
Abstract
Objectives
To determine whether a brief telephone support intervention could increase breast cancer screening uptake among lower socio-demographic women in Scotland, via eliciting and addressing barriers to screening attendance.
Methods
In a pilot randomized controlled trial, participants receiving a reminder letter for a missed screening appointment (February-June 2014) were randomized to four arms: No telephone call (control), Simple telephone reminder (TEL), Telephone support (TEL-SUPP), or Telephone support plus anticipated regret (TEL-SUPP-AR). Primary outcomes were making an appointment and attending breast screening.
Results
Of 856 women randomized and analysed on intention-to-treat basis, compared with controls, more women in the telephone intervention groups made an appointment (control: 8.8%, TEL: 20.3%, TEL-SUPP: 14.1%; TEL-SUPP-AR: 16.8%, χ2(3) = 12.0, p = .007) and attended breast screening (control: 6.9%, TEL: 16.5%, TEL-SUPP: 11.3%; TEL-SUPP-AR: 13.1%, χ2(3) = 9.8, p = .020). Of 559 women randomized to the three telephone groups, 404 were successfully contacted and 247 participated in the intervention. Intervention participants (ie. per protocol analysis) were more likely to make (17% versus 10%, χ2(1) = 7.0, p = .008) and attend (13% versus 7%, χ2(1) = 5.5, p = .019) an appointment than non-participants, but there were no differences in attendance between the three telephone groups.
Conclusions
A simple telephone reminder doubled attendance at breast screening in women from lower socio-demographic areas who had not attended their initial appointment, compared with a reminder letter only (odds ratio 2.12, 95% CI (1.2, 3.8)). However, contacting women proved problematic and there was no additional effect of telephone support or anticipated regret.
Introduction
Breast cancer is the second leading cause of cancer deaths in women in the UK. Screening is key to early detection. The UK Breast Screening Programme is a nationwide, free at point of delivery screening service, to which all women aged between 50 and 70 are invited every three years. Currently over three-quarters of invited women regularly attend screening, however, there is a clear socio-economic divide in breast screening uptake. In Scotland from 2010 to 2012, 62.8% of women in the lowest Scottish Index of Multiple Deprivation (SIMD) quintile (ie. the 20% most deprived areas) attended breast screening versus 81.0% in the least deprived quintile. 1
Our research is underpinned by the Health Belief Model. 2 This suggests that the likelihood of engaging in a particular health preventive behaviour, such as attending breast screening, is influenced by the perceived benefits of that behaviour in relation to the perceived barriers to carrying out the behaviour, alongside perceptions of risk and the severity of the targeted illness. Women express many barriers to attendance at breast screening, including personal factors (eg. anxiety, embarrassment, or fear of diagnosis), concerns about the procedure (eg. test efficacy, fear of pain), and practical difficulties in access to screening (eg. time off work, carer responsibilities, cost of transport).3,4 Lower socio-economic women appear more likely to express ‘passive’ barriers to non-attendance (eg. lack of perceived benefit and practical barriers to attendance), rather than making a calculated decision not to attend. 5 An Australian government report concluded that: ‘the benefits of screening need to be reinforced and women reminded that these outweigh the barriers, even though the downsides may seem more numerous and immediate.’ 5
Interventions designed to reinforce the benefits of and address barriers to preventive health behaviour have been successfully used to increase treatment adherence in a range of long-term conditions, including cardiovascular disease, diabetes, arthritis and stroke.6,7 A study investigating attendance at a rehabilitation programme aimed at preventing secondary cardiac events found that those whose concerns outweighed perceived necessity were less inclined to attend. 8 A recent telephone coaching intervention to address perceived barriers significantly increased uptake of breast screening in low-income women in the US, indicating that the negative influence of barriers to mammography uptake can be overcome. 9
Engaging in health behaviour, such as screening participation, is shaped by two distinct systems: 1) a reflective, rational, value-driven goal-oriented system, requiring cognitive capacity, and 2) an automatic, affective system, requiring little cognitive engagement, guided by immediate feelings and emotions. 10 Targeting emotions may be more effective at changing health behaviour in lower socio-economic groups. 11 Regret is one such negative cognitive-based emotion, experienced when we imagine that an outcome could have been better had we acted differently. We can also anticipate regret, and act to avoid this. Abraham and Sheeran 12 found that anticipated regret (AR) adds significantly to the prediction of intentions and prospective health behaviours, over and above the traditional attitudinal components of influential social cognitive theories such as the Theory of Planned Behaviour. AR has been shown to markedly increase attendance at cervical cancer screening in a simple questionnaire-based intervention. 13
We aimed to elicit and address barriers and facilitators to breast screening attendance in low socio-economic women via a brief, personalized, telephone intervention, with the objective of increasing screening uptake. We also tested whether asking questions about AR could further increase screening uptake. We employed four treatment groups of increasing intensity (usual care, plus telephone reminder, plus telephone support addressing barriers, plus AR), an approach demonstrated to effectively increase colorectal cancer screening. 14 We also examined whether this brief intervention was feasible and acceptable to low-income women.
