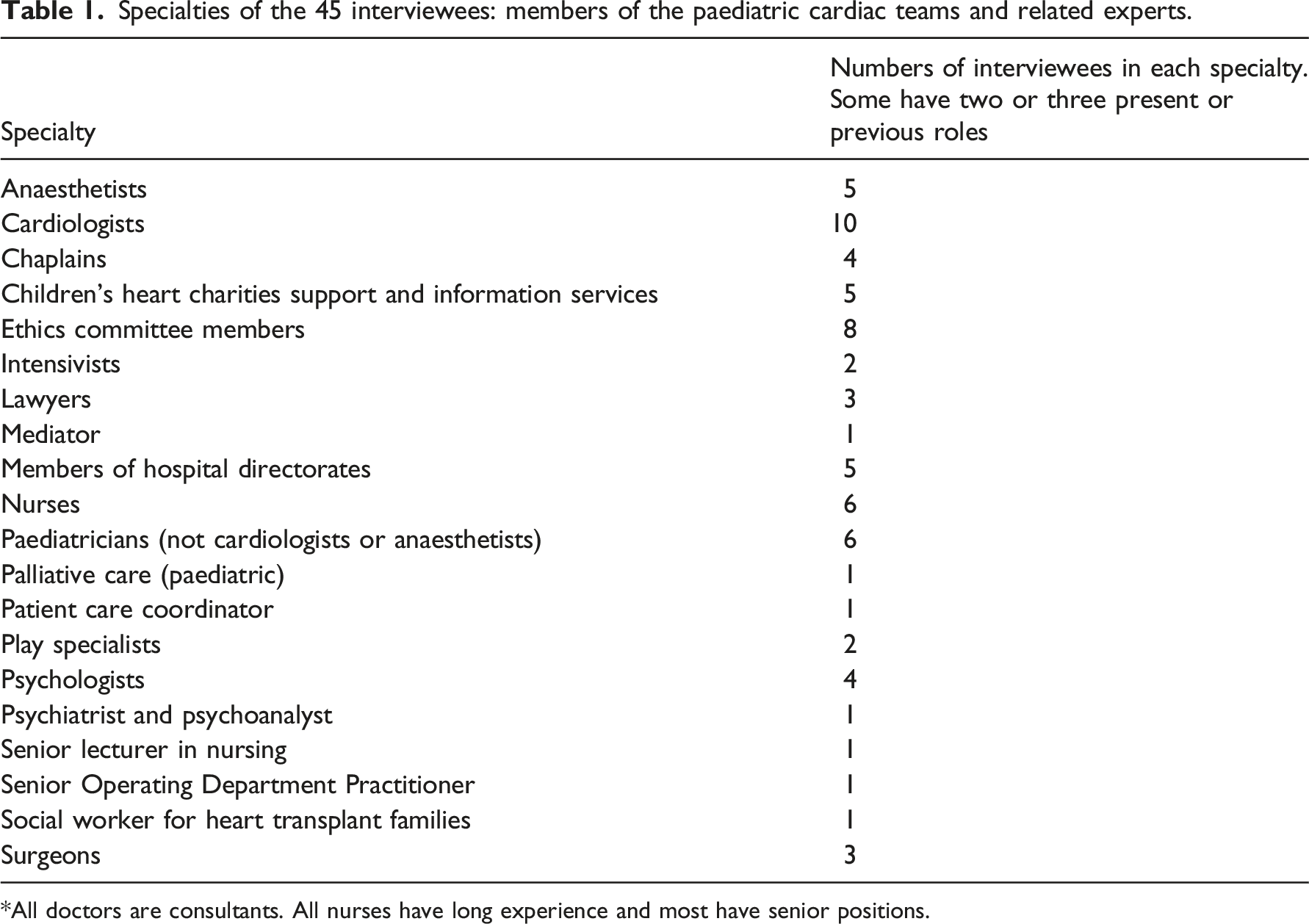
*All doctors are consultants. All nurses have long experience and most have senior positions.
