
Abstract
This article examines the development of sanctioning practices by disciplinary bodies in the United Kingdom in response to medical error using the Bawa-Garba case as a benchmark for analysing reform. It combines statistical analysis of General Medical Council (GMC) and Medical Practitioners Tribunal Service (MPTS) sanctioning data from 2019 to 2024 with qualitative case studies to identify changes in regulatory responses after Bawa-Garba, including a reduction in investigations but an increase in the severity and probability of sanctions when cases proceed. By analysing selected MPTS decisions related to clinical failings, the study highlights an increased focus on contextualised culpability, remediation, and the systemic factors contributing to errors rather than outcome. The article draws on Merry and Brookbanks’ error/violation framework aswell as Cribb, O’Hara and Waring’s justice typology, to advocate for a ‘qualified blame’ approach to medical error as an alternative to retributive or ‘no blame’ approaches. This approach, focused on contextualising errors, promotes openness, learning, and continuous improvement in patient safety thereby contributing to the development of a ‘just culture’.
Sanctioning medical professionals plays a critical role in safeguarding patient rights, maintaining professional standards, and shaping the culture in medicine. Imposing sanctions on doctors following professional or regulatory proceedings after a medical error occurs is an important process undertaken by the General Medical Council (GMC). It occurs at the end of the fitness to practise assessment where a doctor is judged to have failed to meet the standards of good medical practice required by the medical profession. Importantly, its overarching purpose is to protect the public by ensuring that registered doctors uphold high standards of conduct and competence and so are fit to practise. However, in pursuing this aim, it is essential to ensure that doctors are treated fairly through proportionate and just sanctioning decisions.
The R v Bawa-Garba (Hadiza) (2016) case, involving the death of 6-year-old Jack Adcock, represented a watershed moment in the debate on whether doctors are sanctioned appropriately by their regulator. 1 It highlighted the difficulty in attaining a just outcome for the doctor in a sanctioning decision when other systemic factors including poor working conditions, rota gaps, and technological failures contribute to shortcomings in patient care. 2 This case has been the focus of extensive discussion involving conflicting arguments within the medico-legal sphere, especially in relation to the criminal offence of gross negligence manslaughter (GNM), but also in relation to the medical profession’s perception of lack of fairness of the sanctioning process by the GMC. For the purposes of this article, the Bawa-Garba case serves as a benchmark for examining changes in sanctioning practices between 1 January 2019 and 1 January 2024.
This article examines how disciplinary bodies in the United Kingdom, particularly the GMC and MPTS, have responded to medical error and proposes recommendations for improving this process. It begins by setting out the challenge of medical error and the role of regulation in improving patient safety. The article initially adopts a broad definition of medical error being ‘the failure of a planned action to be completed as intended or the use of the wrong plan to achieve an aim’ 3 but later introduces Merry and Brookbanks’ distinction between errors and violations to assess culpability more precisely. 4 It then uses Cribb, O’Hara, and Waring’s justice typology relevant to patient safety to evaluate the responses of disciplinary bodies and their implications for healthcare culture. 5 The key argument presented is that neither a retributive nor a purely ‘no blame’ approach to medical error is sufficient in the clinical context. Instead, a ‘qualified blame’ approach is advocated for which involves the dispersion of blame among all those involved in the error including the individual, the organisation, and the system. This recognises the complexity of medicine without scapegoating. The article proceeds to explore how this framework aligns with recent developments in fitness to practise outcomes, drawing on both quantitative and qualitative data. It demonstrates that while there is some movement towards contextualised, remedial sanctioning, the approach remains inconsistent and lacks a coherent, principled foundation. The article concludes by calling for reform that embeds a ‘qualified blame’ approach into regulatory guidance and practice.
To examine disciplinary bodies’ approach to medical error, this article uses a mixed-methods approach combining both statistical data and case study analysis. The statistical data is drawn from publicly available GMC and MPTS sources, including its annual Fitness to Practise reports and MPTS reports to Parliament on the types and rates of sanctions that have taken place post Bawa-Garba between 1 January 2019 and 1 January 2024. This data is used to identify broader trends in sanctioning and demonstrates that while the number of fitness to practise investigations has decreased, when doctors are investigated, they are more likely to be sanctioned and the sanction is likely to be more severe. The next section of the article presents a case study analysis. This begins with the well-known Bawa-Garba case and extends to more recent decisions published by the MPTS between 1 January 2022 and 1 January 2024. This 2-year timeframe was selected as it aligned with the period during which this article was being written, and because all decisions remain available on the MPTS website for a period of 12 months, enabling a rolling analysis. During this period, 523 MPTS decisions were published. These included 128 erasures, 210 suspensions, 31 conditions, 1 undertaking, 36 findings of no impairment with a warning, 6 findings of impairment with no further action, 107 findings of no impairment, and 4 voluntary erasures. For the purposes of this article, five decisions were selected for detailed analysis. The selection process followed a purposeful sampling strategy. First, cases were filtered to include only those involving allegations of deficient clinical care as opposed to cases based primarily on criminal convictions, sexual misconduct, or dishonesty in non-clinical contexts, which represented the majority of MPTS decisions during this period. Second, only cases involving a single instance or consistent type of clinical failure were included, excluding more complex cases where allegations spanned multiple different incidents or extended timeframes. Finally, from this subset, one case was selected to represent each major type of regulatory outcome from no impairment to erasure in order to illustrate the spectrum of responses to medical error and assess how these align with the theoretical justice models examined in this article.
This study contributes to the existing literature by combining statistical data with detailed case analysis to examine how sanctioning practices have evolved in the years following the Bawa-Garba case. The statistical analysis highlights broader trends, notably, a decline in the number of investigations, a rise in the proportion of those investigations resulting in sanctions, and a consistently high use of erasure and suspension. While these figures suggest that sanctions remain a common outcome, they do not explain the reasoning behind them. The case studies fill this gap by providing qualitative evidence of how the MPTS approaches sanctioning decisions and this demonstrates an increasing focus on culpability, remediation, and the systemic context of medical errors rather than on clinical outcomes alone. This article overall critically examines the current methods used by disciplinary bodies to address medical error and suggests improvements to this process, aiming to inform and influence policy development in this under-researched area of health and medical law literature.
The challenge of medical errors and determining the appropriate response
Patient safety has not formed part of the regulatory conversation in medicine until relatively recently. The ‘To Err is Human’ report published in 1999, brought to light issues regarding patient safety and the widespread occurrence of mistakes being made in hospitals in the United States. 6 This report caused a ripple effect around the world and marked the beginning of a strong patient safety movement. 7 In England, in a report published in 2020, it was estimated that there were between 19,800 and 32,000 cases of ‘probably avoidable’ significant harm to patients in primary care each year and the cost of clinical negligence claims incurred as a result of incidents in 2020 was £7.9 billion. 8 It was also estimated that in 2020, 237 million medication errors occurred in England, contributing to more than 1,700 deaths. 9 These figures reflect not only the scale of avoidable harm, but also the urgent need for intervention to improve the safety and reliability of healthcare delivery. One such mechanism is regulation. Julia Black describes regulation as ‘the sustained and focused attempt to alter the behaviour of others according to defined standards or purposes with the intention of producing a broadly identified outcome or outcomes, which may involve mechanisms of standard-setting, information-gathering and behaviour modification’. 10 In the clinical context, regulation encompasses professional registration, conduct standards, governance mechanisms, and disciplinary oversight each aimed at shaping practice, reducing risk, and supporting safe care. It is therefore important that the role of professional regulation as a method of altering behaviour to improve safety is examined.
