
Abstract
To prevent and reduce the transmission of the coronavirus to vulnerable populations, the World Health Organization recommended the restriction of visitors to nursing homes. It was recognised that such restrictions could have profound impact on residents and their families. Nonetheless, these measures were strictly imposed over a prolonged period in many countries; impeding families from remaining involved in their relatives’ care and diluting the meaningful connections for residents with society. It is timely to explore the impact of public health measures on people living in nursing homes from an ethical perspective. In order to foreground the ethical dimensions of the implications of visitor restrictions in nursing homes, we compiled an ethical case that reflects some recent experiences of nursing homes residents and their families, in the Irish Republic. We describe a series of events encountered by a woman and her family during the first wave of the pandemic in 2020 and we deploy an ethical decision-making tool to guide and structure our analysis. Our case analysis draws attention to ethical principles that are relevant to explicating the ethical duties and obligations that arise in relation to the interests, well-being, and safety of residents and their families, as well as nursing home staff and the wider community during a pandemic. These include the right of autonomy, trust, minimising harm, and proportionality. We conclude that a number of different strategies should be adopted by nursing homes and relevant regulatory bodies. This includes honest, regular communication between the nursing home staff, the resident and their family. Central to communications is the resident’s wishes, their current clinical status and the all-important wider public health obligations. National strategies include mass vaccination, the timely provision of guidance documents and interventions from regulatory bodies that are patient-centred, adaptable, and cost effective.
Keywords
Introduction
Coronavirus disease (COVID-19) is highly transmissible. According to the most recent World Health Organization (WHO) 1 global report on the 9 February 2021, the total number of confirmed cases has reached over 105 million worldwide. Residents in nursing homes are at a higher risk of being susceptible to infection from COVID-19, and for subsequent adverse outcomes. 2 In western countries, about 2%–7% of older people are living in nursing homes. 3 Initially nursing home outbreaks showed much higher risk of COVID-19 infection and mortality for residents than in the community.4,5 It is estimated that up to 50 percent of all COVID-19 deaths to date have occurred among nursing home residents.6–8 As the disease spread, it emerged that people living in nursing homes or long-term residential care facilities were at particularly high risk of becoming infected with COVID-19 and suffered greater levels of complications. 9
Early in 2020 little was known about COVID-19 globally, and governments, healthcare facilities and communities were not prepared for the emerging crisis. To curb the transmission of coronavirus (COVID-19), strict public health measures and technical guidance was published by the WHO and the European Centre for Prevention and Disease Control. 10 The National Public Health Emergency Team (NPHET) in Ireland swiftly followed these recommendations. The priority in early government policies related to visitation and minimising the risk of COVID-19 outbreaks in nursing homes. Subsequently, during the first wave of the virus, the Irish Government introduced stringent lockdown restrictions, and visiting restrictions were imposed on all nursing homes. Across Europe, many countries, including Germany, the Netherlands, Belgium, and France, enforced the exclusion of visitors from nursing homes with legislation. 11 The term long-term care (LTC) residential facility, nursing homes or care homes are used internationally to describe facilities where residents live. 12 However, in the international literature, there is also ambiguity regarding the term ‘nursing home’. 13 In Ireland, ‘nursing home’ is used to refer to a collective institutional setting in which care is provided to older adults, on-site 24 hours a day, including on-site or off-site nurses and medical staff. This case is based on a resident living in a nursing home.
Families are an integral part of resident’s care, to help maintain feelings of social inclusion and an overall sense of belonging.
14
Unfortunately, within the context of COVID-19 transmission, the role of families is represented as a risk or threat to residents. In Ireland, as with most other countries globally, the first response to the outbreaks was a radical ban on ‘visitors’ to protect our most vulnerable individuals and groups. Residents were restricted to their single bedrooms without family visits for many months. Many of these families had previously provided companionship and various forms of assistance.
15
The support that families provide is often seen as additional to the care provision by nursing home staff which can result in the family involvement being unrecognised.
16
However, as the Irish Department of Health (DoH) states, ‘Very often, visitors are not guests in the usual sense, but family members visits are what makes life meaningful for individuals in LTC facilities and are a bulwark against loneliness, anxiety and depression. They have a pivotal role in the ongoing wellbeing and resilience of residents, e.g., providing emotional support, reminiscing, preserving identity and continuity, as well as acting as advocates, communicators and allies’.
17
(p. 6)
In order to engage our ethical intuitions and reasoning skills in relation to the ethical challenges that visitor restrictions in nursing homes have given rise to, we have compiled a hybrid case study drawn from a number of recent clinical and personal experiences of the authors. In the interests of protecting the confidentiality and anonymity of those involved, we have used pseudonyms and changed identifiable details. Our case describes a series of events encountered by a woman and her family during the first wave of the COVID-19 pandemic in 2020.
