
Abstract
This study explores how legal experts and physicians ensure the autonomy of individuals with dementia when assessing the need for legal guardianship and appointing guardians. Through interviews with 20 legal experts and 30 physicians, and thematic analysis, the research identified key analytical groups. Legal experts focus on (1) Ascertaining the individual’s views and (2) Minimising interference with autonomy. Physicians emphasise (1) ascertaining the individual’s views, (2) Supporting the realisation of autonomy and (3) Providing accurate information on the legal process. The study found that legal experts strongly respect autonomy, sometimes even deviating from strict legal requirements to ensure that individuals with dementia are heard and their opinions considered during court proceedings. Although physicians generally stress the patient’s autonomy, they prioritise protecting the individual more than legal experts.
Introduction
The principle of autonomy, defined here as self-governance free from external control and from restrictions that hinder meaningful choice, 1 is widely recognised as a cornerstone of clinical ethics. 2 Autonomy is also universally upheld by numerous legal frameworks, including the UN Convention on the Rights of Persons with Disabilities (CRPD) and the UN General Assembly’s Universal Declaration of Human Rights (UDHR). Autonomy is a fundamental principle of the CRPD (Article 3a), guiding the interpretation of all other provisions within the convention. The CRPD mandates that the 192 parties 3 that have ratified it ensure that individuals with disabilities can exercise autonomy equally to non-disabled individuals.
Autonomy is a multifaceted concept that includes individualistic, relational and procedural aspects, especially when it comes to the autonomy of individuals with dementia. 4 One way to conceptualise autonomy is to divide it into three subdivisions of self-determination: (1) the right of a legally competent individual to make independent decisions; (2) the right to be heard as part of self-determination; and (3) respect for the previously expressed or presumed views of an individual with diminished mental capacity. 5
The topic of the autonomy of individuals with dementia has been the subject of extensive research. 6 Previous research has focused, among other things, on the experiences of individuals with dementia, the role of their relatives, and the factors that may limit their autonomy. 7 Further studies have examined how health and legal professionals conceptualise their roles in the practice of providing support for decision-making by people living with dementia. 8 Furthermore, studies have specifically examined the criteria for appointing a guardian for an individual with dementia, 9 and how dementia symptoms are assessed when evaluating the need for guardianship. 10
However, what methods and principles legal experts and physicians use to ensure an individual’s autonomy is respected when assessing the need for and appointing a guardian remains unexamined. This question is crucial, as the autonomy of individuals with dementia is not always considered in accordance with the requirements of the CRPD during assessment of the need for legal guardianship. 11 This factor, combined with the fact that loss of autonomy is a fundamental challenge for individuals living with dementia, 12 underscores the importance of research aiming to identify ways to support autonomy. It should be noted that autonomy is not only a right protected by legal instruments but also a fundamental human need. The need for autonomy refers to the desire to self-regulate one’s experiences and actions, characterised by behaviours that are self-endorsed and aligned with one’s genuine interests and values. 13 Meeting this need enhances the well-being of individuals with dementia. 14
Here, our aim was to identify the practical methods and principles employed by legal experts and physicians to ensure that individuals’ autonomy is respected when evaluating the need for legal guardianship and appointing guardians in Finland. In this article, the guardianship appointment process includes medical and legal evaluation of the need for legal guardianship and the appointment of a guardian. Thus, the topic was approached with an interdisciplinary methodology, combining legal and medical perspectives. The topic was examined through semi-structured thematic interviews conducted with legal experts and physicians who participate in guardianship appointment processes as part of their professional roles. Although the final decision on guardian appointment is made by a judge or a specialised guardianship authority, it heavily relies on the medical assessment conducted by a physician. Therefore, the integration of legal and medical perspectives is crucial. Although these professions are frequently perceived as being at odds with each other, 15 they should work together to ensure that individuals’ autonomy is fully respected.
Considering the differing views of these professional groups in assessing the need for legal guardianship is valuable, also from an international perspective. Although legal systems regulating guardianship measures vary across countries, the final assessment is legal in nature and made either by a court or a designated administrative authority – not only in Finland but also in many other countries. Moreover, legal assessments across jurisdictions rely heavily on medical expertise, although the requirement for the medical certificate varies. 16
Autonomy and guardianship
Globally, guardianship policies are regulated at the national or state level, and may use various terms such as guardianship, conservatorship, deputyship and curatorship depending on the legal system. These terms refer to the legal authority granted to manage the affairs of individuals whose mental capacity is diminished. Despite the differences in legal systems, the common legal standard for appointing a guardian requires that the individual is incapacitated, and that the appointment is necessary to protect the individual’s interests. 17 In this article, the term ‘guardianship’ refers to the appointment of a legal representative to oversee the financial or personal affairs of an individual with dementia and diminished mental capacity. The term ‘client’ refers to an individual under guardianship, and ‘potential client’ refers to an individual being assessed for the need for guardianship.
Although no international conventions specifically address the rights of individuals with dementia, several treaties and specific articles within broader conventions also apply to the rights of adults with disabilities. In addition to the CRPD and the UDHR, examples include the European Convention on Human Rights, the Charter of Fundamental Rights of the European Union, the European Social Charter and the Convention of 13 January 2000 on the International Protection of Adults. In this study, the CRPD serves as the framework through which Finnish national legislation is linked to the international context, as the CRPD is a widely accepted international convention and significant legal instrument that sets standards for the rights of persons with disabilities, including those living with dementia.
The CRPD highlights the significance of autonomy, especially in the realms of decision-making and legal capacity. The CRPD acknowledges that, with the right support, individuals with disabilities are capable of making their own decisions. This perspective suggests that autonomy is not solely an individual attribute but is facilitated by a network of social supports. 18 Especially in the context of legal guardianship, autonomy should be understood in a broad sense – as relational autonomy, which is constructed and developed through interaction with others and within a social context. 19 Article 12 of the CRPD guarantees equal legal recognition and legal capacity for individuals with disabilities in all aspects of life. In this context legal capacity means the formal ability to possess and to exercise rights and duties. 20 It has been suggested that Article 12 prohibits traditional guardianships and advocates for their substitution with ‘supported decision-making systems’. 21 This is because, while the intent of legal guardianship is to safeguard the interests and rights of individuals with diminished mental capacity and to ensure they receive the necessary support, in practice it often restricts their autonomy and legal capacity. 22 Guardianship can, for instance, limit the client’s ability to make independent decisions regarding their finances or living arrangements. 23 Instead, with supported decision-making, adults with disabilities receive assistance in decision-making but retain ultimate authority and choose their supporters. 24
However, assessing the need for legal guardianship and appointing a guardian are balancing acts between autonomy and protection. 25 In addition to respecting autonomy, the States Parties to the CRPD must also protect other rights, including the rights to health, freedom from abuse and protection against ill-treatment. 26 Dementia is a progressive disease that impairs an individual’s mental capacity, putting them in a vulnerable position. 27 For instance, the individual may lose the capacity to formulate a legal will, as they are no longer capable of making rational and legally binding decisions regarding their financial or personal affairs. 28 This incapacity may lead to neglect of their affairs, susceptibility to financial exploitation or engagement in legal transactions that they cannot fully comprehend. 29 Therefore, even countries that have fully ratified the CRPD continue to give competence to legal authorities to appoint guardians to protect people with reduced mental capacity. 30 The requirements to safeguard individuals’ rights that ensure their physical, mental and financial well-being sometimes lead to conflicts with respect for individual autonomy.
The legal requirement to respect autonomy during the guardianship evaluation and appointment process in Finland
Finland ratified the CRPD and its Optional Protocol in 2016, 31 but also has legislation that allows the appointment of guardians and the restriction of legal capacity. In Finland, the regulation of legal guardianship and the appointment of guardians is governed by the Guardianship Services Act (442/1999, the GSA). The CRPD and the GSA form the central legal framework of the study, guiding both the research perspective and interpretation.
The GSA places strong emphasis on respecting autonomy. The GSA aims to ensure that any necessary restrictions on an individual’s decision-making authority for their protection are specifically tailored to their specific needs, thereby avoiding unnecessary limitations on their autonomy. The appointment of a guardian is intended to occur only when it is genuinely in the individual’s best interests. 32 In the Finnish legal guardianship context, the principle of autonomy can be seen as an optimisation directive: procedures should be selected to promote the individual’s right to make decisions about their own affairs as fully as possible. 33
The GSA contains several provisions that emphasise respect for the client’s autonomy in situations where a guardian is being appointed. First, the Act outlines the conditions for appointing a guardian: a court may appoint a guardian for an adult who, due to illness, impaired mental functioning or deteriorated health, is incapable of overseeing their own interests or managing their personal or financial affairs that need to be managed and could not be appropriately managed in any other way (Section 8.1). Guardianship is therefore a secondary measure for managing an individual’s affairs, and the appointment of a guardian is unnecessary if the affairs of an incapacitated individual can be managed through other means, such as with informal assistance from family members. A guardian can be appointed to represent the client in matters concerning their property and financial affairs (Section 29.1), personal matters (Section 29.2), for a specific legal transaction or matter or regarding a specific property (Section 8.3). The aim of this regulation is to ensure that individuals can be protected while guaranteeing their right to autonomy is limited only as much as is necessary to protect their interests. 34
In Finland, the role of a guardian is primarily to support the client; the client retains their legal capacity alongside their guardian (Section 14). The appointment of a guardian does not revoke the client’s legal capacity, nor does it inherently interfere with the competence of the client unless otherwise provided by law. If the appointment of this kind of supporting guardian is insufficient to protect the individual’s interests, their legal capacity can be restricted by a separate court decision. (Section 18)
The appointment of a guardian impacts a client’s autonomy even though their legal capacity is not explicitly restricted. A guardian has significant discretion, for example, regarding access to a client’s bank account and receivables. If a client has an account with a credit institution, the guardian must notify the institution as to who has the right to withdraw funds from the account (Section 31.2). Receivables pertaining to any property under the guardian’s administration can only be collected by the guardian or paid into an account designated by them for the client (Section 31.1). In addition, the client is required to tolerate changes to their legal status that the guardian can make by exercising decision-making authority alongside the individual without their consent. Overall, the realisation of the right to autonomy of a client is largely dependent on how their guardian seeks to respect their autonomy. 35 These aspects conflict with the CRPD, as they impose significant restrictions on legal capacity and autonomy. Consequently, the Finnish guardianship system as a whole does not fully comply with the CRPD. 36
The legislation also includes procedural provisions aimed at safeguarding autonomy. 37 If an individual understands the significance of a guardian and voluntarily requests one, the guardianship authority may appoint one (Section 12). The threshold for appointing a guardian is intended to be lower in cases where the individual themselves understands that they need guardianship and, being aware of the effects of appointing a guardian, consents to a specific person being appointed as their guardian. 38 Conversely, if a guardianship evaluation is initiated by someone other than the individual themselves, or if the individual objects or does not understand the necessity for a guardian, the court assesses the need for a guardian and appoints one if required. In situations where the individual does not oppose the appointment of a guardian, the court should not interpret the conditions for appointing a guardian very rigorously. However, even in such cases, the court must still determine that appointing a guardian is necessary. 39 If the individual resists, the court can still appoint a guardian if the objection is deemed insufficient based on the evidence presented (Section 8.2). In other words, an individual’s right to self-determination can be overridden if the court deems them to be in need of a guardian. The legislation does not provide explicit guidance for situations where the individual’s opinion cannot be ascertained. However, in such cases, a more thorough investigation into the necessity for guardianship must be conducted compared to cases where the individual has explicitly consented to the appointment of a guardian. 40
The legal assessment of the need for legal guardianship made by the court is primarily guided by Chapter 8 of the Guardianship Services Act. In addition, the judicial procedure is partially detailed in Chapter 8 of the Code of Judicial Procedure, on consideration of petitionary matters, as well as other applicable provisions of the Code of Judicial Procedure.