For the purposes of the following section, an error is broadly defined according to James Reason’s definition used in ‘To Err is Human’ as ‘the failure of a planned action to be completed as intended or the use of the wrong plan to achieve an aim’. 11 Fundamentally, underlying the debate on regulating for patient safety is a variety of opposing points of view on how individuals who make medical errors should be treated by the professional regulatory system. At one end of the spectrum, it is argued that errors that harm patients or threaten patient safety are the result of individual failings and that those individuals should be ‘blamed and shamed’ for the adverse patient outcome. At the other end of the spectrum lies a ‘no blame culture’, wherein healthcare practitioners are never held personally responsible for errors. Instead, transparency is regarded as an effective approach to facilitate learning and minimise the occurrence of future mistakes. 12 However, most errors in the healthcare environment are complex, involving several contributing factors that have converged such as communication breakdown, systems failure, equipment issues, to name just a few. Consequently, the debate on the allocation of responsibility and blame for medical error lies on a spectrum.
The concept of a ‘just culture’ is a major focus in healthcare safety research and policy. 13 This proposes somewhat of a middle ground in the spectrum of blame apportionment as it has been recognised that ‘a unidimensional focus on creating blame-free culture carries its own risks for patient safety’. 14 A ‘just culture’ recognises that healthcare errors arise as a result of imperfect systems, as well as the errors of individuals within the system. 15 Therefore, rather than choosing to apportion full blame to single individuals or to a single systemic failure, a ‘just culture’ aims to promote accountability. However, Wachner and Pronovost have opined that finding the appropriate middle ground between both sides of the debate to create a ‘just culture’ has unfortunately proven to be ‘elusive’. 16
It is important to note that despite this recognition, over the past two decades, cultures found within National Health Service (NHS) trusts have been cited as contributing to major failings in patient safety and care. 17 Several high-profile scandals in the healthcare system such as the Shipman case and the Alder Hey organ scandal have seriously undermined the trust that was previously placed in healthcare professionals and put pressure on the UK government to strengthen accountability methods. 18 The first key report on culture in healthcare ‘An Organisation with a Memory’ was published in 2000 by the Department of Health. It aimed to address this problematic culture by promoting the introduction of an overall ‘informed culture’ within the NHS. 19 Several years later, in 2018, the NHS published another report on the importance of culture to promote safety in the healthcare environment. A ‘Just Culture Guide’ for ‘supporting consistent, constructive and fair evaluation of the actions of staff involved in patient safety incidents’ was published. 20 It notes that an ‘important part of a “just culture” is to be able to explain the approach that will be taken if an incident occurs’ and the guide offers several questions to be asked to deem whether the issue is with the individual or whether it is a wider systems issue. 21 The NHS also published a ‘Being Fair Report’ which focused on the importance of human factors in improving fairness and accountability in the management of clinical incidents. 22 These publications demonstrate that the NHS has been aware of the imperative to move towards a ‘just culture’ since 2000. However, despite this recognition, there has been a lack of clear, coordinated implementation at organisational level. As a result, these initiatives have failed to produce sustained or meaningful change in practice.
This was demonstrated by the Williams Review (2018) 23 and Hamilton Review (2019) 24 which reported that the perception of the culture within healthcare remained a culture of blame. 25 The context of these reviews is important as they were active in highlighting the negative impact of a ‘blame culture’ on patient care, especially after the conviction and imprisonment of David Sellu for GNM following a medical error in 2012 and his successful appeal in 2016. 26 His conviction led to outrage and fear among doctors and even the formation of a group named ‘Doctors and Manslaughter’ in the wake of his conviction. 27 This sentiment was also reflected in the British Medical Association’s (BMA) survey conducted in 2018 which noted that over half (55%) of the doctors surveyed (7,887 doctors) worry that they will be unfairly blamed for errors that are due to systems failures and undue pressures on doctors working in such environments. 28 Furthermore, a more recent NHS staff survey in 2021 affirmed this culture of fear. It stated that 25.1% of respondents felt insecure about raising a concern regarding unsafe clinical practice and 40.6% did not have the confidence in their organisation to address the concern. 29
These statistics immediately followed the conclusion of the Bawa-Garba case, and they demonstrate the concerns experienced by doctors as they practise in fear that even non-culpable errors may result in a sanction. The overarching purpose of sanctioning is the protection of the public. However, determining how best to deliver justice while fostering patient safety and countering a culture of fear is a complex task for the regulator and critical to the protection of the public. Cribb, O’Hara, and Waring suggest that ‘despite aspirations for a “just culture”, the idea of justice itself is rarely discussed explicitly or in depth’. 30 In their 2021 paper, they discuss three accounts of justice that are applicable to patient safety: justice as facing sanctions (retributive justice) which involves a corrective approach; justice as no blame or qualified blame which promotes learning and proportionality; and justice as repair or restorative views of justice which emphasises apology and restoration. 31 These different understandings of justice each have shared important values that contribute to improving patient safety; however, they contend that ‘part of the ongoing muddle about patient safety cultures stems from the lack of focused attention on the nature of implications of justice in the field of patient safety’. 32 While Cribb, O’Hara, and Waring develop their conceptions of justice in relation to the wider patient safety system, they are also of relevance to the fitness to practise regime as both aim to protect the public. The safety regime is prospective, and system-focused, aimed at learning through tools such as incident reporting and risk management. By contrast, sanctioning is retrospective and norm-driven, concerned with adjudicating breaches of professional standards. These regimes operate at different levels: one promotes system resilience, the other promotes individual accountability. However, a ‘just culture’ cannot be achieved without realising consistency between the two regimes. If the safety regime encourages openness and learning, while the disciplinary regime reinforces fear and blame, the system as a whole becomes incoherent. Thus, when examining the GMC’s approach to sanctioning, it is important to consider not only the decisions themselves but also the type of justice they promote and their effects on doctors and patients.
This article advocates for ‘qualified blame’ as the primary approach to addressing medical errors. Rather than advocating for a ‘no blame’ approach which risks excusing even negligent conduct, or a ‘retributive’ approach which may lack context specificity especially in the complex environment of medicine and risks scapegoating individuals, ‘qualified blame’ allows for a contextualised response based on the degree of individual culpability and taking into account all relevant factors. Addressing incidents proportionately even after they have occurred promotes an environment where professionals are encouraged to report occurrences and reflect on their actions without fear of blame. This approach furthers the objective of continuous improvement and overall resilience in the patient safety system.
