
Abstract
Nasogastric tube feeding may be imposed on adults with anorexia nervosa without their consent. Although it can preserve life, it can also cause significant and lasting distress, and it is widely accepted that the intervention should be employed only as a last resort. However, the concept of last resort remains insufficiently defined. Clinical guidance and case law in England and Wales use the term to guide decision-making, but the thresholds by which a particular action can be considered a last resort are varied and ambiguous. Informed by human rights principles, this article articulates the relevant thresholds for last resort decisions relevant to detention, restraint, and high-risk or speculative treatments, clarifying operative meanings by way of a typology.
Introduction
Last resort measures are invoked when available responses are limited and ethically or clinically contested. This article examines last resort treatment options for adults with anorexia nervosa (AN) in England and Wales. 1 Treatment for AN presents distinct legal sensitivities because, although individuals with the condition are often highly articulate and hold clear views about their treatment, the disorder can, nonetheless, impair autonomous decision-making while producing life-threatening medical deterioration in the absence of self-harm intent. Timely compulsory interventions, including invasive nasogastric tube feeding, not only can avert a risk of death, but also constitute substantial intrusions on autonomy and bodily integrity, and therefore require clear clinical justification, lawful authorisation, and stringent safeguards.
Compulsory treatment in this context is governed by two overlapping statutory frameworks: the Mental Health Act 1983 and the Mental Capacity Act 2005. Neither statute explicitly refers to last resort, yet the notion has become an important organising principle within both regimes to help gauge when interventions are justified. This article argues that distinct clinical and judicial decisions concerning compulsory treatment for AN require correspondingly distinct conceptualisations of last resort. To that end, we propose a typology to clarify these variations and to support the selection of the appropriate conceptualisation for the decision under consideration.
The significance of the project lies in the implications of the ambiguity of ‘last resort’ and the legal regime it supplements, for both patients and clinicians. Although, as we shall demonstrate, clinical guidelines rely on the principle of last resort, they do not always explain how to determine the threshold for invoking it in different last resort decisions. Setting the threshold too high may block actions that are justified to avert serious harm. Conversely, applying too low a threshold risks authorising interventions that are not genuinely a last resort, the dangers of which are exacerbated by the perceived threat of legal action, professional criticism, and an over-stretched mental health service. The implications for patient autonomy and liberty are significant.
Relatedly, there is evidence that last resort can function as a legitimation device. In the context of decisions about restraint, an ethnographic study by McKeown et al. examining staff cultures and attitudes in a range of UK mental health settings indicates that presenting restraint as a last resort can justify staff actions and provide reassurance to staff who experience moral discomfort. 2 The authors note that such legitimation is not value neutral; it can reinforce perceptions of patient ‘otherness’, reduce empathetic engagement and contribute to cultures of coercion and control. 3 The process of legitimation may also entrench the use of restraint, with the attendant risk of desensitising clinicians to the traumatic nature of such measures and thereby undermining the very idea of restraint as an exceptional intervention.
Last resort is a useful term to emphasise the importance of justifying actions as necessary and proportionate, but risks inappropriate and inconsistent thresholds if there is a paucity of guidance as to how it can be recognised in different contexts. It is essential that when clinicians seek to justify restraint and other pertinent decisions as a last resort, the application of the principle is coherent and aligned with its protective function. The aim of this article is to support that objective.
We begin by setting out the clinical and legal setting and outlining two reasons why the principle of last resort is relied upon in this context. The first arises from the uncertainties surrounding compulsory nasogastric treatment for AN, which create scope for clinical discretion. The second stems from the legal framework, which inevitably offers limited guidance on how that discretion should be exercised in this context. We then justify our claim that last resort functions in both clinical guidance and case law as a guiding principle. Finally, we examine the ambiguities this generates and provide a typology grounded in human rights principles to help address them.
Anorexia Nervosa
AN is a serious and sometimes fatal condition 4 that can be accompanied by severe mental and physical complications. These include bradycardia (slow heart rate), heart attack, suicide, and death from malnutrition. 5 Long-term treatments include psychological treatments (e.g. cognitive behavioural therapy), family-based interventions, and multidisciplinary outpatient care, 6 sometimes combined with psychiatric interventions including pharmacological treatment to address comorbidities. 7 These options are not feasible if the patient is at such a low weight that the AN is impacting on cognition and with it their ability to engage or benefit from them. 8 Instead, short-term and emergent treatments primarily focus on restoring and maintaining a patient’s weight.
Where physiological needs can only be met through nutritional intervention and the patient refuses to eat enough, nasogastric feeding may be clinically indicated. Where the patient withholds consent, as we shall examine below, there are circumstances in which the clinical team can decide to administer treatment under chemical or physical restraint. Once the immediate danger to life is passed, some patients will consent to managed oral or nasogastric food intake, while others will continue to resist. In instances where resistance persists, clinicians must consider whether and for how long nasogastric feeding under restraint can continue and how that might be clinically supported.
Nasogastric tube feeding under restraint can avert a serious risk of death 9 but it also carries short-term risks associated with underfeeding, misplacement or dislodgement of the tube, discomfort, and severe psychological distress. 10 Pharmacological treatment (medications) may be helpful, particularly if resistance is impacted by depression, psychosis, or autism. 11 Sedation can reduce the trauma associated with feeding under restraint 12 and reverse the effects of malnutrition. However, sedation is also resource-intensive and limits any learning experiences associated with coming to terms with refeeding. 13 People with AN are also at a risk of ‘refeeding syndrome’, a potentially fatal condition brought on by metabolic and electrolyte changes during the reversal of malnutrition, 14 and which requires close supervision.
The longer-term benefits of involuntary treatment are variable and poorly understood. 15 Outcomes are highly individualised, with some patients responding well to nasogastric feeding under restraint. There is research to suggest that although involuntary patients often have a worse baseline than voluntary patients on admission, their long-term prospects are broadly comparable. 16 Moreover, the longer-term perspective of patients who have been fed under restraint is not universally negative. Some patients retrospectively recognise its relevance and importance. 17 Physiologically, it will remove the immediate threat posed by malnutrition giving longer-term strategies a chance to take effect. Some will consent to further treatment once the impacts of malnutrition are mitigated through initial compulsory intervention. 18 However, Westmoreland and Mehler have estimated that involuntary treatment yields no sustained benefits for around 25% of patients. 19 There is a paucity of good quality clinical research on AN, 20 but efforts are being made to better understand its onset and progression with a recent focus on novel therapies such as psilocybin (‘magic mushrooms’), esketamine, 21 and neuromodulation (such as deep brain stimulation) 22 to aid in treatment delivery. 23
The limited understanding of AN, poor prognosis in persistent cases and traumatic nature of feeding under restraint makes it an exceptionally difficult treatment for clinicians to administer, for families to witness and for patients to undergo.
24
In the case of Northamptonshire Healthcare NHS Foundation Trust v AB, the patient described the experience of force-feeding, thus:
I have been held down by my legs with a tube thrust forcefully and forcibly up my nose. I have had food inserted through a syringe so quickly and violently that I was sick. . . . I have been restrained and force fed in front of other patients. I have been left covered in bruises and scratches. I have been thrown down on to a bed because I refused to sit in a chair. I have had my feet stamped on when being manhandled. . . . I have been helpless – and watched helplessly – as every aspect of my life, every aspect of my being, has been controlled by those with the power to do so. In turn, I have kicked and screamed until I’ve been hoarse.
25
We can conclude that it is often unclear when treatment should be initiated, what form it should take or for how long it should continue. It is within this context that the last resort principle is used to help make the relevant decisions.
Last resort in context
In this section, we examine how clinical guidance builds on law and clinical research by employing last resort as a guiding principle. This reflects both the complexity of the clinical presentation and the broad statutory framework within which last resort is applied. We also consider how judges draw on the principle when making declarations about patient mental capacity and best interests.