In matters concerning the appointment of a guardian for an adult, the person whose interests are to be overseen must be given an opportunity to be heard (Section 73.2). The purpose of hearing the potential client is to determine their opinion, specifically whether they oppose the legal guardianship. If they oppose the appointment of a guardian, the hearing can gather information on the reasons for their opposition. 41 Hearing the potential client is crucial for the client’s legal protection. Since guardianships interfere with the client’s autonomy, the court must obtain accurate information to base its decision on. 42 According to the legal principle established in the Supreme Court precedent KKO:2012:109, the hearing of the potential client may be waived only in the exceptional circumstances specified in Sections 73.4 and 73.5 of the Guardianship Services Act. These exceptions apply in situations where a notice of the opportunity to be heard must be served by public notice, or where such notice cannot be served due to the potential client’s condition, and the legal protection of the person concerned does not require the appointment of a guardian ad litem.
The spouse of a potential client must also be given an opportunity to be heard (Section 73.2). Consulting the spouse is essential to reliably assess the need for legal guardianship and to avoid unnecessary interference with the individual’s autonomy by appointing a guardian in situations where it is not necessary. 43 In matters concerning the restriction of an individual’s legal capacity, the court must hear the person whose interests are to be overseen in person (Section 74).
In matters concerning the appointment of a guardian or the restriction of an individual’s legal capacity, the court must, on its own motion, order the procurement of all necessary evidence (Section 78) and, if necessary for the person’s legal protection, appoint a legal counsel or guardian ad litem for the purposes of the judicial proceeding (Section 82). The appointment of a legal counsel or guardian ad litem is relevant inter alia when the individual opposes the appointment of a guardian but, due to their condition, is unable to articulate the reasons for opposition. Thus, a legal counsel or guardian ad litem is an important means to ensure that an individual can exercise their autonomy in court and is duly heard during the proceedings. A legal counsel can be appointed in situations where the individual can oversee the legal counsel’s actions and provide them with instructions. In such cases, the relationship between the potential client and the legal counsel mirrors the common client–lawyer relationship, where the lawyer presents various options and their potential consequences to the client, enabling the client to make an informed decision. In these situations, the ultimate decision-making power regarding how to approach guardianship and how to proceed with the case lies with the client, and the client can exercise autonomy with the assistance of legal counsel. In contrast, the appointment of a guardian ad litem is considered if the individual is incapable of overseeing a legal counsel’s actions and providing them with instructions. A guardian ad litem is appointed specifically to represent an individual’s interests in court proceedings. In matters concerning legal guardianship, an individual’s best interests may sometimes conflict with their wishes and views, necessitating the appointment of a guardian ad litem to highlight the need for protection, even if the potential client opposes guardianship. 44
The medical assessment conducted by a physician plays a crucial role in determining the necessity for legal guardianship. Currently, there are no guidelines in Finland that provide instructions on how autonomy should be considered during the medical assessment for the need for legal guardianship. The medical assessment is not regulated by the GSA nor by the Act on the Status and Rights of Patients (785/1992), which details the key legal principles related to the treatment and care of patients. The Ministry of Social Affairs and Health in Finland has issued guidelines on physicians’ statements in guardianship matters, 45 and the national guardianship authority provides a template for medical reports to be used when assessing the need for legal guardianship; these documents contain some guidelines on conducting the assessment. 46 The documents guide physicians, for instance, to ascertain the patient’s perspective on legal guardianship, as the template for medical reports includes a section where the patient’s perspective must be recorded.
Data and methodology
This article draws on the findings of a semi-structured interview study into how legal experts and physicians strive to ensure that autonomy is respected to the greatest extent possible when assessing the need for legal guardianship and appointing guardians for people with dementia in Finland.
Eligibility to participate and recruitment
Legal experts (district registrars who work for the national guardianship authority and district judges) and physicians (geriatricians, neurologists, and general practitioners) were eligible to participate if they had experience of assessing the need for legal guardianship as part of their professional duties. The national guardianship authority oversees the rights and interests of individuals who are unable to manage their affairs and may file a petition for guardianship appointment with a court as needed. Furthermore, the guardianship authority supervises the activities of guardians. 47
We selected participants purposively to access professionals with varied personal and professional backgrounds. 48 The interviewees were recruited through professional network of the research team, and snowball recruitment. Twenty-five physicians took part in the interviews after receiving an email invitation. We also emailed the senior medical officer of one hospital district, requesting them to distribute the invitation to physicians. The first two respondents were accepted. In addition, one physician, having heard about the ongoing study elsewhere, volunteered as an interviewee. Fifteen legal experts took part in the interviews after receiving an email invitation. We also emailed the national guardianship authority and the chief judges of district courts, asking them to forward the invitation to legal experts. The first four respondents were accepted. One legal expert who had heard about the research from elsewhere also volunteered for an interview.
Data generation
All participants provided informed consent to participate. The interviews took place between August 2021 and February 2022. Interviews were conducted via video or telephone call, except for one interview which was conducted face-to-face. All interviews were conducted by the same interviewer (KN). The interviews were audio-recorded and transcribed verbatim.
The interviews aimed to investigate how legal experts and physicians assess the need for legal guardianship of individuals with dementia. The research theme of this article concerns the methods and principles used by legal and medical experts to ensure that the autonomy of potential clients is upheld when assessing the need for legal guardianship and appointing guardians. Other interview themes included the conditions that must be fulfilled for an individual with dementia to require legal guardianship and the conditions that affect the need for legal guardianship. 49 Furthermore, the interviews examined the relationship between dementia, mental capacity and the need for legal guardianship in the context of various cognitive and neuropsychiatric symptoms. 50 A semi-structured interview schedule was used. Most questions were open-ended, allowing participants to fully discuss their views and experiences. 51 The interview content was based on the requirements set by Finnish legislation for appointing a guardian.
Data analysis
Identifying information was removed before the analysis. The participants were given pseudonyms to ensure their anonymity, and details that could jeopardise their anonymity have been omitted from the research article.
The data were analysed using thematic analysis, which is useful for identifying and analysing patterns and meanings within data. 52 The analysis was partly theory-oriented, as it concerned assessing the need for legal guardianship and appointment of guardians as provided for in the GSA and in other legislation. However, the authors were not tied to a single theory nor seeking to substantiate a priori assumptions.
The legal experts’ and physicians’ interviews were analysed separately, to make the differences in professional groups’ attitudes towards supporting autonomy visible. The analysis was conducted manually. The analysis process began with a thorough review of the data, followed by the generation and development of initial themes. Key concepts were subsequently identified, and broad thematic index codes were created. Initial themes were developed by grouping these codes and identifying patterns within the data. These initial themes were then refined and evaluated to ensure accurate representation of the data. To construct a coherent overview of the data, the final themes and subthemes were refined, defined and named. Finally, an examination of the codes and the coded data was conducted to derive patterns of meaning and themes.
Although the data were analysed by a single author (KN), the findings were discussed among the research group, which consisted of legal experts and a neurologist, at various stages of the analysis. 53
Ethical approval
The Ethics Committee of the University of Eastern Finland stated that this study did not need ethics committee approval according to Finnish Law (letter from the committee of 8 December 2021).
Findings
Twenty legal experts (10 district judges and 10 district registrars) and 30 physicians (12 geriatricians, 11 neurologists, and 7 general practitioners) were interviewed (Table 1). The duration of the interviews ranged from 50 to 120 minutes.
Demographic characteristics of the study participants.
