
Abstract
Objectives
Although cervical cancer screening guidelines in France recommend a smear test every three years, many physicians order more regular screening. We aimed to assess the benefits or harms of shorter intervals between screenings, both for women and public health.
Methods
For a retrospective cohort of women aged 25–65 who had two normal smears and at least one additional smear, data were sourced from a regionally organized cervical cancer screening programme in France, with follow-up for nine years. Based on the interval between the second and third smear, two groups were formed; the first comprised overscreened women (interval <24 months), and the second of ‘correctly’ screened women (interval between 24 and 42 months). The primary outcome was cervical intraepithelial neoplasia 2 or worse (CIN2+); secondary outcomes were cervical cancers and CIN1 lesions.
Results
Among 63,821 women, CIN2+ incidence rate per 10,000 women per year was 14.5 for 40,350 overscreened women, and 11.5 for 23,471 correctly screened women. Age-adjusted relative risk was 1.22[1.02; 1.46]. We found no significant difference for cancer (RR = 1.39; 95%CI = [0.60; 3.61]), but did find additional CIN1 in the overscreened group (RR = 2.09; 95%CI = [1.76; 2.51]).
Conclusions
A shorter interval between smears has a low benefit for CIN2+ lesion detection, which may not help avoid cancer. The excess number of CIN1 detected by overscreening may cause needless risk and excess costs due to overtreatment.
Introduction
Since 1990, the recommended screening interval for cervical cancer screening in France has been once every three years, after having two normal smear results at least a year apart.1,2 Despite these guidelines, many clinicians perform screening annually, even after two normal smears. In France, regularly monitored women aged 25–65 (who have a smear at least once every three years) are generally overscreened, with an average interval between screenings of 24 months (median = 22.3 months). A 2007 paper by the French National Institute of Cancer estimated that only 15% of women are screened every 2.5 to 3.5 years, 3 and in an Australian survey, the early rescreening rate was estimated at 15.3% of women who have a cervical smear test. 4 Resistance to less frequent screening may be due to a perception that the danger of cervical cancer presents an excessive risk, 5 but this overlooks the risk of treating an overscreened patient with, for example, a spontaneous regressive lesion, and the likely additional cost of annually repeated smears. 6
Many studies have analysed the screening interval impact,7,8 and there is great diversity among European guidelines, ranging from annual screens (e.g. Germany, Austria) to every five years (e.g. Finland, Netherlands, Northern Ireland), 9 although European guidelines advise screening no more than once every three years. 10 Frequency of screening for those with only negative tests remains an open question, especially for clinicians.
In Alsace, in spite of organized cervical cancer screening, we suspect many women may be overscreened. This study aims to estimate the benefit of overscreening in terms of increased detection of cervical intraepithelial neoplasia (CIN)2+ and to assess whether a shorter interval between smears presents a benefit for screening participants and for public health by reducing cancer incidence, and also to illuminate possible harms, due to overtreated patients attributable to increased CIN1 detection, and/or excessive cost for public health.
Methods
We analysed data from the EVE Association, a French regional programme for organized cervical cancer screening. With the approval of the ‘Commission Nationale de l’Informatique et des Libertés’ (the French data protection authority), this association collects results from cervical smears and further examinations (e.g. biopsy, conization, and curettage) from women aged 25–65 living in Alsace. These data are sent directly from pathologists and physicians who perform the examinations. The Alsatian database used for our study has existed since 1994 and collects all smear results from regional and neighbouring laboratories (public and private). For each abnormal smear, a questionnaire is sent to physicians to determine whether further examinations are performed and to obtain histological results. Since 2007, all histological examination results of the uterine cervix have also been provided to the database by laboratories.
To enhance reliability, Eve data were compared with that from the two departmental cancer registries, 11 allowing for complete cancer ascertainment, including for diagnoses made after the onset of symptoms and smear-free biopsies. Participants were informed about the collection and use of data by flyers and posters in physician waiting rooms, reminder letters, and pathological prescriptions, and may refuse collection of their data by contacting the EVE association. Those who opted out of data collection represent less than 2% of the subjects. This study was non-interventional and did not require the agreement of the Comité de Protection des Personnes (Ethical Research Committee).
Eligible women were those who lived in Bas-Rhin, who were aged 25–65 at their first smear and had had two normal smears and at least one additional test. We selected those whose second smear was performed between 1 January 1998 and 31 December 2002. We excluded women with an interval of 43 months or longer between the second and the third smear, to ensure that only well-monitored subjects were included.
