
Abstract
Background:
School nurses have great responsibilities as the connecting link between school, children/adolescents, parents, and other healthcare services. Being in this middle position, and handling complex situations and problems related to children in school, may be demanding and also lead to ethical challenges. Clinical ethics support, such as ethics reflection groups, may be of help when dealing with ethical challenges. However, there is little research on experiences with ethics reflection groups among school nurses.
Aim:
The aim of this research was to explore how nurses in school healthcare experience their role, and how they experience participation in ethics reflection groups, using a model for systematic ethics reflection, the Centre for Medical Ethics model.
Research design:
The project had a qualitative design, using focus group interviews and thematic analysis.
Ethical considerations:
The study was evaluated by the Data Protection Official at the Norwegian Centre for Research Data (project no. 57373). The participants were given oral and written information about the study and signed a written consent.
Participants and context:
Twelve participants from school healthcare were recruited to the interviews.
Findings:
School nurses described their role as extremely challenging. How the school nurses experienced their role also influenced how they experienced participating in ethics reflection groups. The Centre for Medical Ethics model was experienced as both challenging and comprehensive. However, they also experienced that the model helped them to clarify their role and could also help them to find better solutions.
Conclusion:
The role as school nurse is complex and demanding, with several ethical challenges. Ethics reflection groups may be of great help when dealing with these challenges. However, it is of great importance that the methods used are adjusted to the professionals’ needs and context.
Keywords
Introduction
According to the World Health Organization (WHO), 1 school health services exist in high-, middle-, and low-income countries. Globally, the WHO works to support member states in strengthening school health services. The support from the WHO focuses on implementation of the four pillars for so-called Health Promoting Schools: (1) Health promoting school policies, (2) Safe and healthy learning environment, (3) Skills-based health education, and (4) School-based health and nutrition. 1
School healthcare in Norway is part of community healthcare, and hence also funded by the municipalities. In 2017, the first national guidelines for school healthcare in Norway were introduced. 2 According to the guidelines, the main goal of school healthcare is to promote mental and physical health, promote good social and environmental conditions, and prevent disease and harm.
According to the national guidelines, there are no legal standards for how many school nurses there should be in each school. The document only states that the municipalities are responsible for having school nurses. This means that one school nurse may work alone, independent of how many pupils there are at the school. The guidelines also state that the municipalities should have control systems to secure a clear distribution of responsibilities and tasks. 2 School nurses are important as the connecting link between school, children/adolescents, parents, and other healthcare services, and often must interact with all these actors. Being in this middle position—often alone as school nurse—between all these instances, and handling complex situations and problems related to children in school, may be demanding and also lead to ethical challenges. An ethical challenge may be defined as a value conflict, or a situation where there is doubt and disagreement about what is morally best to do. 3 To enhance ethical competence and awareness and prevent moral distress, it is of great importance to have the opportunity to reflect on and discuss the ethical challenges that arise. Clinical ethics support services (CESS), like ethics reflection groups, may then be an important support.
Project with ethics reflection groups in school healthcare
In 2016, the Centre for Medical Ethics (CME) at the University of Oslo started a project, “Ethics in School Health Care,” implementing ethics reflection groups, in collaboration with the school healthcare services of a municipality in the eastern part of Norway. The aim was to increase the ethics competence and ethical awareness among healthcare workers in school healthcare. In addition, the aim was to offer them a tool and model (the CME model) to use when they experience ethical problems in practice. The project leaders gathered all the healthcare workers from the school healthcare services in the participating municipalities for a two hours session, to inform about the project. During this session, we also introduced some basic theory on ethics and how to use the CME model in ethics reflection. After this first introduction, some of the healthcare workers were trained in how to facilitate ethics reflection groups, using the CME model. The project period lasted till May 2018.