Case study
Mary O’Reilly, aged 95, was fully independent and lived a very active life up to two years ago when she moved to a nursing home due to failing health and mild vascular dementia. She has four very supportive children who live close by and visit regularly. Her eldest daughter, Kate, visits daily and is the primary family contact with the nursing home staff.
On the 6 March 2020, Nursing Home Ireland (NHI), followed by Health Service Executive (HSE) on 13 March, imposed visiting restrictions on nursing homes. All residents including Mary, were placed in isolation in their single rooms to provide protection against the spread of COVID-19. In mid-March, Kate, received a text message to say that three residents in her mother’s nursing home had contracted COVID-19. She was reassured that her mother was well. A further text message was received from the nursing home one week later to say that no further testing would take place currently. This was a time of great concern, giving rise to feelings of helplessness among all the family members. Kate resorted to checking the online Death Notices to see if any residents had died there.
It was mid-April before the HSE announced that all residents and staff in nursing home would be tested for COVID-19. Mary subsequently tested positive for COVID-19, much to the surprise of the staff–she was one of the many residents who was asymptomatic. Mary recovered from COVID-19, but Kate and her siblings felt that communication relating to their mother’s condition was unsatisfactory. The family were concerned about their mother’s health condition and how she was coping with isolation and lack of family interaction. On the phone, Mary continued to ask her children why they are not visiting and questioned when she would see them. Mary found it difficult to comprehend a visiting ban. Kate stated that, over time, Mary became more withdrawn on the phone and no longer showed interest in her children’s lives.
Case analysis
Our exploration and analysis of the case draws on an ethical decision-making tool developed by Campbell and McCarthy. 22 This tool is a variant of existing clinical ethics decision-making frameworks.23–27 All of these frameworks emphasise adequate clinical information, inclusion of appropriate decision-makers and careful consideration of the harms and benefits associated with proposed courses of action. Furthermore, clinical ethics decision-making frameworks pay particular attention to what is ethically troubling about a particular case. 22
The Campbell and McCarthy tool (Figure 1) was specifically designed to enable healthcare practitioners confront challenging situations in the absence of any formal ethics support structure such as clinical ethics committees. The latter play, at best, only a marginal role in healthcare organisations in Ireland where existing clinical ethics support is generally inadequate, fragmented and poorly resourced. 22 The tool follows a transparent stepwise procedure which avoids an overly dense or detailed analysis, while remaining sensitive to the complexity of the issues addressed. A further strength is that it makes an explicit association between each step of the decision-making process and one or more of the ethical responsibilities based on widely agreed norms of ethical decision-making in healthcare and in the wider public context. This makes it particularly suitable for ethical decision-making in the context of a pandemic. Moreover, the tool has been used successfully in several other contexts 28–30 and more recently informed (in part) the DoH publication on ‘Procedural Values for Decision-Making in a Pandemic’. 31 (p. 4) Applying the steps of the decision-making tool to the case of Mary O’Reilly gives rise to the following considerations.
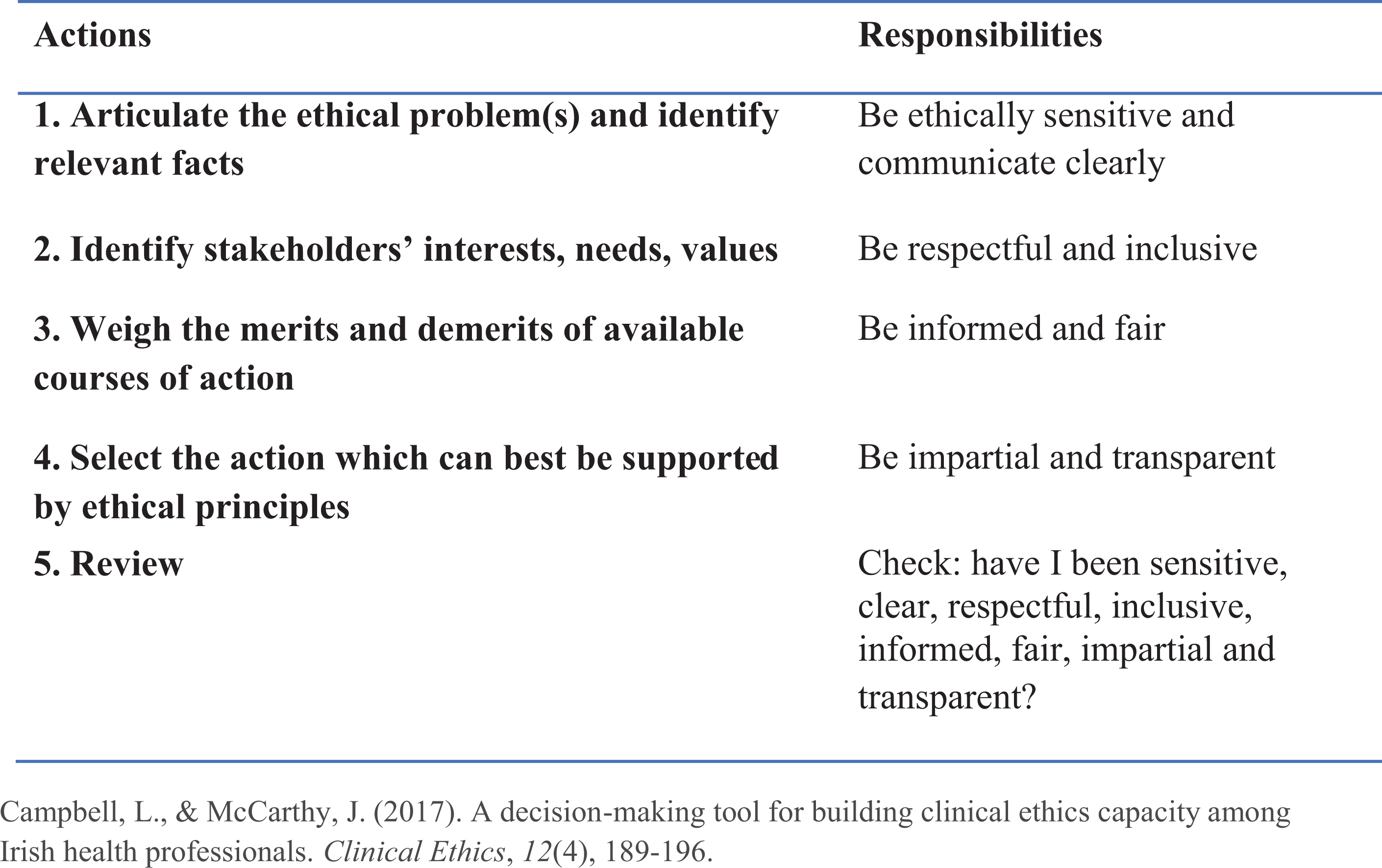
Decision Making Tool. Campbell and McCarthy. 22
