
Abstract
Background:
The Voluntary Assisted Dying Act 2017 passed into law in Victoria, Australia, on the 29 November 2017. Internationally, nurses have been shown to be intimately involved in patient care throughout the voluntary assisted dying process. However, there is a paucity of research exploring Australian nurses’ perspectives on voluntary assisted dying and, in particular, how Victorian nurses anticipate the implementation of this ethically controversial legislation will impact their professional lives.
Objectives:
To explore Victorian nurses’ expectations of the ethical and practical impacts the voluntary assisted dying legislation will have on their professional lives.
Research design:
This qualitative study analysed nurses’ free text responses collected as part of a larger mixed methods online survey investigating staff views on the Voluntary Assisted Dying Act. Data were collected during the period between the passing of the voluntary assisted dying legislation and the start date and were analysed using inductive content analysis.
Participants and research context:
Free text survey responses were analysed from 1873 nurses employed across seven Victorian health services located in both metropolitan and regional areas of the state.
Ethical considerations:
The study obtained research ethics approval and all participants were informed of the voluntary and anonymous nature of their participation.
Findings:
This study identified three broad areas of Victorian nurses’ professional lives that they expected to be impacted by the implementation of voluntary assisted dying: professional identity, career development and workplace relationships.
Conclusion:
Participants anticipate diverse and nursing-specific impacts of the implementation of voluntary assisted dying in Victoria. Their insights can inform health services in jurisdictions considering or already implementing voluntary assisted dying, to develop policies, procedures and staff training programmes that safeguard the well-being and legal rights of their nursing staff.
Introduction
There is an increasing global momentum around legalising voluntary assisted dying (VAD). 1 At the time of writing, some form of voluntary assisted dying was permitted in Belgium, the Netherlands, Switzerland, Luxembourg, Colombia and Canada, and in eight states in the United States. 2 New Zealand’s recent referendum means that voluntary assisted dying will become legal, and other countries are actively debating the legalisation of voluntary assisted dying. 3 In Australia, the Voluntary Assisted Dying Act 2017 (Victoria) passed into law in the state of Victoria on 29 November 2017 and came into effect on 19 June 2019. 4 This legislation made Victoria the first Australian jurisdiction to pass voluntary assisted dying legislation since the Rights of the Terminally Ill Act 1995 (Northern Territory) was swiftly overturned in 1997. The state of Western Australia has since followed, passing similar voluntary assisted dying legislation in December 2019, with a planned start date in 2021. 5 The state of Queensland is also currently drafting its own legislation. 6
Features of the Victorian voluntary assisted dying legislation are summarised in Box 1. In Victoria, nurses cannot assess patients’ eligibility for voluntary assisted dying, nor prescribe the medication. Despite this, evidence from other countries where voluntary assisted dying is legal suggests that nurses are involved throughout the voluntary assisted dying process due to the nurse–patient relationship. Nurses are intensely involved in the care of terminally ill patients and their families. 8 It is, therefore, unsurprising that a nurse is often the first person to receive a request for voluntary assisted dying.9,10 Following a patient’s request, nurses report engaging in an interpretative dialogue with the patient to gain a better understanding of the underlying reasons for their request as well as passing on this information to medical practitioners and other members of the treating team. 11 The provision of ongoing psychosocial support to the patient and family is also central to nurses’ role in situations where patients request voluntary assisted dying.9,11
Key features of the Voluntary Assisted Dying Act 2017 (Victoria). 7
To access voluntary assisted dying, a patient must
be an adult Australian citizen or permanent resident and reside in Victoria,
have decision-making capacity in relation to voluntary assisted dying,
have a medical condition that is incurable, advanced, and progressive,
have a prognosis of no longer than 6 months (or 12 months in the case of neurodegenerative disease), and
be experiencing suffering caused by the relevant condition, that cannot be relieved in a manner that the patient deems tolerable.
The patient needs to make at least three formal requests for voluntary assisted dying: a minimum of two verbal and one written.
For eligible patients, the medical practitioner will write a prescription for a lethal medication that the patient can ingest at a time of their choosing. For those patients who are unable to self-administer, the voluntary assisted dying medication can be administered by the physician.