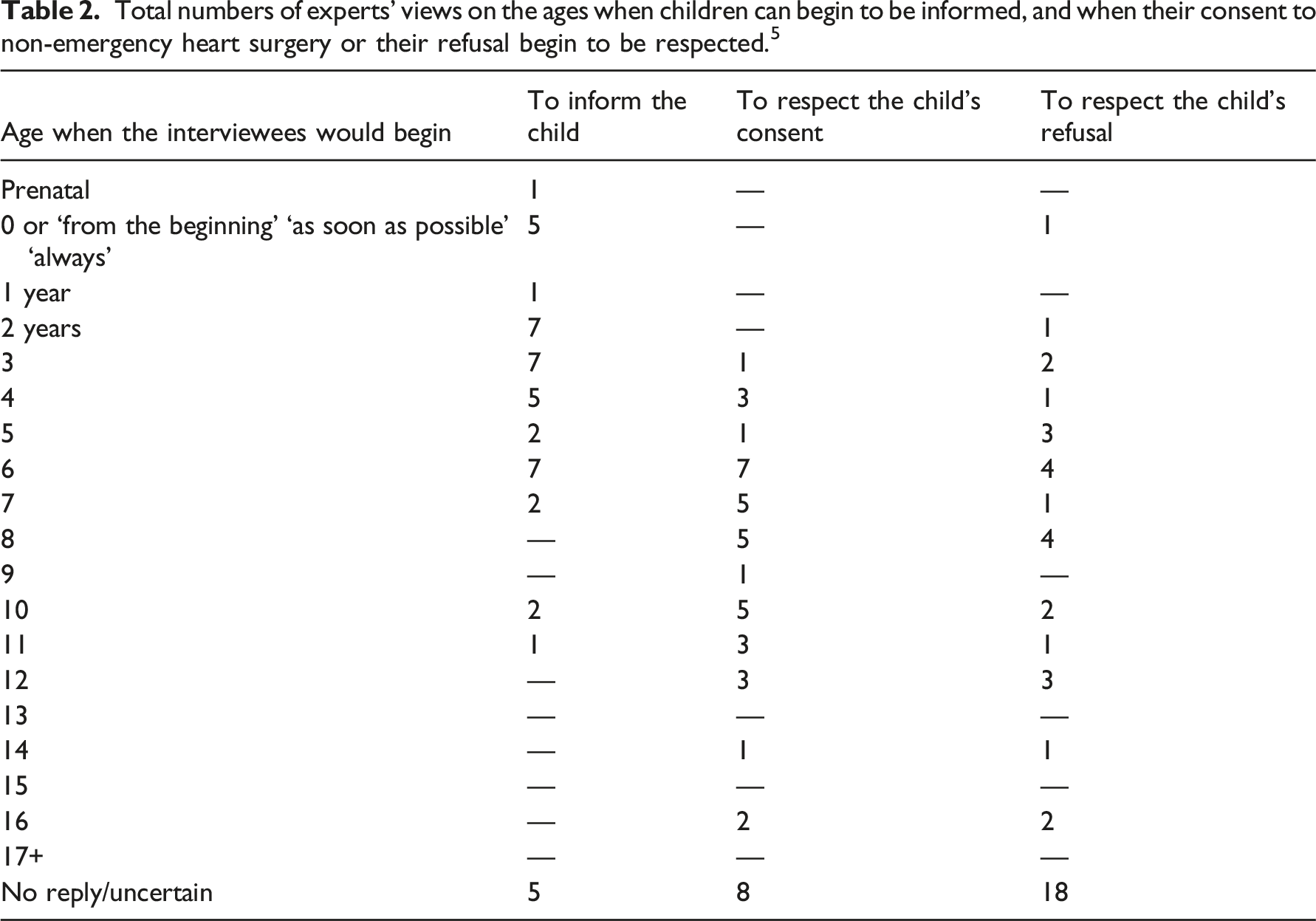
Total numbers of experts’ views on the ages when children can begin to be informed, and when their consent to non-emergency heart surgery or their refusal begin to be respected. 5
Intellectual informed consent
The literature on consent is dominated by three authorities, which all set high ages for when legal minors can begin to give informed consent to medical treatment or research. There is the law, based on historical precedent,4,13 bioethics that draws on patriarchal philosophy and supports adult-centric reason and autonomy, 14 and pharmaceutical companies running large trials that need rapid, legally valid consent systems.15,16 In healthcare and research, detailed informed consent has become a contract to defend against costly litigation, 17 so that information should be as detailed as possible. 18 The few published papers on children’s consent to treatment concentrate on those aged 12 years upwards, deemed in the (formerly British) Commonwealth Gillick competent, 19 and in the US mature minors. 20 Some lawyers are critical that ‘adolescent autonomy is little more than a myth’ and state that ‘no minor has a right to refuse treatment’. 4 High standards of informed consent promote respect for adult patients and for parents, but leave children deemed pre-competent with no right to be informed, or involved in decisions. For children, consent is frequently replaced by the US concept of assent, which ‘is ill thought-out, confused and harmful’. 21 Assent contradicts English Gillick law that children aged under-16 may consent, with no specified lower age, and assent need not be at all informed, but may be taken as agreement when children feel unable to refuse. 22 Enforced treatment is then tacitly endorsed, 23 despite official guidance to avoid coercion. 24
Patients’ competence to consent is assessed by a) legal status, b) outcome (does the assessor consider the person’s decision is reasonable?) or c) function (even if the assessor disagrees with the patient’s decision does the reasoning that explains and justifies the decision seem valid?). 25 Most adults are assessed as competent by status alone, whereas most children fail that test. They are then assessed for their reasoning (outcome, function) to high standards that many adults would fail, when Gillick competence involves ‘sufficient understanding and intelligence to understand fully what is proposed’.