Action 1. Articulate the ethical problem(s) and identify relevant facts
A number of ethical issues arise in this case. A lack of recognition of the central role that Mary’s family play in her life, health and well-being. Poor on-going communication from the nursing home staff significantly weakens the family ties with their mother and undervalues their contribution to her care. Mary’s knowledge and understanding of her situation is unclear and it seems that she has not been involved in any of the decisions regarding her treatment and care. Nor have her family been invited to contribute their understanding of their mother’s wishes The HSE and the nursing home have a responsibility to protect the lives and health of Mary, the other residents and staff of the nursing home, and the wider community. Therefore, restrictions on individual liberty is required to comply with government restriction and infection control policy. The ethical question to be considered is whether or not the banning of visitors and isolating residents is proportionate.
The A nursing home is a communal setting, therefore all residents and staff are at risk of contracting COVID-19 Mary has experienced a prolonged period of isolation in a single room pre- and post-contracting COVID-19 The level and severity of Mary’s dementia seems to increase over the period of isolation Mary’s family support and involvement in her life is now absent The level of expertise and preparedness to manage the COVID-19 pandemic is challenging for all concerned.
Action 2. Identify stakeholders’ interests, needs, and values
Inclusiveness is a core requirement of ethically sound decision-making. Any person who is affected by a decision should be included in the decision-making process – they must have an opportunity to communicate what is important to them and should not be excluded without good reason. The key stakeholders in this case are Mary, her family, other residents, and staff. However, because the case takes place in the midst of the global pandemic of COVID-19, other important stakeholders are the DoH and two national regulatory agencies, HSE and Health Information and Quality Authority (HIQA), as these parties are responsible for the state’s health and ethical interests. Additional stakeholders are Nursing Home owners, as nursing homes may be owned and operated by private providers.
Resident: Mary
Mary’s beliefs, values, preferences, knowledge of her situation and understanding of the impact of COVID-19 should be a central focus in the decision-making process. Mary may have different levels of capacity to make decisions regarding her treatment, care, her move to a single room and she may well prefer not to be involved in these decisions. In addition, Mary may have a very good understanding of the symptoms of COVID-19 but may need some help to understand transmission, social distancing, and the need to stop visitations. Mary’s safety, health and well-being, as she understands it, also need to be considered. The nursing home is, understandably, following HSE advice and putting systems in place to protect her from contracting COVID-19. However, Mary seems to be increasingly confused and she does not understand why her family have stopped visiting.
Family
Mary’s family are deeply involved in her life and concerned about her safety and well-being. Their role in Mary’s life as advocates and allies as well as their contribution to her care, health and well-being deserves respect and recognition. When Kate joins her mother in her encounters with doctors and other professionals, neither she nor Mary may view her role as merely an accompaniment. Her mother may rely on her help to remember what was said during medical encounters, to ensure that Mary’s own questions are raised, to judge the trustworthiness of the recommendations given, and help her to decide what is the best course of action for her.