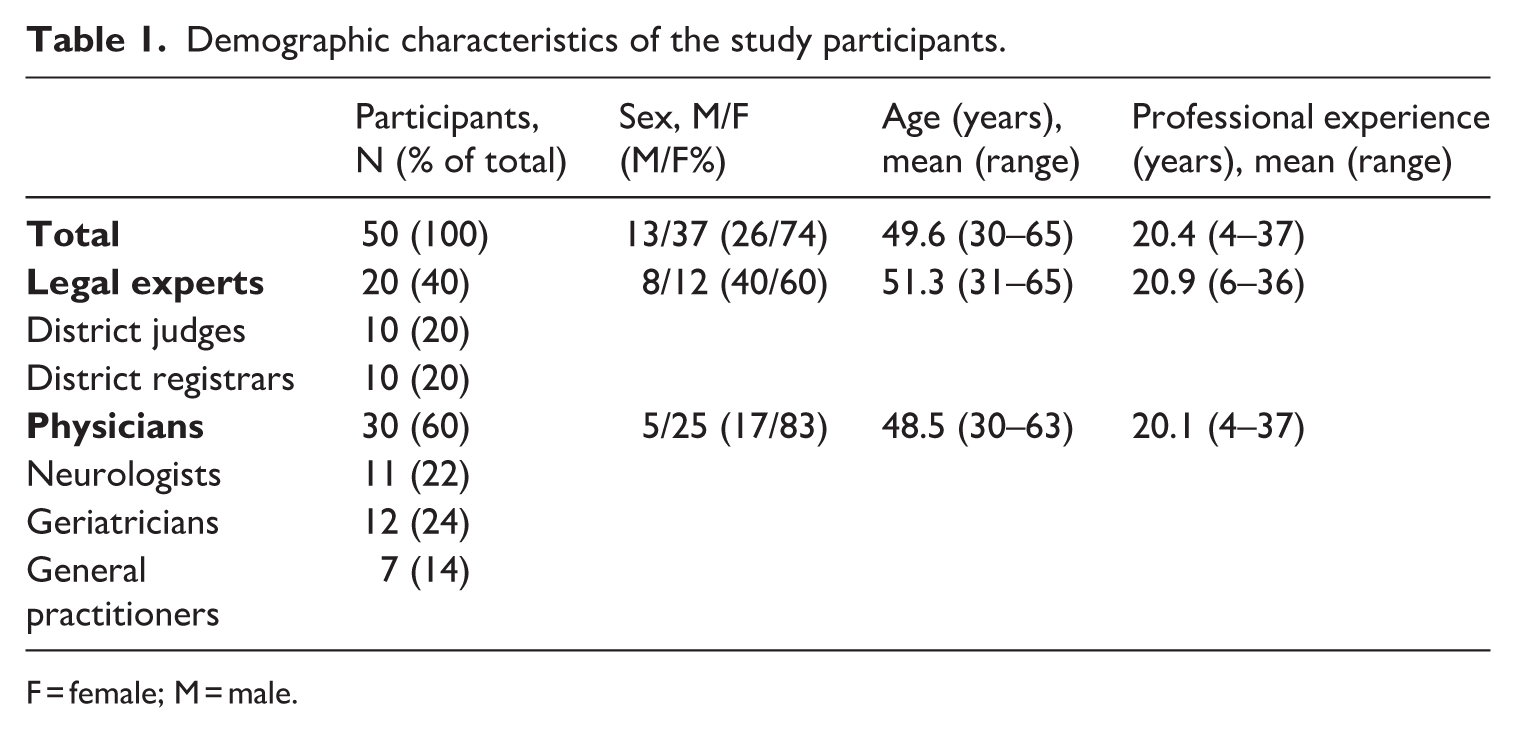
F = female; M = male.
The interviewees’ responses were categorised into five main categories, which were further divided into subcategories. The main category (1) Ascertaining the individual’s views emerged from the answers of both professional groups. The main category (2) Minimising interference with autonomy was specific to legal experts. In contrast, the main categories specific to the physicians’ responses were (3) Supporting the realisation of autonomy, and (4) providing accurate information on the legal process.
Legal experts’ descriptions of respect for autonomy
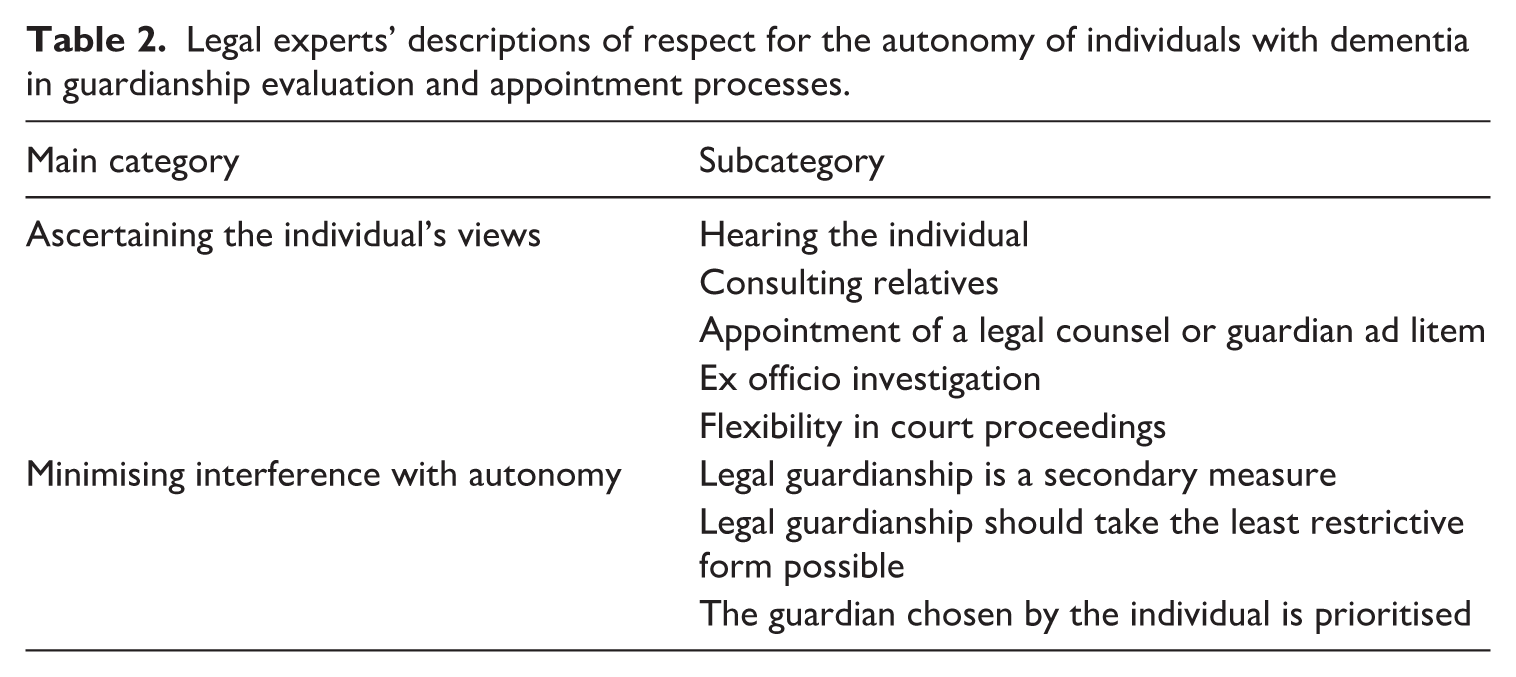
The legal experts’ answers were categorised into two main categories, which were further divided into subcategories. The main categories that emerged from the legal experts’ responses were (1) Ascertaining the individual’s views and (2) Minimising interference with autonomy. The main categories and subcategories of the legal experts’ answers are presented in Table 2.
Legal experts’ descriptions of respect for the autonomy of individuals with dementia in guardianship evaluation and appointment processes.
Ascertaining the individual’s views
This main category based on the legal experts’ responses consists of five subcategories: (1) Hearing the individual, (2) Consulting relatives, (3) Appointment of a legal counsel or guardian ad litem, (4) Ex officio investigation, and (5) Flexibility in court proceedings. The main category ascertaining the individual’s views was common to both legal experts and physicians, although it consisted of different subcategories in each case.
All the legal experts emphasised the importance of hearing the individual, justifying this by noting that appointing a guardian is a significant intrusion on autonomy:
Appointing a guardian interferes in a person’s life. And restricting legal capacity represents a very severe interference. Thus, a lot of listening and requirements are involved. We didn’t understand this when the law was enacted, but now we do, as the Supreme Court has issued decisions highlighting this . . . One must hear, discuss and review much more than in other matters. (LE4)
To ascertain the individual’s opinion, it is not sufficient to merely provide an opportunity to submit a written statement like in many other matters handled by the court. Instead, the individual’s opinion must be determined more effectively:
I see it starting with the bailiff assessing the situation and asking the potential client – if they can be asked – their opinion and writing down their response, so we always get the message if the potential client says guardianship is not needed or they strongly oppose it or something else. I strive to ensure that their voice is heard, even if they cannot provide a written statement. I readily call them to a court hearing if they oppose. (LE6)
However, several legal experts pointed out that there are specific characteristics related to the vulnerable position of individuals with dementia which can sometimes make respect for their autonomy merely superficial:
When hearing an individual, there is often an assumption and expectation of more self-determination or capacity for self-determination than exists. This leads to unpleasant situations, especially if relatives are contentious. Each one, in turn, whispers into the potential client’s ear, disparages others, and tells their own truths. As a result, the potential client’s opinion frequently changes based on who last spoke with them. (LE19)
This quote illustrates that determining the true opinions of individuals with dementia is challenging and requires special expertise from legal professionals.
Although all the legal experts expressed that hearing the client is a central issue when assessing the need for and appointing guardians, one district judge admitted to sometimes bypassing it:
I believe that at least in [large city], where the number of cases is considerable, there are judges who, based solely on the medical report, become convinced that it is no longer worthwhile to hear the person on the matter and do not send the bailiff to meet the person, but just rule on the case. I believe this happens, and I do it myself. (LE9)
Such a procedure does not meet the requirements of a fair hearing and does not allow for the exercise of autonomy. The quote shows that although the importance of hearing the potential client in guardianship cases is recognised, the rights of vulnerable individuals are compromised due to the considerable number of cases judges must rule on.
The importance of consulting relatives was considered almost self-evident by the legal experts:
I certainly consider it important to hear the relatives. It is a natural part of the matter. (LE19)
Consulting relatives was deemed particularly important in order to ascertain the previously expressed or presumed views of the individual. Presumed views refer to the assumptions made about what the person would want, especially in terms of their care and treatment, based on their preferences, values and beliefs as expressed before dementia set in.
54
Prior or presumed views are respected if the individual is no longer able to communicate their views clearly due to severe dementia:
When a person cannot express their will in this matter, such as who should take care of them and how, and whether they trust someone, it is necessary to try to determine the person’s will somehow. These situations are difficult, and the answers are not visible in any medical reports; they only become clear from the relatives’ accounts. (LE1)
Legal experts also emphasised the importance of hearing multiple relatives, even though the law does not require it:
The legal obligation to hear is not very strict. The potential client and their spouse are heard, and who else is heard is left open. It would be good to consider hearing as many close relatives as possible to obtain sufficient information. (LE4)
Legal experts also recognise the risks associated with hearing relatives. For example, they noted that the relative being heard is often an heir of the individual with dementia. Therefore, the relative might promote their own financial interests in the case. Despite this risk, almost all legal experts considered hearing relatives to be one of the key measures during guardianship evaluation.