Methods
We conducted a single-centre trial at the National Health Service (NHS) East of Scotland Breast Screening Centre in Dundee. Detailed methods are available in the published protocol. 15 The research was conducted in accordance with the Helsinki declaration (1975, revised 2000) and ethical approval was granted by Tayside NHS Board, East of Scotland Research Ethics Committee REC 1 (ref. no. 13/ES/0128), (trial registration: Current Controlled trials: ISRCTN06039270, 16 January 2014).
The simple, between-groups, four-arm prospective randomized controlled trial design targeted women due to be sent a reminder letter (ie. non-attenders at a scheduled appointment). The four groups were: Letter reminder (ie. Treatment as usual: control), Telephone reminder (TEL), Telephone reminder plus telephone support (TEL-SUPP), and Telephone reminder plus telephone support plus AR (TEL-SUPP-AR) (see Figure 1).
Consort Diagram.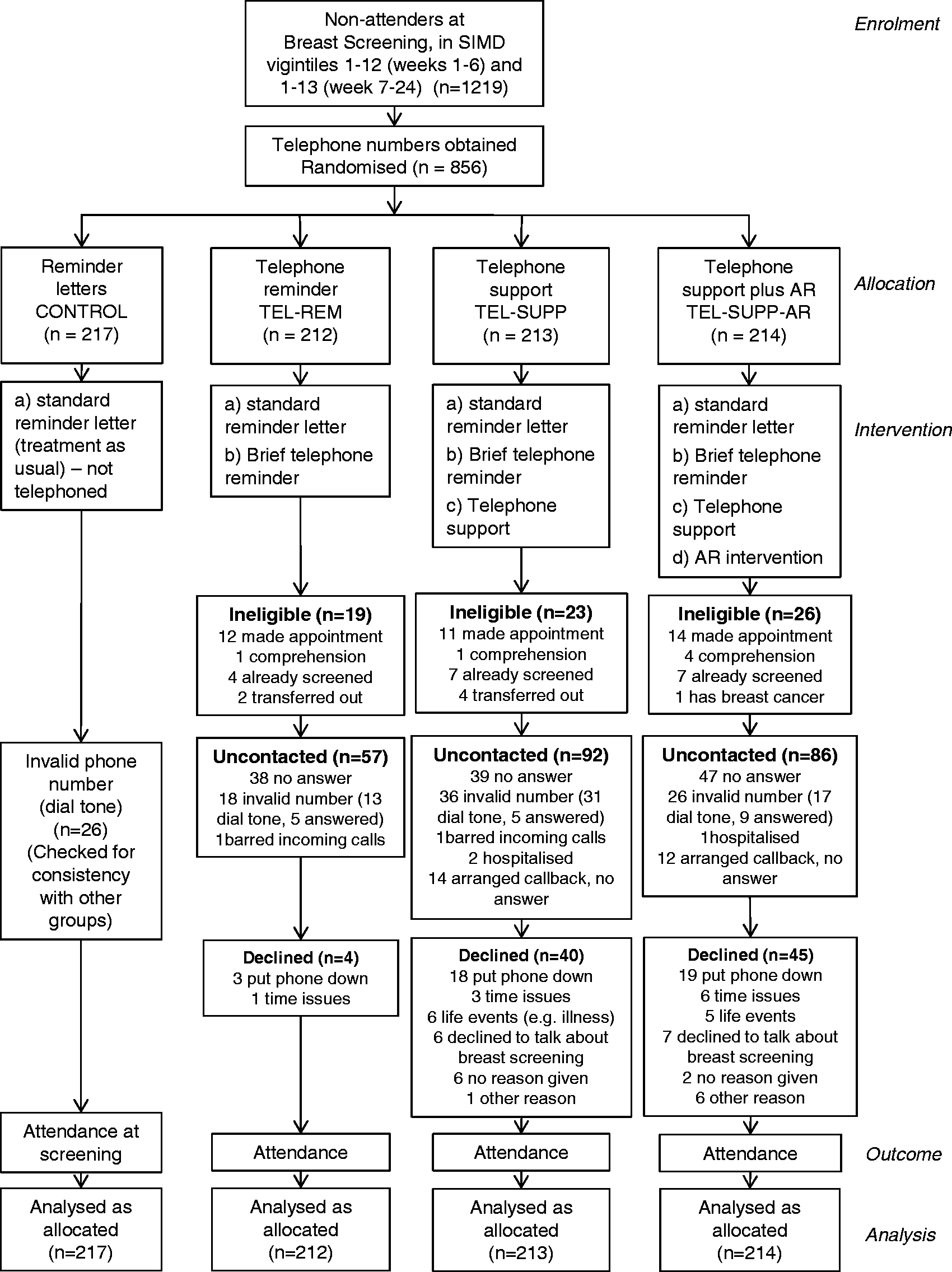
Women who had failed to attend their scheduled appointment and had not cancelled or re-arranged that appointment before the reminder letter was sent were recruited via the computer-generated reminder letter lists over a 24-week period from February-June 2014. We targeted women from SIMD vigintiles 1-12 (representing the lowest 60% of socio-economic areas in Scotland, based on factors including income, employment, health, education, housing and crime) (Footnote a ). Our protocol permitted the addition of higher SIMD vigintiles, if required, to achieve recruitment targets, resulting in the inclusion of vigintile 13 from week 7 (Figure 1).