Other residents in the nursing home
All of the nursing home residents are likely to have an interest in being safe and healthy. At the same time, their individual liberty, their values, preferences, and well-being are important.
State Department of Health and regulatory agencies
In brief, the DoH is a division of the Irish government which is responsible for providing leadership, policy direction, and governance of the Irish health services. Its Statement of Strategy mission, which is outcome oriented, is to ‘improve the health and wellbeing of people in Ireland by: keeping people healthy; providing the healthcare people need; delivering high quality services; and getting best value from health system resources’ 32 (p. 2). Its values focus on the ethical virtues of the public service providers such as integrity, impartiality, respect and equality as well as more utilitarian goals of accountability, efficiency and value for money.
The HSE is the state provider of public health services in the hospitals and community health settings across Ireland. Its goals, similar to those of the DoH, are outcome oriented but also include attention to rights and virtues include promoting health and wellbeing, providing fair and equitable, safe and quality treatment, fostering an honest, compassionate, transparent and accountable culture, developing and supporting the workforce of health providers and managing resources efficiently. Its stated values focus on ethical virtues such as care, compassion, trust, and learning. 33
HIQA is an independent statutory authority which reports to the DoH and is responsible for promoting safety and quality in the provision of health and social care services for the benefit of the general public. In normal times it is the regulator and body which inspects nursing homes and many other healthcare organisations. During COVID-19, HIQA is considered to be a nursing home representative for residents on the NPHET.
The orientation of all three stakeholders – DoH, HSE, HIQA – is towards improving the health of the general public through the judicious management of resources and good governance. In March 2020, the DoH produced an Ethical Framework which specified the state’s interest in ensuring an equitable, non-discriminatory, and proportionate response to the COVID-19 pandemic while at the same time attaining utilitarian goals regarding the allocation of limited resources: ‘The main goals of the public health response to a pandemic should be to minimise the negative health impacts of the pandemic (i.e., the number of hospitalisations and deaths) and to maintain a functioning society. This goal may be achieved through the use of effective management and containment strategies and the prudent stewardship of resources’.
34
(p. 3)
Nursing home staff