Among the legal experts interviewed, the district judges in particular regularly emphasised that the appointment of a legal counsel or guardian ad litem is a crucial means to ensure that the perspective of an individual with diminished capacity is considered when assessing the need for a guardian:
In my opinion, it [the appointment of a guardian ad litem] may be the most effective way to ensure that individuals receive the necessary support and assistance to express their perspective. (LE5)
In addition, some district judges require assessment of the individual’s presumed views:
It is also about more than just presenting the potential client’s opinion. It concerns the individual’s life history, what they have thought, done and truly wanted, and how they now perceive the situation and would perceive it if they understood everything. (LE4)
Hearing all parties thoroughly and comprehensive investigation were also considered highly significant for the final decision, as evidenced by the following quote:
In a way, the individual’s true situation, reality, becomes apparent in these investigations, and quite often leads to the rejection of guardianship applications. (LE7)
It is noteworthy that the option to appoint a legal counsel was mostly nominal according to the district judges, though it should be the primary option according to the law. Generally, district judges appointed a guardian ad litem for individuals with dementia instead of a legal counsel:
I almost always appoint a guardian ad litem – specifically a guardian ad litem and not a legal counsel. Because based on that [medical report], I have determined that their understanding has already diminished to the extent that they may not be able to independently manage the legal proceedings. (LE5)
The preference for appointing guardians ad litem may be due to the need to protect the client for the reason mentioned in the above quote. Alternatively, it may reflect the judge’s desire to hear a guardian ad litem’s perspective on a case. Notably, some legal experts have observed that, ideally, a guardian ad litem should communicate not only their client’s opinion but also their own assessment regarding the client’s need for legal guardianship.
However, one district judge admitted to occasionally bypassing this stage of the process:
I confess that sometimes I determine the need for guardianship to be clear, in that the individual doesn’t understand what is in their best interest at all, and legal protection does not require the appointment of a guardian ad litem. In this case I directly appoint a guardian, thinking that they can appeal to the Court of Appeal. This is probably not entirely in line with the principle of autonomy, because they no longer know how to appeal. (LE6)
Previous research has identified mental incapacity as one of the barriers to older people’s access to justice. 55 The quote above indicates that, despite the recognition of this barrier caused by mental incapacity, legal protection for individuals with dementia remains, at times, nominal.
Most of the legal experts highlighted that an important method to ensure autonomy is ex officio investigation. In other words, when a guardianship matter has been brought before the guardianship authority or a court, they must, by their own motion, determine whether the conditions for legal guardianship are met. This encompasses the proactive determination and thorough examination of factors influencing the necessity for appointing a guardian:
Well, maybe the consideration of the legal grounds for guardianship is then . . . a bit like that, where the case is very carefully scrutinised ex officio. (LE8)
The duty to investigate the case ex officio is based on Sections 78 and 91 of the Guardianship Services Act. The duty to conduct an ex officio investigation supports autonomy by ensuring that legal experts cannot automatically make conclusions on the case based solely on the fact that the individual has not provided a reply to the documents sent to them by the guardianship authority or a court. Failure to provide a written reply to the guardianship authority’s letter or to a court’s summons regarding the guardianship case cannot be interpreted as consent to the appointment of a guardian:
It is essential to ascertain whether the absence of a written reply from a potential client definitively means they do not oppose guardianship, or if it is the case that they oppose but have been unable to express their opposition. (LE9).
One interviewee mentioned becoming more actively involved to resolve these situations:
We often have to consider whether we need to personally visit the individual or, for example, contact healthcare staff – such as a medical social worker. (LE9)
Among the legal experts, several district court judges particularly highlighted flexibility in court proceedings. In practice, district judges have significant authority over how court proceedings are handled. Many district judges use this authority to ensure that the potential client is heard, as was mentioned as one of the goals of flexibility. For instance, being heard was regarded as such an important fundamental human right that a separate form for use in guardianship cases was developed in one district court. This form is delivered to potential client along with other documents related to the case. The following quote from a judge illustrates the practice of the district court:
We have made a very simple form, with very large letters so that even those with poor eyesight can read it. It simply states that the national guardianship authority has requested that a guardian be appointed to manage your financial affairs. Then there are checkboxes for ‘I agree’ and ‘I oppose’, ‘I want someone else to be my guardian’, ‘Anything else I want to say’, ‘Date and signature’ and then ‘Who helped fill out the form’. (LE7)
Neither the GSA nor the Code of Judicial Procedure require or mandate the use of such a form, which the judge who spoke about it also acknowledged. However, the judge considered that the use of the form is still justified:
This procedure is not fully compliant with the law, but it is in line with the purpose of the law. Perhaps we could think that an individual’s right to be heard in a guardianship matter is a human right, and the purpose of the law goes beyond its wording. (LE7)
Most judges also reported being flexible with the procedural order of disputes. Judges often described how the hearing on appointing a guardian should be organised according to the letter of the law but stated that they acted differently. Instead of strictly following the procedural order of disputes, the procedure was intended to be an occasion that best serves the goals of hearing and respecting the autonomy of the person with dementia. An example of this is the following quote:
I consider the hearing to be a positive and down-to-earth discussion forum, and I don’t aim to follow any procedural order for disputes, as I find it completely inappropriate for this type of case, and it doesn’t work. I aim for a conversational approach, with the constant goal of potentially reaching a consensus on the matter. (LE9)
The quote indicates that some legal experts consider hearing the individual to protect a central human right, to the extent that they are willing to deviate from rigid legal requirements to ensure that individuals with dementia are heard and their opinions considered. It is also noteworthy that not a single district registrar criticised the district judges for being flexible in court proceedings.
In addition, a few district judges openly stated that they inform the individual about the possibility of bringing the need for legal guardianship back to the court for reconsideration:
I tell the client that this may not necessarily be a final decision, that the decision can be revoked if the need no longer exists. (LE4)
Such guidance exceeds the court’s obligation to provide instructions for appeal. 56 Providing guidance demonstrates a positive attitude towards autonomy on the part of the interviewees. It can be seen as supporting autonomy, although reassessment is primarily a theoretical possibility in cases of dementia, which is a progressive disease.
Minimising interference with autonomy
This main category consists of three subcategories: (1) Legal guardianship is a secondary measure, (2) Legal guardianship should take the least restrictive form possible and (3) The guardian chosen by the individual is prioritised.
All the legal experts emphasised that legal guardianship is a secondary measure in the management of an individual’s affairs. They stated that legal guardianship is considered only when no less restrictive alternative is found to be appropriate or available, which was noted to be due to the requirements of the Guardianship Services Act. This perspective is summarised in the following quotation:
The law sets the criteria that a person must be unable to manage their affairs due to their health condition and that there must be matters to be managed that cannot be managed by less restrictive means than guardianship. Even if their health is poor, if a close relative is already entitled to use their bank account, then matters can be handled by less restrictive means than guardianship. We do not proceed with the matter unless there is evidence of misuse or other issues. (LE14)
In addition, many interviewees stated that autonomy is respected in such a way that guardianship for personal matters, such as deciding on residence or giving consent to care, has a higher threshold than legal guardianship for financial matters. Instead of appointing a guardian, an individual with dementia is more likely to be allowed to make somewhat disadvantageous decisions regarding their personal affairs:
So, the threshold to appoint a guardian to make decisions on another person’s care, living arrangements or such matters, is really high; it usually involves cases where the person is clearly causing harm to themselves. (LE20)
One factor that raises the threshold for appointing a guardian for personal matters in Finland is that according to the Act on the Status and Rights of Patients (1992/785), consent for a patient’s treatment or for a certain measure to be taken can also be given by a close relative or other person closely connected with the patient if the patient cannot decide on the treatment to be given to them (Sections 6.2 and 6.3). In practice, this means that the matter can often be handled by a less restrictive measure than appointing a guardian. 57
All the legal experts emphasised that autonomy should be respected by legal guardianship taking the least restrictive form possible. First, this is evident in the requirement that the guardianship should be as narrowly defined as possible, covering only those tasks for which guardianship is necessary:
We must intervene as little as possible. It is important that a guardian is appointed only for the tasks that absolutely require it. This is how autonomy is respected. (LE4)
Second, the effort to minimise restrictions is evident in the fact that rulings limiting an individual’s legal capacity, which significantly interfere with autonomy, are exceptional. The following quote exemplifies this:
I don’t recall any declarations of legal incompetence in recent years, except perhaps for cases where such a declaration has been revoked. Restrictions on legal capacity have also significantly decreased, and I can’t recall having to resort to such measures in cases related to dementia. (LE15)
This observation aligns with Finnish statistics on legal capacity restrictions. The number of legal capacity restrictions significantly decreased from the early 2010s to the early 2020s. While in the early 2010s the legal capacity of approximately 50 individuals was restricted per year, by the early 2020s this number had decreased to around 15 individuals per year. 58 This highlights a substantial shift in the approach to the management of legal capacity over the decade. Although it is not typical to limit the legal capacity of individuals with dementia, the neuropsychiatric symptoms sometimes associated with dementia can lead to issues such as financial recklessness, 59 necessitating consideration of such measures. 60 Thus, despite their exceptional nature restrictions on legal capacity are not entirely excluded for individuals with dementia.
The rarity of restrictions on legal capacity is primarily attributed to legal requirements. However, some legal experts questioned whether it is necessary to limit legal capacity through a separate court decision at all. Legal guardianship was found to restrict a client’s ability to manage their own affairs even in its mildest form. This perspective is substantiated by legal research, which highlights the adverse impacts of legal guardianship on individual autonomy.
61
This criticism is also illustrated by the following quote:
When a guardianship is entered into the guardianship register, the supervision of the client may be stricter than necessary. This restricts their ability to act, even if they have legal capacity. Potential creditors may hesitate to grant credit, fearing it might later be invalidated, and all other avenues are closed as well. (LE16)
In addition, one legal expert noted that sometimes there is no need to restrict legal capacity because the client is unaware that they retain their legal capacity alongside the guardian:
It is fortunate that many clients believe they cannot do anything. In a way, it is positive that they think the guardian handles everything. I think that if the clients knew they were fully legally competent to perform legal acts, they would do so more often. (LE14)
This unawareness may serve as a protective mechanism, as highlighted by the quote, as clients do not always understand that they are allowed to engage in legal actions. This might lead to more compliance with guardianship decisions, as individuals might not challenge the authority’s actions. Nevertheless, clients’ lack of awareness of their own rights raises ethical questions about the transparency of authorities’ actions and the realisation of individuals’ autonomy and rights. If no one corrects the individual’s unawareness, the outcome for their daily life and perceived well-being is likely to be very similar, regardless of whether their legal capacity is formally restricted or stems from their own belief that it is restricted.