The interval between the second and the third smear determined to which of the two groups participants were assigned, the first group comprised overscreened women (interval <24 months) or the second group comprised those screened at the recommended interval of 24–42 months. To minimize misclassification, we also excluded women whose screening interval from the third smear until the last normal or the first abnormal smear was not either (i) consistently shorter than 24 months (for the first group), or (ii) between 24 and 42 months (for the second group) (Figure 1).
Flow chart.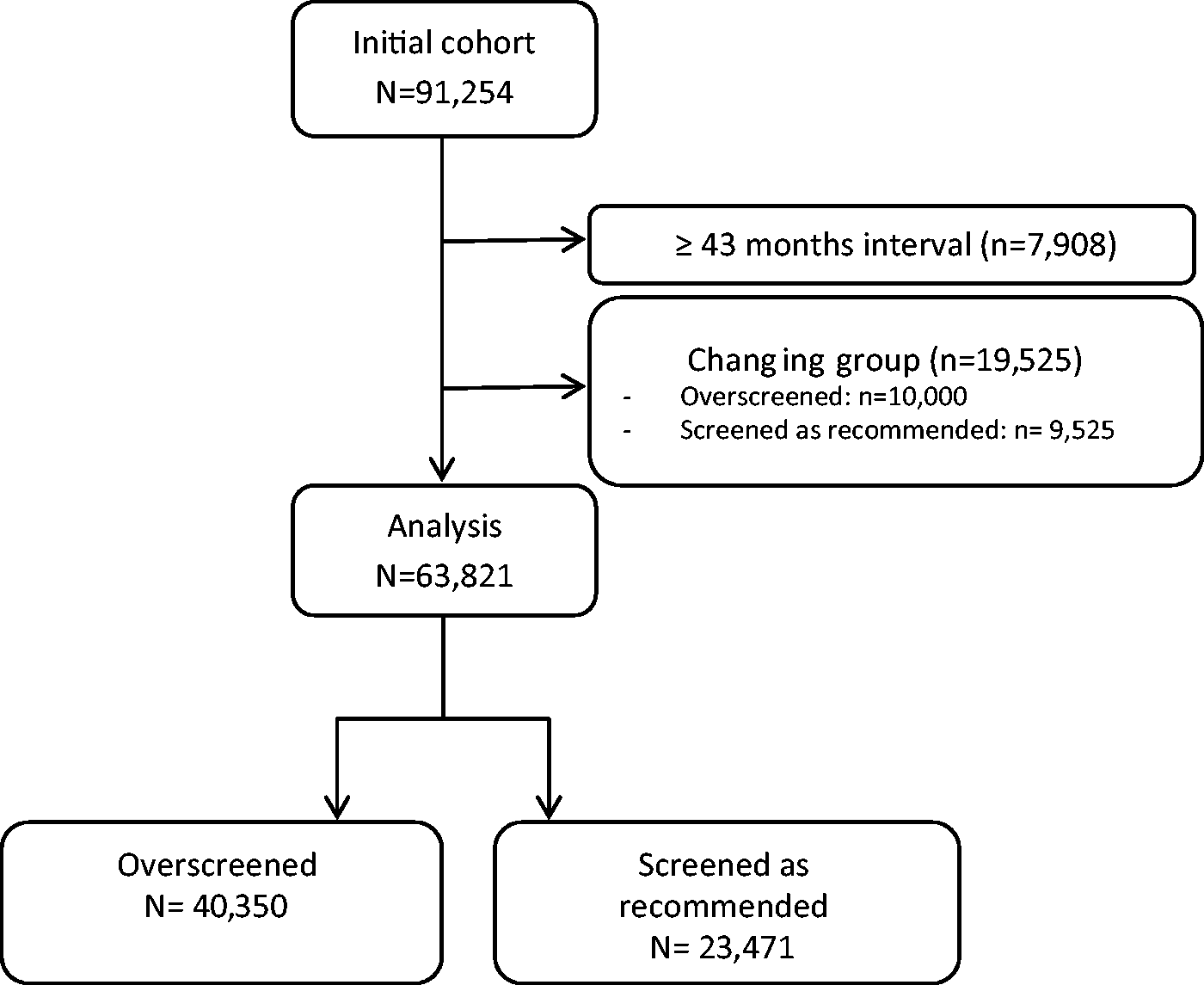
In this retrospective cohort, we collected data on smears (up to 12 per subject) and other examination results (up to 10 per subject) up to 31 December 2011, to allow up to nine years of follow-ups from the second smear. The primary outcome was the occurrence of CIN2+12,13 and secondary outcome was cervical cancer and CIN1 lesions. We also conducted an exploratory study to estimate additional costs.