Adult patients of sound mind who have the requisite mental capacity are entitled to refuse medical intervention even if it will result in their death. 26 This includes the power to refuse food and water, including clinically administered nutrition and hydration. 27 For adults with AN, however, two overlapping legislative schemes may justify their compulsory treatment: the Mental Health Act 1983, as amended (MHA) 28 and the Mental Capacity Act 2005, as amended (MCA). 29 Though the concept of last resort is not mentioned explicitly in either statute, in this section, we explore how it is nonetheless utilised as a guiding principle in three pertinent decisions: detaining the patient, initiating treatment under restraint, and employing novel or high-risk strategies to stabilise the patient’s weight and prevent life-threatening complications. In subsequent sections, we argue that the conceptualisation of last resort differs across these contexts and develop a typology to assist in its application.
Detention
The National Institute for Health and Care Excellence (NICE) recommends inpatient treatment for patients with eating disorders whose physical health is ‘severely compromised’ and significantly declining.
30
NICE advises that
If a person’s physical health is at serious risk due to their eating disorder, they do not consent to treatment, and they can only be treated safely in an inpatient setting, follow the legal framework for compulsory treatment in the Mental Health Act 1983.
31
The MHA sets out a scheme for the detention of people who need urgent treatment for mental health disorders and are at risk of harming themselves or others. As we go to press, the Mental Health Act 2025 has recently received royal assent and amends the 1983 Act in several important respects, although the commencement dates for the provisions most relevant to this paper have not yet been announced. As a diagnosable mental health condition, AN satisfies the definition of ‘mental disorder’ for the purposes of section 1(2), which pertains to any disorder or disability of the mind. Section 63 of the MHA allows ‘medical treatment’ to be given by an approved clinician for mental disorder without consent. Medical treatment is defined in section 145(4) as treatment ‘the purpose of which is to alleviate, or prevent a worsening of, the disorder or one or more of its symptoms or manifestations’. Section 3 allows admission and detention for treatment, currently for up to 6 months, as required for the health and safety of the individual or the protection of others and provided ‘appropriate medical treatment is available’.
32
The Royal College of Psychiatrists guidance ‘Medical Emergencies in Eating Disorders’ (MEED) characterises the decision to detain a patient as a decision of last resort, albeit one which can often be anticipated and planned for:
Although a last resort, the decision to apply the Mental Health Act should be considered from the outset, e.g. when a patient refuses treatment in an emergency department setting.
33
There has been concern that detention in England and Wales is overused and that this failure to make it truly a last resort can breach patient human rights. 34 An independent review of the MHA in 2018 chaired by Sir Simon Wessely recommended both legislative and culture changes ‘to ensure that detention is truly a last resort’. 35 The Mental Health Act 2025 has duly set out amendments to the legal test for detention, which will (when this aspect comes into force) require that the detention averts a risk of serious harm to the patient or others. It will also reemphasise that treatment must be ‘necessary’ and could not be provided without detention. 36 We can see from this first context that there is broad agreement that detention ought to be a last resort, as well as an ambition to raise the threshold for determining when that standard is met.
Initiating restraint
While involuntary treatment under the MHA does not inevitably entail the use of restraint, when restraint is employed, the principle of last resort is once again a central consideration. The courts have confirmed that nasogastric feeding under restraint can fall within section 63 of the MHA. 37 However, the timing of the instigation and method of restraint can be difficult to judge. As Sarah Fuller and Ursula Philpot note, ‘Although research around involuntary NGT feeding exists, there is little published research into the practice of feeding under restraint, including incidence, type, duration, measure of restraint or outcome’. 38 Fundamentally, the dilemma about initiation is this: Move to restraint too soon and the treatment might not be considered sufficiently necessary or proportionate. On the other hand, failure to recognise that life is in danger can be, and has been shown to be, catastrophic. 39 Last resort is used in guidance to help clinicians navigate this dilemma and subsequent quandaries about method and duration.
The MHA is accompanied by a Code of Practice which sets out principles including choosing the least restrictive option.
40
A 2019 joint statement on nasogastric feeding interprets this to require that restraint is used only as a last resort:
Any use of restraint, including nasogastric feeding under restraint, should always be a measure of last resort when best efforts to support oral nutrition fail with subsequent deterioration in physical health.
41
As such, last resort can offer the necessary justification for a restrictive option being the least restrictive viable option.
Last resort is more explicitly relevant to the Mental Health Units (Use of Force) Act 2018, which sets out provisions for the appropriate use of ‘force’ defined as ‘use of physical, mechanical or chemical restraint of a patient, or the isolation of a patient (which includes seclusion and segregation)’. 42 The Ministerial Foreword states unequivocally, ‘The use of force must always be used proportionately, in accordance with the law, and only ever as a last resort’. 43 The Act requires mental health units to publish a policy on the use of force and convey to patients their rights, including ‘a clear statement that the use of force is only ever used proportionately and as a last resort and that it can never be used to cause pain, suffering, humiliation or as a punishment’. 44
The Royal College of Psychiatrists MEED guidance seeks to help health professionals decide when a situation becomes urgent. It states,
Physical restraint of patients should only be considered when absolutely essential and for the shortest period of time and should be carried out by nurses or other staff trained in control and restraint.
45
MEED reasserts the principle that ‘restraint is a last resort, and all other alternatives should be tried first’. 46 We can conclude that in relation to restraint, although the term ‘last resort’ does not appear in the text of the MHA, it is in practice relevant. Furthermore, restraint as a last resort invokes overlapping but also distinct considerations to those applied in decisions about detention.
Speculative treatments
The last resort principle is also relevant when the available treatment pathway becomes speculative. This may occur where clinicians consider a novel or experimental intervention for a patient with AN, or where they withdraw active compulsory treatment and place reliance on the hope of voluntary engagement. In both circumstances, the remaining speculative option is pursued, not because it offers a predictable therapeutic benefit, but because established interventions have been exhausted or have repeatedly failed to yield positive long-term results. The decision therefore reflects a last resort strategy in which the only remaining prospect for progress lies in a treatment course whose effectiveness cannot be assured.
Before outlining examples of such cases, it is necessary to consider the legal framework within which they are determined. So far, our focus has been on the MHA. As stated in section 145(4) of the MHA, (to be replaced with section 1A when it comes into force), treatment must have as its purpose ‘to alleviate, or prevent a worsening of, the disorder or one or more of its symptoms or manifestations’. Appropriate treatment can therefore include therapies designed to contain as well as to treat 47 and is not restricted to treatments likely to bring about remission or cure. 48 That said, recognition that a patient can be treated under section 63 does not automatically mean that they should be so treated. 49 Repeated use of the MHA to forcibly provide treatment for patients with long-standing severe eating disorders has, in several cases (some of which we discuss below), led to questions about whether this course of action should be repeated. 50
While the patient’s objection to treatment does not render it inappropriate, it is a relevant factor in the application of the ‘appropriate medical treatment’ test. 51 If the clinical team have collective concerns about the appropriateness of the treatment on these grounds, they may choose not to rely on the MHA. In such cases, clinicians can apply to the Court of Protection if the decision is finely balanced, 52 and must do so if the decision relates to provision of life-sustaining treatment where the issue is finely balanced, there is a difference of medical opinion, or a lack of agreement by those concerned with P’s welfare. 53 Where so, the Trust will generally propose a course of action or set out options for the court to consider. 54 In many such cases, the declarations sought concern findings that the person (P) lacks capacity and either a speculative treatment or de-escalation of compulsory treatment would be in P’s best interests. There is a growing body of case law illustrating how these principles are applied in specific AN cases. 55 There is evidence that the principle of last resort is sometimes used to help assess what options are justified in all the circumstances.