The consent literature raises questions about informed consent: When can young children begin to understand their heart surgery? What do they need to know if their consent can be informed?
Interviewees’ views about intellectual informed consent.
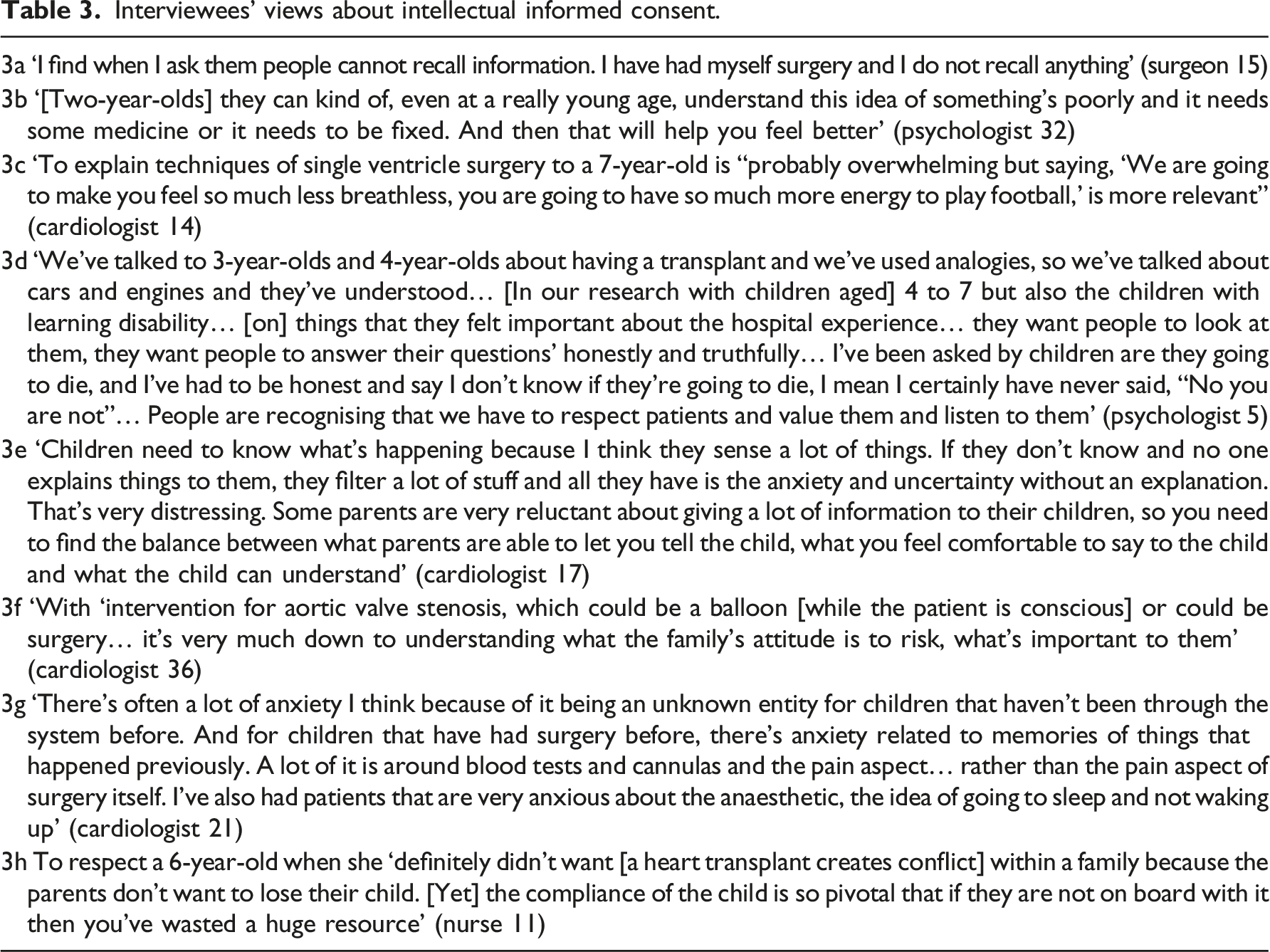
Consent cannot involve understanding ‘fully’, the Gillick term, when it is given to partly unpredictable risks and futures. In paediatric cardiology, new knowledge and ‘far reaching’ change constantly emerge from research, experience and experiment. 26 Doctors readily accept that their own knowledge is partial and fallible. The phrase, ‘I don’t know’, echoes through the interviews. They can tell even adult patients only a fraction of their specialized information, and find that adults and children have limited recall (Table 3a). Acknowledging experts’ partial knowledge encourages respect for young children’s limited though sometimes profound knowledge gained from experiencing serious illness and treatment (Table 3b–3d).
