
Abstract
Background:
Eating disorders are serious conditions which also impact the families of adult patients. There are few qualitative studies of multifamily therapy with adults with severe eating disorders and none concerning the practice of therapists in multifamily therapy.
Objectives:
The aim of the study is to explore therapists’ practice in multifamily therapy.
Research design and participants:
A grounded theory approach was chosen. Data were collected through participant observation in two multifamily therapy groups and qualitative interviews with the therapists in those groups.
Ethical considerations:
The study conforms to the principles outlined in the Declaration of Helsinki. All participants in the multifamily therapy groups received information about the research project and signed consent forms. The data are treated confidentially and anonymised.
Findings:
The core category was identified as ‘having many strings to one’s bow’, consisting of three subcategories: ‘planning and readjusting’, ‘developing as therapist and team’ and ‘regulating the temperature of the group’. This article discusses the empirical findings in the frame of Aristotelian virtue ethics.
Keywords
Introduction
Eating disorders are difficult and expensive to treat, and 20%–30% of patients develop a chronic condition. 1 –3 Anorexia sufferers have a mortality between 1.85% and 5.9%, the highest of any mental illness. 1,2,4 –6
A family with an eating disordered member is much affected 7 and under considerable strain. 8 –13 De la Rie et al. 12 studied caregivers in such families and found their quality of life to be lower not only than that of caregivers in normal families but also than that of caregivers in families of patients with other mental illnesses. Worry and anxiety dominate the emotional responses of family members of someone with an eating disorder. Families are organised and steered by anxiety for the condition. This can lead to the development of maintaining and change-inhibiting behaviours. 14,15
Multifamily therapy (MFT) was developed in the 1960s for the treatment of psychosis, substance abuse and developmental disorders. 16 MFT has been adapted 17,18 for the treatment of eating disorders, specifically anorexia nervosa in children and adolescents. This work is described in English 14,19,20 and German literature. 21 –23 Manuals 17,24 are available with respect to this work. Similar work has been done in Scandinavia since 2005. 24,25 At the Maudsley Hospital, MFT has been developed to include the families of adult sufferers of eating disorders. 9,10 More recently, Toronto General Hospital in Canada has developed a model of MFT for adult patients. 26 –28 In the United States, MFT for adults is described in a qualitative study. 29
The Regional Centre for Eating Disorders (RESSP) at Nordland Hospital in Bodø, Norway, has developed a new model and a handbook for the treatment of young adults (18–30 years) with severe eating disorders. 30 In this model, the families of patients are actively involved in a treatment programme over approximately 12 months. The RESSP model can be considered ground-breaking, unique in its form and extent. 25 The MFT programme at RESSP is offered to families with an adult member suffering from a severe eating disorder (anorexia or bulimia) who has not yet established an own family. Six to eight families participate in six gatherings (each 2 or 3 days, 13 days in total) over the course of a year. Ten such groups have been run since 2006. These MFT groups are led by two group leaders and a multi-disciplinary team of co-therapists.
While studies 19,31 –33 indicate that MFT is effective in treating children and adolescents, there have been few studies regarding MFT for severely eating disordered adults 9,10,27 –29 and most are quantitative. Goodsell and Whiting 34 suggest research following Aristotelian theory, such as observational research, participant observation studies or grounded theory studies exploring processes in families. The literature relating virtue ethics to professional practice is largely philosophical. 35,36 We have not found empirical studies on therapists’ practice in MFT, nor in conjunction with virtue ethics. This article explores MFT therapists’ practice. The principal findings are discussed in the frame of Aristotle’s virtue ethics.
Methodological approach
A grounded theory (GT) approach was chosen. GT is a means of deriving theory from empirical data. One considers the patterns emerging from the data and constructs theory, using the constant comparative method. Data collection and analysis take place in parallel. 37 –44
Study setting, participants and data collection
The MFT programme comprises six group gatherings (each 2–3 days) over the course of 12 months. The frame of MFT is based on various group settings and includes a variety of methods of intervention, such as role play, family mapping, sculpture and other creative work.
Relevant and important themes are highlighted, both through psycho-educational sessions and clinical group work. Issues such as relationships, interaction, communication, conflict management, motivation and feelings of guilt are addressed during the gatherings.
The data comprised approximately 180 h of field observations in two MFT groups.
Data collection was carried out by B.S.B. between 2015 and 2017. Twelve young women (18–22 years, eight with anorexia and four with bulimia), 12 sets of parents (mother and father), eight sisters, one brother, one grandmother and two partners participated in the two MFT groups. Most patients in the MFT groups were treated in community-based clinics, but some were residential patients.