CIN2+ incidence rates were estimated in each group. The follow-up time was defined from the second smear to the last screening observation or the occurrence of CIN2+. We used a log-linear model with adjustment for age to estimate the relative risk (RR) of CIN2+ diagnosis. Interaction between age and group has been checked, as well as the analysis of the cervical cancer incidence. To study CIN1, we used the same methodology, but patients with CIN2, CIN3, or cervical cancer were excluded, so that only subjects without precancerous lesions were selected. For example, patients with CIN1 that progressed to CIN2+ were considered as CIN2+ and excluded from the CIN1 study.
To determine cost difference between the groups, we estimated the cost that the CIN1 study subsample would have incurred if it had had the same rate of smears and examinations as the overscreened group. We calculated the difference between this estimation and the observed cost, to provide an estimated additional cost figure. We estimated the price of each examination using the rate of the French public health system: smear 15.40€, biopsy 27€, colposcopy 37.20€, loop excision 185.36€, and destructive treatment approximately 46€.
Analysis was performed with R 3.1.1.
Results
Group characteristics.
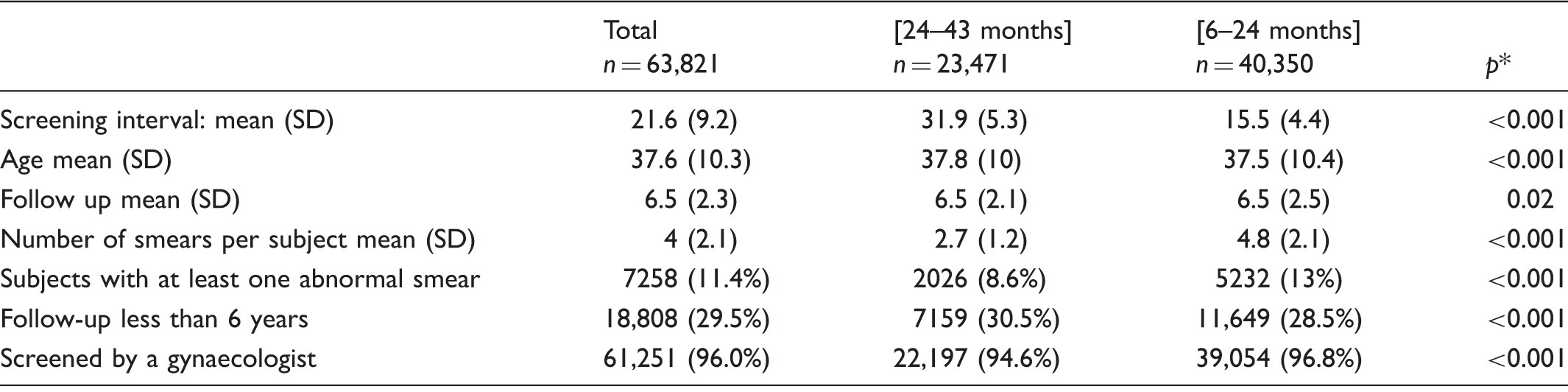
SD: standard deviation.
p values obtained with two sample Wilcoxon tests to compare mean and with χ2 test to compare percentage (α = 5%).
Number and proportion (per 1000 subjects) of histological lesions according to screening interval.