The centre for medical ethics model
The CME model is a reflection model developed by researchers at the CME. The model consists of six steps: (1) Defining the ethical problem or dilemma, (2) describing relevant facts of the case, (3) parties involved in the case and their views and interests, (4) ethical values and principles involved in the case, (5) relevant laws and guidelines, and (6) acceptable solutions or how to best handle the problem. 4
Previous research
Research on clinical ethics supports services has shown that systematic ethics reflection may bring benefits. It may enhance healthcare workers’ competency in ethics in general, but also lead to better solutions and better collaboration between healthcare personnel. In addition, it may increase patients’ and relatives’ involvement in care practices. 5 –9
Research from Canada and Australia has shown that school nurses may experience ethical challenges related to vaccination programs, and especially related to the consent process when vaccinating children in school. In addition, they may experience challenges related to collaboration and information between different authorities. 10,11 Because school nurses have to collaborate with several instances in the school system, they also experience problems related to confidentiality and trust. 12 –14
Other ethical challenges described are those related to documentation of psychosocial problems and documentation of maltreatment. 12 Ethical challenges in conjunction with registration of height and weight and how to approach obesity in adolescents have also been reported. 15 –18
The latest research also reports challenges when children share information with school nurses on smartphones. Information they shared could be related to suicidal ideation, information on potential neglect or abuse, and socially unacceptable content. 19 A US study from 2018 shows that 97% of school nurses experienced moral distress at work. Moral distress may be related to ethical challenges because of lack of time and resources.
Although we know that there are several ethical challenges in school healthcare, we know little about how school nurses handle ethical challenges, or what ethics support tools may help them to handle these challenges. With this article, we will try to fill some of this knowledge gap.
Aim
The aim with this article is to present findings on how nurses in school healthcare experience their role, and how they experience participation in ethics reflection groups, using a model for systematic ethics reflection, the CME model.
Design and methods
The project had a qualitative design, using focus group interviews and thematic analysis.
Participants and context
For the focus group interviews, we recruited participants from school healthcare services who had participated in the project “Ethics in School Health Care.” Among the participants were both school nurses and a few psychologists working in school healthcare. Only two psychologists participated in interviews, both of them were facilitators. The findings reported here, therefore mainly focus on the nurses’ experiences.
The school nurses and psychologists were already organized in groups that met every second week to discuss challenges and experiences. Each of these groups had a facilitator. In this project, the facilitators were trained to facilitate the ethics reflection groups along with a co-facilitator. The training period consisted of four half days, where they got some theoretical teaching in addition to practical training on how to facilitate ethics reflection groups (ERGs).
After the training period had finished, the facilitators facilitated two to four ethics reflections before the focus group interviews. The project leaders (AK and BA) participated as observers in some of the groups. Data from the observations are not included in this article. The participants in the focus group interviews were recruited by their managers.
Focus group interviews
There was one focus group interview with the six facilitators, and two focus group interviews with six school nurses who had participated in ethics reflection groups.
Two researchers who were not responsible for the training of the participants, did the interviews (MM and RF). The interviews were conducted in September and October 2018. Interviews were based on an interview-guide with open-ended questions. Among the questions, they were asked how they had experienced the sessions with ethics reflection, and how they experienced using the CME model during the ethics reflections. The interviews were audio-recorded and transcribed verbatim. Each interview lasted 1–1½ hours.
Analysis
We did a thematic content analysis following the six steps described by Braun and Clarke. 20 These six steps are (1) becoming familiar with the material by reading it openly, (2) generating tentative codes, (3) searching for themes, (4) evaluating themes, (5) define and name themes, and 6) writing the text or paper.
All the authors read the data material independently (step 1). The project leaders (AK and BA) did the main analysis in steps 2–3, and met several times to discuss tentative codes and themes. In steps 4 and 5, the project leaders and the two researchers who had done the focus group interviews met to discuss and evaluate the themes.
Ethical considerations
The Data Protection Official at the Norwegian Centre for Research Data (NSD) approved the study before we started the collection of data (project number 57373). The participants were given both verbal and written information about the study and signed a written consent.
Results
Throughout the interviews, informants often referred to the particular features of the role as school nurses. Although not emphasized in the interview guide, these characterizations ended up providing a highly illuminating context for the informants’ experiences with ethics reflection. Both the school nurses themselves and the psychologists talked about the demanding role of the school nurses. How the school nurses experienced their role also influenced how they experienced participating in ethics reflection groups and using the CME model.
Main themes and subthemes are listed in Table 1:
Themes and subthemes.