Respect for autonomy is also evident in the requirement that the guardian chosen by the individual is prioritised. This means that compelling reasons are needed to appoint a guardian whose identity is out of line with the individual’s views. The compelling reasons must be concrete and clear in order to override the client’s preference of guardian:
Of course, if the client has a clear desire to have someone as their guardian, I don’t really see why the court would not appoint that person. There must be strong counterarguments, such as evidence of abuse, conflict of interest, or some other concrete reason why the person desired by the client would not be suitable as a guardian. (LE16)
According to the Guardianship Services Act, the person appointed as a guardian must be suitable. In the assessment of suitability, the skills and experience of the nominee and the nature and extent of the duties must be taken into consideration, among other things (Section 5). Legal experts focused more on clear factors determining unsuitability rather than the suitability criteria given in the Act. The most common reason cited for the unsuitability of a guardian was debt enforcement:
Well, if there are 19 pages of debt enforcement records, then sorry, the potential client’s wishes can no longer be followed. (LE17)
Previous research has shown that older people count on their relations and safety nets for support to make decisions and plans. 62 Therefore, it is natural that persons with dementia also wish for a close person to be their guardian instead of a public guardian. If the individual’s wish to avoid the appointment of a guardian cannot be fulfilled, the least that can be done to respect their autonomy is to strive to respect their views regarding the identity of the guardian.
Physicians’ descriptions of respect for autonomy
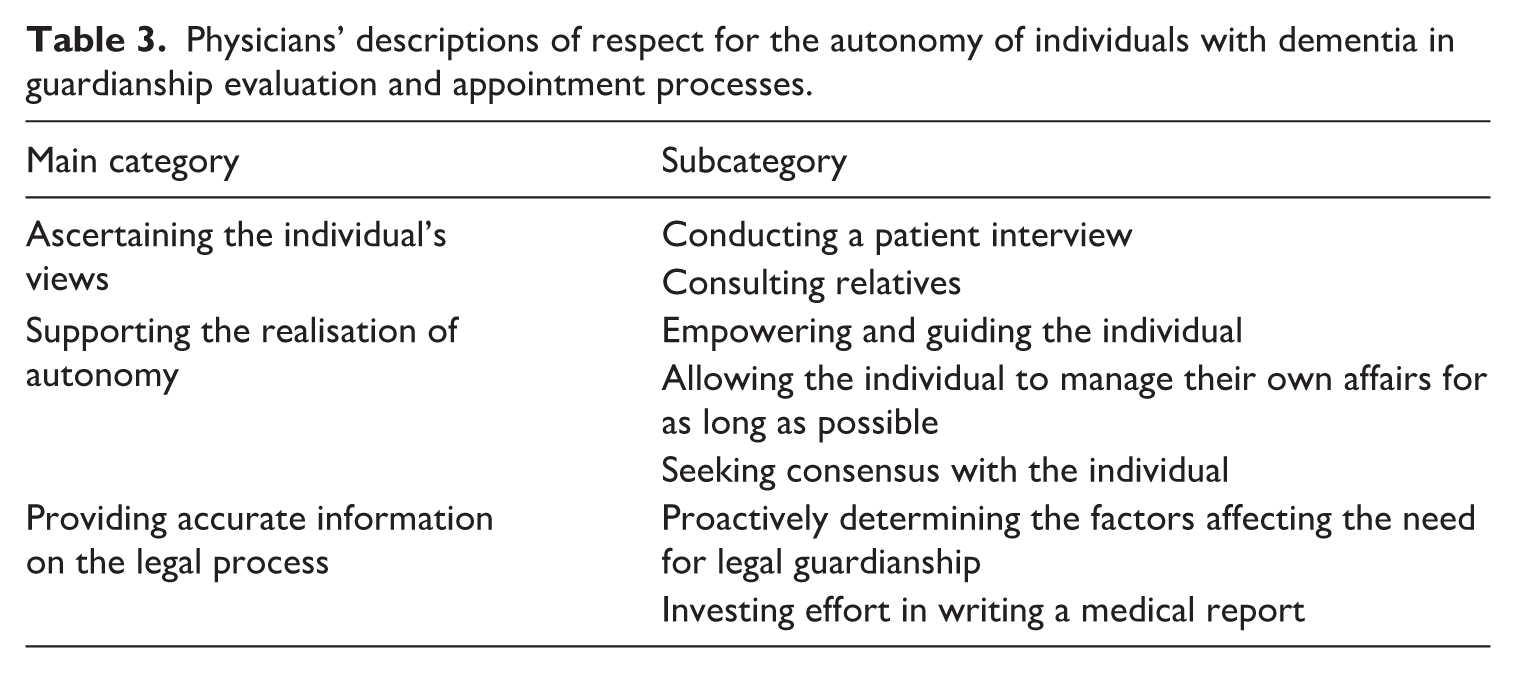
The physicians’ responses were categorised into three main categories: (1) Ascertaining the individual’s views, (2) Supporting the realisation of autonomy and (3) Providing accurate information on the legal process. The main categories and subcategories of the physicians’ answers are presented in Table 3.
Physicians’ descriptions of respect for the autonomy of individuals with dementia in guardianship evaluation and appointment processes.
Ascertaining the individual’s views
This main category encompasses two subcategories: (1) Conducting a patient interview and (2) Consulting relatives.
All the physicians stated that conducting a patient interview is fundamental in assessing the need for legal guardianship, in order to ensure that their views are heard and respected. The interviewees also highlighted that efforts are made to respect verbally expressed views whenever possible:
I ask the patient their opinion on guardianship, as even the medical statement requires that the individual’s opinion be sought. I do not push for guardianship without clear grounds but rather follow what the individual wants. (P22)
This quote shows that the national guardianship authority’s template for medical reports indeed guides doctors to hear potential clients’ opinions. Several physicians also emphasised the way the interview should be conducted. Particular attention was paid to ensuring that the interview takes place without the presence of family members:
If a family member is present during the interview, they might take over and answer all the questions on behalf of the patient. Therefore, it is very important to meet the patient one-on-one. (P21)
Consideration of the individual’s current views and preferences, as highlighted by the interviewees, plays a pivotal and intrinsic role in the process of capacity determination. 63 It is practically impossible to ascertain an individual’s perspective without hearing them in person. Furthermore, the literature emphasises the importance of interviewing the individual alone and for a sufficient time. 64
In addition, a close and trusting relationship between the physician and the patient was also seen as a prerequisite for a successful interview, especially in situations where the patient is in a very vulnerable position:
The older, frailer, and weaker the elderly person is, the smaller their voice becomes compared to the voices of their family members. And family members do not always represent the best interests of the elderly. As a physician, you need to get close enough to the elderly person that they feel safe to express their own wishes. (P30)
This physician’s observation is consistent with the fact that older people are not often used to sharing ideas on their personal beliefs and commitments. 65
All physicians said that consulting relatives is an important means to ascertain the individual’s views and avoid unnecessary appointment of a guardian. However, consulting relatives was sometimes described as an ideal, as the reality is that not all patients have relatives, or the physician may not always be able to talk with them. The importance of consulting relatives in order to ascertain the individual’s prior views was emphasised:
I ask my patients to name an individual that knows them well and with whom I could discuss the case with their permission. I then ask that person about what kind of thoughts my patient had, even twenty years ago, about the world, life, and their property in the future. Well, what were the important things for him or her? Because primarily, I would like to act as the patient would have always wanted their physician to act [regarding guardianship] before this illness occurred. (P20)
This quote indicates that the relatives of a person with dementia can play a significant role in determining what that individual’s prior views and preferences were before the onset of dementia. At the same time, it highlights the fact that a physician cannot contact a patient’s relatives without the patient’s consent. Balancing the prior and current views of persons with dementia is complex. The concept of precedent autonomy supports the idea that the views expressed by individuals before the onset of dementia should be respected. However, adhering to the prior views of individuals with dementia, especially if they later express that they have changed their mind, has faced criticism. 66
Consulting relatives was also seen to ensure that protective measures are only taken if inappropriate behaviour is due to illness, not individual personality traits:
I always try to find someone who knows the patient well and can confirm whether this behaviour is new, which would indicate dementia, or if the person has always been like this, which could mean it is part of the patient’s personality and characteristic behaviour, that it is their lifestyle and a choice. In such cases, the threshold for intervention is significantly higher. (P21)
It is common for the personality and behaviour of individuals with dementia to change. 67 However, unusual behaviour or behaviour that goes against one’s own interests does not always relate to dementia; it may simply reflect an individual’s unique personality. As noted in the above quote, the GSA stipulates that legal guardianship should be considered when the individual has a specific illness or otherwise impaired health condition.
Interestingly, many physicians pointed out that consulting relatives also serves the opposite purpose. Relatives play a crucial role in providing information if a potential client’s perspective on their own situation is unreliable, for example, due to anosognosia. In this way, consulting relatives can have a limiting effect on a potential client’s autonomy rather than supporting it.
Some participants also noted that consulting relatives may involve risks, for example if the relatives are unreliable. However, even the physicians who spoke about these risks emphasised that consulting relatives is important. To obtain a reliable picture of a potential client’s situation, information must be gathered as broadly as possible.
Experience has taught me not to take anyone’s word without questioning it. It is best to listen and try to investigate while remaining very impartial. But still to gather information as comprehensively as possible. (P30)
In addition, the physicians stressed the importance of careful execution of interviews with the potential client:
If there is any discrepancy between the accounts of the patient and their relatives, you must discuss this with the patient one more time. And absolutely ensure that no relatives are present. (P20)
Overall, family members can play a crucial role in enabling an individual’s autonomy, provided the physician considers family dynamics and patient safety when family members are present during a physician’s appointment. 68
Supporting the realisation of the right to autonomy
The meaning of supporting the realisation of the right to autonomy was described in terms of three subthemes: (1) Empowering and guiding the individual, (2) Allowing the individual to manage their own affairs for as long as possible and (3) Seeking consensus with the individual.