The process of sanctioning medical professionals
The MPTS adjudication process
The GMC has tasked the MPTS with adjudication of the Fitness to Practise Process. The MPTS is a ‘statutory committee of the GMC and is accountable to the GMC Council and the UK Parliament’. 33 It is ‘independent in [its] decision-making and operates separately from the investigatory role of the GMC’. 34 The legal basis for any decision taken by the MPTS is grounded in the Medical Act 1983 and must be consistent with its overarching objective to:
(a) protect, promote, and maintain the health, safety, and well-being of the public;
(b) promote and maintain public confidence in the medical profession; and
(c) promote and maintain proper professional standards and conduct for members of that profession. 35
Sections 35D and 38 of the Medical Act 1983 set out the main powers of the MPTS and rules 15-17 of the GMC (Fitness to Practise) Rules 2004 as amended set out the fitness to practise procedure and how the tribunal works. 36 The arrangements and composition of the MPTS are set out in the GMC (Constitution of Panels, Tribunals and Investigation Committee) Rules Order of Council 2015 statutory rules. 37 The MPTS is responsible for determining whether a doctor’s fitness to practise has been compromised, and if so, what actions need to be taken to address the breach of GMC standards. The tribunal assesses the case and determines whether the allegations are true, whether the doctor’s fitness to practise has been affected, and what action, if any, should be taken. 38 The tribunal can choose from a range of actions, including taking no action, accepting undertakings from the doctor (if agreed upon by the GMC), placing conditions on the doctor’s registration, suspending the doctor’s registration, or erasing the doctor’s name from the medical register, preventing them from practicing medicine. 39
The Sanctions Guidance
The MPTS has published a Sanctions Guidance document for the tribunal and GMC decision-makers. 40 This guidance is for use by the MPTS when considering what sanction to impose following a finding that a doctor’s fitness to practise is impaired. 41 The current guidance applies to new hearings starting on or after 5 February 2024. 42 The guidance makes sure that the parties are ‘aware from the outset, of the approach that the tribunal will take to imposing sanctions’. 43 It has been outlined by the court on multiple occasions and recently in General Medical Council v Simon Bramhall (2021) that departure from the Sanctions Guidance must be accompanied by clear reasons why this departure was necessary. 44 According to the guidance, the tribunal ‘must consider the overarching objective of protecting the public’ and a proportionate approach must be taken by the tribunal to imposing sanctions. 45 Importantly, the guidance notes that ‘sanctions are not imposed to punish or discipline doctors, but they may have a punitive effect’. 46
Recent data on sanctioning
The statistical analysis presented in this article draws on publicly available data from the GMC’s website, including its annual Fitness to Practise reports and MPTS reports to Parliament over the 5-year period following the conclusion of the Bawa-Garba case between 1 January 2019 and 1 January 2024. A summary of key figures is set out in Table 1.
Summary of GMC Fitness to Practise Data (2019-2023).
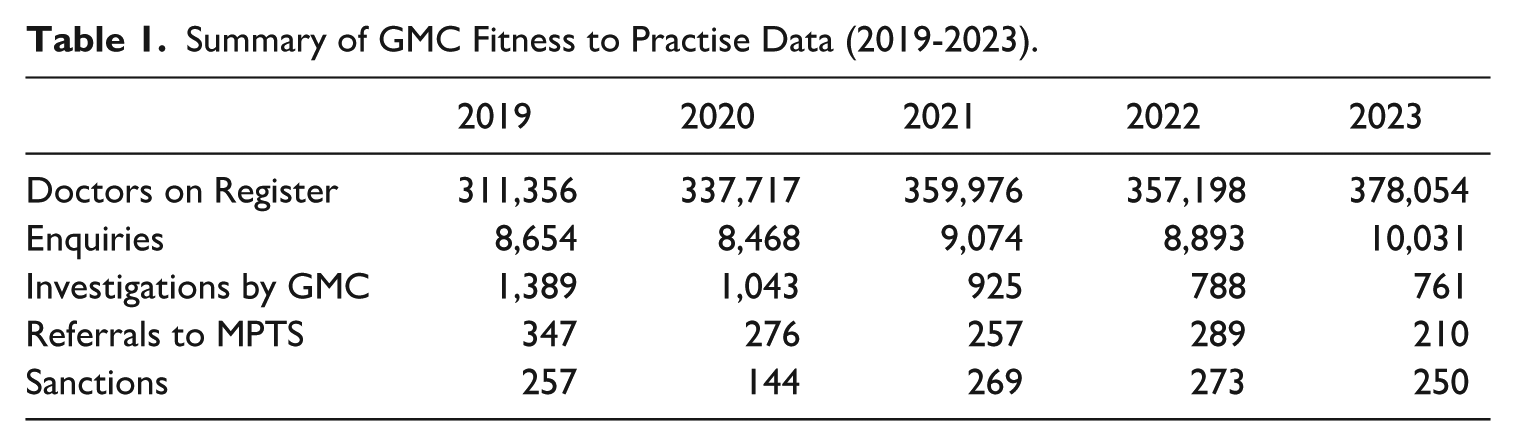
As can be seen from Table 1, over the 5 years studied (2019–2023), the number of fitness to practise investigations conducted by the GMC has decreased significantly from 1,389 in 2019 to just 761 in 2023. This decline has occurred despite a rise in both the number of doctors on the medical register and the number of initial enquiries made to the GMC. One likely explanation is due to the commitment by the GMC to only investigate issues that are serious rather than trivial. 47 Currently, complaints can be made by a wide range of individuals, including patients, families, colleagues, other healthcare professionals, to the employer through a complaints process before being sent to the GMC where appropriate. Notably, the BMA has recently reiterated its call on the GMC to only investigate ‘significant breaches’ of Good Medical Practice guidelines and not to ‘impose sanctions on vulnerable doctors as a way of sending a message to the wider medical profession’. 48 It is also noteworthy that in certain years, the number of sanctions recorded exceeded the number of referrals to the MPTS. This may be attributed to factors such as the time lag between referral and sanctioning, as well as instances where multiple sanctions are issued within a single case or cases are reheard or reviewed.
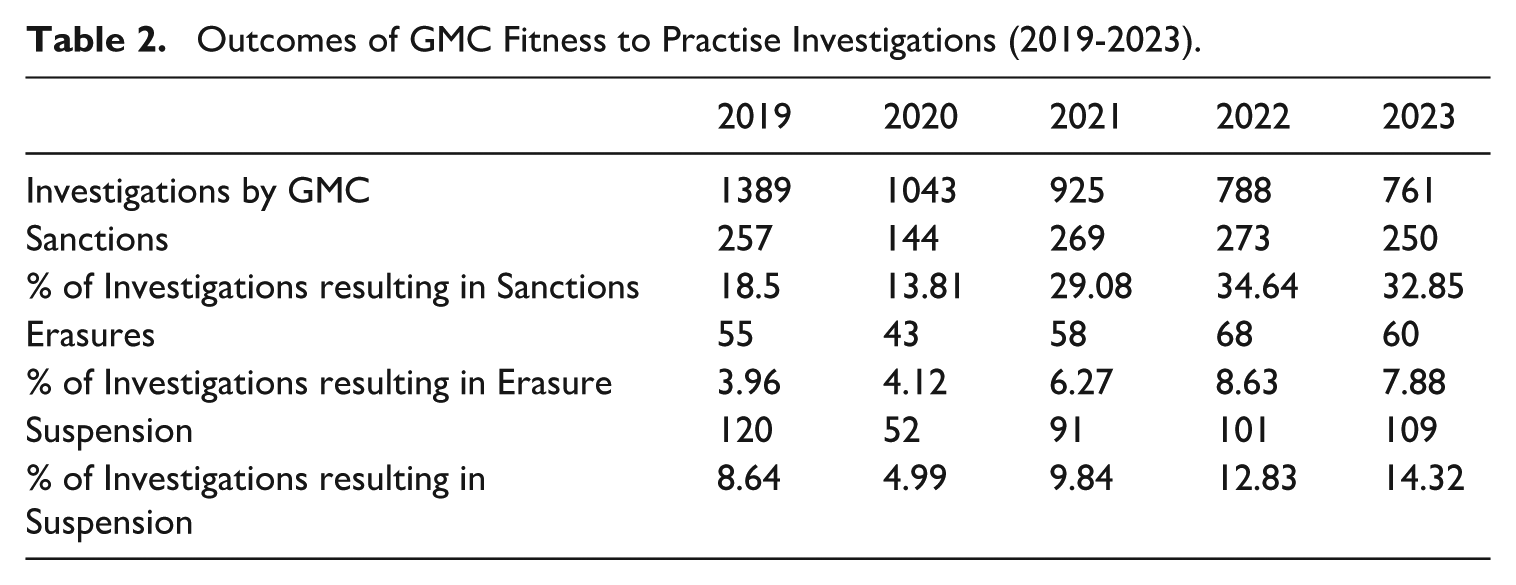
Despite the decline in investigations, Table 2 demonstrates that the percentage of those investigations that resulted in sanctions has steadily increased from 18.5% in 2019 to over 32% in 2022 and 2023. This suggests that although fewer doctors are being investigated, those who are investigated are more likely to be sanctioned. A similar trend is seen with erasures. While the overall number of erasures has remained fairly consistent year to year, the percentage of investigations ending in erasure has almost doubled from 3.96% in 2019 to 7.88% in 2023. Similarly, although the number of suspensions has only slightly decreased from 120 in 2019 to 109 in 2023, this now represents a much larger proportion of total investigations rising from 8.6% to over 14%. These figures indicate that the GMC is becoming more selective about who it investigates, but also more likely to impose serious outcomes once an investigation is underway.