Reasons given for informing children include that they want and need to know what will happen to them (Table 3e), 27 to correct misunderstandings and avoidable fears, and to understand that the purpose of surgery is well-intentioned, to help them (Table 3f). Traditionally, adults assumed they knew children’s ‘best interests’ and must override the objections of foolish, ignorant, potentially self-harming children.28,29 Recent guidance, however, challenges these assumptions advising that children should be ‘be kept as fully informed as they wish, and as is possible… to have their views and wishes sought and taken into account as part of promoting their welfare in the widest sense’. 24 Interviewees repeatedly said that respecting children’s interests involves listening to their views about their interests and needs, to the extent of postponing non-urgent surgery to allow time to help children overcome their reasonable fears about risky painful interventions (Table 3g). At times the child’s choice is decisive, when there is a choice between surgery and an alternative intervention. With the scarcity of small hearts for transplantation, and if children still refuse after weeks of negotiation, donated hearts are reserved for informed, committed patients (Table 3h).
Those who cite high ages before minors can consent or refuse refer to informed consent as a legal contract, to the need for full details about the nature, purpose, procedures, risks, benefits and alternatives, and to the legal veto on minor’s refusal. Interviewees who cite lower ages tend to work more directly with young children informing them and, as far as possible with non-emergency treatment, respecting their consent or refusal. When preparing children for a heart transplant, during several in-patient days, clinical teams find that young children can have deep though not necessarily detailed understanding, that is respected as necessary and sufficient for consent or refusal.
Practical signified consent or refusal
Interviewees’ views about practical signified consent.
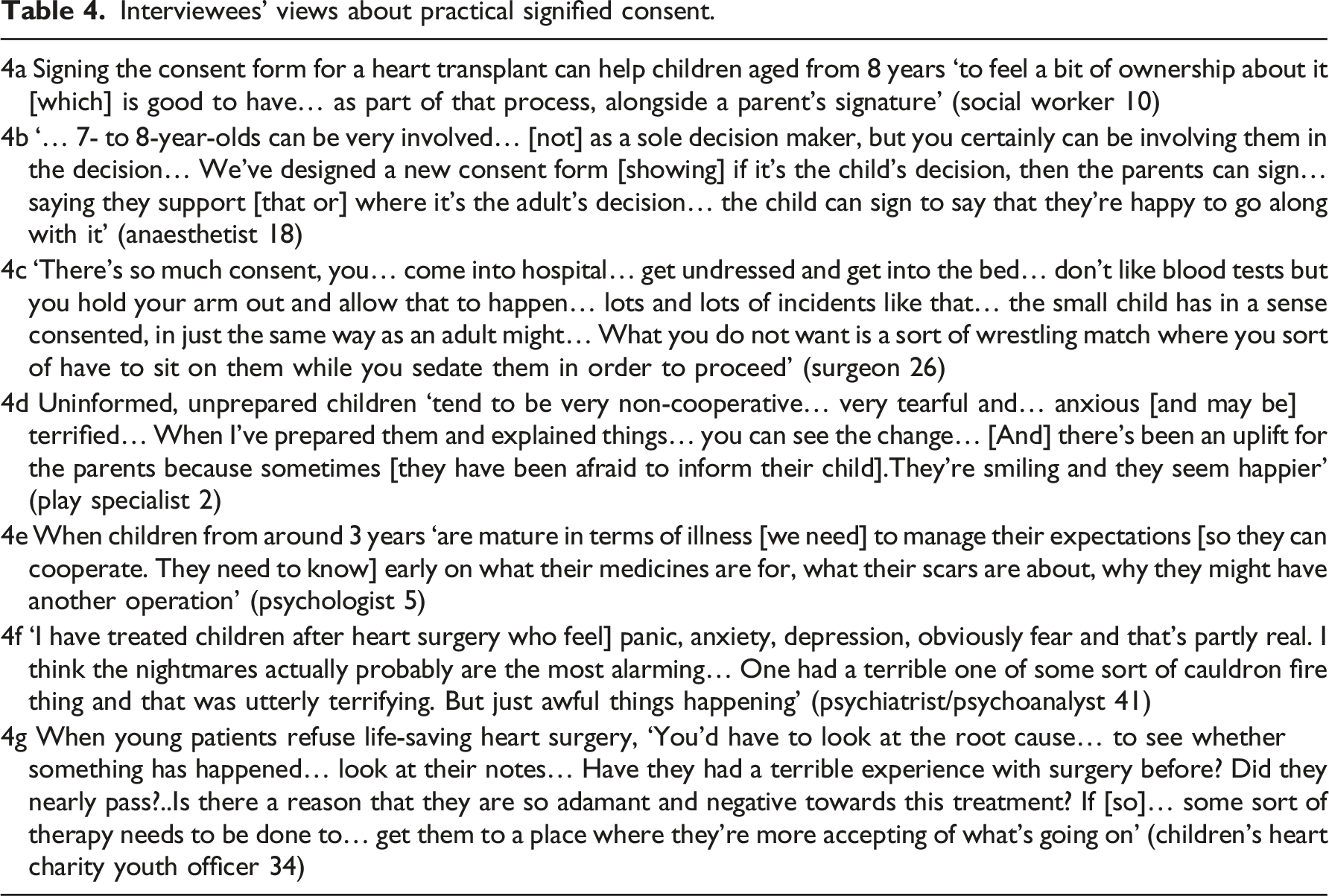
Resistance can express children’s need for more information and support. Interviewees reported that children ask more about procedures done while they are conscious, than about surgical techniques, so that they can understand and prepare for what they will experience. They can then signify their consent through informed cooperation (Table 4d, 4e). Practitioners often have to persuade protective parents to allow their child to be informed, and many described the dangers of overriding children’s resistance (Table 4f).