Some physicians concluded that empowering and guiding the individual to exercise their autonomy is an essential part of their work. Physicians considered it important for patients to actively participate in managing their own affairs and to exercise their autonomy as much as possible:
We always investigate whether an enduring power of attorney exists, and if it does, we discuss with the patient whether to exercise it at this stage or not. The power of attorney simplifies matters, as guardianship is a bigger issue for many, including both the patient and the relatives. (P21)
The following quote demonstrates how dementia patients are guided to exercise their autonomy and actively work towards their overall well-being at a geriatric clinic:
We strive to empower patients. We place strong emphasis on non-pharmacological treatments and encourage patients to participate in their own care, particularly in terms of exercise and nutrition. When a patient comes for a first appointment, they are asked if they have made an advance health directive or enduring power of attorney. If they have not, our nurse provides information about these options. At the follow-up appointment, approximately six months later, we check whether the patient has taken any legal anticipatory steps. If not, we provide further briefing and encouragement to take these steps. (P13)
Such counselling is very supportive of autonomy, as older people sometimes lack knowledge about the various options available for successful later life legal planning, 69 even though different measures and tools for legal planning are essential elements to secure the autonomy of people with dementia. 70 Overall, the involvement of health care professionals in facilitating the realisation of the rights of people with dementia is essential. 71 By receiving information and encouragement related to the establishment of an enduring power of attorney, an individual can proactively prepare for incapacity and avoid legal guardianship, as their affairs are properly managed in another way. 72 This kind of autonomy-supporting and comprehensive counselling goes beyond health professionals’ obligation to provide information and guidance. 73
Most physicians also considered that autonomy is primarily reflected in allowing the individual to manage their own affairs for as long as possible. The patient’s views should be respected if the patient does not endanger their own well-being or that of others:
If the patient strongly opposes guardianship but is safe, does not harm themselves or others, and has access to services such as meal delivery and home nursing, then guardianship should be avoided. (P6)
This perspective is well aligned with the principle of using the least restrictive means possible, as contemplated in the legislation concerning legal guardianship.
74
However, some physicians deemed protection of the patient so paramount that the need for legal guardianship was primarily determined by the hypothetical worst-case scenario if a guardian was not appointed:
[To meet the need for guardianship] it is enough to have [impaired] understanding, because one day, for example, a telemarketer or some salesperson might come. Additionally, there are many close relatives who try to take advantage of people with dementia. So, it is the hypothetical idea of what would be the worst that could happen. (P29)
Such a view, which primarily emphasises threat assessment rather than evaluating whether the individual has personal or financial affairs that need to be managed, elevates the protection of the individual above autonomy. This perspective is not entirely in line with the requirements for legal guardianship as outlined in the Guardianship Services Act.
Furthermore, although respect for autonomy was generally considered important, the high threshold for appointing a guardian also received strict criticism from a few physicians:
From a doctor’s perspective, nowadays, the protection of autonomy has become so prioritised, even in cases of dementia, that a guardian is often appointed too late. (P1)
Some physicians pointed out that seeking consensus with the individual is part of respecting their autonomy. These physicians described how patients often understand the need for legal guardianship when they are openly informed about the nature of dementia and the purpose of a guardian:
Usually, when it is calmly explained to the patient that dementia is an insidious disease and causes problems that the patient does not notice themselves, things generally go well. Patients feel heard and understand that their financial situation is being safeguarded [by appointing a guardian] to prevent them from doing harm to themselves. (P25)
Striving for consensus was also considered important even in situations where the physician’s and the patient’s views on the need for legal guardianship do not align in the end:
If there are clear grounds for guardianship being genuinely necessary, then the statement is made to protect the patient. However, even in such situations, it must be communicated to the patient, and an attempt should be made to reach a consensus. (P20)
The interaction and mutual understanding between the physician and patient are central to patient autonomy and the physician-patient relationship. Investing in these aspects is worthwhile, as successful interaction not only supports patient autonomy but also positively influences their satisfaction, the development of trust and treatment outcomes. 75
Providing accurate information on the legal process
This main category consists of two subcategories: (1) Proactively determining the factors affecting the need for legal guardianship and (2) Investing effort in writing a medical report.
Most physicians emphasised their responsibility to proactively determine the factors affecting the need for legal guardianship. The methods physicians use to assess the patient’s situation were described as multidisciplinary collaboration with other social and healthcare professionals:
The doctor needs a lot of information, often from a social worker, nurse specialised in neurocognitive diseases, or case coordinator in addition to the patient. Sometimes we also use occupational therapists to determine the patient’s actual functional capacity. So, assessment is often quite multi-professional. (P7)
Such proactive investigation supports the patient’s autonomy if it is determined that the patient’s affairs are being managed appropriately, but it can also result in the determination that the patient needs protection through legal guardianship.
Many physicians emphasised the obligation to invest effort in writing a medical report. As an autonomy-emphasising factor related to the content of the medical report, these interviewees highlighted the importance of recording the differing opinions regarding a potential client’s need for legal guardianship:
If necessary, I document that relative A says this, relative B says that, and the patient themself holds this opinion. I strive to ensure that these details are visible in the medical report when it is submitted to the deciding authority. (P24)
However, several physicians noted that the medical report should also include information that may have implications for autonomy if this information is crucial for the individual’s protection:
The report should reflect whether we have records of abuse by relatives. And if a relative is not suitable as a guardian, I have also documented that, in my opinion, the individual requires a public guardian. (P5)
Indeed, a public guardian may be appointed if there are no suitable family members or if family members are deemed unsuitable to act as guardians. 76
Conclusion
In this study, we investigated the views of physicians and legal experts regarding consideration of individual autonomy when assessing the need for and appointing a guardian for individuals with dementia. The study clarifies the methods and principles used by legal experts and physicians to ensure respect for autonomy in guardianship cases. As a whole, this study demonstrates that legal experts and physicians are aware of the essential nature of autonomy and its three dimensions, as outlined in the introduction. However, it also highlights certain shortcomings in how these aspects of autonomy are realised from the perspective of potential clients.
Both professional groups agreed that hearing the individual is fundamental to respecting autonomy. Notably, district judges, part of the group of legal experts, considered hearing the individual a central human right to such an extent that they were willing to deviate from rigid legal requirements during court proceedings to ensure that individuals with dementia were heard and their opinions considered. Not a single district registrar criticised the district judges for their flexible approach to court proceedings. However, despite the emphasis on hearing the individual as a crucial means of respecting autonomy, there were situations where this was compromised due to the high number of cases judges hear. This is a significant shortcoming concerning the autonomy of individuals with dementia, as it infringes particularly upon one of the key dimensions of autonomy – the right to be heard as an integral part of self-determination. In addition, it emerged that in some cases, the legal remedies available to individuals with dementia are merely nominal. This can be seen as a barrier to access to justice, which previous research has shown to be a significant issue for elderly individuals. 77
According to this study, physicians also strive to respect potential clients’ autonomy. However, some physicians thought that the need for protection sometimes supersedes the right to autonomy, and that an individual may need a guardian to safeguard them and to prevent the worst-case scenario from happening. Furthermore, the high threshold for legal guardianship was criticised by a few physicians. Thus, although physicians generally emphasised the patient’s right to manage their own affairs for as long as possible, protection of the individual was emphasised more compared to the responses of legal experts. Among the legal experts appointing a guardian was truly seen as a secondary measure to manage an individual’s affairs. This highlights that an attitude of strong respect for autonomy has been adopted among legal experts.
This study supports the conclusion of previous research that guidance provided by health care personnel is important for individual autonomy. 78 Although legal experts also provide autonomy-supporting advice on guardianship matters, such as pointing out the possibility of having the case re-examined by the court, their advice often comes so late that it no longer has practical significance in dementia cases.
The study also highlighted that restricting legal capacity is very rare in the context of dementia, which is in line with the statistics. 79 This is not surprising, as according to the law interference with an individual’s legal capacity should be avoided, but also because some legal experts do not even recognise, for example, the neuropsychiatric symptoms of dementia as indicating a need for legal guardianship. 80 This is despite the fact that neuropsychiatric symptoms can cause behaviour that puts a person’s financial situation at risk, 81 which is a fundamental basis for legal guardianship. 82 This raises the question of whether autonomy is sometimes respected to the extent that protection becomes insufficient. However, the study revealed that formal restriction of legal capacity is often practically unnecessary. The research findings also highlighted that individuals do not always know that their legal capacity does not end with the appointment of a guardian, which reduces the need for restriction of legal capacity. A client’s unawareness of their own rights involves ethical concerns. If this unawareness is not addressed, its impact on the individual’s daily life will likely be the same whether or not their legal capacity is formally restricted by a court’s decision.
To address the shortcomings identified in this study is of considerable importance for ensuring access to justice for individuals with dementia. Despite the emphasis placed on hearing the potential client in the GSA and the precedent KKO:2012:109, practical implementation reveals notable deficiencies. These shortcomings persist even though legal experts are aware of the normative guidance. To remedy these issues, it is essential to increase resources allocated to the courts, ensuring that heavy workloads do not lead district judges to bypass the hearing of potential clients. Furthermore, it is crucial to provide additional training on the value of autonomy, the importance of hearing the individual, and the ethical dimensions of such practices.
In addition, access to legal advice must be improved so that individual can receive support before significant deterioration in their mental capacity. This would enable them to engage in legal foresight and planning, thereby making greater use of autonomy-enhancing legal instruments such as a continuing power of attorney.
The strengths of this study include the integration of legal and medical perspectives on autonomy. In addition, the study benefits from a large sample of interviewees, which enhances the reliability of the findings. 83 Furthermore, sufficient depth of information was ensured through individual interviews conducted by a trained interviewer. The collaboration between legal researchers and a neurologist bolstered the reliability of data collection and analysis. The research group possessed substantial practical and scientific expertise in this field. By integrating insights into legal norms and prevailing legal practices with clinical perspectives into cognitive decline and patient interaction, the study enabled a nuanced examination of how autonomy is interpreted and operationalised in practice.
A limitation is that the data were collected solely in Finland. This must be considered when assessing the international generalisability of the results, as procedural laws and practices regarding legal guardianship vary between countries.
Footnotes
Acknowledgements
None.
Author contributions
Kaisa Näkki: Conceptualisation; formal analysis; data curation; writing original draft; review and editing.
Anna Mäki-Petäjä-Leinonen: Conceptualisation; review and editing; resources.
Kaijus Ervasti: Conceptualisation; review and editing.
Eino Solje: Conceptualisation; review and editing; resources.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Finnish Brain Foundation [grant number 20210092]; the Kone Foundation [grant number 202105674]; the Olga and Kaarle Oskari Laitinen Foundation; the Centenary Foundation of Kymi Corporation; the Foundation of the Finnish Bar Association (Suomen Asianajajaliiton Säätiö sr.); the Research Council of Finland [grant number 355192]; State Research Funding; the Sigrid Juselius Foundation; the Finnish Medical Foundation, and the Wihuri Foundation. Funders did not have any role in the conceptualisation, design, data collection, analysis, decision to publish or preparation of the manuscript.
Ethical considerations
The Ethics Committee of the University of Eastern Finland stated that this study did not need ethics committee approval according to Finnish Law (letter from the committee of 8 December 2021).
Consent to participate
All participants in this study provided informed consent to participate, which was confirmed verbally during the audio-recorded interview.