Outcomes of GMC Fitness to Practise Investigations (2019-2023).
In terms of the reasons cited by the MPTS for findings of impaired fitness to practise, misconduct remains the most common. In 2023, 77.6% of all findings of impairment were attributed to misconduct, a slight increase from 75.1% in 2022. This change is not statistically significant using a two-proportion z test, suggesting the change is likely attributable to random variation rather than a substantive shift in regulatory decision-making. However, this apparent stability must be interpreted in the context of broader changes to the GMC’s approach. Over the same period, the number of investigations declined markedly, while the overall number and severity of sanctions increased. This raises the possibility that the cases now being investigated are on average, more serious or clear-cut. In this light, the consistent proportion of misconduct-related sanctions may reflect a more selective and targeted regulatory strategy, in which lower-level concerns are filtered out earlier, and those that proceed to investigation are more likely to involve serious misconduct. Thus, while the proportion itself appears unchanged, it may in fact signal a shift in the nature and gravity of the cases being pursued. The second most frequently cited reason for impaired fitness to practise was criminal conviction, accounting for 9.2% of impairment decisions in 2023 and 9.5% in 2022. From a qualitative review of the decisions resulting in erasure and suspension published on the MPTS website in 2022 and 2023 for the purposes of the case study analysis later on in this article, the most common categories of misconduct include sexually motivated behaviour or harassment towards colleagues or patients, dishonesty on job applications or other documentation, and issues related to inappropriate prescribing.
Overall, the statistical data presented in this section reveals an important shift in the GMC’s approach to fitness to practise investigations over the studied period. While the total number of investigations has steadily declined, the proportion of those investigations resulting in sanctions, particularly suspensions and erasures, has increased. Misconduct continues to be the most common basis for a finding of impairment, and although the proportion of misconduct-related sanctions has remained statistically stable, this must be understood in the context of a more selective investigative process. The narrowing of the investigative scope appears to reflect a prioritisation of high-risk or egregious cases, with less serious concerns increasingly filtered out. This shift is further evidenced by the rise in sanction severity, including an increase in the proportion of erasures. Collectively, these trends suggest a regulatory strategy that favours fewer investigations but stronger outcomes, signalling that serious misconduct will attract a robust and decisive response.
The complexity of sanctioning medical mistakes
Sanctioning medical errors is inherently complex. Merry and Brookbanks suggest that medical mistakes should be grouped into two broad categories: ‘errors’ and ‘violations’, to apportion individual blameworthiness. 49 In their view, an ‘error’ is a mistake that occurs by virtue of the individual being human and lacks all culpable elements, except in the case of an ‘egregious error’ which equates with ‘grossest ignorance’. 50 Importantly, it is the ability or unexercised capacity to do things differently that is the necessary ingredient for culpability. 51 A ‘violation’, on the other hand, is defined as intentional deviation ‘from those practices deemed necessary . . . to maintain the safe operation of a potentially hazardous system’. 52 In this instance, the doctor may have chosen to ‘risk some aspect of safety or the system’. 53 Importantly, violations ‘involve choice’ and are therefore always culpable, although they are not all equally blameworthy. 54
The categorisation of errors and violations in healthcare is especially persuasive as when a doctor ‘tries to do the right thing and ends up doing the wrong thing’, it can result in death or serious lifelong injury for the patient. 55 It follows that regulatory sanctioning should be grounded not in the outcome alone, but in a proper assessment of the practitioner’s moral responsibility. However, in practice, error responses sometimes prioritise harm or reputational impact over culpability or context, contributing to a blame culture and the risk of scapegoating. In contrast, the approach developed by Merry and Brookbanks centres on culpability while also recognising the wider organisational and systemic contributors to medical error. This approach is compatible with the ‘qualified blame’ model proposed by Cribb, O’Hara, and Waring as under this model, blame is not isolated at the ‘sharp end’ of the error but is understood as potentially dispersed across multiple actors and institutional layers who have collective responsibility for the organisation and its systems. ‘Qualified blame’ is distinct from retributivism but shares with it concern for moral responsibility. Retributive theories of justice hold that punishment is justified when deserved. ‘Qualified blame’, while not incompatible with this view, goes further by emphasising the systemic and organisational context in which clinical errors occur, ensuring that responsibility is fairly distributed and proportionate to actual control and decision-making capacity. It aligns closely with the values of a ‘just culture’ recognising the limitations of individual blame within complex systems and acknowledging that patient harm is rarely the result of individual wrongdoing alone. 56
However, neither the Sanctions Guidance nor the Good Medical Practice document refers to ‘intention’ or ‘mistake/error’. Indeed, the ‘Making Decisions on Cases at the End of the Investigation Stage: Guidance for the Investigation Committee and Case Examiners’ document which is used in the preliminary investigation stage of the fitness to practise process also does not mention intention as a factor that is taken into consideration. 57 All the guidance documents mentioned focus on the seriousness of the misconduct and subsequently, the doctor’s actions following the incident. There is a brief mention of mistake/error in the Fitness to Practise Guidance that notes that ‘doctors do make mistakes’ and ‘once off mistakes are unlikely to result in an impairment of the doctor’s fitness to practise’. 58 However, ‘serious or persistent’ failures to follow guidance may put a doctor’s registration at risk. 59 While these documents repeatedly stress the need to protect the public, they do not clearly define how key concepts such as ‘seriousness’ or ‘persistence’ are to be interpreted, nor do they require an assessment of intention, foresight, or culpability. As a result, significant discretion is afforded to decision-makers, allowing them to project different meanings onto these terms without a principled or transparent framework. The definition of ‘seriousness’ generally in fitness to practise decisions has been examined by Bryce et al. across a number of professional regulators including the GMC, the General Dental Council, and the Nursing and Midwifery Council and they concluded that ‘there is no clear and concise definition of seriousness in relation to fitness to practise nor did one arise from [their] research’, and at an individual case level, there can be within regulator variation depending on the features of the specific case. 60 This means that, considerable discretionary power is afforded to tribunals and investigatory committees depending on the facts of the case, and how ‘seriousness’ is defined. The result is a regime where doctors may be sanctioned not because they were culpable, but because harm occurred or standards were breached repeatedly depending on the interpretation of ‘serious or persistent’ by the tribunal on the day of their decision. This does not lead to consistency in decision-making and creates uncertainty among doctors regarding the standards they should follow.
To address this, the Sanctions Guidance should be revised to incorporate a principled framework for evaluating culpability and moral responsibility. Merry and Brookbanks’ framework offers a useful foundation for differentiating between errors and aligns with a ‘qualified blame’ conception of justice. Without reform, regulatory sanctioning remains overly discretionary, unpredictable, and not conducive to the promotion of a ‘just culture’.