B.S.B. also conducted fieldwork in planning, ongoing evaluation and supervision meetings for the therapists and in a 1-year (about 80 h) group-meeting-based training for therapists.
Fieldwork in the MFT groups was carried out with B.S.B. present as an ‘ordinary participant’, taking part in group activities on more or less the same basis as the other participants, while writing contemporaneous field notes.
Data collection also included qualitative interviews with the therapists involved in MFT (Table 1). Ongoing fieldwork and analysis steered the content of these interviews.
The MFT therapists – ‘the Multi-octet’.
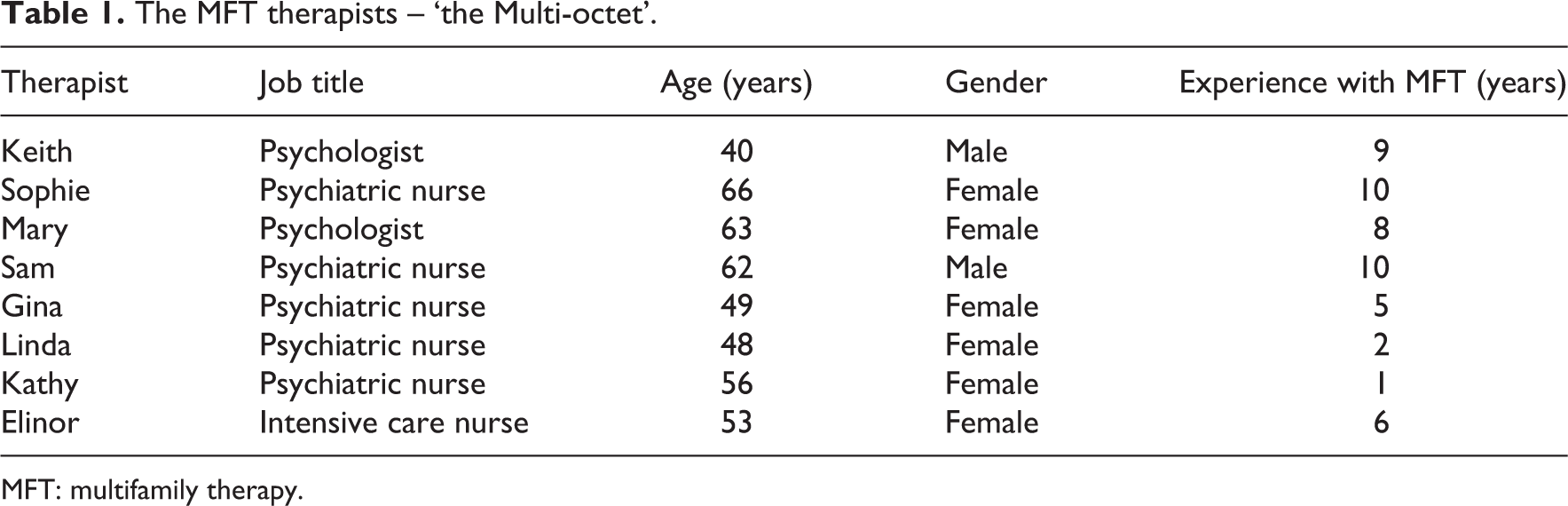
MFT: multifamily therapy.
Data analysis
Data analysis in GT consists of open, selective and theoretical coding, together with memo and theory writing. 37 –44
Field notes and qualitative interviews with the therapists were coded and analysed in parallel with data collection. Transcripts were read line by line and analysed several times using the constant comparative method. Memos were written and sorted. The point with GT is development of theory. One looks for patterns – what is this about, who is involved and what strategies are being deployed?
It is usual in GT that the ongoing analysis steers the sampling and data collection. This is called theoretical sampling. 37,45 Ideally, the researcher selects informants and new areas (incidents) for data collection, based on the results of the ongoing analysis. This can include new groups of informants that were not defined or selected in advance. In studying MFT, there were a set schedule for the meetings, with respect to the patients, their families and therapists; B.S.B. chose to participate in all the meetings, even though data collection is supposed to stop when a saturation point is reached.
Strauss and Corbin 45 discuss the different sampling techniques used in GT. When the researcher does not have unlimited access to persons or informants, the ideal form of theoretical sampling can be difficult to carry out. Sometimes researchers have to accept the data they are able to acquire. Even so, the comparisons are made on the basis of concepts during the analysis. ‘As with all research, there is the ideal way of conducting a study and the practical way (or that for which one has to settle)’. 45
Research ethics
The study conforms to the principles outlined in the Declaration of Helsinki. The research project was approved by Regional Committee for Medical and Health Research Ethics (REK; reference 2014/1621/REK vest). In addition, all participants in the MFT groups received verbal and written information regarding the research project and signed consent forms. The data were treated confidentially and anonymised.
