
Abstract

Beta-thalassaemia, an autosomal recessive condition, is the second most common haemoglobinopathy after sickle cell disease worldwide. In Pakistan, with a carrier rate of 5–13%1,2, an estimated 5000–9000 children are born annually with beta thalassaemia major. Pakistan has a strong tradition of consanguineous marriages, and termination of pregnancy is not acceptable to the majority of people. In 2013 the per capita annual income was $1380 (Pakistan Bureau of Statistics), compared with the estimated $6000/year cost of proper treatment for a thalassaemic child. Thalassaemia prevention in Pakistan is, therefore, both desirable and challenging.
Carrier detection is non-existent at a mass level in Pakistan, although identification of index case (cascade testing) 3 , either incidentally or in antenatal clinics with extended family screening 1 , has been described. Sophisticated antenatal testing utilizing chorionic villous sampling and amniotic fluid analysis is invasive and expensive, and is restricted to a few large cities. Thalassaemia screening prior to marriage is potentially an easier and more cost effective technique. Although the Pakistani government is currently planning the implementation of a law for mandatory pre marriage screening, we could find no studies of pre-marital thalassaemia trait screening conducted in Pakistan.
We therefore developed a study to explore the option of pre-marital screening, in a suburban area of Karachi. We aimed to determine the frequency of at risk couples for beta thalassaemia minor, and to observe the acceptability of this approach among masses.
In June 2010 our team visited five different areas of Sindh province, where 45–50% of the population is of reproductive age, most belonging to low socio-economic groups and with low literacy levels. We identified individuals planning to marry, as they may better understand the purpose of this exercise at this point in time. Informed verbal consent was obtained with assistance from the Fatimid Foundation Karachi (a non-governmental organization which supports diagnosis and patient care for thalassaemia patients).
Complete blood counts were performed on all subjects as an initial screening test (automated haematology analyzer, Beckmann coulterTM, Miami, FL, USA). Individuals having hypochromic (mean corpuscular Hb (MCH), <26 pg) and microcytic (mean corpuscular volume (MCV), <76 fl) red blood cell indices continued to haemoglobin variant analysis (Bio-Rad variant II high performance liquid chromatography analyzer; beta-thalassaemia short program; Bio-Rad laboratories, Hercules, CA, USA). An HbA2 level of ≥3.5% was considered diagnostic for beta-thalassaemia trait. Statistical package for social sciences (SPSS-19) was utilized for data analysis (SPSS Inc., Chicago, IL, USA). The computerized data were encrypted to maintain anonymity.
Beta-thalassaemia carrier status of 128 couples.
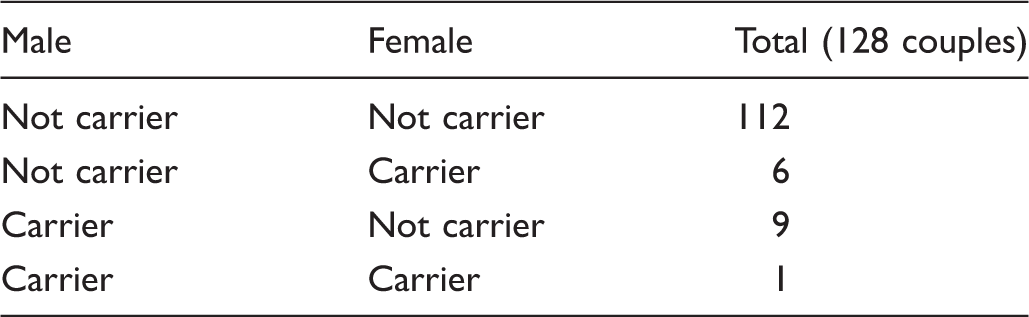
Of the 256 subjects, one (0.78%) couple was found to be at risk of having beta-thalassaemia major children. The frequency of beta thalassaemia minor was 6.6%, in concordance with national data.2,4 The second most commonly identified variant after beta-thalassaemia trait was haemoglobin D trait (n = 5; 1.9%). As expected, the current study showed a high prevalence of beta thalassaemia in the general population. Despite the small sample size, the study demonstrated the social and cultural acceptability of pre-marital screening among the Pakistani population.
In Pakistan, health facilities for proper management of thalassaemia major are inadequate, as a result of poverty, lack of education, the unavailability of safe blood, and a poorly developed health care system. These factors contribute significantly to limit the average life expectancy of a thalassaemia major child to just 10 years. Under the present circumstances, thalassaemia can at best be prevented, rather than optimally treated.
Premarital thalassaemia screening has been implemented effectively elsewhere, for example, in Cyprus, where there were no affected births reported between 2002 and 2007. 5 Similarly in Saudi Arabia, more than a 70% reduction in the prevalence of β-Thalassaemia was reported six years after the premarital screening programme was introduced. 6
Approximately 50% of the Pakistani population is of reproductive age group. Prior studies in Pakistan have focused on antenatal screening only, but a strength of our study was the distinctive targetting of couples just before marriage. Focusing on this population highlighted the significance of premarital screening. Considering only the prevalence rate in general population may perhaps not attract people for premarital screening. The significant prevalence of thalassaemia trait, and hence at risk couples, warrants the establishment of a premarital screening programme in Pakistan. Screening for thalassaemia before marriage appears to be a viable option in terms of acceptability to the Pakistani population. Mass screening of all individuals may initially be a challenging concept in terms of cost-effectiveness, but it would eventually reduce the burden of thalassaemia major in Pakistan. For such a programme to succeed, there is an urgent requirement for mass education, the involvement of health care providers, and of religious figures to motivate people for thalassaemia screening before marriage.