It must be stressed that the MCA and MHA are distinct legal frameworks, albeit there is a degree of overlap in their remit. The MHA scheme, broadly conceived, gives powers to responsible clinicians to make decisions about detention and restraint in the public interest. The MCA permits the use of restraint and restrictions only where P is found to lack capacity and they are in a person’s best interests and are both necessary and proportionate. Additional safeguards – known as the Deprivation of Liberty Safeguards 56 – are required when P is subject to continuous supervision and control and is not free to leave. 57 Under the MCA, P is presumed to have decision-specific mental capacity, 58 which can be rebutted only through the application of a two-stage test set out in sections 3 and 2 of the Act. P cannot be considered to lack capacity merely because their decision is unwise. 59 Under the MCA scheme – in contrast to section 63 of the MHA – a person who has mental capacity can make a determinative decision, including the decision to stop medical treatment such as nasogastric feeding, even if that will shorten their lives. 60
The section 3 functional test assesses P’s ability to understand and retain relevant information, their ability to use and weigh it in the decision-making process, and communicate their decision. In the context of AN, P’s ability to use and weigh information may be questioned. 61 If this ability is impaired and can be causally linked to their underlying AN (thus satisfying the section 2 diagnostic test), they lack capacity and may be treated in their best interests as stipulated in section 1(5). A range of factors is considered by the decision-maker, 62 but best interests is viewed from the patient’s point of view. 63 Section 6 of the 2005 Act and guidance in paragraphs 6.40 to 6.48 of the Mental Capacity Act Code of Practice 64 impose conditions on the use of restraint which the decision-maker must reasonably believe is necessary to prevent harm to P, and that it is proportionate to the likelihood of P suffering harm and the seriousness of that harm.
Turning now to illustrative examples of the application of the above principles – and acknowledging their fact-specific application in each case – in Pennine Care NHS FT v T,
65
‘Amy’ was being fed by nasogastric tube under restraint but had developed a technique to purge, rendering the treatment ineffective. The Trust proposed to admit Amy to intensive care for a 3- to 7-day period of sedation under general anaesthetic. The medical evidence suggested that
. . . the proposed benefit of admitting [Amy] to ICU for re-feeding is entirely speculative. It may cause significant harm or even hasten death; it may be wholly successful. Nobody knows, but experience tells me it will be somewhere on a spectrum between these two extremes. There is no evidence base that I or my colleagues can draw on when assessing risk/benefit analysis to make any predictions hence it should be tried as a last resort.
66
In St George’s University Hospitals Foundation Trust & Anor v LV, 20-year-old LV had been on a ward for 2 years and was currently being fed by nasogastric tube twice a day under restraint. Like Amy, LV had learned to purge during or after the treatment. As a result, she was close to dying. The Trust sought a declaration that LV lacked capacity and that it was in her best interests to try something experimental: to feed her under sedation in the intensive care unit. Granting the declaration, Morgan J began by noting that ‘The treatment is characterised as a treatment of last resort by all those medically qualified witnesses from whom I have heard’. 67
Barnet, Enfield and Haringey Mental Health NHS Trust v CC & Ors 68 provides another example of the consideration of novel or experimental measures when other options have proved ineffective. CC, aged 21, had treatment-resistant AN, autism spectrum disorder (ASD), and depressive disorder. One of the experts, Dr W, suggested use of Esketamine which CC strongly supported. But as a treatment for AN Hayden J noted that it had ‘very little evidence base’ 69 and that the hallucinations it would cause ‘might be distressing and cause agitation’. 70 Hayden J found that CC lacked capacity and preferred the view of a second expert, Dr Cahill, that the immediate focus in CC’s best interests should be on improving the symptoms of her ASD. If that did not work, and only then should Esketamine be considered: ‘Alarming though all this sounds, it is not difficult to see why [Esketamine] might be worth trialling if the alternative is speedy deterioration and death’. 71 The language of ‘last resort’ is not explicitly employed here, but it is clear that Hayden J considers that other less risky approaches currently exist and that this treatment might be resorted to if those approaches fail and the alternative is death.
The principle of last resort is also engaged where clinicians consider withdrawing compulsory feeding from patients with long-standing AN in the hope that this may prompt voluntary engagement with treatment. Where these cases have come before the Court of Protection, the courts have usually found that P lacks capacity
72
and in several cases have concluded that ongoing coercive treatment is not in their best interests.
73
In A Mental Health Trust v ER, for example, Lieven J said,
The parties agree, and I accept, that it is not in ER’s best interests for her to be forced to accept treatment for her anorexia which she does not wish to accept. In particular, she should not be forced to go into any inpatient hospital and treated against her wishes.
74
The hope underpinning many of these cases is that by lifting the pressure of compulsion and allowing P to take control of their destiny, they will choose to engage in treatment and to live. 75 The judges in these cases acknowledge that the prospect of success is often low. Guidance makes clear that until the point at which life-sustaining treatment is no longer in the patient’s best interests, it should be pursued. 76 But while there is strong emphasis on keeping patients alive, it is trite law that it is not always in the best interests of patients to prolong life: in Burke it was accepted that where a patient is close to death, the object of doctors might be to make dying comfortable. 77 In the relevant AN cases, the court turns to de-escalation as a last resort, and one that can in some circumstances later be revisited if it proves not to be in P’s best interests. 78
The variable conceptualisation of last resort
Requiring nasogastric feeding to be used only as a last resort can reflect several distinct conceptualisations, each involving a different threshold for intervention. For example, one conceptualisation might treat compulsory nasogastric feeding as justified only in an immediate emergency, where there is an acute and imminent risk to life and no other measure could avert death. Another understanding extends beyond the immediate emergency and permits intervention when it is the least restrictive option with a realistic prospect of preventing a serious, short- or longer-term threat to life, once other options have been ruled out as inappropriate. A third approach might view last resort through the lens of restrictiveness, allowing compulsory feeding only when all less restrictive relevant treatments have been attempted and it is reasonable not to revisit them at the current stage of treatment. A fourth and broader understanding might focus on overall benefit, permitting compulsory feeding when alternative options are not reasonable in the circumstances, even if they are not strictly ruled out or previously attempted. The three contexts – detention, initiating restraint, and speculative treatment – described in the preceding section reflects distinct conceptualisations of last resort as a guiding principle. In this section, we consider how human rights principles give substantive content to the otherwise ill-defined concept.
Detention
Detention is considered a last resort because justifications for involuntary hospitalisation under the MHA are designed to ensure that the person is not detained unless outpatient care, community support, or adjustments to existing treatment plans will suffice to keep them and the public safe. This in turn flows from a requirement that detention is a proportionate response to interference with the person’s rights to liberty and autonomy.
There is an extensive jurisprudence from the European Court of Human Rights (the Strasbourg court) on the upper and lower limits of the thresholds of proportionality under Articles 5 and 8 of the European Convention on Human Rights (ECHR), which was relevant to the framing of the MHA and remains relevant to its interpretation. Article 5 protects the right to liberty except where prescribed by law including ‘the lawful detention of persons for the prevention of the spreading of infectious diseases, of persons of unsound mind, alcoholics or drug addicts or vagrants’. 79 The Strasbourg court has used the principle of last resort to assess the lawfulness of detention by reference to the availability of alternative measures. 80 Where a patient is deprived of their liberty on the basis that they are of ‘unsound mind’, the Strasbourg court requires evidence of mental disorder, that it warrants compulsory confinement, and that it persists throughout the period of detention. 81 In Stanev v. Bulgaria, for example, the Court held that placing Mr Stanev, who had schizophrenia, in a remote social care home was not, as the government argued, ‘an appropriate response to a social and medical emergency’ but a deprivation of liberty that breached Article 5. 82 Mr Stanev had not consented and the decision was not justified by the severity of his disorder. In that case there was also breach of Article 3, which protects in absolute terms the right to freedom from inhuman and degrading treatment, because of the suffering and humiliation he suffered because of the poor living conditions in the home and the lack of effective remedy in Bulgarian law. 83
Last resort is less directly relevant to Article 8(1), which protects the right to respect for private and family life subject to qualifications in Article 8(2), including where interference is necessary in the interests of the protection of health and in the interests of public safety. Treatment without consent will interfere with Article 8 unless it is a proportionate measure that is justified to protect the patient or others. 84 If detention is a last resort, it may be considered necessary and proportionate, but it does not follow that detention must be a last resort to be Article 8-compliant.