Findings
MFT for adults focuses not on food and the treatment of symptoms but rather on communication and relationships within the families. These patients are adult and must themselves take responsibility for eating. The main concern in MFT for adults with severe eating disorders is how one can establish improved communication and interrelationships in the families, so that they can become better equipped to be supportive of the young person as they get better and move towards recovery, independence and separation from their family of origin.
‘Having many strings to one’s bow’
‘Having many strings to one’s bow’, with its subcategories ‘planning and readjusting’, ‘developing as therapist and team’ and ‘regulating the temperature of the group’, explains how the therapists in MFT try to solve the main concern and improve communication and cooperation among the families. The subcategories partly overlap and refer to parallel processes while ‘having many strings to one’s bow’.
The English expression, ‘Having many strings to one’s bow’, implies multiple options, versatility or resourcefulness. Its original meaning refers to an archer’s bow, but it can also be related to the bow used to play an instrument, such as a violin. Here, we relate it to the musician making music with the ‘many’ strings of his instrument. In the very first session observed, the therapists gave themselves the name ‘the Multi-octet’. They use themselves as instruments, and in doing so can be thought of as a kind of orchestra in which the conductor, leader and musicians ‘play on their many strings’. The therapists have a large repertoire to draw on. They improvise and use different instruments and scores when they make music together. And, importantly, the young women and their families must be included in this orchestra. In MFT, the whole orchestra selects scores, instruments and music that they like to play; there should not be just solos from individual therapists or from the therapist team.
‘Having many strings to one’s bow’ includes reading and understanding the group process. One needs to change position and perspective all the time, from wide angle to narrow focus, and to see the whole group, as well as each family and each individual. Meta-perspective and overview are more important than preoccupation with detail; being active, not too laidback, loosening, changing, making safe, discussing, sharing, deploying resources, summing up, producing inspiring words and creating space for feelings and pain. Also, teaching, imparting knowledge, accountability, awareness, tidying up, offering affirmations and making the content applicable to all: To bring out the unique capabilities that each family has, and the abilities emerging from the interaction between the families is probably the most special thing. (Sophie) Using yourself as an instrument, a clear, clean tone. Sometimes you are restrained, at times more to the fore, at times a soloist and at times playing quiet parts. (Sophie) We have been given some chords, but none of the notation – and none of us knows what the melody will be until we start to play – we just take it from there. (Elinor) I have no idea where it comes from; before, there was just technique. (Mary) Something a bit magical happens between them. (Linda) The things that happen right there and then, some in the big group, some with the mothers, some with the girls. They encourage each other. There is a synergistic effect in this. You get life in the here and now, you get relating. It’s not often as a therapist that you have the opportunity to be with people in the here and now. Quarter of an hour in such circumstances can be more meaningful than twenty hours of individual therapy. It is something particularly rewarding. (Mary)
‘Planning and readjusting’
‘Planning and readjusting’ means bringing together and constructing the MFT group and therapist team and planning, changing and altering the content in the light of the pulse and temperature of the group: We never know where we will end up. (Sophie)
In the planning phase, the MFT team meets often. It is helpful to have variety and interdisciplinarity, both more and less experienced therapists. There must be sufficient therapists, at least one per family, and the members of the team must be able to work together, help and complement each other. That some have a background in nursing is also important through an ability to understand physical symptoms, the somatic, blood test results and acute physical reactions.