The patient must be assessed by two medical practitioners. The medical practitioners must be either a vocationally registered general practitioner or a specialist, and have completed the approved voluntary assisted dying assessment training. At least one must have held their specialist fellowship or be a vocationally registered general practitioner for a minimum of 5 years. At least one must have expertise in the relevant condition.
Health practitioners can conscientiously object to participating in various processes involved in providing voluntary assisted dying.
Health practitioners must not initiate discussion about voluntary assisted dying with a patient, and must report colleagues whom they reasonably believe have initiated such discussions.
Existing research shows that legalising voluntary assisted dying creates challenges in nurses’ practice. A 2018 review of literature exploring nurses’ experiences of legalised voluntary assisted dying identified three common challenges: role ambiguity, lack of interprofessional collaboration and conscientious objection. 12 In addition, nurses have expressed fears of being judged, discriminated against and stigmatised by their peers on the basis of their stances on voluntary assisted dying. 13 More recent studies conducted in the Canadian context also highlight more positive impacts of the legislation on nurses’ professional lives. Beuthin and colleagues demonstrated that for many nurses, voluntary assisted dying was perceived as an extension of the nursing profession. These nurses viewed the legislation as reinforcing their duties to provide holistic care and advocate for their patients’ choices. 13 Some nurses’ experiences of providing end-of-life care have been positively transformed by participating in voluntary assisted dying, describing feelings of satisfaction, gratitude, honour and privilege in being involved.13,14 Finally, residual discomfort remains for some nurses who raise concerns about potential future impacts of the legislation which are as yet unknown. These include concerns about the practice becoming routinised and nurses becoming desensitised over time as well as the yet unknown longer-term emotional impacts of nurses participating in voluntary assisted dying. 14
In the Australian context, there is very little research capturing the nursing perspective on voluntary assisted dying. Of the research published in the past 20 years, only two studies explore Australian nurses’ attitudes towards voluntary assisted dying.15,16 While recent work in Victoria has begun exploring the challenges of voluntary assisted dying anticipated by a range of Victorian clinical staff,7,17,18 there has been no published Australian research investigating the expected impact of voluntary assisted dying legislation on nurses specifically. Given the recent legalisation of voluntary assisted dying in Victoria and Western Australia and moves towards legislative change in other Australian states and similar health systems worldwide, this is a key gap in knowledge.
This study, therefore, sought to explore Victorian nurses’ expectations of the impact that this significant and ethically controversial change in health law will have on their professional lives.
Methods
Design
This qualitative study adopted a symbolic interactionist framework. i In positing that humans’ perspectives on particular matters are socially constructed, this sociological theory provided a useful explanatory model for gaining a deeper understanding of the multiple, subjective expectations of individual nurses towards the impacts that implementing voluntary assisted dying will have on their professional lives.
The study analysed free text data collected as part of a larger mixed methods study. The larger study used an anonymous online survey to investigate views of voluntary assisted dying across medical, nursing and allied health staff employed at seven Victorian health services. Participants responded to quantitative and qualitative questions. The present study specifically analysed the qualitative data from the 1873 nurse respondents. Other papers report quantitative findings on willingness to participate in voluntary assisted dying across the whole medical, nursing and allied health sample (unpublished data), and qualitative results from other clinical groupings.7,20
Participants
Purposive sampling was used. Participants were included in this study if they indicated their role as ‘nurse’ in the quantitative section of the survey, and they provided a written response to at least one of the four free text questions in the survey.
A total of 2936 nurses completed the survey, and 1873 of these provided written responses to at least one of the four free text questions and were therefore included in this study. The breakdown of study participants by health service is described in Table 1. Diverse health services were included in the study: five in metropolitan Melbourne, one in outer suburban Melbourne and one in a regional area of the state.
Study sample.
Data collection
Participants were recruited using two strategies: emails to clinical staff lists via the employing health services and a link to the online survey on the staff intranet. The online survey was available for 3 weeks at each health service, with data collected between November 2018 and January 2019, prior to the June 2019 start date for the legislation.
The survey questions were developed via review of relevant literature and expert discussion within the multidisciplinary research team working on the larger mixed methods survey project. The questions were tested with the VAD working group at one of the health services involved.