These obligations must be balanced with the duty incumbent on the state to safeguard the lives of those within its jurisdiction. Article 2 imposes a positive obligation on states to protect the right to life. This extends both to providing a system of protection and an operational duty to take appropriate measures to protect the person where their life is at risk. It has been applied in the context of healthcare and to protect persons from suicide risk in involuntary hospitalisation. 85
In the context of mental disability, ECHR rights are supplemented by the United Nations Convention on the Rights of Persons with Disabilities (CRPD) which was passed by the General Assembly in 2006, entered into force in 2008 and was ratified by the United Kingdom in 2009. Though it is not legally binding on the UK courts, it is relevant in the interpretation of the ECHR. The CRPD protects the right to legal capacity on an equal basis with others under Article 12; liberty and security under Article 14; prohibition of torture and cruel, inhuman, or degrading treatment or punishment under Article 15, protection against violence, exploitation, and abuse under Article 16; the right to physical and mental integrity under Article 17; and the right to health care on an equal basis with others and based on informed consent under Article 25. The Committee on the Rights of Persons with Disabilities set out in a General Comment the importance of the right of persons with disabilities to enjoy legal capacity on an equal basis with others.
86
It notes that many states have yet to shift from substituted decision-making to supported decision-making in accordance with Article 12 of the CRPD.
87
The Strasbourg court and, as will be clear from this article, the English and Welsh jurisdiction have not fully aligned with the CRPD emphasis on supported decision-making to promote and follow P’s will and preferences, but there are efforts to improve alignment. As noted by Lady Hale P v Cheshire West,
[I]t is axiomatic that people with disabilities, both mental and physical, have the same human rights as the rest of the human race. It may be that those rights have sometimes to be limited or restricted because of their disabilities, but the starting point should be the same as that for everyone else. This flows inexorably from the universal character of human rights, founded on the inherent dignity of all human beings, and is confirmed in the United Nations Convention on the Rights of Persons with Disabilities.
88
When considering the correlation between human rights considerations and the treatment of eating disorders, it is important to note that the number of patients with eating disorders has risen exponentially in recent years 89 and services are under intense systemic pressures. 90 As discussed above, the Mental Health Act 2025 seeks to raise the threshold for compulsory detention by requiring evidence of a risk of serious harm to the health and safety of the patient or others.
In sum, a human rights–compliant approach to detention requires the state to ensure the availability of meaningful alternatives so that detention operates as a measure of last resort. At a clinical level, last resort signifies that clinicians must follow procedures prescribed by law, consider less restrictive options in a structured manner, and reach a conclusion that detention is a necessary and proportionate response to the severity of the patient’s condition. As we have seen, there is ambition for a higher threshold for detention as a last resort which will depend on the relevant sections of the amended 1983 Act being implemented, as well as systemic improvements, and changes to practice.
Initiating restraint
Where a person has been detained, the decision to restrain them invokes a new and separate assessment of proportionality and necessity. The Council of Europe has said that restraint should only be used ‘as a measure of last resort (ultimo ratio) to prevent imminent harm to themselves or others and restraint should always be used for the shortest possible time’. 91 In Spivak v Ukraine, the court confirmed that compulsory treatment requires rigorous oversight to prevent abuse and ensure that any interference with autonomy is proportionate, justified, and both appropriate and necessary. 92 In this case, the absence of adequate safeguards governing the use of chemical restraint 93 meant that the domestic framework failed to meet the state’s positive obligations under Article 3. 94
There will be no breach of Article 3 in cases of medical necessity, provided the necessity has ‘been convincingly shown to exist’. 95 It was violated in VI v Moldova 96 when a 15-year-old orphan with an intellectual disability for whom there was no appropriate care option was placed in a psychiatric hospital without therapeutic purpose and given psychiatric treatment as a chemical restraint. In Aggerholm v Denmark, 97 a patient with paranoid schizophrenia was strapped to a restraint bed for 23 hours in a psychiatric hospital. The Danish court considered the restraint to be a matter of last resort to prevent harm to others. Aggerholm argued that this treatment was neither necessary nor in compliance with human dignity. The Strasbourg court found that the procedural safeguards were insufficient. The duration of restraint was not justified, resulting in a violation of Article 3. 98
In light of the patient experience of compulsory nasogastric feeding under restraint, as considered above, such intervention must be demonstrated to constitute a medical necessity, comply with the procedural safeguards set out in the MHA, and involve no greater degree of force than is required. 99 But what is meant by ‘medical necessity’? Defining it will help articulate whether the action can be considered a last resort. Clearly necessity could be established if the patient is likely to die without the proposed intervention. After all, failure to initiate feeding when a patient will otherwise die, and treatment is appropriate, has potential to breach the positive obligation set out in the Article 2 right to life. However, the domestic courts have held that this duty is relatively easily satisfied 100 and does not require the state to assume responsibility for every aspect of a patient’s physical health. 101 Necessity may nonetheless be established even if the patient is not likely to die, if, for example, they would otherwise come to very serious harm. 102
Speculative treatment
The conception of last resort used to guide decisions about what we have termed ‘speculative treatment’ for AN is substantively and procedurally different to the conceptions about MHA detention and initiating restraint. Procedurally, it is more likely to invoke the MCA rather than the MHA regime, though there is overlapping relevance and consequently a grey area between the two. Substantively, the justification in these circumstances must remain holistic and grounded in the individual’s situation, while recognising the state’s positive obligation to protect life under Article 2. A speculative or untested intervention that exposes a patient to disproportionate distress or risk may contravene Article 3 yet persisting with coercive treatment when prospects of benefit are minimal may also raise Article 3 concerns. The absolute nature of Article 3 requires the court to ensure that the overall package of care does not reach the threshold of inhuman or degrading treatment, but this assessment must be read alongside the duty to take reasonable steps to preserve life.
In relation to Article 5, if a novel or speculative treatment necessitates additional constraint or prolonged detention, the state must demonstrate clear medical evidence of necessity, proportionality, and the presence of adequate procedural safeguards. Article 5 is equally engaged by proposals to reduce coercion or to shift towards a voluntary framework, because a less restrictive programme may diminish or remove any deprivation of liberty. In both directions, the patient’s assent, where they lack capacity, is an important factor and may reinforce the proportionality of adopting a less restrictive approach within the overall human rights balance.
A typology
We have shown that clinical guidance relies on the principle of last resort to guide action across a range of different decisions pertinent to the nasogastric feeding of adults with AN, and that the different decisions invoke variable thresholds and different human rights considerations. There is a risk, however, that the ambiguity of the concept relied on could undermine the requirements of necessity and proportionality in decision-making. In this section, we set out what last resort means in the different contexts of detention, restraint, and speculative treatment, proposing a typology intended to guide decision-making.
In articulating the different thresholds, it is important not to lose sight of the conceptual overlap between the three contexts. The classification of a treatment as a last resort should not be understood merely as an inherent quality of the treatment itself, but as a contextual judgement grounded in the specific circumstances of the individual case. 103 Our aim is not categorically to endorse or reject any usage, but rather to guide discussion and highlight the importance of clearly articulating the intended meaning in each instance, since different interpretations may yield alternative outcomes.
As discussed above, last resort can be conceptualised in several ways: as a narrow emergency standard confined to imminent threats to life; a broader life-risk standard tied to the least restrictive option capable of averting serious harm; a restrictiveness-based standard requiring prior attempts at less intrusive measures; and an evaluative standard focused on overall benefit where alternative options are considered unreasonable in the circumstances. While we acknowledge the relevance of each interpretation and their overlap, we propose that certain conceptualisations align more appropriately with the three specific decisions under consideration: detention, restraint, and speculative treatment.
Currently, a minimal threshold for last resort in the context of detention is that other options are not reasonable in the circumstances. This approach requires evidence that less restrictive options are not practical. The evidential focus will not inevitably rest solely on the patient. In practice, a last resort decision may be justified by wider considerations, including the impact of the patient’s refusal of food on other patients, pressures arising from limited bed availability, or even the efficient allocation of staff time. 104
With regard to restraint, the focus on ‘last resort’ supplements the focus on the least restrictive option by emphasising the need to ensure that there is no alternative that would reduce the risk to an acceptable level, and also that the risk itself is sufficiently serious to justify the restraint. But equally, it is also important that the threshold for restraint as a last resort is not raised too high. Last resort could be interpreted to apply only as a narrow emergency standard confined to imminent threats to life, but the courts have recognised in non-AN contexts that restraint as a last resort extends beyond life-saving measures to also ‘prevent a serious deterioration in . . . mental health’. 105 This reasoning is similarly applicable to situations when it would be relevant to move to nasogastric feeding of a patient with AN to prevent a serious deterioration in physical health that would, in turn, physiologically impact upon P’s mental health. Emergency-only criterion would also fail to accommodate clinical and legal realities in situations when a planned, discussed, and timely transition to restraint is warranted. 106 Nor should the threshold for last resort operate so rigidly as to preclude continued treatment once the immediate danger to life has passed, if the physiological impacts of malnutrition have not yet been overcome. Qualitative studies indicate that weight restoration can lead to a change of perspective of the patient and to improved outcomes. 107 The threshold for restraint as a last resort must not be set so high that it causes a revolving cycle of critical malnutrition and temporary stabilisation through nutritional intervention. The emphasis in this conceptualisation is on necessity and proportionality: nasogastric feeding must be shown to be optimal for this patient, at this time, because other less restrictive measures are insufficiently likely to bring about short- or longer-term rehabilitation.