If children resist, interviewees advised taking time to calm them, to give more reassurance and information (Table 4g) combined as needed with some distraction, toys, books and videos to absorb the child, and some sedation before anaesthesia or lengthy procedures. Non-urgent surgery may be postponed, and nurses, play specialists and psychologists help the child to prepare to accept later surgery, assisted by imaginative programmes.30–32 Some practitioners advise replacing information with distraction techniques or medication to reduce pre-operative anxiety levels and distress. 33 However, our interviewees used distraction and sometimes pre-operative medication to supplement but not replace discussions, and to support children’s informed cooperation. As one of the interviewees (with colleagues) stated publicly: ‘We often see children who are terrified, and have clearly suffered significant psychological trauma, having previously been held down at induction of anaesthesia by teams who did not mean to cause harm, but were just trying to get a procedure done. Rebuilding lost trust is a long and difficult process’. 34
Negotiations with resisting children might seem to gently override children’s withholding of consent. Yet patients of all ages, who consent to the hoped-for benefits of surgery, may still fear the means towards achieving those ends: needles, incisions, scars, pain. Helping them to cope with distressing processes can respect their main decision. Lower ages of consent were cited by those closely involved with children’s practical signified consent.
Emotional voluntary consent
More relational concepts of children’s decision-making capacity have been advocated to increase practical respect for children, 35 and these practitioner-patient, adult-child relational concepts are developed in this section. A frequent phrase is ‘young patients must consent’ to heart surgery. Yet that denies how consent can only be voluntary, freely given. Valid consent has long been identified with the rational person who calmly rises above emotions. 17 Yet the Nuremberg Code emphasizes voluntary consent, feeling free not coerced. 8 Consent involves trust, hope and belief in the benefits. ‘Belief’ originally meant ‘hold dear’, ‘consent’ meant ‘feel with’, and confidence meant ‘with faith’, all grounded in emotions.