Nurses’ written responses to the following four free text questions were included in this analysis: Overall, what is your position on Victoria’s recent legalisation of voluntary assisted dying? Is there anything else you would like to add about your reasons for being willing or unwilling to participate in voluntary assisted dying? What challenges (if any) do you envisage voluntary assisted dying will create in your work? Do you have any other comments in relation to the issues raised in this survey?
Data analysis
Written responses to the four free text survey questions were analysed using qualitative inductive content analysis. 21 JS coded the dataset and developed a coding framework in consultation with BP and RM. All data were coded into categories of meaning and then grouped into smaller numbers of higher order headings until the final themes emerged. 21 The aim of this process is to transition from a specific to a more general account of the phenomenon, in this case nurses’ expectations of VAD’s impact on their practice. 21 Saturation was reached at the point at which no new codes were generated. The qualitative data analysis software NVivo Version 12 was utilised.
Ethics
Ethical approval for the larger study was granted by the Austin Health Human Research Ethics Committee (reference number HREC 45754 Austin 2018). Participants were provided with information about the study on the first page of the online survey and advised that proceeding to answer the survey questions would be taken as an indication of their consent to participate in the study. Within the survey, completing the textbox questions was not required to progress.
Findings
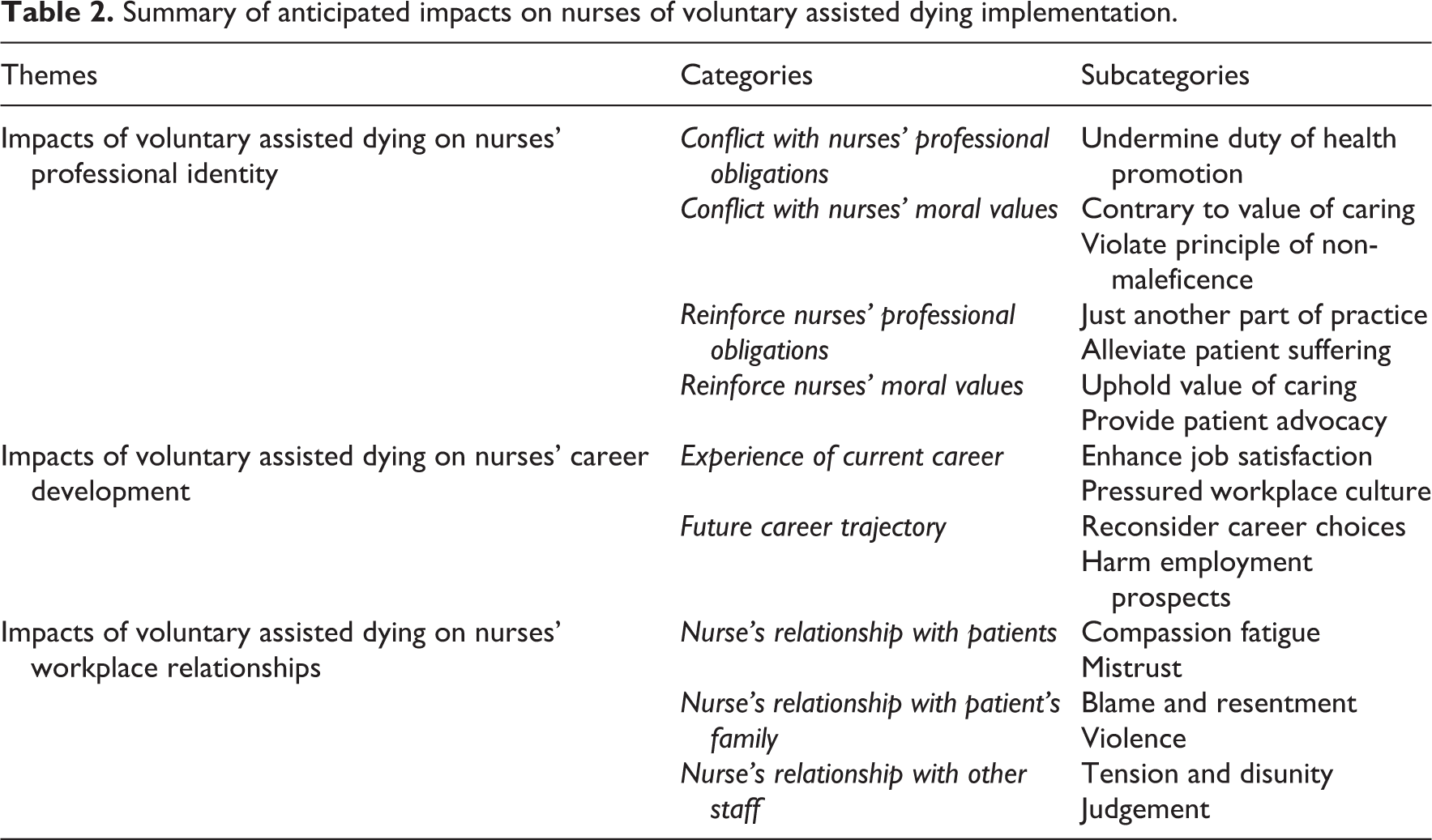
Inductive content analysis identified three broad areas of nurses’ professional lives which they expected to be impacted by the implementation of voluntary assisted dying: moral integrity and professional identity, career development and workplace relationships (Table 2).
Summary of anticipated impacts on nurses of voluntary assisted dying implementation.
Impacts of voluntary assisted dying on nurses’ professional identity
Nurses in this study anticipated that the implementation of voluntary assisted dying would impact upon their professional identity. This impact was expected to manifest as either congruence or incongruence with the professional obligations or moral values inherent to the professional identity of nurses.