The evolution of sanctioning: case studies on the changing approach to medical errors
The Bawa-Garba case 61
On the 18th of February 2011, 6-year-old Jack Adcock, a child with Down’s syndrome and a known heart condition who had undergone previous cardiac surgery and required long-term medication, was admitted to the Children’s Assessment Unit at the Leicester Royal Infirmary. Following his admission, Dr Hadiza Bawa-Garba, a trainee doctor in her sixth year of Paediatric Specialty training, who had just returned from 14 months maternity leave, was responsible for his care with the assistance of two nurses. Dr Hadiza Bawa-Garba was the most senior trainee doctor on duty that day and admitted Jack and diagnosed him with acute gastroenteritis and dehydration. After an X-ray, he was subsequently treated for group A streptococcal infection (pneumonia) with antibiotics, but by that stage the infection had caused his body to go into septic shock, resulting in multi-organ failure. Resuscitation was initially interrupted due to a mistaken belief that Jack was a child with a ‘Do Not Resuscitate’ order. All subsequent efforts to resuscitate him failed and he went into cardiac arrest and died a few hours later.
Several systemic factors affected Jack Adcock’s care. There was a delay in obtaining the results of his examinations, including the result of his chest X-ray due to a breakdown in the computer system in the hospital, a shortage of permanent nursing staff with a resulting reliance on short-term agency nurses (one of whom failed to record his temperature, heart rate and blood pressure regularly and communicate his deterioration), further delays by nursing staff to inform Dr Hadiza Bawa-Garba that the Jack’s X-ray results were available, and delayed administration of prescribed antibiotics. 62 It should be noted that it was accepted that even on his admission, Jack was at risk of death from his pre-existing medical condition (quantified in the range of 4%–20.8%). However, expert evidence revealed that clinical signs of septic shock were present in Jack on admission. Following a post-mortem, the cause of death given was systemic sepsis complicating a streptococcal lower respiratory infection (pneumonia) combined with Down’s syndrome and previous heart surgery.
The case was brought by the Crown, that all three members of staff on duty that evening contributed to or caused Jack’s death and there was serious neglect that fell so far below the standard of care expected of competent professionals, that it amounted to the criminal offence of GNM. In 2015, Dr Hadiza Bawa-Garba was convicted in the High Court of GNM and given a 2-year suspended sentence. On 29 November 2016, the Court of Appeal (Criminal Division) refused her leave to appeal her conviction. Following this conviction, the MPTS convened in February 2017 to determine whether Dr Hadiza Bawa-Garba’s fitness to practise was impaired. On 13 June 2017, the MPTS issued a decision of impairment and imposed an immediate suspension for a period of 12 months. It found that the maximum suspension of 12 months was sufficient to maintain public confidence in this case, given the mitigating factors present and the fact that she did not present a risk to future patients and had undertaken significant remediation since the incident occurred.
Subsequently, the GMC exercised its right of appeal under s.40A of the Medical Act and appealed the decision of the MPTS to the Divisional Court to ‘uphold the reputation of the profession’. 63 The High Court concluded that Dr Hadiza Bawa-Garba should be erased from the medical register on the basis that ‘given the verdict of the jury which held that her conduct was “truly exceptionally bad” in the criminal case, nothing short of erasure would uphold public confidence in the profession’. 64 Following the court’s decision, massive crowdfunding took place by colleagues in the medical profession in response to what they felt was the ‘scapegoating’ of Dr Hadiza Bawa-Garba for systemic faults within the healthcare system. The funds raised were used by Dr Hadiza Bawa-Garba to appeal the decision to the Court of Appeal which then overturned the Divisional Court’s decision, stating that the ‘presumption of erasure’ adopted by Judge Ouseley in the GMC appeal was ‘impermissible’. 65 The court held that ‘although there are some cases where the facts are such that the most severe sanction, erasure, is the only proper and reasonable sanction, this [was] not one of them’. 66 It reinstated Dr Hadiza Bawa-Garba’s suspension in place of erasure and remitted the matter to the MPTS for review.
The 2018 review convened by the MPTS determined that Dr Hadiza Bawa-Garba’s fitness to practise was still impaired, and she should be subject to a further 6-month suspension period. In 2019, the tribunal determined that it was satisfied that Dr Hadiza Bawa-Garba ‘had sufficient insight into her conviction, its seriousness and its consequences’. 67 The tribunal also held that as she had already served a 18-month suspension ‘the public interest had been served’ and instead, conditions were placed on her registration for 24 months and eventually, in 2021, Dr Hadiza Bawa-Garba was reinstated to practise without conditions.
Reflections on the Bawa-Garba case: a disjointed approach to justice
The Bawa-Garba case highlights the inconsistent approaches to justice taken by each of the bodies involved in her sanctioning. Initially, the MPTS decided to suspend Dr Hadiza Bawa-Garba for 12 months, taking into account mitigating factors and determining that she posed no risk. This decision aligned with a ‘qualified blame’ approach that contextualised her errors considering the systemic issues present on the day. The GMC then appealed this decision to uphold the public’s trust in the profession. This appeal took a more retributive approach which focused on the gravity of the outcome (the criminal conviction and the patient’s death) as deserving of a correspondingly severe sanction. At the Appeal, the High Court focused on Dr Hadiza Bawa Garba’s conduct being ‘truly exceptionally bad’ as the basis for warranting erasure, signalling that certain levels of error necessitate corresponding levels of sanctioning. This approach was later reversed on appeal by the Court of Appeal who held that there was no presumption of erasure and reverted to a ‘qualified blame’ approach, indicating that the severity of the sanction should be based on the facts of the case.
Procedurally, this case demonstrates that no presumption of erasure exists following a conviction of GNM as the Court of Appeal made it clear that the Sanctions Guidance should not be taken to guide the MPTS towards erasure after ‘serious harm to others deliberately or through incompetence’. 68 It confirmed that it merely permits erasure in those circumstances. 69 Hodson has criticised the language of the Guidance, arguing that it gives no absolute circumstances in which a doctor should be erased or suspended and therefore fails to be directive. 70 For instance, paragraph 109 of the Guidance states that ‘any of the following factors present may indicate erasure is appropriate (the list is not exhaustive)’. 71 The word ‘may’ in this sentence gives the MPTS the discretion to decide whether or not to erase the doctor and states no definitive circumstances where erasure is mandatory. Hodson argues that this diminishes the fundamental importance of the GMC Good Medical Practice document which is directive in its provisions using language such as ‘you must’ and ‘you should’. 72 This lack of direct guidance gives the tribunal considerable discretionary power in their decision-making but gives the doctor less certainty of the possible consequences of their actions. 73 While the GMC claims that the guidance makes sure that ‘parties are aware from the outset of the approach the tribunal will take to imposing sanctions’, this demonstrates that this is not the case.
Overall, the Bawa-Garba case exemplifies a disjointed approach to justice and a clear mismatch between the GMC literature promoting the implementation of a ‘just culture’ in medicine, and the ‘blame culture’ that exists in practice. Given that the MPTS had previously determined that Dr Hadiza Bawa-Garba did not pose a risk to future patients, there was no clear public protection rationale for the GMC’s appeal. In the absence of the need to protect the public from Dr Hadiza Bawa-Garba’s practice, the decision to pursue erasure appeared symbolic, aimed at preserving institutional credibility rather than the public’s protection. The Williams Review which followed the case recommended removing the GMC’s right of appeal, a recommendation which has yet to be implemented. For many in the medical profession, the GMC’s appeal represented ‘post-conviction litigation’ and the GMC ‘going after doctors’. 74 Rather than fostering accountability rooted in learning and reflection, the response projected an institutionally defensive approach, where a tragic outcome outweighed a nuanced understanding of culpability. If, as Merry and Brookbanks contend, violations deserve sanction and errors demand support, then the GMC’s actions inverted this principle penalising a doctor for a system failure.