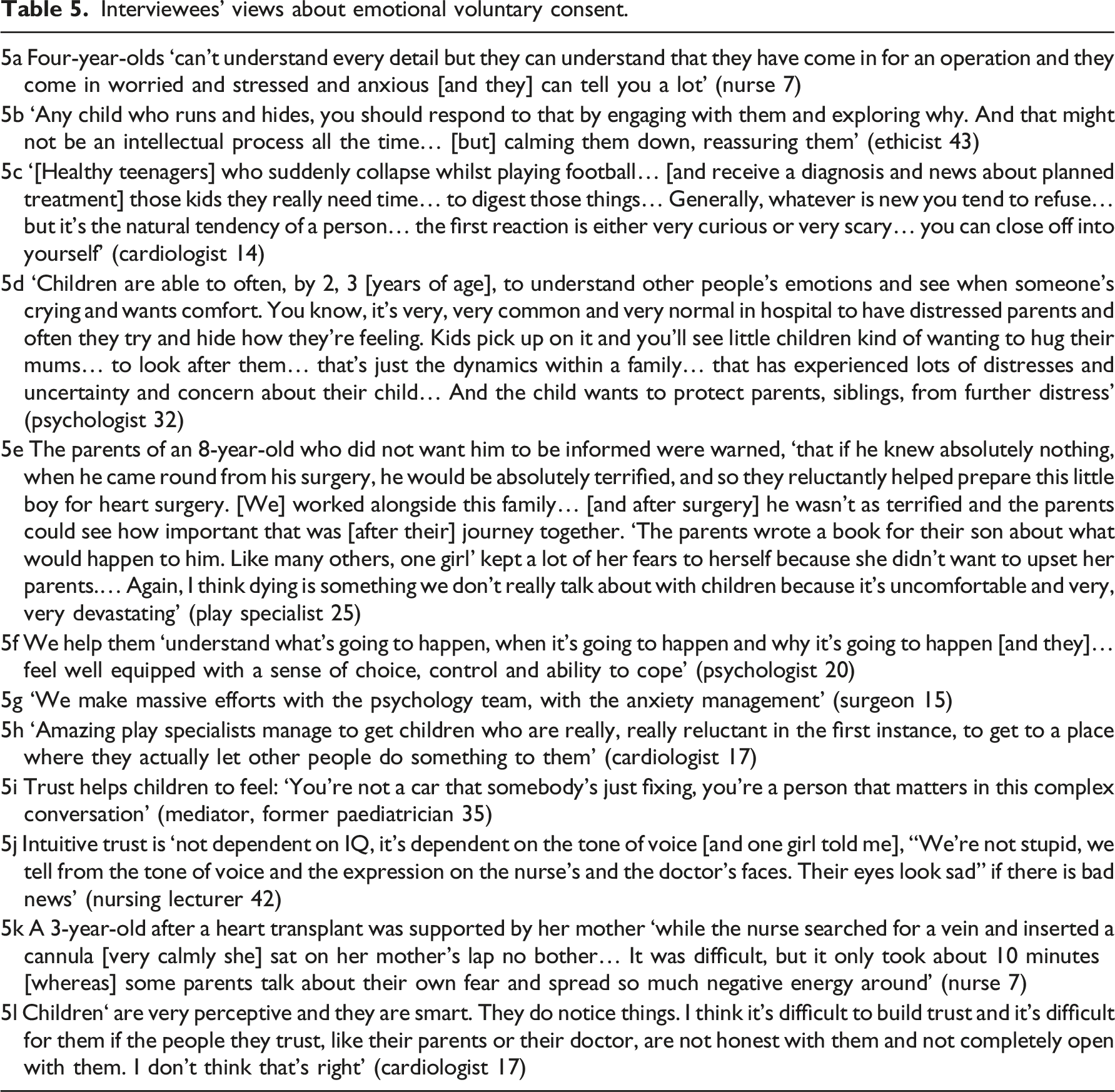
Interviewees’ views about emotional voluntary consent.
Discussion
Differing views about children’s competence to understand and consent are associated with differing emphases on consent as an intellectual or practical or emotional process.