In planning for the group gatherings, weight is given to a good structure contributing to the creation of a secure framework for good discussion. One wishes to create an arena supportive of development and growth, to create a frame for the process, ‘like a playpen, with a frame around it, a safe environment’ (Sophie). The planning is thoroughgoing, but loosely structured. Things are never as planned, but look as if they were to the participants. The therapists have with them a ‘toolbox’ of different techniques, but they must also have a considerable capacity for flexibility, to be able to trust themselves and the group and to change direction. They have frequent ad hoc meetings to adjust the content in light of the group process. The adjustments and changes flow from a joint understanding, even during a single session, on account of the temperature of the group: Orientating towards what is happening in the group rather than putting forward a theme in a particular way…It is more about how it is being received than with what is being put out. (Keith)
‘Developing as therapist and team’
‘Developing as therapist and team’ involves using yourself as an instrument, and being good as your own instrument, together with finding your place in the team/orchestra. Beyond that, it means developing yourself to bring out the best in yourself and in the team. Ongoing self-development enables one to go further in relation to both individuals and families. It involves being in the here and now, being able, as a therapist, to tolerate more even though that is not always pleasant. There must be unease if the family patterns are to change: Experience has taught me that it’s not so dangerous, we come out of it in one piece. (Sophie) As a therapist, you cannot help others to go further than you have dared to go into yourself. (Sophie) We are the safe-making ones. (Elinor)
Teamwork in the MFT orchestra also concerns the ability to engage in interplay with fellow therapists: You meet so few people during your career where you can think a thought and he will think the rest. Maybe it’s him who starts the humour, but then I think of something amusing and keep it going. There are so few people that one can have that with. (Mary)
‘Regulating the temperature of the group’
‘Regulating the temperature of the group’ involves facilitating the group process such that the climate of the group is therapeutic. The temperature, or pulse, is a measure of the energy level in, and level of engagement of, the group. It is not static but is always changing. It should not be too warm, but neither too cold, and not too relaxed; with sufficient drive, tension, challenge, unease and small crises such that there is always material to work with. One must take care that there is no ‘crash’ between the theme taken up and what is happening in the group. The therapists help the group to ‘tune in’ to the theme being presented. One also balances the needs of the group and those of the individual group members and the families. The therapists follow the group and are spontaneous in response to the group’s process. If things go flat or become too theoretical, one looks to find a connection to where the participants are.
Humour, used rightly, is a strategy or device contributing to the regulation of the group’s temperature. Humour implies the ability to be playful and have an informal style while retaining a seriousness and earnestness of purpose: Amidst all the seriousness it is possible for them to see, and to work on, themselves with a degree of playfulness. This maybe sounds a little strange, as if one is not taking things seriously. But humour relieves part of the tension, so that it is easier to address difficult matters. (Sam) These girls take everything extremely seriously. They lack a gene – the ‘don’t-give-a-fig’ gene. (Sam)
Temperature regulation also involves the creation and management of small crises. This is done by addressing difficult themes, putting ‘on the table’ things that one is observing and taking note of in the group, the way in which one asks questions about and invites expansion of things shared in the round (pulse). An example of such a crisis could be that one of the young women feels herself to have been exposed in the main group, giving rise to many emotions and leading to the young woman running out in tears. There must be sufficient discomfort in the group and a sufficient temperature – it is then that there is room for growth. The whole time is balancing between building up and soothing down.
Concluding discussion
In this article, we decided to present the main findings in the context of Aristotle’s virtue ethics. Aristotle was the first to write a philosophical work, the Nicomachean Ethics 46 in which ethics is a discrete subject, and many of his thoughts continue to be relevant to contemporary ethics debate. Rather than starting from universal principles where we act according to moral rules (deontological ethics), or from maximising the best consequences of our actions (utilitarian ethics), virtue ethics starts with the agent’s life and asks how we should live our lives. ‘Ancient ethical theories are concerned with the agent’s life as a whole…concern with character and choice, with practical reasoning and the role of the emotions’. 47 This leads to a reflection on what the good life is and what ‘human flourishing’ consists of. Although we agree that the final end or telos that we seek is happiness, there are many opinions as to what constitutes happiness. Yet Aristotle argues that virtues are necessary components of happiness, and that human flourishing consists of being virtuous in accordance with reason. 48 ‘Aristotelianism provides a coherent framework for social science research and the study of families that includes virtues, values, goals and “the good” in relationships’. 34 We believe that the focus on the agent’s view of her life, the role of emotions and the reflection on human flourishing provides virtue ethics with resources that are particularly suitable for therapists in an MFT setting.
In moral philosophy, virtue is an aspect of character that affects moral attitude and actions. It concerns personal qualities which enable a person to behave morally and well. Radden 49 argues that ‘…psychiatric practice introduces extra challenges for the application of virtue ethics that do not arise…with the same force, in other professional practices’. Which qualities and virtues are important for the therapists in MFT?
Instrumental rationality is the dominant mode of thought in our time, the focus most often on the aim and outcome of our actions. Practice is the term for human activity where the aim is not primarily a product. Talking together, playing a musical instrument, dancing or satisfying physical needs are activities or processes which are ends in themselves. MFT for adults with serious eating disorders can also be considered a kind of practice where the process is as important as are the aims of MFT. We have likened MFT to an orchestra, in which the therapists, patients and their families create music together. In this way, MFT practice represents the full range of human possibilities; sometimes joyful but not always so. It is about coping with life; encountering and dealing with different life situations.