Telephone numbers are not currently held on the screening database, and were sought from the local hospital or the telephone directory. The feasibility of obtaining telephone numbers was an important secondary outcome.
All women due to be sent a reminder letter who had not cancelled or rearranged that appointment, were resident in one of the specified SIMD vigintile areas (derived from postcode), and for whom telephone numbers were obtained, were included in the study and randomized to treatment. There were no exclusion criteria with regard to the intention-to-treat (ITT) analysis (ie. where participants were analysed as allocated to treatment group). For intervention participation, exclusion criteria were: appeared (when telephoned) to have difficulty comprehending the verbal information presented about the study (including understanding of English) or to be incapable of giving informed consent; reported they had already made another appointment for breast screening, been recently screened elsewhere, or had been diagnosed with breast cancer; and/or had moved outwith the Breast Screening service area.
Written informed consent was not sought from participants. Verbal informed consent was obtained from participants in the two TEL-SUPP groups, after the Patient Information Sheet was read out. Verbal informed consent was not feasible in the control arm (as they were not telephoned) or telephone reminder arm (as reading the information sheet would take longer than the brief intervention), and so was not sought. We did not seek consent to collect follow-up attendance data from any participants, as this information is routinely available at the Breast Screening service. Full UK NHS IRAS ethical approval was obtained for this approach (ref. no. 13/ES/0128).
Participants randomized to the control group received the reminder letter only, as current practice, sent from the East of Scotland Breast Screening Centre. All three telephone intervention groups received the same standard reminder letter as the control group. Participants in the intervention groups were telephoned by the Research Assistant from the University of Stirling within two weeks of the reminder letter being posted. Women who did not answer when telephoned were called a maximum of five times, after which they were recorded as uncontacted. The TEL group received a simple telephone call to remind them that they had not attended their scheduled appointment and to provide information on how they could rearrange this appointment. Participants allocated to the telephone support intervention (TEL-SUPP and TEL-SUPP-AR) were told that we were trying to understand why some women do not take up their invitation to attend for breast screening when invited, and asked whether they would be prepared to answer some questions. Consent was sought to audio-record the interviews to check for treatment fidelity, however, women who declined to be recorded could still participate.
Those who consented were asked to describe any reasons they had for missing their scheduled appointment, and where appropriate, any barriers they mentioned were addressed using a pre-specified list of responses, generated from previous research (data available from the authors). Any patient queries or concerns about the breast screening appointment were also addressed, using responses from existing screening materials. Participants were then asked whether they intended to make an appointment to attend for breast screening, whether they minded being telephoned about breast screening, and whether they found the telephone call helpful in addressing any concerns/queries they may have had (Yes/No/Maybe/Don’t know). Participants in the TEL-SUPP-AR group received exactly the same intervention as the TEL-SUPP group, with the addition of two questions relating to Anticipated Regret.
Randomization was carried out using minimization via the MINIM software 16 with age bands (50–56, 57–63,–64 or older) and SIMD quintiles (ie. 1, 2, 3 equivalent to vigintiles 1–4, 5–8 and 9–12) as the minimization variables in a simple 1:1:1:1 ratio (footnote b ). The researcher (JC) who carried out the randomization and collected the three-month follow-up data did not conduct the intervention, and remained blind to treatment group until the intention-to-treat analysis was completed. Participants were not told there were different treatment groups, and so were blind to treatment allocation.
Primary outcomes were whether or not a woman had made another appointment for breast screening, and whether or not they had attended screening, collected at three months follow-up (to October 2014) of the reminder letter or telephone call. Number of previous attendances and previous failures to attend, as well as whether they attended their last appointment, were also collected.
Intention to make an appointment was measured in the two telephone support groups by a single item (Do you intend to make an appointment for breast screening?: Yes/No/Maybe/Don’t know). This was coded as 0 = No, 1 = Maybe, and 2 = Yes (no-one answered ‘Don’t know’).