Here, professional identity in nursing is conceptualised as a sense of oneself as an individual who thinks, feels and acts like a nurse. 22 Two key attributes forming this self-conception are doing by adhering to the professional obligations of nursing and being by acting in line with the moral values of the profession. 22 The professional obligations of nurses include the protection, promotion and optimisation of health; the prevention of illness and injury; and alleviation of suffering and advocacy in the care of individual patients and their families. 23 Regarding nursing ethics, the major moral values include advocacy, accountability, collaboration and caring. 24
Conflict with nurses’ professional obligations
Nurses in this study expressed their apprehensions regarding the introduction of voluntary assisted dying, predicting that it would negatively impact their nursing identity: I think this is asking health professionals to radically change their roles. I am very uncomfortable about this. Every day, I am assisting patient to live, regain their health and leave the hospital. I also help patients during their last days, when illness becomes too much. I have a great love for this part of my job, it is a beautiful thing to make my patients comfortable and happy in their final hours. I work hard every day to maintain my patient’s safety and wellbeing and the act of assisting them in suicide rocks me to my core.
Conflict with nurses’ moral values
Other nurses anticipated that their professional identity would be negatively impacted due to voluntary assisted dying being in conflict with their moral values as nurses. As a registered nurse this act goes against everything I believe in. The law needs to be reversed. We are not in healthcare to assist people to die. We are here as nurses to care for these patients. It is part of a nurses’ duty of care and nurses’ Hippocratic oath to do no harm to patients.
Reinforce nurses’ professional obligations
In contrast, other nurses regarded voluntary assisted dying as being strongly aligned with both the professional obligations and ethical values underpinning the nursing profession. As such, these nurses anticipated that this new practice would reinforce their nursing identity. Some nurses expressed the opinion that voluntary assisted dying would become just another part of their practice in the provision of patient care generally and end-of-life care specifically: It’s just another part of caring for an individual. No different to providing life-saving care. In my role I already discuss advanced care planning, palliation etc. and I just see voluntary assisted dying as an extension to that. I don’t believe they should not have to participate, as it should just be another part of nursing care. There is no point lying to a person, providing them unnecessary and often painful treatments to facilitate an extra few weeks of life. Nurse will be happy to assist patient[s] through providing a comfortable and supported death.