Nursing home staff may experience conflict in respect of balancing their concerns about Mary’s autonomy with their duty of care to all residents in the nursing home. They may also be concerned about their own and their family’s safety. The health professionals and other staff may also be concerned about their perceived professional duties to follow HSE and HIQA policy. They may also feel conflicted about their duty of care to Mary’s family. As a result of these conflicts, staff may experience moral distress, as isolating Mary and banning visitors may be contrary to their own moral values and personal integrity. Moreover, they may view these actions as inconsistent with a caring ethos of person centredness. Finally, staff, especially management, have additional responsibilities towards the wider community in relation to the stewardship of scarce resources such as Personal Protective Equipment (PPE) and staffing levels, as well as disrupted care processes, testing backlogs and lack of access to swabbing.
Action 3. Weigh the merits and demerits of available courses of action
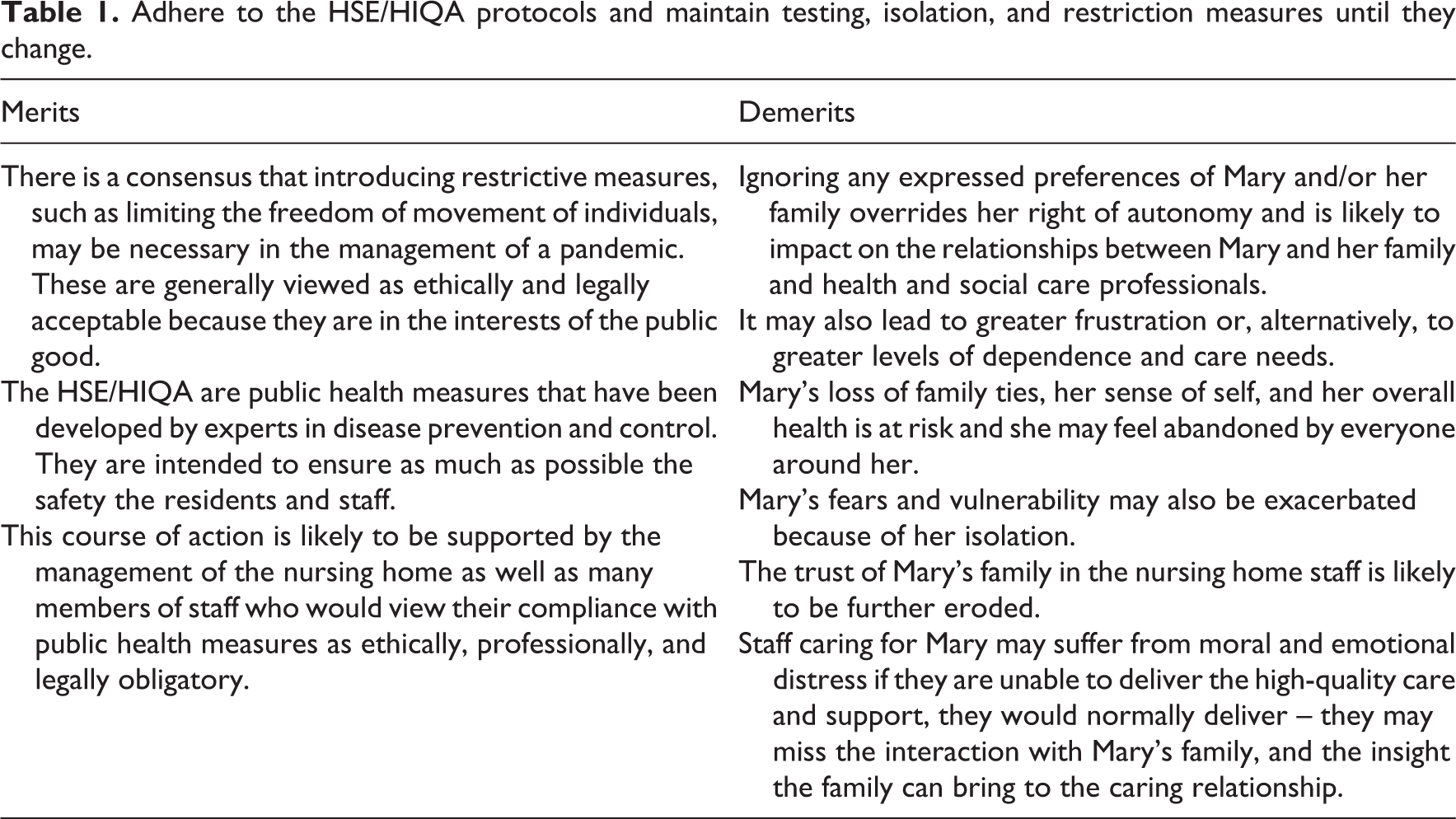
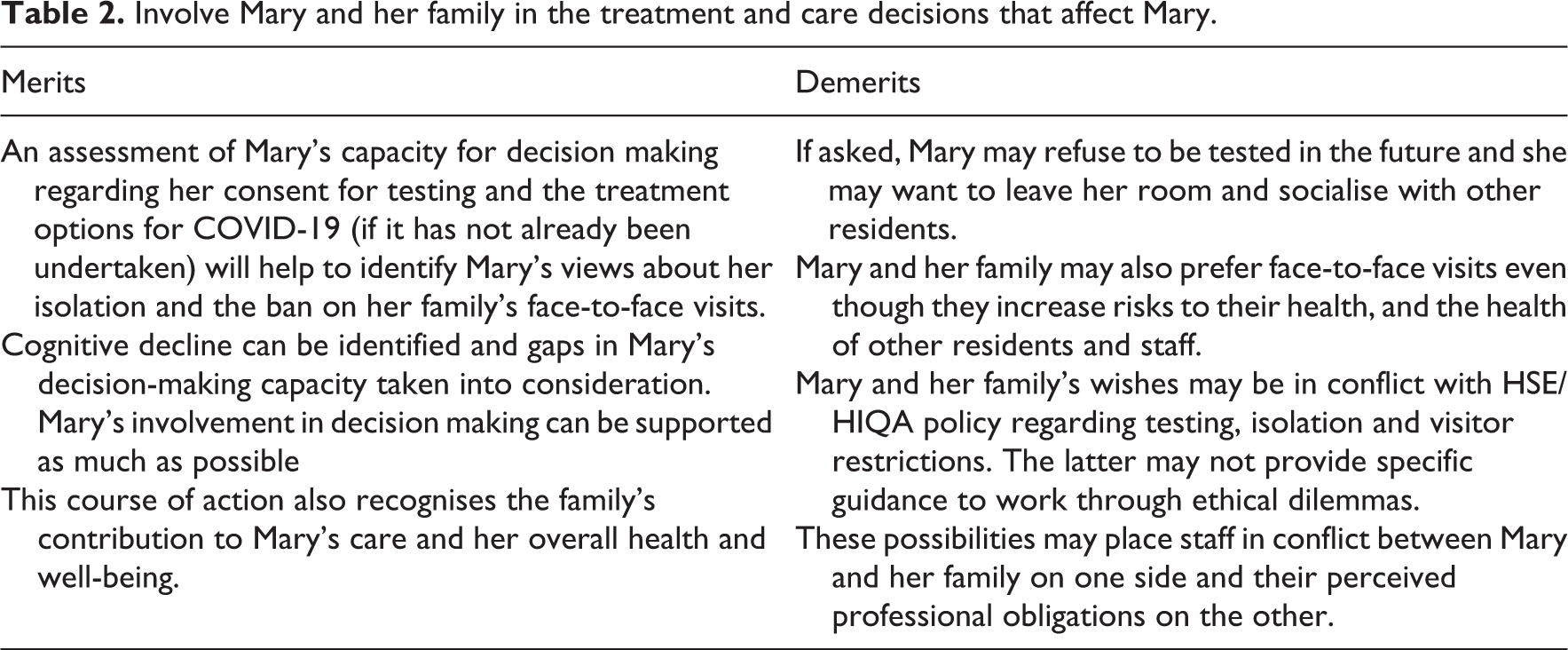
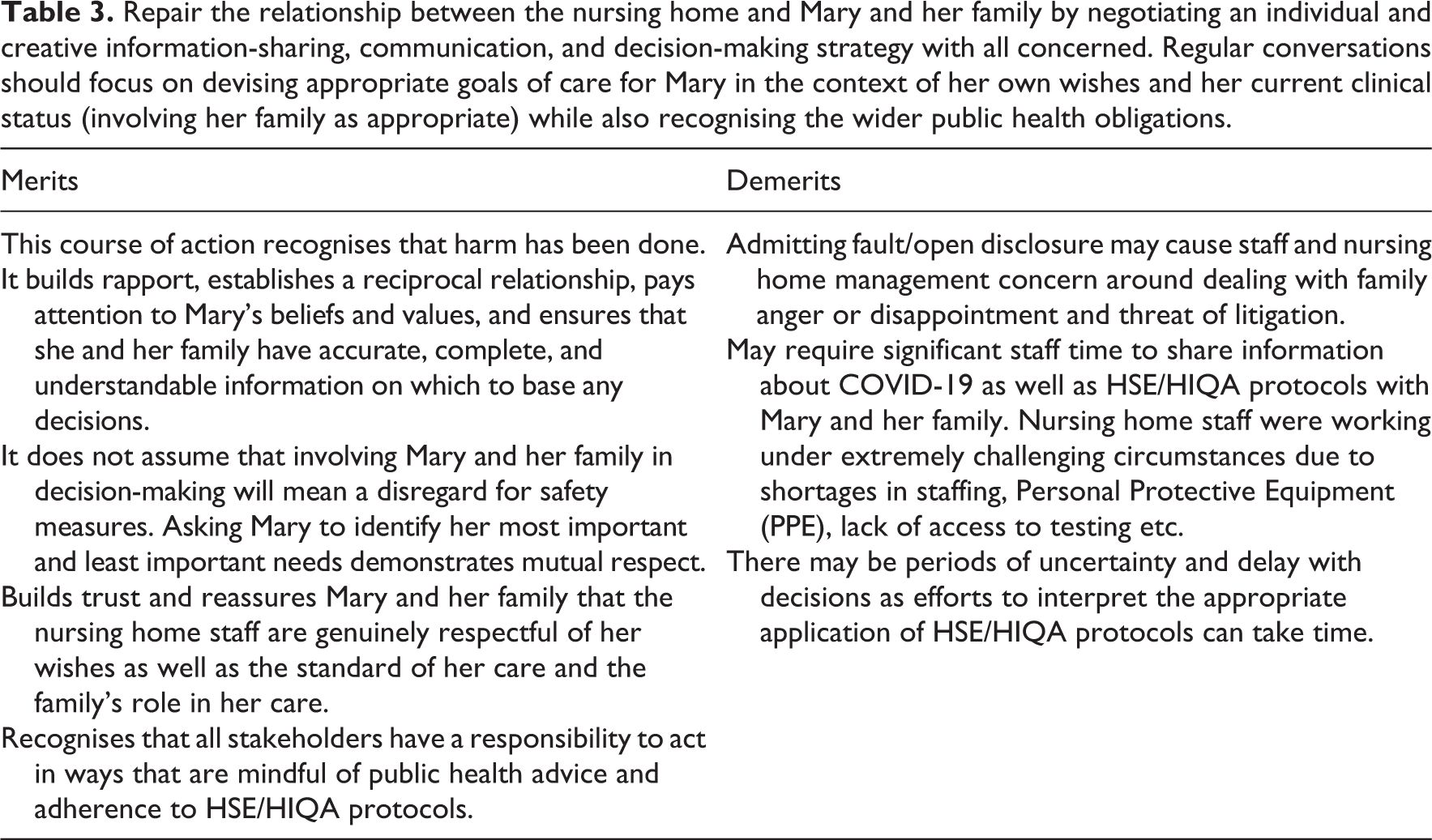
There are any number of different courses of action that we suggest staff in the nursing home might pursue in order to respond to Mary’s current situation. First, we briefly consider two options (A Table 1) and (B Table 2), which we think go to the heart of the ethical concerns in this case. Then, drawing on our consideration of these options, we suggest a third option (C Table 3) that we think is likely to yield the most satisfactory and ethically sound outcome for all concerned.