AR was measured in the TEL-SUPP-AR group only by two items (asked immediately before the question relating to intention to attend screening): ‘If you didn’t make another appointment to attend for breast screening, would you later wish you had?’ and ‘If you didn’t attend for breast screening, would you later regret it?’ (Yes/No/Maybe/Don’t know). Responses on each item were coded as 0 = No, 1 = Maybe, and 2 = Yes. ‘Don’t know’ was coded as user-missing. A mean score was calculated from the two items; if only one item was valid (n = 2), this was used as the mean score.
Our primary analysis was on an intention-to-treat basis, (ie. including all those randomized to treatment group, irrespective of contact or intervention participation status). All analysis was carried out in SPSS version 19; one-way ANOVAs and χ2 were used to test basic differences between treatment groups and logistic regression was used to assess predictors of ‘made appointment’ and ‘attended’. Kendall’s tau was used to assess first-order correlations with AR and intention (footnote c ).
A power calculation, based on a χ2 test comparing two proportions, indicated that a sample size of 600 participants (150 randomized to each group) would provide 76% power (at 5% level) to detect an increase in overall attendance of 7% combined across the three telephone intervention groups versus no increase in the control group, assuming a current attendance rate of around 69% in the targeted socio-economic groups (ie. vigintiles 1–12). 19
Results
Baseline characteristics by treatment group (n = 856).
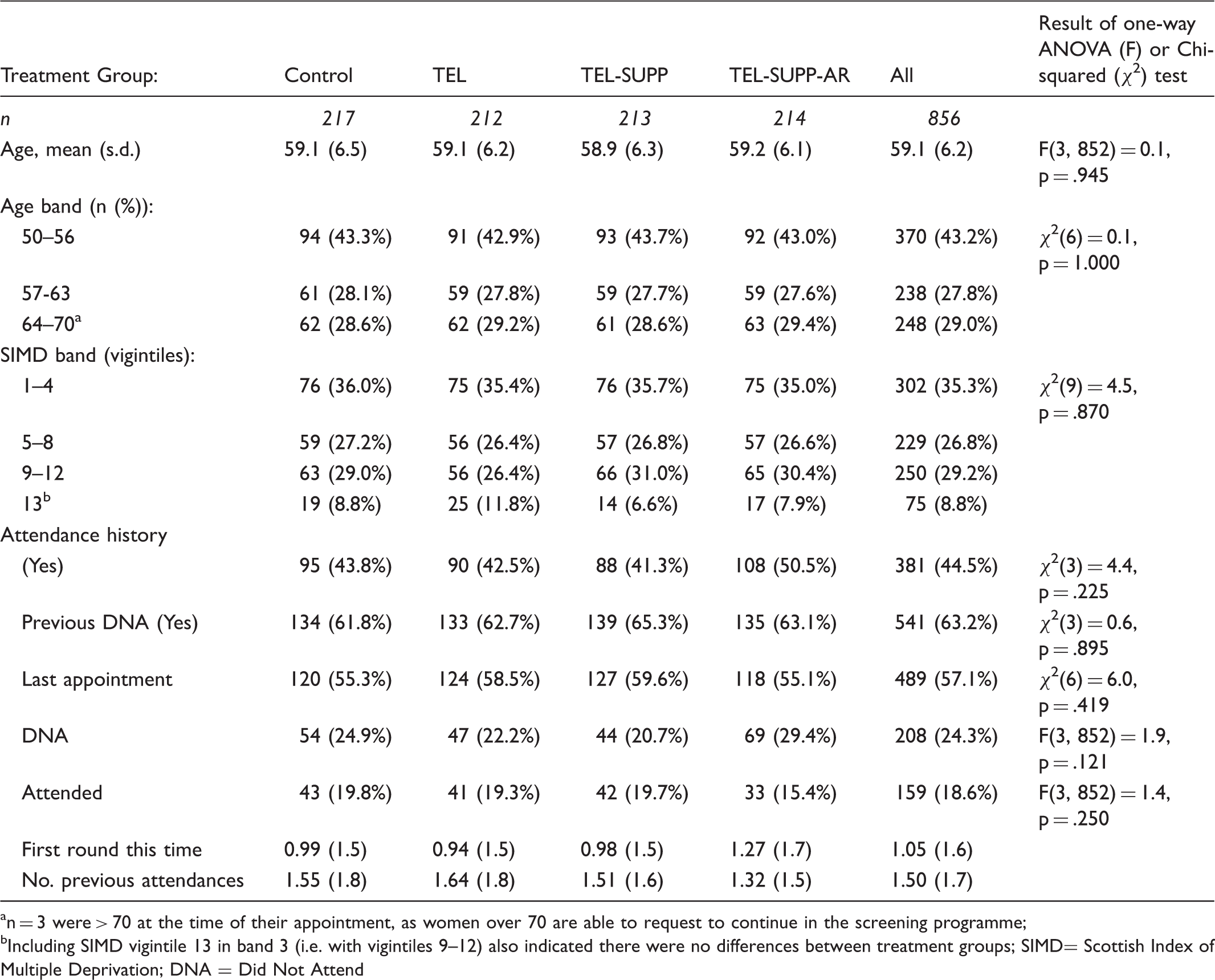
n = 3 were > 70 at the time of their appointment, as women over 70 are able to request to continue in the screening programme;
Including SIMD vigintile 13 in band 3 (i.e. with vigintiles 9–12) also indicated there were no differences between treatment groups; SIMD= Scottish Index of Multiple Deprivation; DNA = Did Not Attend
Appointment status by treatment group (Intention-to-treat).