Data availability
Due to the identifiable nature of the interviews, the raw data are not openly available. However, anonymised data may be shared at the reasonable request of a qualified investigator for the purposes of replicating the procedures and results.
1.
See e.g. I. Berliin, ‘Two Concepts of Liberty’ in I. Berlin ed., Four Essays on Liberty (Oxford: Oxford University Press, 1969), pp. 118–172; J. Feinberg, ‘Harm to Self, vol. III’ in J. Feinberg ed., The Moral Limits of Criminal Law (Oxford: Oxford University Press, 1986), ch 18-19; T. Hill, Autonomy and Self-Respect (Cambridge: Cambridge University Press, 1991), ch 1-4.
2.
T. L. Beauchamp and J. F. Childress. Principles of Biomedical Ethics, 7th ed. (New York: Oxford University Press, 2013), p. 459.
3.
https://treaties.un.org/Pages/ViewDetails.aspx?src=TREATY&mtdsg_no=IV-15&chapter=4&clang=_en (accessed 20 May 2025).
4.
R. Harding, ‘Legal Constructions of Dementia: Discourses of Autonomy at the Margins of Capacity’, The Journal of Social Welfare & Family Law 34 (2012), pp. 425–442; R. Harding, Duties to Care : Dementia, Relationality, and Law (Cambridge: Cambridge University Press, 2017), pp. 15–37; M. Aalto-Heinilä, S.-M. Saarelainen, R. Pahia, and A. Mäki-Petäjä-Leinonen, ‘“If I Lose My Mind, She Will Take Care of Me.” The Importance of Relational Autonomy and Legal Planning in Later Life’, Nordic Journal on Law and Society 7 (2024), pp. 1–27.
5.
A. Mäki-Petäjä-Leinonen, ‘Protecting a Person with Dementia through Restrictions of Freedom? Notions of Autonomy in the Theory and Practice of Elder Care’ in A. Griffiths, A. Mäki-Petajä-Leinonen, and S. Mustasaari, eds., Subjectivity, Citizenship and Belonging in Law: Identities and Intersections (London: Routledge, 2016), pp. 146–170.
6.
See e.g. A. Bosco, J. Schneider, D. M. Coleston-Shields, K. Jawahar, P. Higgs, and M. Orrell, ‘Agency in Dementia Care: Systematic Review and Meta-Ethnography’, International Psychogeriatrics 31 (2019), pp. 627–642; M. Altieri, F. Garramone, and G. Santangelo, ‘Functional Autonomy in Dementia of the Alzheimer’s Type, Mild Cognitive Impairment, and Healthy Aging: A Meta-Analysis’, Neurological Sciences 42 (2021), p. 1773; V. M. E. B. Delineau, A. Rita Ferreira, L. Passos, and L. Fernandes, ‘The Impact of Behavioral and Psychological Symptoms of Dementia on Individual’s Autonomy: A Scoping Review’, Archives of Clinical Neuropsychology 40 (2025), pp. 351–362; S. Kinch, F. Schou-Juul, S. S. Skov, N. C. H. Kongsholm, and S. Lauridsen, ‘The Use of Advance Directives for Autonomy in Dementia Care: A Scoping Meta-Review and Thematic Synthesis’, Archives of Gerontology and Geriatrics 126 (2024), p. 105498.
7.
See e.g. Bosco et al., ‘Agency in Dementia Care’, pp. 627–642; J. Bhatt, H. Walton, C. R. Stoner, K. Scior, and G. Charlesworth, ‘The Nature of Decision-Making in People Living with Dementia: A Systematic Review’, Aging & Mental Health 24 (2020), pp. 363–373; and T. Tannou, F. Gzil, S. P. Kennelly, J. Tournoy, V. Frisardi, and P. Soysal, ‘How Do Geriatricians Evaluate Decision-Making Ability for Older Adults with Cognitive Impairment? Results from an European Survey’, European Geriatric Medicine 14 (2023), pp. 953–960.
8.
C. Sinclair, J. Bajic-Smith, M. Gresham, M. Blake, R. S. Bucks, S. Field, J. M. Clayton, H. Radoslovich, M. Agar, and S. Kurrle, ‘Professionals’ Views and Experiences in Supporting Decision-Making Involvement for People Living with Dementia’, Dementia 20 (2021), pp. 84–105.
9.
K. Näkki, A. Mäki-Petäjä-Leinonen, K. Ervasti, and E. Solje, ‘Evaluating the Need for Legal Guardianship in People with Dementia: Gaining Insight Into Professionals’ Assessment Criteria’, International Journal of Law, Policy and the Family 38 (2024), p. ebae005.
10.
K. Näkki, A. Mäki-Petäjä-Leinonen, K. Ervasti, A. Halkoaho, S.-M. Nurmi, A. Solomon, N.-M. Suhonen, A. M. Portaankorva, J. Krüger, and E. Solje, ‘Diverging Medical and Legal Perceptions of the Need for Legal Guardianship in People with Dementia: A Qualitative Study’, European Journal of Neurology 31 (2024), p. e16334.
11.
Näkki et al., ‘Evaluating the Need’, p. ebae005; M. Fallon-Kund, M. Coenen, and J. E. Bickenbach, ‘Balancing Autonomy and Protection: A Qualitative Analysis of Court Hearings Dealing with Protective Measures’, International Journal of Law and Psychiatry 53 (2017), pp. 69–76.
12.
H. de Waal, ‘Rethinking Dementia: How Autonomy and Control Can Be Fostered Through the Development of Person Centred Services’, Working with Older People 18 (2014), pp. 82–89.
13.
R. Ryan and E. Deci. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness (New York: Guilford Press, 2017), pp. 10–12.
14.
M. Meïdy and M. Guillaume, ‘Basic Psychological Needs in Alzheimer’s Disease: A Self-Determination Theory Perspective’ in A. M. Columbus, ed., Advances in Psychology Research: Volume 154 (New York: Nova Science Publishers, 2024), pp. 153–169.
15.
N. Tupanceski and D.Kiprijanovska, ‘Medicine, Law and Human Rights – A Symbiotic Relationship’, Medicine and Law 33 (2014), pp. 40–63.
16.
S. McSwiggan, S. Meares, and M. Porter, ‘Decision-Making Capacity Evaluation in Adult Guardianship: A Systematic Review’, International Psychogeriatrics 28 (2016), pp. 373–384; J. Tsoh, C. Peisah, J. Narumoto, N. Wongpakaran, T. Wongpakaran, N. O’Neill, T. Jiang, S. Ogano, M. Mimura, Y. Kato, and H. Chiu, ‘Comparisons of Guardianship Laws and Surrogate Decision-Making Practices in China, Japan, Thailand and Australia: A Review by the Asia Consortium, International Psychogeriatric Association (IPA) Capacity Taskforce’. International Psychogeriatrics 27 (2015), pp. 1029–1037; A. Ward, ’Legal Protection of Adults – An International Comparison’, Elder Law Journal 147 (2017), pp. 147–159; M. Domański and B. Lackoroński, eds., ‘Models of Implementation of Article 12 of the Convention on the Rights of Persons with Disabilities (CRPD) – Private and Criminal Law Aspects’ (London: Routledge, 2023), pp. 61–605.
17.
K. Zietlow, L. Dubin, A. Battles, and C. Vitale, ‘Guardianship: A Medicolegal Review for Clinicians’, Journal of the American Geriatrics Society 70 (2022), pp. 3070–3079; Domański and Lackoroński, eds., Models of Implementation of Article 12, p. 61–605; M. Donnelly, ‘Best Interests, Patient Participation and the Mental Capacity Act 2005’, Medical Law Review 17 (2009), pp. 1–29.
18.
See e.g. R. Dinerstein, ‘Implementing Legal Capacity Under Article 12 of the UN Convention on the Rights of Persons with Disabilities: The Difficult Road From Guardianship to Supported Decision-Making’, The Human Rights Brief 19 (2011), pp. 8–12; L. Series, ‘Relationships, Autonomy and Legal Capacity: Mental Capacity and Support Paradigms’, International Journal of Law and Psychiatry 40 (2015), pp. 80–91.
19.
M. Hall, ‘Dementia, Autonomy and Guardianship for the Old’ in C. Foster, I. Doron, and J. Herring, eds., The Law and Ethics of Dementia (Oxford: Hart Publishing, 2014), pp. 339–348.
20.
M. Donnelly, R. Harding, and E. Taşcioğlu, ‘Situating the Right to Enjoy Legal Capacity’ in M. Donnelly, R. Harding, and E. Taşcioğlu, eds., Supporting Legal Capacity in Socio-Legal Context (Oxford: Hart, 2022), pp. 1–16; N. Devi, ‘Supported Decision-Making and Personal Autonomy for Persons with Intellectual Disabilities: Article 12 of the UN Convention on the Rights of Persons with Disabilities’, The Journal of Law, Medicine & Ethics 41 (2013), pp. 792–806.
21.
United Nations Committee on the Rights of Persons with Disabilities. 2014. General Comment No. 1 Article 12: Equal recognition before the law. UN Doc CRPD/C/GC/1 (19 May 2014)
22.
See e.g. K. Booth Glen, ‘Changing paradigms: Mental Capacity, Legal Capacity, Guardianship, and Beyond’, Columbia Human Rights Law Review 44 (2012), pp. 93–169; E. Wood, P. Teaster, and J. Cassidy, Restoration of Rights in Adult Guardianship: Research & Recommendations (Washington, DC: American Bar Association, 2017); A. Mäki-Petäjä-Leinonen, ‘Autonomy of a Person under Guardianship: Self-determination on the Theory and Practice on Guardianship Law in Finland’ in M. Donnelly, R. Harding, and E. Taşcioğlu, eds., Supporting Legal Capacity in Socio-Legal Context (Oxford, Hart Publishing, 2022), pp. 215–233.
23.
R. Diller, ‘Legal Capacity for All: Including Older Persons in the Shift from Adult Guardianship to Supported Decision-Making’, Fordham Urban Law Journal 43 (2016), pp. 495–538.
24.
M. Jameson, T. Riesen, S. Polychronis, B. Trader, S. Mizner, J. Martinis, and D. Hoyle, ‘Guardianship and the Potential of Supported Decision Making with Individuals with Disabilities’, Research and Practice for Persons with Severe Disabilities 40 (2015), pp. 36–51.
25.
Fallon-Kund et al., ‘Balancing Autonomy and Protection’, pp. 69–76.
26.