Adhere to the HSE/HIQA protocols and maintain testing, isolation, and restriction measures until they change.
Involve Mary and her family in the treatment and care decisions that affect Mary.
Repair the relationship between the nursing home and Mary and her family by negotiating an individual and creative information-sharing, communication, and decision-making strategy with all concerned. Regular conversations should focus on devising appropriate goals of care for Mary in the context of her own wishes and her current clinical status (involving her family as appropriate) while also recognising the wider public health obligations.
Action 4. Select the action which can best be supported by ethical principles
While the course of action outlined under option C) will take time and resources, it is consistent with some of the core ethical principles that are crucial to the delivery of person-centred care in the nursing home context. These include: the right of autonomy; trust; minimising harm; and proportionality. These principles and their relevance to Mary’s situation are outlined below:
Autonomy
Autonomy is the capacity for self-determination; a person’s ability to make choices about their own life based on their values and beliefs about what is important. The principle of respect for autonomy recognizes the unique values, priorities and preferences of individuals and supports them to participate as fully as possible in decisions about their care. It should not be presumed that, simply because a person lacks the capacity to make a specific decision about a particular treatment or care, they do not have the capacity to make other decisions.
Option C) promotes and protects Mary’s right of autonomy – and recognises the role of Mary’s family in her life and their possible role in supporting her decision-making. It is also consistent with the requirements of the HSE National Policy and the Irish Assisted Decision-Making (Capacity) Act 2015 which stipulates that, whatever level of capacity for decision-making an individual may have, their will and preferences should inform any decisions concerning them.35,36 In addition, the Irish DoH specifies that nursing homes have a ‘special responsibility’ in this regard, ‘Institutions whose purpose is to care for vulnerable people have a special responsibility not to multiply the vulnerabilities of those in their care. Decision-making for people with intellectual disabilities or diminished capacity must promote inclusion, autonomy and participation to the greatest extent possible’. 37 (p. 2)
Trust
For health professionals and institutions to be considered worthy of trust, or trustworthy, O’Neill determines three core characteristics: reliability, competence, and honesty. 38,39 Trust in healthcare is generally understood as a kind reliance on the part of those receiving care that their carers will behave according to certain standards of care and that they can be held responsible if they fail to do so. Specifically, in nursing homes, trust implies a duty of care on the part of health professionals who are presumed to care about, respect, and have regard for the overall dignity and well-being of residents.
When communication between Kate and the nursing home staff ceased during the early days of the pandemic, Kate relied on media information for updates on the nursing home situation. This absence of communication contributed to the family’s growing sense of mistrust and heightened anxiety.
When trust is damaged in this way, it needs to be repaired. In the communication strategy of option C) the nursing home staff should acknowledge their responsibility for the mistakes made, apologise for them, and reassure the family that they are renewing their commitment to their goals of person-centred care, standards of quality care, and revising their policies relating to isolation and visitation during periods of lockdown. 40 Moreover, they might adopt honest, transparent, and clear communication strategies e.g. weekly global communications with family members and provide regular information (various formats) on the organisation’s approach to implementing the public health measures and subsequent implications for care.
The HSE and HIQA were also obliged to provide additional support to nursing homes during this crisis. HIQA set up a quality assurance process whereby all nursing homes were phoned on a fortnightly basis by an inspector of social services. These calls were to assess the welfare of the residents, how nursing homes were coping, any concerns they had, and any deficiencies identified in their ability to sustain a safe, high-quality service. The Government set out a National Action Plan on COVID-19, setting out the course for how state bodies would manage the crisis. The HSE made additional provision for staffing, PPE, and access to testing in nursing homes during April.
Minimising harm
The principle of minimizing harm in the context of COVID-19 has been defined by the Irish DoH in the following way:
‘A foundational principle of public health ethics is the obligation to protect the public from serious harm. Harm is a broad concept, but includes physical, psychological, social and economic harm. In a pandemic, restrictions to individual liberty (e.g., asking people to self-isolate), access to services (e.g., cancellation of elective procedures/out-patient clinics) or service areas (e.g., limiting visitors to hospitals/residential facilities), as well as the imposition of infection control practices (e.g., restricting public gatherings), may be necessary to protect the public from harm. Where such restrictions are being considered, decision-makers should provide reasons for the public health measures to encourage compliance and should establish a mechanism to review decisions.’ 34 (p. 6)
Mary did, in fact, contract COVID-19. She was further disadvantaged as there seemed to be a lack of involvement in any decision-making regarding her isolation Furthermore, her family were not consulted about her wishes, nor were they involved in her care. The communication strategy in option C) focuses on repairing the damage done to Mary and her family may address any harm caused and minimise any further harm.