More recent sanctioning decisions: a change in approach
The statistical data has quantitatively demonstrated the evolution of sanctioning practices in recent years. The following section will review case studies of recent MPTS sanctioning decisions to introduce a qualitative perspective to provide a more fulsome understanding of the MPTS’ approach to decision-making.
Dr Susannah Rowles – July 2022 75
Consultant Physician, Dr Susannah Rowles placed an elderly patient on palliative care without the patient or her family’s consent. She was accused by the GMC of a number of clinical failings aswell as failing to actively treat the condition of the patient. She was also accused of making untrue entries in the medical notes regarding the primary cause of death noting it to be a pulmonary embolism rather than sepsis. At the hearing, the tribunal held that the failure to treat the patient’s condition and failure to control atrial fibrillation were serious omissions with grave consequences and accepted the expert evidence that the lack of antibiotics and rate control contributed most to the deterioration and death of the patient. However, it was found that Dr Rowles truly believed that the patient had a pulmonary embolism rather than sepsis and an expert witness at the hearing opined that this was a plausible diagnosis. The tribunal therefore did not find the dishonesty charges against Dr Rowles proven.
In considering the imposition of a sanction, the panel considered Dr Rowles remediation, lack of repetition, and the fact that this was a ‘single clinical incident, in the context of a long unblemished career’. They noted the fact that she had admitted from the outset that she had made an error in deciding not to actively treat the patient’s sepsis, ‘a decision she cannot explain and has lived to regret’. 76 The tribunal concluded that Dr Rowles’ fitness to practise was impaired by reason of her serious misconduct. However, it chose not to take any action against her reasoning that the finding of impairment alone ‘sent out a signal that was strong enough’ and that ‘the exceptional circumstances of the case mean that any further sanction would be disproportionate’. 77
This case is significant when viewed through the lens of the conceptions of justice discussed earlier. It strongly reflects a ‘qualified blame’ approach as the tribunal recognised that the error occurred within a complex clinical situation, that systemic factors were at play, and that Dr Rowles had shown insight and remediation. The misdiagnosis itself fits within Merry and Brookbanks error category as it was deemed to be unintentional given Dr Rowles’ belief that the patient had a pulmonary embolism rather than sepsis. The tribunal’s reasoning avoided conflating the tragic outcome with culpability and this decision should come as a welcome relief to doctors as it demonstrates that where a doctor acts on a mistaken but plausible belief they will not be sanctioned for this decision. However, it is notable that no formal sanction was imposed despite a finding of ‘serious misconduct’. Instead her fitness to practise was deemed impaired as a signal to others rather than affecting her own ability to practise. This approach raises questions about the meaning of a finding of impairment and whether such decisions provide clear guidance to other doctors or cause confusion when ‘serious misconduct’ results in no sanction.
Mr Zulfiquar Rahimtoola – December 2021 (Review 30 August 2022) 78
Hand Surgeon Mr Zulfiquar Rahimtoola accidentally made an incision in the wrong side of a patient’s wrist. He then lied to the patient about the procedure and also lied in writing to the patient’s General Practitioner. 79 At the MPTS hearing, Mr Rahimtoola admitted to almost all of the allegations against him and it was held that his error and dishonesty about what had occurred ‘amounted to serious professional misconduct’. 80
In considering whether Mr Rahimtoola’s practice was impaired as a result of his misconduct the tribunal considered whether this misconduct could be remediated, whether there was evidence of remediation and the likelihood of repetition. It was found that the risk of repetition was extremely small and Mr Rahimtoola had carried out extensive remediation. Therefore, with regard to the surgical error, Mr Rahimtoola’s fitness to practise was found not to be impaired. However, with regard to his dishonesty and failure to comply with the duty of candour, the tribunal noted the principle established in the case of Yeong v GMC (2009)
81
that where a finding of impairment is necessary to uphold public confidence in the profession and to uphold proper standards of behaviour, less weight should be given to the evidence of remediation. In coming to their decision they examined the length of the period of Mr Rahimtoola’s dishonesty aswell as the fact that he was a senior surgeon at the time of the misconduct. The tribunal determined that in view of the seriousness of Mr Rahimtoola’s dishonesty, a finding of impaired fitness to practise was necessary to uphold professional standards and maintain public confidence in the profession.
82
The tribunal then considered the sanction to be imposed and decided
that a member of the public, fully informed about all the circumstances of the case would take the view that the sanction of erasure would be disproportionate and that there was a public interest in Mr Rahimtoola being able to continue to practise.
83
Therefore, a 9-month suspension was imposed.
This case demonstrates the application of Merry and Brookbanks’ framework, which treats human error as non-culpable as the tribunal carefully distinguished between the initial mistake, an unintentional surgical error, and the doctor’s subsequent dishonest response, which constituted a violation as it involved a conscious choice. In doing so, it recognised that while the initial mistake caused harm, it was not blameworthy and did not, on its own, amount to impaired fitness to practise. This reflects a ‘qualified blame’ approach, whereby Mr Rahimtoola’s entire career was taken into account to contextualise the error. However, despite Mr Rahimtoola’s remediation and excellent record, due to his immediate dishonesty after the error, his fitness to practise had to be deemed impaired and a sanction was imposed. This case contains some directive commentary from the MPTS which made clear that in most cases, where there has been dishonesty, a finding of impairment will be made. Unlike the outcome-driven approach seen in Bawa-Garba, this case reflects an effort to impose accountability proportionately and fairly.
Dr Faye Hawkins – November 2022 84
Dr Faye Hawkins, a Consultant Paediatrician, misdiagnosed appendicitis as a stomach upset in a 5-year-old child and inappropriately allowed the ill child to return home from the hospital. The child subsequently died. The tribunal held that Dr Hawkins had failed to see a ‘paediatric red flag’ when the child presented with lethargy, failed to check her hydration status, carry out a second abdominal examination, or look for other possible red flags. However, the tribunal concluded that ‘Dr Hawkins has demonstrated a commitment to ongoing personal and professional development [. . .] it was an isolated incident four years ago in an otherwise unblemished career’ and Dr Hawkins was given a warning.
This decision is another example of the recent approach of the MPTS in considering the entire career of the doctor as well as actions of remediation following the error. Despite the tragic outcome, the tribunal did not treat the clinical failings as amounting to misconduct or impairment, thereby clearly rejecting an outcome-driven approach and demonstrating a clear departure from the Bawa-Garba case. The tribunal’s reasoning reflects aspects of both ‘restorative’ and ‘qualified blame’ conceptions of justice. It prioritised learning, rehabilitation, and the doctor’s insight. At the same time, it did not deny the seriousness of the errors but contextualised them as unintentional lapses rather than a culpable violations, consistent with a ‘qualified blame’ model. While these errors may not have been intentional, from a patient’s perspective, this case raises the question of when mistakes cross the line into incompetence. An incompetent doctor practicing might be considered reckless, potentially constituting a violation under Merry and Brookbanks’ framework. This underlines the need for sanctioning guidance to provide a clear way of distinguishing between human error and professional incompetency.