Finally, in relation to speculative treatment of patients who are found to lack mental capacity, decisions will generally be made by the Court of Protection because they are, by their nature, finely balanced and most such decisions will relate to provision of life-sustaining treatment. In these cases, speculative treatment as a last resort generally arises when standard interventions have been exhausted or are assessed as unlikely to be effective in the medium to long term. The focus will be on whether the proposed option offers a prospect of averting a life-threatening risk, but a limited prospect will not preclude justification where the evidence demonstrates that the last resort option is the only viable means of sustaining life. The proportionality assessment requires that other, less speculative treatments should have been tried or ruled out before a novel experimental approach is taken. 108 Treatment under this conceptualisation requires justification by reference to the patient, driven by a best interests approach that takes into consideration the patient’s will and preferences.
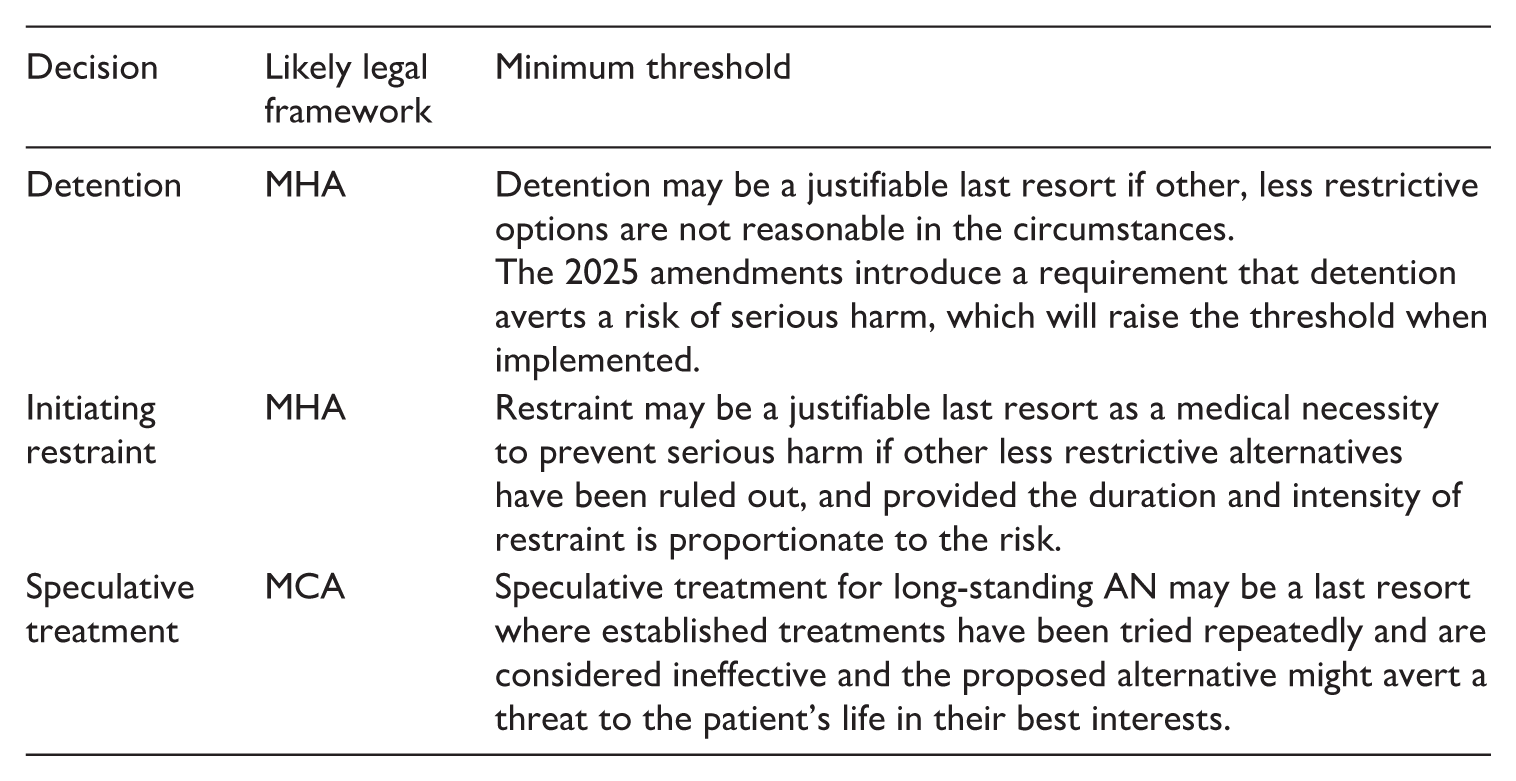
Bringing together our discussion of the different contexts, legal frameworks, measures, and conceptual models, we would suggest that a starting point for discussion of last resort in the contexts of detention, restraint, and speculative treatment should incorporate the following minimal threshold for last resort:
We have argued that reference to last resort across different guidelines, and with limited explanations of meaning, could lead to the blurring of the different conceptualisations we have articulated. Determining the extent of the problem is difficult given scant empirical research on the incidence and use of nasogastric feeding. We have articulated risks of imposing too high a threshold. If, for example, the threshold that has been applied by the Court of Protection to determine whether speculative treatment meets the standard of last resort were also applied to decisions to initiate restraint, it could expose patients to unjustified harm. Evidence suggests that thresholds for intervention have, at times, been set excessively high, leading to adverse outcomes. 109
However, the converse also applies. If the threshold and considerations relevant to detention, for example, are applied to restraint, then this could lead to unjustified restrictions on the patient’s liberty. This too is a real threat. According to a recent audit by Sarah Fuller and others, 622 people received the treatment in 2020, of which 136 were adults in specialist eating disorder units.
110
Some of these patients had only a single treatment, but the mean duration was 29.1 weeks and 17 patients received it for more than a year. The study includes children where the emphasis on enforcing life-sustaining treatment is particularly strong. Nevertheless, the audit raises a concern that in some cases, the threshold for intervention is set too low. Fuller and others note this possibility in a subsequent paper:
It is important to note that some clinicians will state that ‘if we stop feeding and they don’t eat, the eating disorder will get stronger’ and that, because of this view, NGT feeding under restraint may be maintained appropriately. NGT feeding under restraint should only be continued if it is clinically indicated and not because of the clinician’s anxieties around the patient not having adequate nutrition.
111
We suggest that our guidance on what last resort requires in different contexts can help prevent reliance on interpretations that inappropriately raise or lower the threshold for compulsory intervention.
Conclusion
The administration of compulsory nasogastric feeding under restraint in the treatment of AN involves a complex interplay of clinical necessity, legal authority, and ethical justification. Although such intervention can prevent death and, in some cases, support recovery comparable to that achieved through voluntary treatment, it remains highly distressing for patients to experience and challenging for clinicians and families.
Legal authorisation may arise under either the MCA or MHA, and although neither statute expressly incorporates a last resort requirement, the concept has become embedded in clinical reasoning and case law as a guiding principle. Judges applying the MCA in Court of Protection cases have invoked last resort when assessing the justification for escalated or novel treatments, while decisions under the MHA rely on related principles including least restriction and necessity. These legal standards operate within a broader human rights framework, which requires any coercive measure to be proportionate, necessary, and attentive to patient autonomy interests.