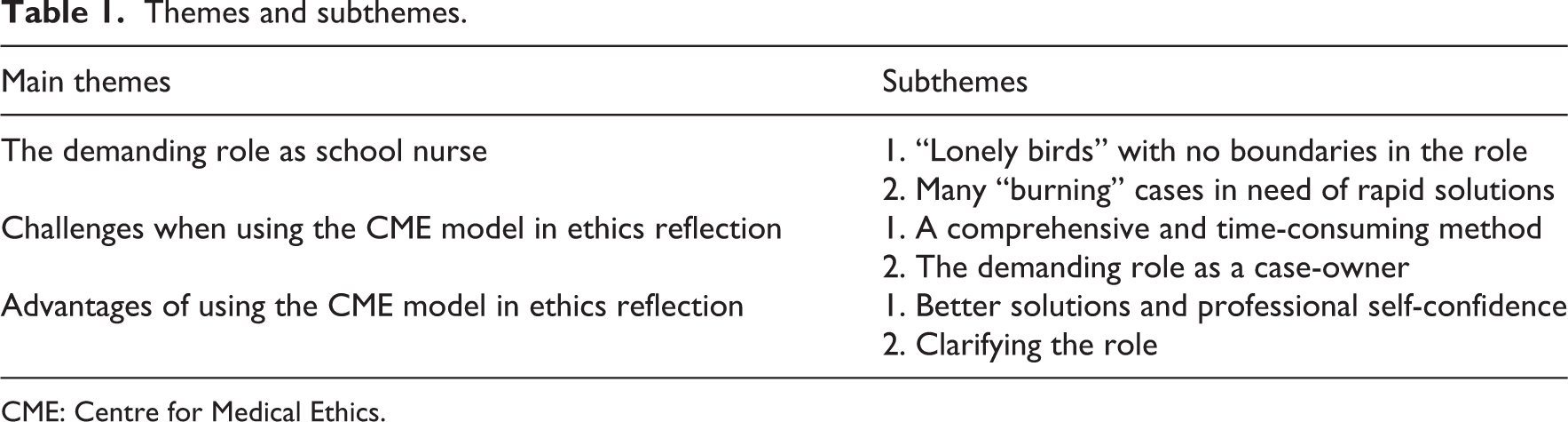
CME: Centre for Medical Ethics.
The demanding role as school nurse
“Lonely birds” with lack of role clarity
All the informants described the role as school nurse as very demanding: C: So yes, we touched on that, and it was always brought up that the school nurse often had, a difficult role, right? In these cases, since the school nurse often is the one the parents or child come to first, and then you have to maneuver among laws and ethics and this…right? What, what to do… E: And each of us has over 500 pupils on our lists, and many of them struggle with things we don’t even know about. That’s how it is. E: No. That’s it. They are very happy to pass the ball to whomever catches it, in a way. When the kid isn’t as expected. “Can someone fix this kid?”
Many “burning” cases and need for rapid solutions
The demanding role as school nurse was also related to all the cases and ethical challenges they had to deal with alone. They talked about many “burning” cases which should be handled rapidly. The school nurses described the situations as “vehement.” To handle all the “burning” situations, the solutions were often characterized as “firefighting,” a superficial handling of the most acute features of the problem, without the opportunity to go more to the roots of the problems. In their biweekly meetings, they wanted colleagues to give them some quick advice and feedback on how they had handled the situation. D: Everyone is responsible for at least one or two fairly serious situations, that are difficult, and that require discussion. Whether you have gotten on with it, and just need confirmation, like you said, “yes, I would’ve done the same,” right? Or that you need “what do I do now?” And you often need that. Immediately, right?
Challenges with ethics reflection groups
A comprehensive and time-consuming model
School nurses expressed an immense need to share their problems and challenges with each other. But because they often needed quick and rapid answers and solutions on the many “burning” cases, they found the CME model too time-consuming and extensive. F: Sometimes, in the group there is resistance [to the CME model]. Yes, because it takes so long. I have found that. D: Supervision [i.e., the biweekly meetings] is something you look forward to, because you are getting help. Hard things you are dealing with. At least I feel that way […] But, of course, when the supervision is over, and you are still stuck with the things that…Personally, your needs, that weren’t covered […]. [The CME model] is pretty extensive. Yes, filling it out and such, but maybe that will get easier as we go along, but […] To get to what felt right, it took a very long time. F: So that is part of the dilemma here, when we are going to…use ethics reflection as a method, […] I think they feel like they lose something else. […] and they need the…the more informal where everyone gets to talk about their situation, and then it is a little unfortunate that ethics reflection maybe came instead. So, so I think that, yes, that it would more easily be met in a positive way, if, if it came in addition to, and wasn’t in a way, stealing the time that they really need.