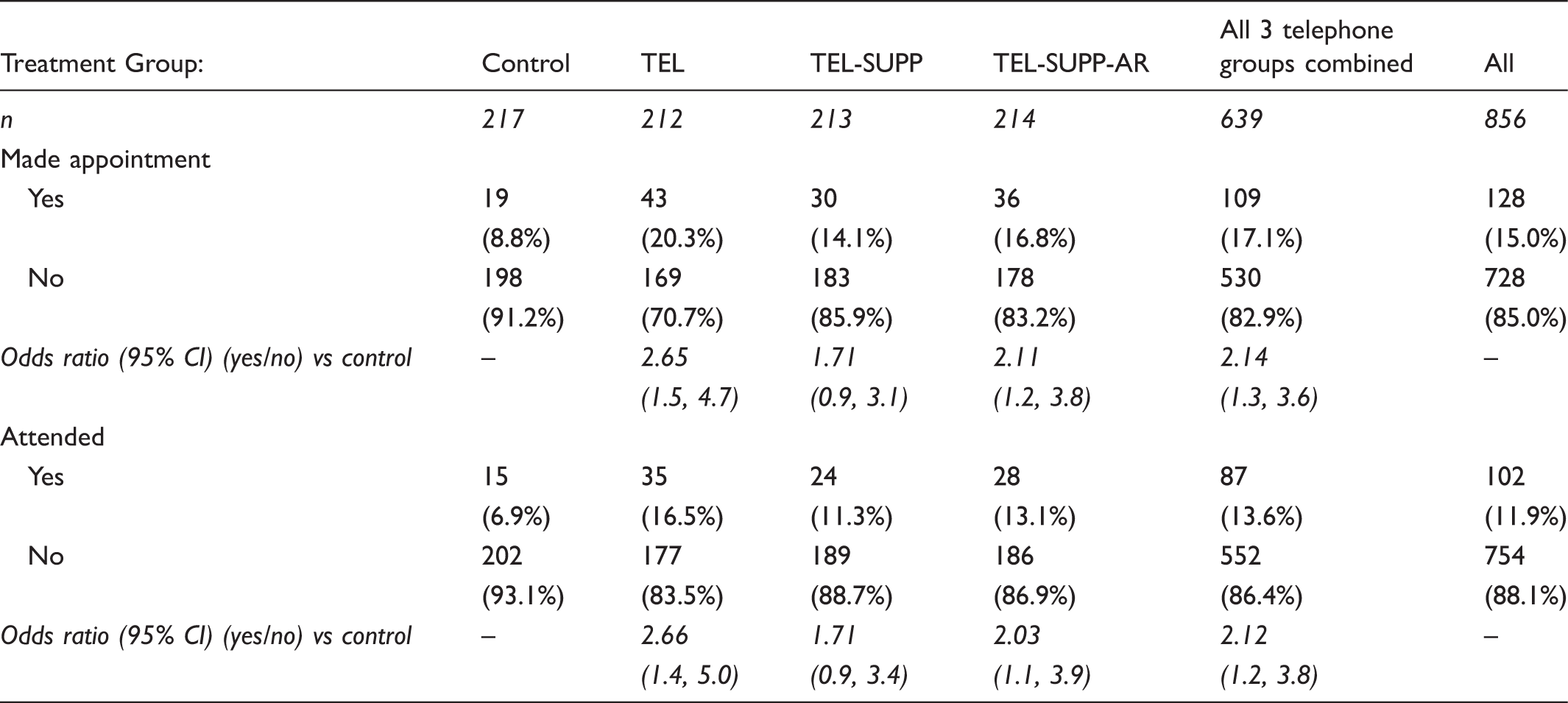
(χ2(3) = 12.0, p = .007) and attending (χ2(3) = 9.8, p = .020). The odds ratio (compared with the control group) of making and attending an appointment was significant for both the TEL and TEL-SUPP-AR groups (Table 2). Overall, being in one of the three telephone intervention groups more than doubled the odds of both making an appointment (χ2(1) = 8.8, p = .003) and attending it (χ2(1) = 6.9, p = .008), compared with the control group (see Table 2). Table 2 seems to indicate that the TEL group was more successful that the two TEL-SUPP groups, however, we believe this is due to the higher number of successful contacts in this group, explored in more detail below.