Reinforces nurses’ moral values
These nurses described several ways in which voluntary assisted dying upholds their moral values as nurses. Some felt voluntary assisted dying allowed them to uphold the value of caring by giving them the opportunity to provide compassionate care to their patients: Nurses do not care about prolonging life, we care about caring for people. Making sure people are comfortable, supported and educate[d] on their health. Patient centered care – to me this says everything. I believe as a nurse that if a [patient] is suffering and meets the criteria, it is our role to support and advocate for the [patient] if this is an option they are wanting to explore or utilize.
Impact of voluntary assisted dying on nurses’ career development
Implementation of voluntary assisted dying was expected to have practical impacts on nurses’ current careers, as well as how they navigate their future career trajectories.
Experience of current career
Some nurses who support voluntary assisted dying expressed a potential for enhanced job satisfaction as a result of being able to better carry out their patients’ final wishes: I feel it will make work more meaningful as patients’ wishes are being carried out. I am both honoured and humbled as a practitioner to be able to provide this much needed service to the Victorian community in 2019.
Workplace pressure
Other nurses predicted that the introduction of voluntary assisted dying may negatively impact some nurses’ experiences of their current career by fostering a workplace culture that places pressure on staff members who conscientiously object to voluntary assisted dying. Despite the Victorian voluntary assisted dying legislation clearly stipulating the right for staff to conscientiously object, these nurses anticipated that pressure to participate would likely arise. They predicted a workplace culture would develop that places a social expectation, rather than a legal obligation, on staff to participate in voluntary assisted dying. That culture would emphasise being a ‘team player’ and maintaining workplace flow: I know we don’t have to participate, but it can be difficult to say no in a busy hospital environment, where staff are time-poor and you don’t want to let your colleagues down or add to their work-load. ‘Silent’ pressure to do it despite it being against my values just to be a ‘team player’. A culture developing of non-involvement as it would be seen as opposed to professional values. To push against a healthcare culture is very detrimental to an individual healthcare worker.
Future career trajectory
Of the nurses who objected to voluntary assisted dying, some anticipated its imminent implementation in their workplace would impact their future career decision-making. Some stated that the implementation of voluntary assisted dying would cause them to reconsider the areas of nursing practice that they will pursue in the future: I think the introduction of this legislation will force me to think seriously about what areas of nursing I continue to work in. I strongly disagree with this and feel that I would psychologically be impacted for life if I had to even deal with the situation of a patient coming to me and requesting voluntary assisted dying. I don’t know what I would, to the point that I will not put myself in this situation and have actively started to apply for jobs in other areas with the aim of leaving nursing. I do not want my career negatively impacted also, due to my conscience stance on VAD.
Impacts of voluntary assisted dying on nurses’ workplace relationships
Nurses in this study anticipated that the implementation of voluntary assisted dying would impact upon three of their workplace relationships: with patients, with patients’ families and with other staff members.
Nurse’s relationships with patients
Some nurses raised their concerns that voluntary assisted dying would disturb the normal nurse–patient relationship: I think the VAD act will damage the therapeutic relationship between the clinician and the patient. Disturbs the normal patient-nurse relationship. I am concerned that it will create a relationship that lacks emotional connection and compassion. …feel uneasy about participating due to fear of compassion burnout… Misperception of being treated like [an] angel of death. Complete loss of trust of any patient who fits the criteria for VAD. They may well think ‘am I [nurse] one of “those” health professionals who gives patients like me lethal medication’.
Nurse’s relationships with patient’s family
Many nurses identified their interactions with family members of patients who had requested voluntary assisted dying as presenting possible challenges in their professional lives.
The most commonly described scenario of concern was where a patient’s family either did not understand or explicitly disagreed with a patient’s wish to use voluntary assisted dying. Due to voluntary assisted dying being an extremely emotional and sensitive issue, nurses anticipated that conflict among family members will likely arise if not everyone is in agreement with the patient’s decision. Being on the frontline, nurses expected that they would likely be the ones left to deal with these complex family dynamics: Family challenges and difficulty getting family to agree with the patient. This may cause family tension and drama which can often be put back on the nursing staff. Blame and resentment to health practitioners from family who are not supportive of their family member’s decision to participate. At times in my job I already receive abuse regarding the administration of medication to patients during end of life care. If medical staff deem a patient fit to make decisions about their uptake of voluntary assisted dying and the family disagree with the patient’s capacity I am concerned about aggression and family anger towards staff. I already feel threatened and intimidated at times when family are not accepting that their relative is dying and I need to administer medication – I can only imagine what legalizing voluntary assisted dying will do when families are not all on board with the decision made by the patient.