The demanding role as case-holder
When following the CME model, one of the participants shares a case he or she has experienced as an ethical challenge. Yet, sharing a case with colleagues was seen as quite demanding for some of the case-holders; both because they had to prepare the case presentation before they met and because sharing the case in the group was in itself demanding. They were being asked several detailed questions on how they had handled the situation. Some of them described it as being in an “examination.” Emotionally, it was demanding to be exposed to your own doubts, and to talk about very difficult situations. F: Yes, I think…Yes, I have noticed that in some of them. At least the roughest cases, if they come up in ethics reflection, you get very…Actually feel very exposed, or something. It can be a little scary, actually. F: I feel like it depends on who’s in the group, because I feel more comfortable with some than others. This group we are in now, I think it’s more…I think it’s ok to bring things up. Actually. Yes. So it’s very dependent upon…It’s very, in a way, a little dependent upon how well you know each other, really. C: Yes, or you have to have [the case], sort of processed a little by yourself, before bringing it up.
Advantages of using the centre for medical ethics model in ethics reflection
Better solutions and self-confidence
Several of our informants found that they ended up handling problems better and found better solutions, after raising the problems ethics reflection groups and using the CME model. They also found that the solutions were better founded than when they only were “fire-fighting.” Going through the CME model also brought confidence and strength in their lonely role: D: So I think, through supervision, through reflection [using the CME model: our comment], we are strengthened in solving things by ourselves. E: I guess we agreed in the group that…When we did it a few times, that the conclusions were not changed by doing the reflection, but that sometimes it was nice to have done the reflections, when looking back, to see, yes, you have actually done what you could have done, even if you had done it. So, seeing that your natural instinct isn’t so bad, but to have it confirmed and supported that you did the right thing. That you didn’t step on any toes by being unethical, that was, in a way, maybe most of what came out of it. C: Maybe you had thought it was right, but then at least you get that, now we have properly looked at it and…more weight in the decision, I guess. B: But by using the CME model, you get more solutions to, how we can see it, or how we can understand…the problem. C: We got more perspectives, thought about more things, than you normally would. So you have a stronger foundation for your decision.
Systematic ethics reflection helps clarify the role
When reflecting on ethical problems, the school nurses found that they got the opportunity to “tidy up,” and also clarify their role related to ethical challenges. These could be challenges where teachers came to the school nurses and wanted them to solve problems. Through the ethics reflections, it became clear that the case actually should have been handled by teachers or school management instead, the actual “owners” of the problem. E: And what I thought was the most exciting was really, who is really a part of…Who is relevant in this problem? Whose case is it? Because that brought us to many useful things. Because as school nurses, we are so…we are just brought into others’ problems, so…We are supposed to handle all the difficult things. Both the shameful things, and the emotional things, and those things that are uncomfortable for others to handle. Those are just thought of as “school nurse can handle that.”
Discussion
Our findings show that systematic ethics reflection may be time-consuming and therefore challenging to implement in practice, when the healthcare workers need or expect quick solutions. This has also been reported in a previous study of ethics reflection in community healthcare. 21 According to Söderhamn et al., 21 it may be important to use different methods and organize ethics reflections in different ways depending on healthcare personnel’s needs. One solution could be to only use some parts of a reflection method, like the CME model, or to use a simplified versions of the model if the healthcare workers find it to be too extensive or time-consuming. At the same time, our participants emphasize that it was the model’s ability exhaust and make explicit the morally relevant points, that enabled them to find better and more solidly founded solutions. Fire-fighting may help in the short run, but does not help in the long run. Using the CME model made them more confident with the final solutions. According to previous research, healthcare personnel may experience frustration if ethics reflection does not lead to solutions. 22 Coming to a better solution may therefore be one of the main objectives when using a reflection model like the CME model.