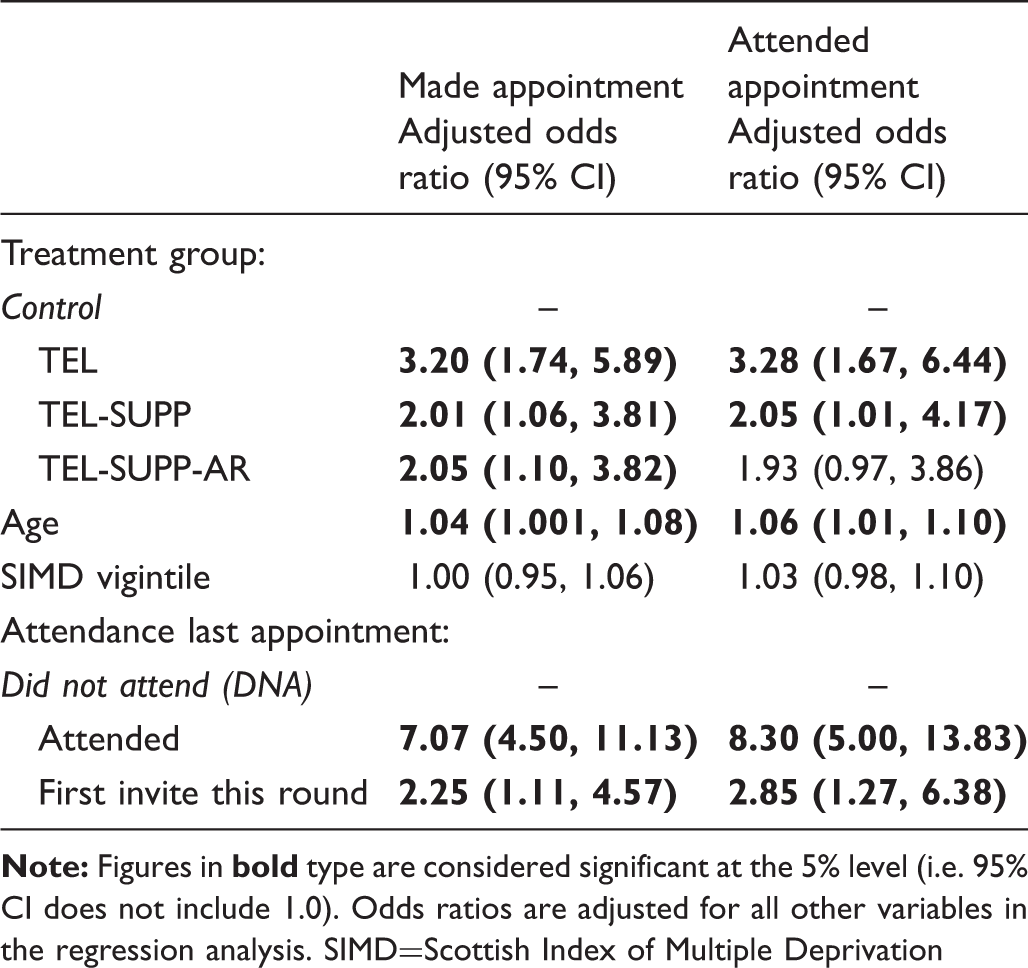
Logistic regression of current appointment status (n = 856).
Although telephone numbers were obtained for 856 eligible women in the reminder lists, 108 (13%) of these proved invalid when telephoned (ie. no dial tone or recorded message saying number did not exist, person answered and said it was a wrong number, or phone barred incoming calls) (Figure 1). Successful telephone contacts were made with 404 women in the three intervention groups, but 68 of those contacted proved ineligible for the intervention (37 already made appointment, 19 screened recently, 6 poor comprehension or inability to speak English, 6 transferred out of area) (Figure 1). Thus, 336 eligible women were successfully contacted, equating to just 60% of those with valid telephone numbers in the three intervention groups (n = 559).
More than a quarter (n = 89, 26%) of contacted women declined to take part in the intervention (Figure 1). Almost half of those declining (n = 40) put the phone down either before (n = 13), during (n = 20), or immediately after (n = 7) the introduction/information sheet was read out. It is therefore unclear whether these were true refusals of the intervention, or simply a refusal to be “cold-called”. There were therefore 247 intervention participants (Figure 1), representing 44% of contactable women, meaning our secondary analysis was underpowered.
The mean interview lengths were 2.2 minutes (standard deviation 1.1, median 2.0, range 0-6) for the TEL treatment group, and 13.4 minutes (standard deviation 6.8, median 12.0, range 0-63) for the two TEL-SUPP treatment groups. Almost all women in the two TEL-SUPP treatment groups (n = 112/115, 97%) said they did not mind being telephoned, and over 65% (n = 74) said they had found the phone call helpful, indicating that the telephone intervention was acceptable to participants.