Nurse’s relationships with other staff
Many nurses in the study expected the implementation of voluntary assisted dying to negatively impact upon their workplace relationships with other staff members who possess divergent ethical views on the matter, both within nursing staff and with other members of the wider healthcare team. Two commonly used words to describe the expected negative sentiment felt between colleagues with opposing views were ‘tension’ and ‘friction’: I imagine that the difference of opinions between colleagues about VAD will create tension making it sometimes difficult to work together. I believe there will be a big divide amongst staff for those who agree with the new legislation and those who don’t. It will polarize us. I fully anticipate a degree of disdain and contempt for nurses that do not follow the generally accepted thought process of VAD – how could it be otherwise when people are discriminated against for not agreeing with any position other than that which is politically and now socially accepted and promoted as the norm. There will be staff who feel they cannot participate, and I am worried that they may feel animosity towards me for participating.
Discussion
This is the first study specifically exploring Victorian nurses’ expectations about what impact voluntary assisted dying legislation will have on their professional lives. Victorian nurses in this study identified three broad areas of potential impact: their professional identity, career development and workplace relationships. These areas offer important insights for Victorian health services and health services in other jurisdictions considering or already implementing voluntary assisted dying. Attending to nurses’ concerns about professional identity, career and relationships will be crucial to the design of voluntary assisted dying implementation policies, procedures and staff education resources that aim to ensure the physical safety and uphold the legal rights of hospitals’ largest clinician group.
There was a clear division in opinions regarding the expected impact that voluntary assisted dying will, or will not, have on the professional identity of nurses. This divergence was borne out of differences in how nurses in this study viewed voluntary assisted dying in terms of its level of alignment with the professional obligations and moral values important to the identity of nurses. These findings are consistent with existing literature.26,27 Previous empirical studies have demonstrated that nurses who envisage voluntary assisted dying as reinforcing their professional identity perceive the practice as aligning with their professional obligation to alleviate suffering28–30 and moral duty to uphold patient autonomy.31–40 Other studies have shown that nurses who view voluntary assisted dying as conflicting with their professional identity believe so on the basis of its incongruence with their professional obligation of health promotion 37 and their moral duty of non-maleficence.41–43
However, a novel and significant finding of this study is that nurses anticipated the effect of voluntary assisted dying on their professional identity will have tangible flow on effects on their career experience. Some nurses who expected voluntary assisted dying to reinforce their nursing identity also anticipated this enrichment to manifest tangibly in the form of enhanced job satisfaction. While previous studies have described nurses’ positive experiences of harbouring a sense of honour, privilege, gratitude and relief in being part of voluntary assisted dying,13,14,44 this is the first study in which nurses explicitly expressed this positive sentiment translating into enhanced career fulfilment. This insight provides evidence for the potential for voluntary assisted dying implementation to positively impact nurses’ experience of their careers.
In contrast, other nurses anticipated voluntary assisted dying would negatively impact both their current career experience and future career prospects. The anticipation of a discriminatory and culturally pressuring workplace environment has been previously described in the Canadian context. Beuthin and colleagues report nurses’ fears of being judged for their stances on voluntary assisted dying and concerns regarding the prospect of workplace coercion or bullying. 13 Furthermore, while previous studies have demonstrated that some health professionals, namely, emergency physicians and pharmacists, harbour the fear that their decision to conscientiously object to voluntary assisted dying may negatively impact upon their future employment prospects,45–47 this study demonstrates that nurses feel similarly, within a context in which voluntary assisted dying is legal and where their formal involvement is relatively minor. Taken together, these findings indicate the need for health services to implement staff behaviour policies and associated education aimed at fostering and maintaining a positive, safe and non-coercive workplace culture. Such a culture is one in which nurses feel comfortable to discuss and act upon their right to conscientiously object, supported by human resource practices which reassure nurses that doing so will not negatively affect their future employment prospects.