A. Arstein-Kerlsake and E. Flynn, ‘The General Comment on Article 12 of the Convention on the Rights of Persons with Disabilities: A Roadmap for Equality Before the Law’, The International Journal of Human Rights 20 (2016), pp. 471–490; M. Freeman, K. Kolappa, J. M. C. de Almeida, A. Kleinman, N. Makhashvili, S. Phakathi, B. Saraceno, and G. Thornicroft, ‘Reversing Hard Won Victories in the Name of Human Rights: A Critique of the General Comment on Article 12 of the UN Convention on the Rights of Persons with Disabilities’, Lancet Psychiatry 2 (2015), pp. 844–850; G. Szmukler, “UNCRPD: Equal Recognition Before the Law”, Lancet Psychiatry 2 (2015), p. e29; D. Pūras, ‘Human Rights and Mental Health Care – Can We Find a Common Ground?’ European Psychiatry 33 (2016), pp. S3–S4.
27.
M. Rogers, J. E. Storey, and S. Galloway, ‘Elder Mistreatment and Dementia: A Comparison of Older People with and without Dementia across the Prevalence of Abuse’, Journal of Applied Gerontology 42 (2023), pp. 909–918.
28.
A. Mäki-Petäjä-Leinonen and K. Juva. ‘Of Sound Mind? Dementia and Aspects of Assessing Legal Capacity’, European Journal of Health Law 22 (2015), pp. 13–37.
29.
Rogers et al., ‘Elder Mistreatment’, pp. 909–918; D. Marson, ‘Loss of Financial Competency in Dementia: Conceptual and Empirical Approaches’, Aging, Neuropsychology, and Cognition 18 (2001), pp. 164–181.
30.
Donnelly et al., ‘Right to Enjoy Legal Capacity’, pp. 1–16.
32.
Several European countries, such as Sweden, Denmark, Germany and Austria, have enacted legislation like Finland’s to protect individuals unable to manage their affairs due to declining health or similar reasons; Government proposal HE 146/1998 vp 18; T. Mikkola, Family and Succession Law in Finland (Alphen aan den Rijn: Kluwer International B.V., 2022), pp. 70–72.
33.
P. Välimäki, Edunvalvontaoikeus (Helsinki: Talentum Media 2013), p. 19.
34.
The principle of using the least restrictive means to arrange for an individual’s affairs was emphasised in Government proposal HE 146/1998 vp, pp. 10; See S. Silvola and A. Mäki-Petäjä-Leinonen, ‘The Empowerment and Protection of Vulnerable Adults: Finland.’ Country Report, Family & Law (Amsterdam: FL-EUR, 2024)
35.
Mäki-Petäjä-Leinonen, ‘Autonomy of a Person’, pp. 215–233.
36.
In the government proposal, persons with disabilities in Finland are considered equal to other individuals in terms of legal capacity. It is also stated that the restrictions on legal capacity imposed under the GSA are not discriminatory against persons with disabilities. Government proposal HE 284/2014 vp, pp. 42–43.
37.
In legal literature, these procedural provisions are particularly regarded as safeguarding autonomy, especially when considering elderly individuals with diminished capacity. Mäki-Petäjä-Leinonen, ‘Autonomy of a Person’, pp. 215–233.
38.
Government proposal HE 146/1998 vp, p. 19.
39.
Op. cit., p. 31.
40.
Op. cit., p. 19.
41.
Op. cit., p. 65.
42.
See e.g. P. Välimäki. Holhoustoimen pääpiirteet (Vantaa: Talentum Media, 2008), pp. 147–150.
43.
Government proposal HE 146/1998 vp, p. 64.
44.
Op. cit., pp. 67–68.
45.
Sosiaali- ja terveysministeriö. 1999. Lääkärinlausunto holhousasioissa: Sosiaali- ja terveysministeriön määräyskokoelma [The Decree Collection of the Ministry of Social Affairs and Health] 51(1999).
46.
47.
Guardianship Service Act (442/1999), Section 1 and Section 24.
48.
M. Patton, Qualitative Evaluation and Research Methods, 4th ed. (Thousand Oaks, CA: Sage, 2015).
49.
Näkki et al., ‘Evaluating the Need’, p. ebae005.
50.
Näkki et al., ‘Diverging Perceptions’, p. e16334.
51.
A. Galletta, Mastering the semi-structured interview and beyond: From research design to analysis and publications (New York: NYU Press, 2013).
52.
V. Braun, V. Clarke, N. Hayfield, and G. Terry, ‘Thematic Analysis’ in Pranee Liamputtong, ed., Handbook of Research Methods in Health Sciences (Singapore: Springer, 2018), pp. 1–18.
53.
B. O’Brien, I. B. Harris, T. J. Beckman, D. A. Reed, and D. A. Cook, ‘Standards for Reporting Qualitative Research: A Synthesis of Recommendations’, Academic Medicine 89 (2014), pp. 1245–1251.
54.
Mäki-Petäjä-Leinonen, ‘Autonomy of a Person’, pp. 225–230.
55.
Sarah Ellison, L. Schetzer, J. Mullins, J. Perry, and K. Wong, Access to Justice and Legal Needs: The Legal Needs of Older People in NSW (Sydney, NSW, Australia: Law and Justice Foundation of New South Wales, 2004).
56.
The Code of Judicial Procedure (4/1734), Chapter 25 Section 3.
57.
See Silvola and Mäki-Petäjä-Leinonen, ‘The Empowerment and Protection’, pp. 52–53.
59.
F. Kumfor, G. Wei, N. Ries, H. Bennett, M. D’Mello, C. Kaizik, O. Piguet, and J. R. Hodges, ‘Examining the Propensity and Nature of Criminal Risk Behaviours in Frontotemporal Dementia Syndromes and Alzheimer’s Disease’ Alzheimer’s & Dementia 16 (2024), p. e12577.
60.
Näkki et al., ‘Diverging Perceptions’, p. e16334.
61.
Mäki-Petäjä-Leinonen, ‘Autonomy of a Person’, pp. 215–233.
62.
S.-M. Saarelainen, A. Mäki-Petäjä-Leinonen, and R. Pöyhiä, ‘Relational Aspects of Meaning in Life among Older People – A Group-interview Gerontechnology Study’, Journal of Aging and Society 42 (2022), pp. 1035–1053.
63.
J. Moye, S. W. Butz, D. C. Marson, and E. Wood; ABA-APA Capacity Assessment of Older Adults Working Group, ‘A Conceptual Model and Assessment Template for Capacity Evaluation in Adult Guardianship’, The Gerontologist 47 (2007), pp. 591–603.
64.
Mäki-Petäjä-Leinonen and Juva. ‘Of sound mind?’, pp. 13–37.
65.
Saarelainen et al., ‘Meaning in Life’, pp. 1035–1053.
66.
Y. Huang, Y. Cong, and Z. Wang, ‘Rethinking the Precedent Autonomy, Current Minimal Autonomy, and Current Well-Being in Medical Decisions for Persons with Dementia’, Journal of Bioethical Inquiry 19 (2022), pp. 163–175.
67.
See e.g. H. Kales, L. N. Gitlin, and C. G. Lyketsos, ‘Assessment and Management of Behavioral and Psychological Symptoms of Dementia’, BMJ 350 (2015), p. h369; T.-B. Robins Wahlin and G. Byrne, ‘Personality Changes in Alzheimer’s Disease: A Systematic Review’, International Journal of Geriatric Psychiatry 26 (2011), pp. 1019–1029.
68.
F. Omole, C. M. Sow, E. Fresh, D. Babalola, and H. Strothers 3rd, ‘Interacting with Patients’ Family Members during the Office Visit’, American Family Physician 84 (2011), pp. 780–784.
69.
K. Purser, T. Cockburn, C. Cross, and H. Jacmon, ‘Alleged financial Abuse of Those Under an Enduring Power of Attorney: An Exploratory Study’, The British Journal of Social Work 48 (2018), pp. 887–905; G. Stein and I. Fineberg, ‘Advance Care Planning in the USA and UK: A Comparative Analysis of Policy, Implementation and the social work role’, The British Journal of Social Work 43 (2013), pp. 233–248; Sarah Vilpert, C. Borrat-Besson, J. Maurer, and G. Domenico Borasio, ‘Awareness, approval and completion of advance directives in older adults in Switzerland’, Swiss Medical Weekly 149 (2018), p. w14642.
70.
R. Harding, ‘Legal Constructions of Dementia: Discourses of Autonomy at the Margins of Capacity’, Journal of Social Welfare and Family Law 34 (2012), pp. 425–442; Mäki-Petäjä-Leinonen, ‘Protecting a Person with Dementia Through Restrictions of Freedom?
71.
H. Nikumaa and A. Mäki-Petäjä-Leinonen, ‘Counselling of People with Dementia in Legal Matters – Social and Health Care Professionals’ Role’, European Journal of Social Work 23 (2020), pp. 685–698.
72.
One purpose of a continuing power of attorney is to promote the individual’s will and autonomy. See Government proposal HE 52/2006 vp, p. 9 and 15.
73.
The duty to inform patients concerns mainly their health, treatment options, and related care aspects. The information should include details on social and healthcare benefits and social security. Act on the Status and Rights of Patients (785/1992) Section 5 and Elder Care Act (980/2012) Section 12.
74.
Government proposal HE 146/1998 vp, p. 10.
75.
See e.g. S. Deniz, M. Akbolat, M. Çimen, and O. Ünal, ‘The Mediating Role of Shared Decision-Making in the Effect of the Patient–Physician Relationship on Compliance with Treatment’, Journal of Patient Experience 8 (2021), pp. 1–5.
76.
Guardianship Services Act (442/1999), Section 5.
77.
Ellison et al., ‘Access to Justice’; K. Ervasti and A. Mäki-Petäjä-Leinonen. ‘Ikääntyvien ihmisten perheoikeudelliset ongelmat ja oikeudensaantimahdollisuudet’, Defensor Legis 3.(2021), pp. 628–640.
78.
Nikumaa and Mäki-Petäjä-Leinonen, ‘Counselling of People with Dementia’, pp. 685–698.
80.
Näkki et al., ‘Diverging Perceptions’, p. e16334.
81.
Kumfor et al., ‘Criminal Risk Behaviours’, p. e12577.
82.
Näkki et al., ‘Evaluating the Need’, p. ebae005.
83.
N. Burns and S. Grove. The Practice of Nursing Research: Conduct, Critique and Utilization, 5th ed. (Philadelphia, PA: Elsevier/Saunders, 2005).