Appointment status of eligible intervention participants (per-protocol) versus non-participants in the telephone intervention groups (n = 571).
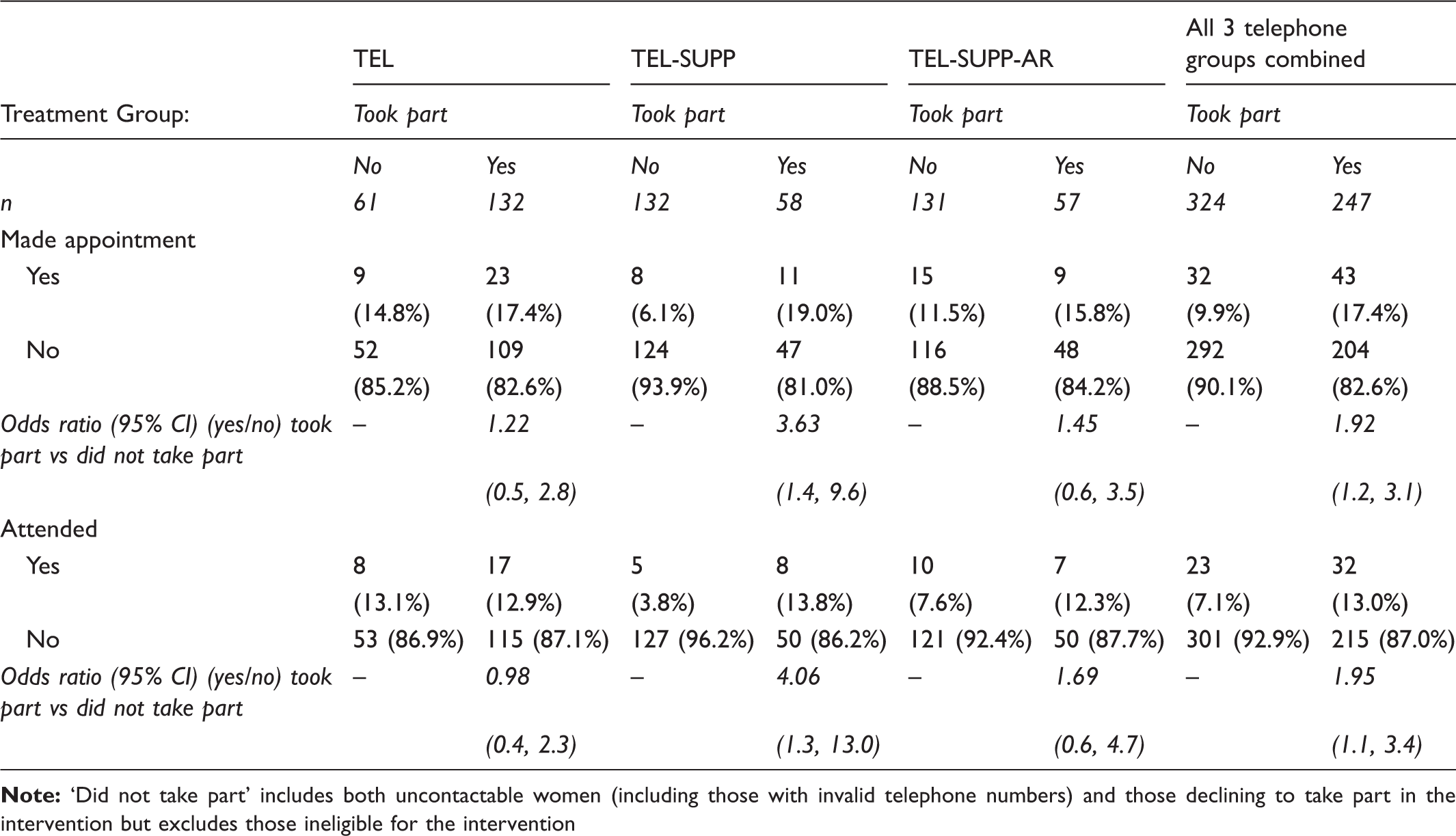
AR and intention were strongly related (n = 57; τ = .69, p < .001) and scores on these variables were significantly related to both making an appointment (AR: n = 57; τ = .26, p = .034; Intention: n = 115; τ = .30, p = .001) and attending (AR: n = 57; τ = .28, p = .024; Intention: n = 115; τ = .25, p = .006). However, simply being asked the AR questions (ie. being in the AR group) did not increase attendance over and above the telephone reminder or telephone support interventions.
Discussion
Routine breast screening, together with improvements in treatment, has almost certainly contributed to reduced deaths from breast cancer in the last 20 years; however, women in the most socially deprived areas are less likely to attend screening programmes, and have the worst breast cancer survival rates. Millar 20 predicted that, if screening uptake for all SIMD quintiles could be increased to the highest observed rate, 49–57 extra cancers would be detected in Scotland annually, with an extra 7–33 lives saved.