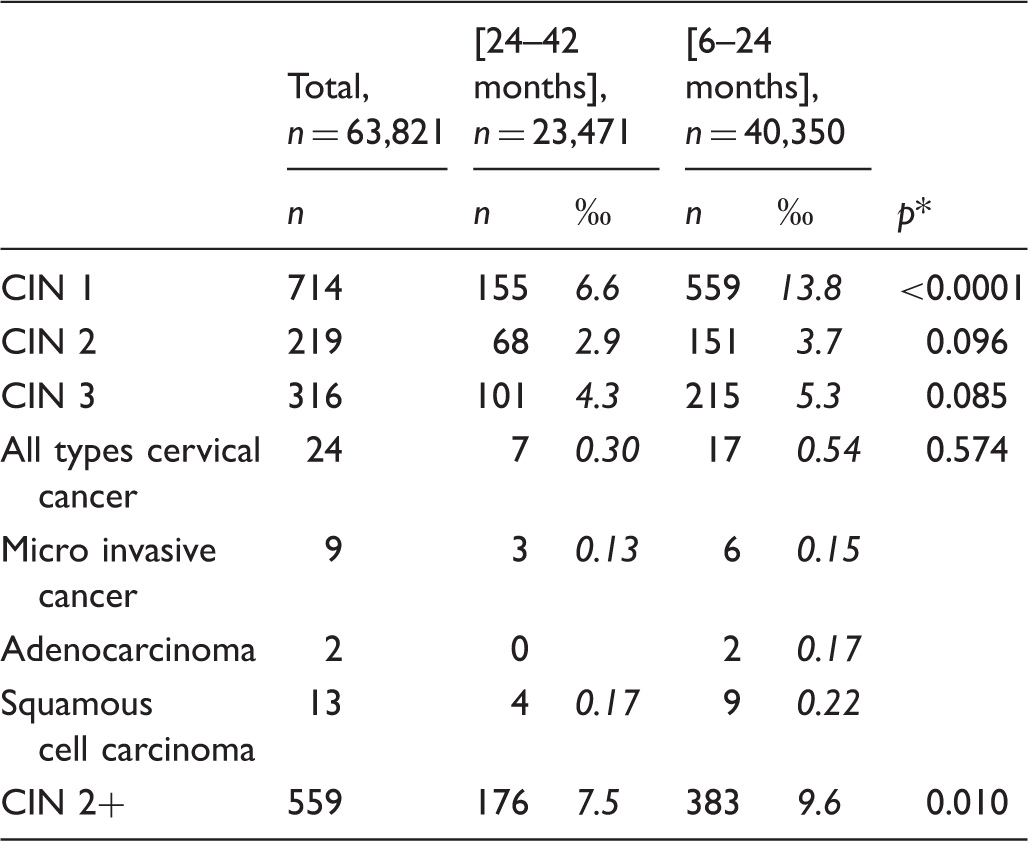
CIN: cervical intraepithelial neoplasia; CIN 1: cervical intraepithelial neoplasia that did not progress during the study period; CIN 2+: cervical intraepithelial neoplasia grade 2 and more (CIN 2, CIN 3 and cancers); CIN 3: CIN 3 and adenocarcinoma in situ.
p values obtained with a two sample χ2 test (α = 5%).
Primary finding
CIN 2+ incidence and relative risk according to age.

RR: relative risk; CI 95%: 95% confidence interval; CIN 2+: cervical intraepithelial neoplasia grade 2 and more (CIN 2, CIN 3, adenocarcinoma in situ and cancers); IC 95%: 95% intra-class coefficient.
Secondary findings
The difference between the incidence rate of cervical cancer per 10,000 subjects per year in the two groups, 0.64 [0.38; 1.00] in the overscreened group and 0.46 [0.20; 0.89] in the other group, was not significant. Age-adjusted RR of cancer was 1.39; 95%CI = [0.60; 3.61] (p = 0.46). As shown in Table 2, we found three micro invasive cancers (0.13%) in the group screened according to guidelines, and six (0.15%) in the overscreened group (p = 1). For invasive cancer (adenocarcinoma and squamous cell carcinoma), we found four (0.17%) and 11 (0.39%) cancers, respectively. This difference was not significant (p = 0.59). There were no interactions between age and cancer. On the third screen, cancer was diagnosed for five overscreened women and two women screened according to guidelines.
Incidence rate of CIN3+ per 10,000 subjects per year was 8.8 [7.7; 10.0] in the overscreened group, and 7.1 [5.8; 8.5] in the group screened between 24 and 42 months. Adjusted RR of CIN3+ was 1.20; 95%CI = [0.96; 1.51] (p = 0.12).
CIN 1 incidence and relative risk according to age.

RR: relative risk; CI 95%: 95% confidence interval; CIN 1: Cervical intraepithelial neoplasia grade 1; IC 95%: 95% intra-class coefficient.
Discussion
The aim of screening is to reduce the rate of cancer incidence and mortality. Our study demonstrated that cervical smear testing at intervals shorter than guidelines resulted in a significantly higher detection of CIN2+ and CIN1 but without any accompanying reduction of cancer incidence. Increased CIN2+ detection with a shorter screening interval did not reduce the rate of cancer, or even invasive cancer. Moreover, despite increased CIN2+ detection, there was no increase in the rate of micro-invasive cases among cancers detected – of interest because rapid discovery of micro-invasive cancers could reduce mortality with early care. There was no significant difference between groups in time to cancer diagnosis after the index screen (whether cancer was diagnosed on the third or on subsequent screens).
Unexpectedly, we observed a non-significantly higher cancer incidence among overscreened women, which we believe is likely due to sampling. With both the long follow-up and number of repeated smears with two normal results to be included on one hand, and the small number of cancers in both subgroups on the other, it is unlikely to be a detection bias due to imperfect cytology sensitivity. Nevertheless, the higher cancer incidence among overscreened women, although not significant, reinforces the statement that overscreening does not protect against cancer.