Measures to manage infection-transmission risks must be balanced with other major risks; especially the risk of losing needed representation and advocacy to ensure that the delivery of health care is aligned with the resident’s needs and wishes. Banning all visitors and socially isolating residents may be viewed as the relatively ‘easy response’ to managing the pandemic. However, as the DoH points out: ‘Given the power asymmetries in LTC facilities between residents, their families, and health and social care workers and managers, care must be taken not to impose disproportionate or coercive measures to achieve the ends of safety, efficiency, or other organisational goals.’
37
(pp. 5–6).
Proportionality
The principle of proportionality in the context of COVID-19 has been defined by the Irish DoH in the following way: ‘Proportionality requires that restrictions to individual liberty and measures taken to protect the public from serious harm should not exceed what is considered necessary to address the actual level of risk to, or critical need of, the community. The least restrictive measures to achieve public health goals should be employed.’
34
(p.6)
Action 5. Review
The process described incorporates each element of responsible and ethical decision making. First, the key ethical concerns that arise and the values that are at risk in Mary’s case have been clearly identified and articulated. Second, the collaborative approach taken is respectful and inclusive of the perspectives and interests of all involved i.e. Mary, her family, other residents, nursing home staff and state regulatory bodies. Third, the decision-making is informed by relevant ethical, legal, clinical, and regulatory standards. Finally, the perspective taken is non-judgmental, and the steps taken are clearly outlined.
Conclusion
Our case analysis draws attention to four ethical principles that are relevant to explicating the ethical duties and obligations that arise in relation to the interests, well-being, and safety of residents and their families, as well as nursing home staff and the wider community during a pandemic. These include the right of autonomy; trust; minimising harm; and proportionality.
The high transmissibility of the COVID-19 virus cannot be overstated in evaluating the case and the fact that little was known during the first wave of the COVID-19 pandemic. While many nursing homes would have experienced disease outbreaks such as the norovirus or influenza, such experiences did not prepare them for COVID-19. Based on public health advice, the HSE and NHI placed a blanket ban on visitors and family caregivers to prevent the spread of COVID-19 infections in nursing homes. This approach failed to recognize the significance of resident-family relationships as a means of supporting resident autonomy and enhancing the quality of residents’ lives and their care. Moreover, agencies were initially slow to respond to the crisis for nursing home providers who faced issues on multiple fronts such as shortage of staffing, PPE, testing backlogs and lack of access to swabbing. The current roll out of mass vaccination, starting with nursing homes and healthcare facilities, mitigates some of these issues in the future.
Nursing homes’ are predominantly based on a social care model. 41 The key characteristic of nursing homes is that they resemble, indeed are, more a home than a health setting. This was largely overlooked by policy makers in the first wave of the pandemic. One lesson learned is that the model of nursing home care nationally and internationally has been questioned – both in design and delivery. 42 There are emerging opinions regarding improved layout to support improved infections prevention and control measures. The National Expert Panel review reported the utility of smaller household models of residential care which permit changes in infrastructure from the traditional institutional model to an environment that more resembles a family home. 2 Finally, different strategies regarding ‘visitors’ should be adopted by nursing homes, depending on the resident’s situation and context. Such a move would be supported by the considerable evidence emerging that restricting visitors, especially close family members, has detrimental effects on residents’ mental health, especially for people living with dementia.
Implications for practice
Genuine respect for the personal autonomy of individual residents and a commitment to protecting and enhancing whatever level of capacity they have to participate (or not) in decisions affecting them.
Not all family members are ‘visitors’ in the usual sense. While they can provide deeply cherished company for older adults, some family members are also the most trusted people in their lives and provide an essential care role and function within the nursing home. Therefore, procedures, such as screening “visitors” for potential infection transmission risk must be implemented and visitors guided to follow needed protective measures to ensure the safety of all people.
There is a need to build the capacity and to improve the ethical literacy and understanding of staff in relation to the ethical challenges that arise in the context of a pandemic where public health safety measures may impact on patient-centred care.
Transparent communication with families is essential at all times, but this needs to be further magnified during a pandemic. Nursing homes need to share policies with families relating to isolation and visitor access during periods of lockdown and involve them in devising appropriate goals of care and preferences around visiting.
Local strategies include honest, regular conversations among residents, family, and staff which are cognisant of residents’ wishes and their current clinical status, but also recognise the wider public health obligations of all. This would help restore families’ confidence and help minimise harm in the event of possible surges in the future.
In the absence of formal relationships between the DoH and regulatory agencies there needs to be greater community support and regular contact for nursing home staff to avail of the public health expertise and guidance during and beyond the COVID-19 pandemic.
There is a need for an independent advisory service to provide additional support for families with loved ones in nursing homes.