The MFT orchestra ‘have many strings to their bow’. During the MFT process, the therapists deploy many different strategies. Some of these can be described as moral virtues, in line with Aristotle’s thinking. The role of the therapist involves mastering different techniques (toolbox), but more so personal qualities. Annas
48
discusses the relationship between skills and virtuous actions. Paine et al.
50
differentiate clinical skills and therapeutic virtues. ‘Virtue is a term in reference to what sort of person the clinician is becoming rather than what skills they are proficient in’. ‘All virtues are supported by skill building through habitual action’.
50
Virtues are developed with experience and practice, through the repetition of patterns of behaviour and using others as models.
46
The therapists use themselves as instruments and must train and practice to be the best they can as their own instrument: …but the virtues we get by first exercising them, as also happens in the case of the arts…we become just by doing just acts, temperate by doing temperate acts, brave by doing brave acts. (NE II 1, 1103a32-b2)
The therapists have to work with crises in the group, contributing to the development of individuals and families. The young women, family members and therapists alike often reported that they enjoyed participating in MFT and found the atmosphere there agreeable. Again, balance is important. It should be neither too pleasant, nice nor relaxed. A suitable temperature in the group should be the golden mean between too hot and too cold. The therapists must be confident and brave enough to tolerate unease. They must not be faint-hearted. Virtues come from the encounter with new situations and through meeting crises with neither too much nor too little anxiety. 46 In this way, possibilities for change and growth are created, necessary if the participants in MFT are to break out of stuck and self-maintaining patterns of family behaviour.
We have seen how therapist Sam constantly maintained a balance while using humour, and that humour used rightly into the right degree and at the right time could contribute to regulating a difficult atmosphere in the group. Excessive use of humour, however, could leave the group flat, and it is important not to use it to draw the sting of all that is difficult. Besides, humour can be taken in different ways; while some find it disarming and liberating, others can feel discomforted or hurt. We have not found empirical research that considers humour used in therapist–patient encounters in the light of virtue ethics. Schöpf et al.
51
consider humour to be relationship building and relationship protecting. McCreaddie and Wiggins
52
distinguish between unproblematic and problematic humour. Gulliksen et al.
53
found that two characteristics of therapists most appreciated by patients with anorexia nervosa were vitality and humour. We regard humour as a therapeutic virtue, which Sam has a particular mastery of. It is essential that humour be used with sensitivity: Those who carry humour to excess are thought to be vulgar buffoons, striving after humour at all costs, and aiming rather at raising a laugh than saying what is becoming and at avoiding pain to the object of their fun; while those who can neither make a joke themselves nor put up with those who do are thought to be boorish and unpolished. But those who joke in a tasteful way are called ready-witted, which implies a sort of readiness…(NE IV 8 1128a5-11)
Virtues are aspects of character or personal qualities which enable a person to behave morally and well. It is commonplace to consider virtues at the level of the individual. Aristotle
46
claims that human beings are by nature social or societal beings. MFT is concerned not only with the individual but equally with teamwork and the group. Within MFT, therefore, it is as relevant to speak of team virtues as of individual virtues. Teamwork in the MFT orchestra requires each individual therapist to play on ‘the many strings of their bow’. At the same time, the therapists must play together. It concerns finding the right tone, in the right place and at the right time: …to feel them at the right times, with reference to the right objects, towards the right people, with the right motive, and in the right way, is what is both intermediate and best, and this is characteristic of virtue. (NE II 6 21b-23) Softly and tentatively the adagio begins. In the background violins reply, the piano is questing, oboes and flutes join in, more strongly, assured, the sound of the piano comes to the fore, the orchestra is quiet, the strings keep the rhythm, the wind instruments respond. Now, the rondo comes to the fore, and the piano emerges, stronger and more striking chords, accompanied by the whole orchestra. (Freely translated after Lohne
54
)
Footnotes
†Dedication
The third author, Mildrid Elisabeth Valvik died before completing the article. We wish to dedicate this article to Mildrid Elisabeth Valvik, “In memory of Mildrid Elisabeth Valvik”.
Acknowledgements
The authors wish to thank professor Erik Christensen, Nord University for his kind and insightful help with Aristotelian virtue ethics. All authors, except C.M., contributed to the research design. B.S.B. collected data from participant observations and qualitative interviews, performed data analysis and drafted the manuscript. M.E.V. drafted the first version of the introduction. C.M. participated in data analysis. All authors provided comments on the manuscript, and all, except M.E.V., read and approved the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.