In terms of the impact of voluntary assisted dying on nurses’ workplace relationships, the finding that some nurses anticipated its implementation to result in a ‘complete loss of trust’ in the nurse–patient relationship is ethically significant. In addition, these nurses’ concern that with time, as voluntary assisted dying becomes integrated into the healthcare system, nurses may become desensitised and experience compassion fatigue is echoed by nurses in the Canadian context. 14
The nurse–patient relationship is built upon a foundation of trust, a value particularly significant in the context of end of life care. 48 Some ethicists even argue against the moral validity of voluntary assisted dying on the basis that it fosters a degree of suspicion and distrust by patients towards nurses, thereby tainting the therapeutic nurse–patient relationship.35,49 However, while present in the nursing ethics literature, evidence of this loss of trust in empirical studies has been limited to date. Exploring ways in which trusting and compassionate nurse–patient relationships might be maintained in the context of legalised VAD will be an important aspect of implementation work in each local setting. Ongoing research is required to ascertain the long-term emotional effects on nurses involved and the flow on effects for patient care.
With regard to nurses’ relationship with the family members of patients requesting voluntary assisted dying, the literature highlights that nurses feel responsible for families’ ongoing care during the voluntary assisted dying process. 50 However, outside of this, little is currently known. This study’s finding that nurses anticipated the occurrence of both emotional abuse and violence towards nurses by family members of patients requesting voluntary assisted dying must be considered with gravity. It should serve to inform health service safety protocols to ensure the emotional, psychological and physical safety of not only nurses, but all hospital staff involved in voluntary assisted dying.
A limitation of this study is that the data were collected in the period after the passing of the voluntary assisted dying legislation in Victoria but before the start date for voluntary assisted dying to be available. Nurses’ responses in this study may have therefore been influenced by feelings of uncertainty and anxiety arising from limited information available at the time of data collection in relation to both the Victorian model of care as set by the relevant government department and the implementation strategy at specific health services. Furthermore, this study captured views from seven Victorian health services with the majority from large hospitals in metropolitan Melbourne. While a large number of nurses participated in the study, the views of these participants cannot be generalised to all Victorian nurses in other healthcare services across the state.
Conclusion
This study demonstrates that while nurses do not have a formal role in the Victorian voluntary assisted dying legislation, they anticipate the implementation of voluntary assisted dying in their workplace to have ethical and practical impacts on several key aspects of their professional lives. As such, this study’s findings offer insights to inform the development of policies and protocols in health services who are currently considering or already implementing voluntary assisted dying, in order to adequately address the potential concerns of their nursing staff.
Based on these findings, we recommend that Health service employment policies explicitly declare nurses’ legal right to conscientiously object to participate in the voluntary assisted dying process, where such a right is specified in the legislative framework in that jurisdiction; Human resources’ practice precludes discrimination among nursing job applicants on the basis of their position on voluntary assisted dying; Staff education programmes are established that foster and maintain a positive, safe and non-coercive workplace culture that respects diverse views on voluntary assisted dying; and Health services institute additional safeguards to address the raised concern of occupational violence towards nurses by family members of patients requesting voluntary assisted dying.
Future research is now required to explore Victorian nurses’ experiences of being involved in voluntary assisted dying post-implementation. During the first year of the Act’s operation, beginning 19 June 2019, 124 Victorians have utilised the legislation to end their lives. 51 Further research is needed to examine the degree to which the anticipated impacts of voluntary assisted dying on nurses’ professional lives expressed in this study have eventuated in practice.
Footnotes
Acknowledgements
We are grateful to all the nurses who participated in this study. We also acknowledge the research team involved in the larger mixed methods survey project: Rosemary Aldrich, Melanie Benson, Karen Detering, Michelle Gold, Barbara Hayes, Courtney Hempton, Anastasia Hutchinson, Jeffrey Kirwan, Lisa O’Driscoll, Marcus Sellars and Mark Tacey.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Dr Danielle Ko is a member of the Victorian Voluntary Assisted Dying Review Board. She has engaged in this research in her role as a clinical ethics researcher and palliative care specialist and not in her role as a member of the Board. Any views expressed in this paper are not to be attributed to the Board. All other authors have no conflicts of interests to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.