Mr Camilo Valero Valdivieso – January 2023 85
This case involved a Norfolk surgeon who performed two laparoscopic cholecystectomy procedures on two different patients on 22 and 27 January 2020, respectively. However, he was deemed to have failed to provide adequate clinical care to the patients during these procedures, resulting in ‘life-changing’ injuries for both patients. Mr Valero misinterpreted the anatomy of both patients, and on one of the occasions severed the patient’s gallbladder. Mr Valero also raised his voice, used an aggressive tone, and made gestures towards one of the patients on two occasions. Furthermore, it was also alleged (although found not proven) that Mr Valero failed to provide good clinical care to a third patient when he inappropriately made the decision to discharge that patient from the hospital without adequate assessment. He was also ‘rude’ and ‘unprofessional’ to the patient’s sister.
In its decision, the MPTS stated that Mr Valero’s conduct had fallen below the expected standards of a doctor and that it had put public confidence in the profession at risk. The tribunal held the view that he had ‘embarked on two procedures that were beyond his level of competence’ when the repercussions for his patients were ‘foreseeable and avoidable’ and that his conduct ‘fell so far short of the standards expected of a doctor as to amount to serious misconduct’. However, in determining his fitness to practise, the tribunal held that two elements of his misconduct, the first relating to his clinical abilities and the second relating to his judgement and decision-making, were remediable. It was therefore held that
whilst his misconduct has not necessitated any restriction on his registration in order to protect patients, due to the level of his insight and remediation, it is necessary to issue this formal warning to declare and uphold proper standards of conduct and behaviour; to maintain public confidence in the profession.
86
Therefore, the tribunal held that his fitness to practice was not impaired.
The outcome of this case was significant given the severity of the injuries to his patients and the fact that the same type of ‘foreseeable and avoidable’ problem had occurred on two different occasions. A finding that his fitness to practise was not impaired highlights the absence of any element of recklessness or carelessness in the decision. These errors arguably represent a violation under Merry and Brookbanks’ framework as Mr Valero ‘made the decision to do something in the knowledge that the given action or decision will place at risk some aspect of safety or of the system’. 87 The limited regulatory response in light of two severe clinical outcomes and a repeated pattern of poor judgement raises questions about consistency and proportionality. It also appears to tip the balance significantly in favour of leniency towards the doctor, in sharp contrast with the Bawa-Garba case where a sanction was imposed despite the presence of systemic pressures and no evidence of recklessness. This decision reflects a ‘no blame’ approach and aligns with a strong restorative conception of justice as the doctor’s remediation or repair efforts were considered paramount in the sanctioning decision.
Mr Isyaka Mamman-Aka’aba – 6 April 2023
In April 2023, Mr Aka’aba was struck off the medical register for the death of Shaheen Parveen following a ‘botched biopsy’. 88 He was also sentenced to 3 years imprisonment by Manchester Crown Court following a guilty plea for GNM. Mrs Parveen died following what should have been a routine bone marrow biopsy procedure as part of investigations into possible myeloproliferative disorder. Mr Aka’aba used the incorrect needle, missed the bone, and pierced Mrs Parveen’s pericardium causing fatal bleeding. 89
The MPTS tribunal took into account guidance from the Court of Appeal in the Bawa-Garba case. It held that a doctor should not automatically be struck off following being found guilty of GNM. 90 It is also noteworthy that the court took into consideration the systemic factors in Bawa-Garba and identified a number of systemic failures in this case, including computer malfunctions, inadequate records, and unclear instructions concerning the patient and a lack of standard operating procedures for bone marrow aspiration. 91
In making its decision, the MPTS compared the case to Bawa-Garba and held that ‘albeit in both cases the doctors were found responsible to the criminal standard for the death of a patient, the tribunal was of the view that Mr Aka’aba’s case could be distinguished’ from Bawa-Garba. 92 First, in Mr Aka’aba’s case, concerns had been previously raised about his competency in undertaking bone marrow transplants and therefore the risk of repetition could not be regarded as low, in contrast to Bawa-Garba. 93 Furthermore, the tribunal noted that it ‘appeared to be accepted by the court that the risk of Dr Hadiza Bawa-Garba’s clinical practice suddenly and without explanation falling below the standards expected on any given day was no higher than for any other reasonably competent doctor’. 94 This was not the case with Mr Aka’aba who had demonstrated little evidence of substantial insight or reflection. The tribunal also considered the systemic failings which contributed to the error; however, it concluded that these failings did not displace or otherwise absolve Mr Aka’aba’s responsibility. 95 Therefore, overall, it was decided that his conduct and conviction for GNM would be fundamentally incompatible with continued registration. 96 The tribunal subsequently determined that given the seriousness of his conviction and sanction imposed, and notwithstanding his custodial sentence, Mr Aka’aba should be erased from the medical register. 97
Although decisions are specific to their facts, this process of decision-making that contextualises the error by taking into account the doctor’s whole career and explicitly acknowledging the systemic factors which affected the doctor’s actions should provide some comfort to doctors and represents a very clear ‘qualified blame’ approach. This approach, in a case with a tragic outcome, should contribute to a change from the culture of blame following Bawa-Garba by allowing some predictability in the absence of directive guidance. It will be interesting to observe whether the same decision-making process will be followed in future cases where a doctor with a similarly unblemished record to Dr Hadiza Bawa-Garba is convicted of GNM. Notably, this case also calls into question whether the MPTS were too lenient in their sanctioning of Mr Aka’aba in the past. It seems contrary to patient safety objectives that a doctor who has previously had complaints made against him to the GMC for substandard care on two separate occasions could have been conducting Mrs Pareveen’s operation unsupervised. This calls into question whether she would still be alive today if Aka’aba had been effectively sanctioned in previous investigations.
How far have we come and recommendations for future improvement
The case study analysis demonstrates a significant shift in how regulatory bodies address medical errors. Harm alone is no longer the determinative factor that will result in a sanction, and greater emphasis will be placed on a doctor’s conduct after the error, particularly their insight, remediation, and professional development. This perspective acknowledges that doctors can actively contribute to repairing harm through constructive actions, which may mitigate the need for punitive sanctions. By emphasising the doctor’s response to the error over the harm caused by the error, this approach encourages doctors to acknowledge mistakes and act constructively, which is essential for fostering a learning culture. It shifts the focus from assigning blame for the harm itself to understanding the professional’s efforts to rectify the situation. This change may promote a culture where doctors feel empowered to acknowledge mistakes and take remedial action without fear of automatic, harsh penalties. This aligns with a move towards a ‘qualified blame’ approach to justice, in which responsibility is assessed in context and sanctions are proportionate to individual culpability rather than consequences alone.
However, this shift in approach is not without its potential flaws. The Rahimtoola case seems to demarcate the line between when an error can or cannot be redeemed by remediation, with dishonesty being the most crucial element. Yet, importantly, the tribunal in Rahimtoola focused heavily on the ‘seriousness’ of the dishonesty and not the fact of dishonesty alone. This suggests that it is not dishonesty per se, but rather the degree or significance of dishonesty that triggers impairment, a distinction not clearly reflected in GMC guidance. The ‘Making Decisions on Cases at the End of the Investigation Stage: Guidance for the Committee and Case Examiners’ document sets out that in cases where allegations of dishonesty are proven, there is a presumption of impaired fitness to practise, and these cases will be adjudicated by the MPTS unless the presumption can be successfully rebutted. However, at the MPTS level, recent cases indicate that significant dishonesty, rather than dishonesty alone, results in a finding of impairment. This may send the wrong signal to the medical profession and may not adequately protect the public if a strict stance on dishonesty is not maintained. It is unclear what type of conduct meets the threshold for impairment. An error is not merely an error when dishonesty is involved; it becomes a violation. Categorising errors based on Merry and Brookbanks’ framework, with violations carrying the presumption of impairment, would provide a much clearer standard against which to judge doctors’ conduct.