As our study only included patients with two normal smears, and because the outcome is mainly based on 2.7 or 4.8 subsequent repeated smears during the 6.5 follow-up years, we expected a rather limited impact from false negative smears. International guidelines that recommend three-year intervals between smears are based on a mean progression time from high grade CIN to cancer of 10 to 15 years, making it possible to perform at least three to five screens. Although it could not be completely excluded that some cancers diagnosed at the third screen resulted following a double false negative smear result, we anticipate that the similar proportion of cancer diagnosed at the third screen in both subgroups, and the similar delay for cancer detection after the second normal smear indicate a rather limited comparison bias.
In the overscreened group, the proportion screened by a gynaecologist was significantly higher, although the difference was only 2%. As gynaecologists see patients for reasons other than cervical cancer screening (e.g. pregnancy, contraception, and hormone replacement therapy), they have more opportunities to take a smear. The high proportion of gynaecologists performing the smears in both subgroups (>94%) does not suggest a selection bias.
It is true that some invasive cancers should have been detected due to symptoms (bleeding or suspicious cervical aspect), and patients with symptoms are more likely to be registered with a shorter interval. However, the low incidence of invasive cancer in both subgroups, the high proportion of gynaecologists performing the smears, and the French guidelines which recommend direct colposcopy rather than a smear allow only a limited bias comparison.
An unanticipated finding was that cancer incidence among screened women was relatively low, particularly in the ‘correctly’ screened group. 14 This might have been because patients were selected after two normal smears. In a study by Boulanger et al., 15 60% of cancers were found in women who had never been screened, or who were screened with an interval longer than three years. In our study, there was no suggestion of additional safety because of shorter interval screening. Our data concerning cancer are likely to be complete because we compared these with data from regional registries.
Although there was a low total incidence of cancers, we did not find a decrease in adenocarcinoma and squamous cell carcinoma incidence, or any increase in micro invasive cases with a shorter interval. A follow-up of four European randomized controlled trials suggested that HPV-based screening provides 60%–70% greater protection against invasive cervical carcinomas compared with cytology. 14 This protection was not significant for squamous cell carcinoma but only for adenocarcinoma, probably because smears are less sensitive to detect glandular lesions. A Finnish study suggests that cancer risk can be more effectively reduced by focusing on the relatively small groups of non-attenders, and women with positive cytology but with no malignancy confirmed, than by introducing shorter intervals between screens. 16
Although it has been suggested that CIN2 could be considered as a benefit, and also that CIN3+ may be considered to be a better proxy for benefit, in this study, we followed the WHO 2013 guidelines and the new classification that recommend considering CIN2 and CIN3 together. Furthermore, we would emphasize that CIN3+ incidence was not significantly different between subgroups. We found fewer precancerous lesions with screening every three years. A plausible explanation could be that a portion of the CIN2 and CIN3 diagnosed could regress. As with CIN1, it has been estimated that 43% of CIN2 and 32% of CIN3 could regress on their own. 17 It may be hypothesized that the shorter interval in the overscreened group provides less opportunity for spontaneous regression before diagnosis, and consequently more opportunity for unnecessary treatment.
Our study confirms that excess smears result in overdetection of low-grade lesions, and especially of CIN1, which are not precancerous lesions, and which typically resolve without the need for medical intervention. Regardless of this, in France today 15% of conizations are ordered to treat CIN1. 3 As it has been suggested that cervical conization could be responsible for miscarriage or premature births,18,19 this unnecessary treatment may also be harmful.
Supplementary smears, further examinations, and treatment also generate additional costs.6,20,21 In our study, the cost associated with overscreening (including supplementary smears, management of abnormal findings, and treatment) was estimated at € 1,307,477, enough to finance half of a screening programme. Per screened patient, the annual cost associated with overscreening is three times higher than the cost of organized screening.
It has been suggested that a three year interval between smears will result in lower overall compliance. In our study, there were significantly fewer patients with a follow-up of less than six years in the overscreened group. This is perhaps due to better compliance, but the difference is relative (28.5% versus 30.5%) and may be explained by the longer time between smears, rather than patients forgetting to follow-up. An organized recall system would be likely to be more efficient than reducing the interval between smears.
Conclusion
Our results suggest that a shorter interval (6–23 months) between screens may not result in any decrease in cancer rates, even if it provides a low benefit for CIN2+ lesion detection. However, significantly more CIN1 are detected when screening interval is less than 24 months, the value of which is questionable. Despite the anguish of many clinicians, there is no argument to screen more often than once every three years.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.