Beyond words on a form, signified consent exists through practitioner-patient interactions and voluntary consent exists within mutually respectful trusting relationships. They are as integral to consent as being informed. Actively involving children in signified and voluntary consent enabled practitioners to recognize their consent more fully. Yet the signified and voluntary elements are largely missing from the consent literature, though without them the nature and purpose of consent can become distorted. There may be undue emphasis on intellectual details that do not significantly alter the patient’s hope for the benefits of heart surgery or their courage to undertake the pain and risk. Consent may be diverted into becoming an abstraction instead of a relationship, serving the legal and financial protection of institutions rather than patients’ needs. Recognition that everyone’s knowledge about surgery is partial and fallible, and partly emotional as well as intellectual, helps to explain respect for children’s consent, when they basically apprehend risk and hoped-for benefit.
Children with congenital heart disease are unusual in that they tend to be highly aware and informed by years of illness and treatment. They depend on lifelong cardiac care. Relationships of informed trust in their healthcare professionals therefore matter far more to them, than they do to children having only brief treatment. Partially informed consent can be deceptive, misleading and can fail in the primary purpose of consent, to protect patients from needless dangers. Yet seemingly fully informed adult consent cannot guarantee full protection from misinformation or misunderstanding. The children in this research had the protections of their parents’ consent, and the weekly clinical team meetings concerned with evidence-based decisions about the best use of limited resources, as well as by both hospitals’ public records of heart surgery outcomes.
The study is limited to two leading hospitals and further research is needed in other centres and clinical specialties to see how these finding are, or could be, more generally applied. Topics briefly referred to in this paper, and missing topics such as assessing competence, are considered in other reports about this research.
Conclusion
Younger children’s consent to heart surgery tends to be seen in the law and literature as neither necessary nor feasible. However, practitioners reported in research interviews that, more than assent, they respect children’s informed, signified and voluntary consent, three activities summed up by a surgeon 25 : ‘I don’t mean that the child should make the final decision and sign the form, but just make sure that the child understands and knows that this is best, and is willing to then go through the surgery and follow instructions afterwards’. This standard, from when children begin to be able and willing to understand and be involved in decisions, is seen by most interviewees as part of effective humane care. Because nurses play such a vital part in children’s physical care and relationships, they are especially aware of all three elements of consent.
The topic is important because, although heart surgery is unusual in being so complex and life-threatening, if young children can be informed and involved in these high-risk decisions, as many can, they suggest that children having many other less dangerous kinds of surgery can also be involved. Internationally, many children in middle-income and low-income countries cannot access much-needed surgical care. Yet, this paper is potentially relevant to all children receiving any kind of healthcare. It is about how healthcare professionals may inform and involve children far more than is often recognized, and encourage parents not only to represent their child, but also to involve their child as much as possible. Paediatric nurses play a vital part in children’s practitioner-patient relationships and physical care and therefore in all three elements of consent. Healthcare leadership, everyday practice, research and education need to be more informed by empirical research about the best current clinical practice, reported in this paper.
Footnotes
What is original
This empirical study of hospital practices found far more humane standards and actual respect for children’s consent than is generally assumed and recommended in the law, ethics and healthcare literature. The signified and voluntary elements of consent are too often neglected, but they are as important as the informed element. Greater concern for signified and voluntary consent promotes greater understanding of and respect for children’s consent.
What impact is the work likely to have on care practice,leadership,research and/or education?
Leadership, research and education need to be more informed by empirical research about the best current clinical practice, reported in this paper. Nurses need to challenge inhumane standards that are generally endorsed in current mainstream literature.
Author’s Note
Twitter
“*New paper* by PA
Acknowledgments
We are very grateful to all the hospital staff and related experts, including Nicola Gregg (psychologist GSTT), and to the families who participated in the research, also to the British Heart Foundation for funding.
Author Contributions
PA and KS conceptualised the research project and setting and methods, and acquired funding.
PA, RM and KS administered the project, applied for research access to the hospitals and interviewees and conducted literature reviews.
PA and RM conducted observations and interviews.
PA thematically analysed the qualitative data and wrote and revised the paper.
RM and KS verified the tables.
HB-R, JB, ND, JH, MJ, SJ, AK, RK, LK, JT, TV, HW, and JW contributed intellectual content.
All authors have critically read and approved the manuscript and accept responsibility for the decision to submit for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The British Heart Foundation (Project Grant no. PG/18/22/33604) had no role in the study design, data collection, analysis or interpretation, or writing of the report. PA, KS, and RM worked on the funded research.