Reliance on last resort reflects both the complex and contested nature of compulsory treatment for AN and the gaps inevitably left by the statutory schemes, which statutory Codes of Practice reduce but do not eliminate. Although this discussion has centred on England and Wales, the legal frameworks governing compulsory mental health interventions and decisions for people who lack mental capacity vary across the devolved nations, and the character of these gaps therefore differ. In Scotland, for example, the Mental Health (Care and Treatment) (Scotland) Act 2003 112 and the Adults with Incapacity (Scotland) Act 2000 113 embed more explicit guiding principles, including the requirements for benefit, respect for the individual’s wishes, and the least restrictive alternative, which might offer clearer direction for the operation of last resort as a threshold or diminish the need to invoke it.
In England and Wales, and Scotland alike, 114 the last resort principle provides a supplement to statute and Codes, emphasising that a high threshold applies. We have argued that the threshold is not single and uniform, but a set of distinct conceptualisations that apply differently to detention, restraint, and speculative treatment. Each reflects different assumptions about risk, urgency, and proportionality. Recognising these distinctions is essential to reducing ambiguity, promoting consistency, and ensuring that coercive interventions, particularly nasogastric feeding under restraint, rest on clear, proportionate, and legally defensible reasoning.
Footnotes
Acknowledgements
We are most grateful to the anonymous reviewers and to Jacinta Tan for comments on a previous draft.
Authors’ note
Emma Cave is Rachel Jenkins’ PhD supervisor.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
No ethics approval was required.
1.
Our focus is on decisions surrounding compulsory nasogastric feeding. For a discussion of the broader decisions around end-of-life issues in the context of eating disorders, see S. Kendall Jamieson, J. O. Tan, K. Piekunka, S. Calvert, and S. Anderson, ‘Navigating the Ethical Complexities of Severe and Enduring (Longstanding) Eating Disorders: Tools for Critically Reflective Practice and Collaborative Decision-Making’, Journal of Eating Disorders 12 (2024), p. 134.
2.
M. McKeown, G. Thomson, F. Scholes, F. Jones, S. Downe, O. Price, J. Baker, P. Greenwood, R. Whittington, and J. Duxbury, ‘Restraint Minimisation in Mental Health Care: Legitimate or Illegitimate Force? An Ethnographic Study’, Sociology of Health and Illness 42(3) (2020), p. 449.
3.
M. McKeown, A. Scholes, F. Jones, and W. Aindow, ‘Coercive Practices in Mental Health Services: Stories of Recalcitrance, Resistance and Legitimation’ in A. Daley, L. Costa, and P. Beresford, eds., Madness, Violence and Power (Toronto, ON, Canada: University of Toronto Press, 2019), pp. 263–285.
4.
See NHS, ‘Anorexia’ (NHS, 18 January 2024) available at ![]() (accessed 25 April 2025); J. Arcelus, A. J. Mitchell, J. Wales, and S. Nielsen, ‘Mortality Rates in Patients with Anorexia Nervosa and Other Eating Disorders. A Meta-Analysis of 36 Studies’, Archives of General Psychiatry 68(7) (2011), p. 724; N. Auger, B. J. Potter, U. V. Ukah, N. Low, M. Israël, H. Steiger, J. Healy-Profitós, and G. Paradis, ‘Anorexia Nervosa and the Long-Term Risk of Mortality in Women’, World Psychiatry 20(3) (2021), p. 448.
(accessed 25 April 2025); J. Arcelus, A. J. Mitchell, J. Wales, and S. Nielsen, ‘Mortality Rates in Patients with Anorexia Nervosa and Other Eating Disorders. A Meta-Analysis of 36 Studies’, Archives of General Psychiatry 68(7) (2011), p. 724; N. Auger, B. J. Potter, U. V. Ukah, N. Low, M. Israël, H. Steiger, J. Healy-Profitós, and G. Paradis, ‘Anorexia Nervosa and the Long-Term Risk of Mortality in Women’, World Psychiatry 20(3) (2021), p. 448.
5.
A. Vannacci, R. Baronti, E. Masini, C. Ravaldi, and V. Ricca, ‘Anorexia Nervosa and the Risk of Sudden Death’, The American Journal of Medicine 112(4) (2002), p. 327.
6.
NICE, Eating Disorders: Recognition and Treatment (NICE guideline [NG69], 23 May 2017).
7.
NICE, op. cit.; H. P. Chiu, M. W. Huang, S. Y. Tsai, and C.-Y. Hsu, ‘A Retrospective Study of Pharmacological Treatment in Anorexia Nervosa: 6-Month and 12-Month Follow-up’, BMC Psychiatry 23(1) (2023), p. 126 indicated that pharmacological treatment (especially antidepressants) is more efficacious than no drug treatment.
8.
S. Zipfel, K. E. Giel, C. M. Bulik, P. Hay, and U. Schmidt, ‘Anorexia Nervosa: Aetiology, Assessment, and Treatment’, Lancet Psychiatry 2(12) (2015), p. 1099.
9.
R. Ramsay, A. Ward, J. Treasure, and G. F. Russell, ‘Compulsory Treatment in Anorexia Nervosa. Short-Term Benefits and Long-Term Mortality’, British Journal of Psychiatry 175 (1999), p. 147.
10.
NICE, NG69, 1.11.10. And see S. J. Fuller, J. O. Tan, and D. Nicholls, ‘Nasogastric Tube Feeding under Restraint: Understanding the Impact and Improving Care’, British Journal of Psychiatry Bulletin 48(3) (2024), p. 163.
11.
See S. Marucci, ‘Anorexia Nervosa and Comorbid Psychopathology’, Endocrine, Metabolic & Immune Disorders-Drug Targets 18(4) (2018), p. 316; J. Brede, C. Babb, C. Jones, M. Elliott, C. Zanker, K. Tchanturia, L. Serpell, J. Fox, and W. Mandy, ‘“For Me, the Anorexia is Just a Symptom, and the Cause is the Autism”: Investigating Restrictive Eating Disorders in Autistic Women’, Journal of Autism and Developmental Disorders 50 (2020), p. 4280.
12.
S. J. Fuller, S. Chapman, E. Cave, J. Druce-Perkins, P. Daniels, and J. Tan, ‘Nasogastric Tube Feeding Under Physical Restraint on Paediatric Wards: Ethical, Legal and Practical Considerations Regarding This Lifesaving Intervention’, British Journal of Psychiatry Bulletin 47(2) (2023), p. 105.
13.
P. Falcoski, U. Philpot, J. O. Tan, L. D. Hudson, and S. J. Fuller, ‘Nasogastric Tube Feeding in Line with New Dietetic Guidelines for the Treatment of Anorexia Nervosa in a Specialist Children and Adolescent Inpatient Unit: A Case Series’, Journal of Human Nutrition and Dietetics 34(1) (2020), p. 33.
14.
I. Cioffi, V. Ponzo, M. Pelligrini, A. Evangelista, F. Bioletto, G. Ciccone, F. Pasanisi, E. Ghigo, and S. Bo, ‘The Incidence of the Refeeding Syndrome. A Systematic Review and Meta-Analyses of Literature’, Clinical Nutrition 40(6) (2021), p. 3688.
15.
I. F. Elzakkers, U. N. Danner, and H. W. Hoek, ‘Mental Capacity to Consent to Treatment in Anorexia Nervosa: Explorative Study’, British Journal of Psychiatry Open 9(2) (2016), p. 147.
16.
A. Ayton, C. Keen, and B. Lask, ‘Pros and Cons of Using the Mental Health Act for Severe Eating Disorders in Adolescents’, European Eating Disorders Review 17(1) (2009), p. 14; A. R. Atti, T. Mastellari, S. Valente, M. Speciani, F. Panariello, and D. De Ronchi, ‘Compulsory Treatments in Eating Disorders: A Systematic Review and Meta-Analysis. Eating and Weight Disorders’, Eating and Weight Disorders Journal, 26(4) (2020), p. 1037.
17.
J. O. Tan, T. Hope, A. Stewart, and R. Fitzpatrick, ‘Control and Compulsory Treatment in Anorexia Nervosa: The Views of Patients and Parents’, International Journal of Law and Psychiatry 26(6) (2003), p. 627.
18.