Our results indicate that a simple telephone reminder and support intervention aimed at increasing screening attendance was feasible and acceptable to women from lower income areas who had missed their initial appointment. The intervention approximately doubled the odds of making and/or attending an appointment in the three telephone groups compared with the control group, supporting earlier evidence that telephone reminders could significantly increase uptake over and above printed reminders. 21 Around 33–34% of women in our targeted SIMD vigintiles currently receive a reminder letter. Given the observed 7% attendance in the control group, attendance following the reminder letter currently accounts for around 2.4% of attendance. As the telephone intervention more than doubled the odds of attendance, we estimate that adding a telephone reminder could increase overall attendance by at least 2.5%, provided telephone numbers could be obtained.
Although the ITT analysis seemed to indicate that the telephone reminder was more effective than the telephone support groups, the per protocol analysis showed that the three telephone groups were similarly successful at increasing attendance. This was contrary to findings from a previous study using a similar stepped approach to increase colorectal cancer screening (ie. usual care, plus letter, plus telephone, plus nurse navigation), which found significant increases in screening uptake as the intensity of the intervention increased. 14 Whilst expressing regret about not making an appointment was related to increased attendance, AR did not confer any advantage in the ITT analysis, in contrast to an intervention for cervical cancer screening. 13 We believe this is the first time an AR intervention has been delivered by telephone. To this end we simplified the possible responses to the AR questions from a 7-point Likert-type scale to a 3-item response (Yes/No/Maybe). Although Conner et al. 22 found effects for AR using a dichotomous ‘Definitely No/Definitely Yes’ item, it is possible that the telephone delivery method and/or the simplified 3-item response-set may have reduced the effectiveness of the current AR intervention. This needs to be clarified in further research.
As telephone numbers are not routinely held on the screening database, our protocol determined that we would only randomize women for whom telephone numbers were obtained from other sources, thus excluding 30% of women who received a letter reminder during the study period. As we did not collect attendance information for this group, it is not possible to consider the effect of excluding these women in estimating the effectiveness of the intervention. A recent trial of a text-based reminder to increase uptake of breast screening was only able to obtain mobile numbers for 41% of women who had been randomized to treatment 23 but, despite this, showed a significant increase in uptake in the ITT analysis. This suggests that telephone or text-based intervention can be effective, even if a large percentage of telephone numbers cannot be obtained. Not holding telephone numbers on the breast screening database also presents practical problems for the service itself, eg. in contacting women if a screening session has to be cancelled at short notice (for example due to equipment failure). If it were decided to introduce telephone or text-based reminders into standard practice, there would be a clear need to include telephone numbers on the existing database.
The difficulties we experienced in contacting women, with almost 200 women either not answering their phone or putting the phone down, may stem from the current climate of cold-calling sales techniques. We were unable to begin our introduction by establishing that this was a bona fide call, or leave any message on answerphones, because our ethics agreement required us to verify that we were speaking to the correct person before disclosing the purpose of the call. This may have resulted in women ignoring what they assumed to be a marketing call. These restrictions would not apply to calls made directly from the breast screening unit, potentially resulting in a higher number of contacted women.
The small number of participants in the two TEL-SUPP groups, resulting from both the contact issues and a high number of women declining to take part, meant that the secondary analysis was underpowered. Hence, although our data suggest that the telephone support intervention did not provide any additional benefits over a simple telephone reminder, this cannot definitely be concluded. A further intervention, which reduces the burden of reading the information sheet/obtaining consent, perhaps by sending these materials in advance, is required to provide a fair test of the telephone support groups compared with the simple telephone reminder. As this was a pilot intervention, we did not estimate cost-effectiveness. This needs to be determined by further research, however, the cost of delivering the intervention is likely to be low. A systematic review 24 of telephone or text-message reminder interventions designed to increase uptake of attendance at hospital appointments found that the average cost of a verbal telephone call was around €0.90 per person (ie. approximately US$1 or £0.65 Sterling).
Ethnicity data was not available for this sample, however, there were no other demographic differences between intervention participants and non-participants, suggesting that those taking part were representative of women randomized to treatment. Our findings may therefore be generalizable to other groups of low-income women who do not attend for breast screening.
Conclusion
A simple telephone intervention was successful at doubling the uptake of breast screening after reminder. We recommend the implementation of a telephone reminder intervention from the breast screening service, which would also provide the opportunity to address practical barriers to attendance.
Footnotes
Acknowledgements
This research was funded by a grant from the UK National Health Service, Tayside. The funding source had no role in any aspect of the study design; the collection, analysis or interpretation of data; the writing of the report; or the decision to submit the article for publication.
Conflict of Interest
None to declare.