The fact that healthcare workers find that systematic ethics reflection led to better solutions and potential improvement of practice, is also reported in previous research from the mental healthcare setting. 3,9 The present project, then, took an established clinical ethics support activity—ethics reflection groups with the CME model—and applied it within a new healthcare setting, that is, school healthcare. In future research and development projects, it would likely be fruitful to work closely with school nurses and their leaders to tailor clinical ethics support activities to the specific needs and working conditions of this group. Previous research has also shown that it may be of great importance to develop projects on ethics support from a bottom-up perspective, with active participation of stakeholders. 23 However, new projects should also learn from other research about barriers and enablers when developing projects on ethics support.
According to our findings, school nurses may experience lack of role clarity. Systematic ethics reflection could contribute to role clarification and thus improved self-confidence. Role clarity implies that the employee knows the job requirements and what is formally and informally expected of him or her. 24 According to the national guidelines, municipalities should have their own control system which should secure a clear disposition of responsibility and tasks, and where goals, tasks, and activities should be clearly defined. 2 This means that there should be a system which ensures role clarity. Our findings show that this is lacking, or the system does not work as intended. Research shows that lack of role clarity might contribute to burnout and higher turnover. 25,26 If systematic ethics reflection may help clarifying the role and prevent burnout and turnover, this may be important knowledge for leaders, since leaders have a crucial responsibility for the work environment. We also know that managers and leaders have a key role when it comes to ethics support in practice, and that systematic ethics work depends on a supportive organization. 9,27 If the leaders do not prioritize time and resources to ethics support, it will not succeed.
Our findings also show that the role as case-owner may be very challenging. Ethical challenges may be emotionally loaded, and it may be demanding to share doubt and uncertainty in complex cases. This corresponds well with research on CESS from other settings. 28 Professionals might be reluctant to expose actions and deliberations that might lead to being criticized. Lowering the felt threshold for presenting an ethical challenge in the CESS is indeed important for the service to be utilized. Previous research has emphasized the importance of taking emotions seriously when reflecting on ethical challenges. 29 The role of emotions in ethics has been discussed extensively. Traditional rationalistic normative ethics theories, such as utilitarianism and Kantianism, have been criticized by care ethicists for neglecting the role of emotions. 30 This has also been a critique of some reflection models, including the CME model. These models may be experienced as having merely a rationalistic view on ethical challenges, and that they do not take emotions into account in ethical reflection. However, we will argue that the model indeed makes room for emotions, if the facilitators are open to it. In particular, emotions may have a place in step 3, “Parties involved in the case and their views and interests.” Here, the school nurse’s own assessment of their situation and their emotions is highly relevant. While it may be emotionally challenging to share ethical doubts, research also show that ethics support, like ethics reflection groups, may help participants in dealing with emotions, and may even lead to a deeper learning process and a deeper deliberation. 29 Moreover, we may need a systematic and rational model so that emotions do not overshadow our reflections, and to help us not becoming emotionally overloaded. Here we think it is important to strike a balance between the emotional and the rational. In order to deal with emotions within a group, a sense of security and comfort within the group is required. This again means that how emotions are dealt with depends on the one who facilitates the group. In our project, the facilitators facilitated the same group through all the sessions. Being dependent on a permanent facilitator makes the reflection groups more vulnerable. Here a solution could be for group members to take turns in facilitating. This could also lead to all the group members assuming a greater responsibility for successful reflections. However, having one facilitator who has the main responsibility for the facilitating will also secure stronger competence over time.
Conclusion
Clinical ethics support such as ethics reflection groups may be both challenging and helpful for healthcare workers, as they often need rapid solutions. However, both our findings and previous research indicate that ethics reflection may lead to better self-confidence and better solutions. What may be of great importance is to further develop existing ethics supporting tools, and tailor the activities to the specific needs and working conditions of the group. There is also a need of more research into the field.
Strengths and weaknesses
One weakness with this study was the time frame. The school nurses tried out ethics reflection as a method during a project which only lasted a year. When the project period was over, the participants could decide themselves if they wanted to continue with the ethics reflection groups or not.
One of the main goals with ethics reflection is to improve practice and healthcare. From our study, we do not know if the care recipients themselves experience a better practice, only that the school nurses report that ethics reflection may lead to better solutions. To get to know how ethics reflection may impact the care recipients, we need more research, and research with mixed methods.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by University of Oslo (norsk: Helse og omsorgsdepartementet).