T. L. Watson, W. A. Bowers, and A. E. Andersen, ‘Involuntary Treatment of Eating Disorders’, American Journal of Psychiatry 157 (2000), p. 1806.
19.
P. Westmoreland and P. S. Mehler, ‘Caring for Patients with Severe and Enduring Eating Disorders (SEED): Certification, Harm Reduction, Palliative Care, and the Question of Futility’, Journal of Psychiatric Practice 22(4) (2016), p. 313. And see R. Mairs and D. Nicholls, ‘Assessment and Treatment of Eating Disorders in Children and Adolescents’, Archives of Disease in Childhood, 101 (2016), p. 1168, suggesting that only 50% of people with eating disorders will make a full recovery.
20.
F. Solmi, H. Bould, E. C. Lloyd, and G. Lewis, ‘The Shrouded Visibility of Eating Disorders Research’, Lancet Psychiatry 8(2) (2021), p. 91.
21.
S. Knatz Peck, S. Shao, T. Gruen, K. Yang, A. Babakanian, J. Trim, D. M. Finn, and W. H. Kaye, ‘Psilocybin Therapy for Females with Anorexia Nervosa: A Phase 1, Open-Label Feasibility Study’, Nature Medicine 29(8) (2023), p. 1947; A. Ragnhildstveit, M. Slayton, L. K. Jackson, M. Brendle, S. Ahuja, W. Holle, C. Moore, K. Sollars, P. Seli, and R. Robison, ‘Ketamine as a Novel Psychopharmacotherapy for Eating Disorders: Evidence and Future Directions’, Brain Sciences 12 (2022), p. 382.
22.
L. Gallop, M. Flynn, I. C. Campbell, and U. Schmidt, ‘Neuromodulation and Eating Disorders’, Current Psychiatry Reports, 24(1) (2022), p. 61.
23.
See, for example, St George’s University Hospital NHSFT & Anor v. LV [2025] EWCOP 9 (T3), discussed below, which considered that feeding under sedation in the intensive care unit was in LV’s best interests.
24.
See J. O. Tan, ‘The Anorexia Talking?’, The Lancet 362(9391) (2003), p. 1246.
25.
Northamptonshire Healthcare NHS Foundation Trust v. AB [2020] EWCOP 40, [48].
26.
St George’s Healthcare NHS Trust v. S [1999] (Fam) 26.
27.
An NHS Trust v. A [2013] EWHC 2442 (COP), [30] (Baker J); R (Nicklinson and Another) v. Ministry of Justice [2014] UKSC 38, [255] (Lord Sumption).
28.
At the time of writing the government had committed to modernising the MHA by increasing the risk threshold for detention and giving more weight to the patient’s view. At proof stage, theMental Health Act 2025 amending the 1983 Act has received royal assent (in December 2025) and phased implementation has begun.
29.
Note that that additional legal and ethical considerations apply in relation to minors which we do not consider in this article.
30.
NICE, NG69, 1.11.
31.
NICE, op. cit., 1.12.1.
32.
Mental Health Act 1983, s.3(2). The Mental Health Act 2007 amended the MHA inserting the ‘appropriate treatment test’ in place of the previous ‘treatability test’ that applied to patients under long-term detention. The Mental Health Act 2025 amended the MHA inserting a new section 1A (not yet in force) defining ‘appropriate medical treatment’ as treatment with ‘a reasonable prospect of alleviating, or preventing the worsening of, the disorder or one or more of its symptoms or manifestations’ and which ‘is appropriate in the person’s case’.
33.
Royal College of Psychiatrists, Medical Emergencies in Eating Disorders (MEED), CR233, (May 2022, updated October 2023), 120 (our italics).
34.
See, for example, M. Bonnet and N. Moran, ‘Why Do Approved Mental Health Professionals Think Detentions under the Mental Health Act Are Rising and What Do They Think Should Be Done about It?’, The British Journal of Social Work 50(2) (2020), p. 616.
35.
DHSC, Modernising the Mental Health Act: Increasing Choice, Reducing Compulsion: Final Report of the Independent Review of the Mental Health Act 1983 (December 2018), p. 13 (our italics). See also p. 23 and p. 33.
36.
See MHA (as amended but not yet in force), s. 3(2)(b)-(d).
37.
B v. Croydon Health Authority [1995] 1 All ER 683; Pennine Care NHS Foundation Trust v. Mrs T & Ors [2022] EWHC 515 (Fam) [4] (Morgan J).
38.
S. J. Fuller, U. Philpot and Working Group, ‘The Development of Consensus-Based Guidelines for Dietetic Practice in Nasogastric Tube Feeding Under Restraint for Patients with Anorexia Nervosa Using a Modified Delphi Process’, Journal of Human Nutrition and Dietetics 33 (2020), p. 287.
39.
40.
DHSC, Mental Health Act 1983 Code of Practice (2015, updated 2017), para 1.
41.
42.
Mental Health Units (Use of Force) Act 2018, s.1(6).
43.
DHSC, Mental Health Units (Use of Force) Act 2018: statutory guidance for NHS organisations in England, and police forces in England and Wales (7 December 2021), 1 (our italics), and see section 5.k.
44.
Op. cit., part 4 (our italics).
45.
Royal College of Psychiatrists, MEED, p. 135; See also DHSC, MHA Code of Practice, para 1.4.
46.
Royal College of Psychiatrists, op. cit., p. 86 (our italics).
47.
R (on the application of Munjaz v. Mersey Care NHS Trust) [2005] UKHL 58.
48.
See DHSC, MHA Code of Practice, para 23.6.
49.
See JK v. Local Health Board [2019] EWHC 67 (Fam), [74] (Lieven J).
50.
F. Marcolini, A. Ravaglia, A. V. Tempia, G. Bosco, G. Marconi, D. Ronchi, and A. R. Atti, ‘Severe Enduring Anorexia Nervosa (SE-AN) Treatment Options and their Effectiveness: A Review of Literature’, Journal of Eating Disorders 12(1) (2024), p. 48.
51.
DHSC, MHA Code of Practice, para 23.19.
52.
Practice Guidance (Court of Protection: Serious Medical Treatment) [2020] EWCOP 2.
53.
An NHS Trust v Y [2018] UKSC 46.
54.
The Court of Protection is unwilling to decide purely hypothetical questions: Re E (Medical Treatment: Anorexia) [2012] EWHC 1639 (COP), [41] (Peter Jackson J).
55.
See E. Cave and J. O. Tan, ‘Severe and Enduring Anorexia Nervosa in the Court of Protection in England and Wales’, International Journal of Mental Health and Capacity Law, 23 (2017), p. 4; E. Cave and J. O. Tan, ‘Evolving Judicial Approaches to Longstanding Anorexia Nervosa’, Clinical Ethics 20 (2025), pp. 222–232, DOI: 10.1177/14777509251391973; J. O. Tan, E. Cave, A. Ruck Keene, N. Kern, A. Bradshaw, J. Griffiths, R. Jenkins and P. Robinson, ‘Legal Decisions on Longstanding Severe Eating Disorders’, The British Journal of Psychiatry. Epub ahead of print 4 December 2025. DOI: 10.1192/bjp.2025.10490.
56.
Mental Capacity Act 2005, ss. 4A and 4B and Schedules A1 and 1A. The scheme is supplemented by the Ministry of Justice, Deprivation of Liberty Safeguards Code of Practice (2008). The Mental Capacity (Amendment) Act 2019 introduced a replacement scheme called the Liberty Protection Safeguards which has not yet been implemented.
57.
P v Cheshire West & Cheshire Council [2014] UKSC 14.
58.
Mental Capacity Act 2005, s.1(2) and s.2(1).
59.
Mental Capacity Act 2005, s.1(4); Heart of England NHS Foundation Trust v. JB [2014] EWHC 342 (COP), Peter Jackson J at [7].
60.
St George’s Healthcare NHS Trust v. S [1999] (Fam) 26.
61.
See T. Hope, J. O. Tan, A. Stewart, and J. McMillan, ‘Agency, Ambivalence and Authenticity: The Many Ways in which Anorexia Nervosa can affect Autonomy’, International Journal of Law in Context 9(1) (2013), p. 20.
62.
Mental Capacity Act 2005, s.4.
63.
Aintree University Hospitals NHS Foundation Trust v. James [2013] UKSC 67, [45] (Lady Hale).
64.
Office of the Public Guardian, Mental Capacity Act Code of Practice (2007, updated 2013 and 2020).
65.
Pennine Care NHS Foundation Trust v. Mrs T [2022] EWHC 515 (Fam). Note that this case was decided under the High Court’s inherent jurisdiction because Amy was 17 years old. We are not focusing on children in this article, but the principle around consideration of a last resort treatment is relevant to our discussion.
66.
Pennine Care NHS Foundation Trust v. Mrs T [2022] EWHC 515 (Fam), [20].
67.
[2025] EWCOP 9 (T3) [1] (our italics).
68.
[2024] EWCOP 65 (T3).
69.
Op. cit., [38].
70.
Op. cit., [43].
71.
Op. cit., [44].
72.
Though consider Lancashire and South Cumbria NHS Foundation Trust v. Q [2022] EWCOP 6 where Hayden J found that a 50-year-old woman with bulimia nervosa had capacity to litigate and make decisions about medical treatment. For discussion of the application of the test for capacity, see Cave and Tan ‘Evolving Judicial Approaches’; Elzakkers et al., ‘Explorative Study’.
73.
For a list of relevant cases, see Cave and Tan, ‘Evolving Judicial Approaches’, Table 1. Cases where ongoing treatment was in P’s best interests include Re E (Medical Treatment: Anorexia) [2012] EWHC 1639 (COP); Patricia’s Father and Ors v Patricia and Ors [2025] EWCOP 30 (T3).
74.
A Mental Health Trust v. ER & Anor [2021] EWCOP 32, [35].
75.
See, for example, Re RD (Anorexia: Compulsory Treatment) [2021] EWCOP 35, [39] (Moor J); Gloucestershire Health & Care NHS Foundation Trust v. FD& Ors [2023] EWHC 2634 (Fam), [13] (Francis J).
76.
See Office of the Public Guardian, MCA Code of Practice, para 5.31.
77.
R (Burke) v. General Medical Council [2005] EWCA Civ 1003, [63] (Lord Phillips MR).
78.
See Patricia’s Father and Ors v Patricia and Ors [2025] EWCOP 30 (T3).
79.
Article 5(1)(e) (our italics).
80.
Enhorn v. Sweden [2005] ECHR 56529/00, [44] (on the lawfulness of detention to prevent the spreading of infectious disease).
81.
Shtukarov v. Russia [2008] ECHR 44009/05, [114].
82.
Stanev v. Bulgaria [2012] ECHR 46, [111].
83.
Op. cit., [213].
84.
Boffa v. San Marino [1998] ECHR 26536/95; Calvi and CG v. Italy [2023] ECHR 46412/21.
85.
Reynolds v. UK 2694/08, (2012). And see Rabone v. Pennine Care NHS Foundation Trust [2012] UKSC 2.
86.
General Comment No. 1: Article 12, Equal recognition before the law (11th sess. Geneva).
87.
Op. cit., para 3.
88.
[2014] UKSC 19, [45].
89.
90.
D. Viljoen, E. King, S. Harris, J. Hollyman, K. Costello, E. Galvin, M. Stock, U. Schmidt, J. Downs, M. Sekar, C. Newell, S. Clark-Stone, A. Wicksteed, C. Foster, F. Battisti, L. Williams, R. Jones, S. Beglin, S. Anderson, T. Jebarsan, V. Ghuys, and A. Ayton, ‘The Alarms Should no Longer be Ignored: Survey of the Demand, Capacity and Provision of Adult Community Eating Disorder Services in England and Scotland Before COVID-19’, British Journal of Psychiatry Bulletin (2023), p. 1.
91.
Council of Europe, European Committee for the Prevention of Torture and Inhuman or Degrading Treatment or Punishment (CPT) Means of Restraint in Psychiatric Establishments for Adults (2017), CPT/Inf(2017)6, 1.2-1.4 (our italics).
92.
[2025] ECHR 136, [176].
93.
Op. cit., [183].
94.
Op. cit., [189].
95.
See Herczegfalvy v. Austria [1993] 15 EHRR 437, [82].
96.
VI v. Moldova [2024] ECHR 251.
97.
Aggerholm v. Denmark 45439/18 (2020).
98.
Op. cit., p. 54.
99.
Jolloh v. Germany App no 54810/00, [2006] ECHR 721, (2007) 44 EHRR 32, [69]; Ciorap v. Moldova App No 12066/02, [2010] EWHR 1138, [77], Nevmerzhitsky v. Ukraine, App No 54825/00, (2006) 43 EHRR 32, [97].
100.
R (on the application of Maguire) v. His Majesty’s Senior Coroner for Blackpool & Fylde and another [2023] UKSC 20, [145].
101.
Maguire, op. cit., [190].
102.
Herczegfalvy v. Austria [1993] 15 EHRR 437 and see Re F (Mental patient: Sterilisation) [1990] 2 AC 1.
103.
On the importance of individualised care see S. J. Fuller, J. Tan, and D. Nicholls, ‘The Importance of Individualised Care, Good Communication and Trust for Reducing Nasogastric Tube Feeding under Physical Restraint: Qualitative Multi-Informant Study’, British Journal of Psychiatry Open 10(3) (2024), p. e86.
104.
See L. Tulloch, H. Walker, and R. Ion, ‘“It’s the Last Resort” Forensic Mental Health Nurses Experience on the Use of Seclusion; Implications for Use and Elimination in Clinical Practice’, The Journal of Forensic Psychiatry & Psychology 33(6) (2022), p. 828, and see R (on the application of Munjaz v. Mersey Care NHS Trust) [2005] UKHL 58 on seclusion as a last resort.
105.
The Mental Health Trust & Ors v. DD & Anor [2014] EWCOP 13, [37] (Cobb J).
106.
On the benefits of early discussions with patients, see S. J. Fuller, J. O. Tan, and D. Nicholls, ‘Decision-Making and Best Practice when Nasogastric Tube Feeding under Restraint: Multi-Informant Qualitative Study’ British Journal of Psychiatry Open 9(2) (2023), p. e28.
107.
J. O. Tan et al., ‘Control and Compulsory Treatment in Anorexia Nervosa’; J. O. Tan, A. Stewart, R. Fitzpatrick, and T. Hope, ‘Attitudes of Patients with Anorexia Nervosa to Compulsory Treatment and Coercion’, International Journal of Law and Psychiatry 33(1) (2010), p. 13.
108.
See discussion of Barnet, Enfield and Haringey Mental Health NHS Trust v. CC & Ors [2024] EWCOP 65 (T3) above.
109.
See, for example, Parliamentary and Health Service Ombudsman, Ignoring the Alarms; House of Commons Public Administration and Constitutional Affairs Committee, Ignoring the Alarms Follow-Up: Too Many Avoidable Deaths from Eating Disorders (2019, HC855).
110.
S. J. Fuller, J. Tan, J. De Costa, and D. Nicholls, ‘Nasogastric Tube Feeding Under Physical Restraint: Comprehensive Audit and Case Series Across Inpatient Mental Health Units in England’, British Journal of Psychiatry Bulletin 47 (2023), p. 322.
111.
S. J. Fuller, A. Ruck Keene, and J. O. Tan, ‘Long-Term Nasogastric Tube Feeding Under Physical Restraint: Indications for Best Practice’, Cutting Edge Psychiatry in Practice Winter (6) (2024), p. 257.
112.
Including, inter alia, taking into account: the care and treatment that will be of most benefit; the range of options available for care and treatment, and the person’s past and present wishes about their care and treatment (section 1(3)).
113.
Including, inter alia, that the intervention must be of benefit to the individual; the least restrictive in relation to the person’s freedom in order to achieve the desired benefit; and take account of the past and present wishes of the adult and other relevant parties (section 1(2)-(4)).
114.
See, for example, Mental Welfare Commission for Scotland, Rights, Risks and Limits to Freedom: Good Practice Guidance (2021), p. 1: ‘We believe that restraint should be seen as a ‘last resort’, where there is absolutely no alternative.’