Furthermore, these recent cases suggest that there is now an allowance by regulatory bodies for the previous conduct and career of the doctor to be a factor in the sanctioning decision. However, this shift raises concerns over whether leniency is being prioritised at the expense of patient safety. While evaluating a doctor’s career pre-error may result in fairer overall assessments, it is crucial to consider the degree of carelessness or recklessness involved in the error. This is especially evident in the Valero case where ‘foreseeable and avoidable harm’ was inflicted on patients, yet the doctor’s recklessness in proceeding with performing the surgeries was not a factor in the decision and his errors were deemed remediable. It seems completely contrary to good medical practice for doctors to be able to knowingly take risks which may seriously harm patients without consequences, even those with an excellent previous career. This approach may leave patients feeling that an error that may have caused serious harm, or even cost a life, and one which Merry and Brookbanks would consider a violation, has been deemed irrelevant and treated as merely an unfortunate statistic in ‘an otherwise competent or useful’ doctor’s ‘otherwise unblemished career’.
There remains a notable lack of clarity in GMC’s guidance on when a medical error will lead to a finding of impaired fitness to practise. While the guidance notes that ‘serious or persistent’ failure to follow guidance will likely result in a sanction, it offers little explanation of what is considered ‘serious or persistent’ in practice. Recent decisions make it difficult to discern how these terms are applied. For instance, Mr Valero made the same error twice on two different patients, on two different days, and his practice was deemed not to be impaired. In contrast, Dr Rowles failed to actively treat a patient and obtain consent which was considered a single clinical event, and her practise was deemed to be impaired. This raises the question: how many times an error needs to be repeated to be deemed ‘persistent’ and what level of harm or deviation from standard practice qualifies as ‘serious’? This absence of definitional clarity leaves doctors uncertain about the boundaries of acceptable conduct and undermines the transparency of the fitness to practise process.
The Aka’aba case reaffirmed that there is no presumption of erasure following a conviction for GNM and therefore reaffirmed the independence of the MPTS and their discretion in following the GMC guidance. However, given that this case involved a doctor with an imperfect medical record, it will be interesting to observe in future similar cases how this decision of whether or not to erase a doctor after a conviction will be approached by the MPTS. Can public confidence in the profession be upheld in the case where a doctor is not erased following a court conviction for GNM?
Taking all of the above into account, the recent decisions show a regulatory climate that is more reflective than Bawa-Garba. This is a welcome development, one that may reduce the culture of blame and encourage openness and learning. But the approach has notable limitations. The lack of clear thresholds for sanctions, the absence of consistent standards for evaluating error versus violation, and the unpredictable interpretation of ‘serious and persistent’ afford too much discretion to the MPTS. A more effective approach to addressing medical error would be to incorporate a ‘qualified blame’ model of justice informed by Merry and Brookbanks’ categorisation of errors. By classifying mistakes based on a clear threshold of individual culpability, this model ensures that blame is applied fairly and proportionately. This framework allows regulators to distinguish between unintentional human error, negligence, and deliberate violations, offering a more principled basis for assessing responsibility. Where appropriate, it leaves space for systemic factors to be taken into account in sanctioning decisions. Crucially, it sets out clear expectations and reduces inconsistent outcomes, helping to ensure that medical professionals are not unfairly punished for system-induced mistakes. In doing so, it offers a more balanced and transparent foundation for professional regulation and is supportive of the development of a ‘just culture’.
Conclusion
This article has critically examined the ways in which disciplinary bodies, particularly the MPTS and GMC, have responded to medical error in the years following the Bawa-Garba case. Drawing on both statistical analysis and case study analysis it has argued that although there is emerging evidence of a shift towards context-sensitive remedial sanctioning decisions, this shift remains inconsistent. Using the conceptions of justice developed by Cribb, O’Hara, and Waring and Merry and Brookbanks’ framework for assessing culpability, the article has shown that justice in this area cannot be achieved through binary models of either retributive punishment or blanket no-blame leniency. Instead, a ‘qualified blame’ approach offers a more principled and balanced foundation, one that recognises the complexity of the clinical environment, differentiates between error and violation, and bases sanctioning on both culpability and context. This approach should be clearly reflected in the GMC’s Sanctions Guidance aswell as the MPTS’ decisions and made easily accessible to doctors and the public to reduce the culture of fear surrounding the fitness to practice process. Only through such principled reform can the profession move beyond the uncertainty and defensiveness triggered by the Bawa-Garba case and embed a culture that supports openness, learning, and justice in healthcare.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author disclosed receipt of financial support for the research, authorship, and/or publication of this article. The author would like to thank the University of Manchester Department of Social Sciences Law Phd Studentship.
Cases
Bawa-Garba v GMC [2018] EWCA Civ 1879.
David Sellu v The Crown [2016] EWCA Crim 1716.
General Medical Council v Simon Bramhall [2021] EWHC 2109 (Admin).
GMC V Dr Hadiza Bawa-Garba [2018] EWHC 76.
R V Bawa Garba (Hadiza) [2016] EWCA Crim 1841.
Yeong v GMC [2009] EWHC 1923.
1.
[2016] EWCA Crim 1841.
2.
3.
Molla Donaldson, Janet Corrigan and Linda Kohn, To Err Is Human: Building a Safer Health System (Washington, DC: National Academies Press,1999).
4.
Alan Merry and Warren Brookbanks in Alan Merry and Alexander McCall Smith’s Errors, Medicine and the Law (2nd edn, Cambridge: Cambridge University Press 2017), pp. 103–183.
5.
Alan Cribb, Jane O’Hara and Justin Waring, ‘Improving Responses to Safety Incidents: We Need to Talk about Justice’, BMJ Quality & Safety 31(4) (2022), p. 327.
6.
Donaldson et al., To Err.
7.
Christopher Neuhaus, Petra Grawe, Johan Bergstom and Michael St. Pierre, ‘The Impact of “To Err Is Human” on Patient Safety in Anaesthesiology. A Bibliometric Analysis of 20 years of Research’, Frontiers in Medicine 9 (2022), p. 1.
8.
9.
Op. cit.
10.
Julia Black, ‘Critical Reflections on Regulation’, Australian Journal of Legal Philosophy 27(1) (2002), p. 1.
11.
James Reason, Human Error (Cambridge: Cambridge University Press, 1990).
12.
Samuel Reis-Dennis, ‘What ‘Just Culture’ Doesn’t Understand about Just Punishment’, Journal of Medical Ethics 44(11) (2018), p. 739.
13.
Cribb et al., ‘Justice’, p. 327.
14.
Robert Wachter and Peter Pronovost, ‘Balancing ‘No Blame’ with Accountability in Patient Safety’, The New England Journal of Medicine 361(14) (2009), p. 1401.
15.
Reis-Dennis, ‘Punishment’, p. 739.
16.
Wachter and Pronovost, ‘Balancing “No Blame”’, p. 14.
17.
Adam Tasker, Julia Jones and Simon Brake, ‘How Effectively has a Just Culture been Adopted? A Qualitative Study to Analyse the Attitudes and Behaviours of Clinicians and Managers to Clinical Incident Management within an NHS Hospital Trust and Identify Enablers and Barriers to Achieving a Just Culture’, BMJ Open Quality 12(1) (2023), p. 01, ![]() (accessed 10 July).
(accessed 10 July).
18.
K. Checkland, M. Marshall and S. Harrison, ‘Re-thinking Accountability: Trust versus Confidence in Medical Practice’, BMJ Quality and Safety 13(2) (2004), p. 130.
19.
Department of Health, UK, An Organisation with a Memory (London: Stationary Office, 2000).
21.
Op. cit.
23.
Sir Norman Willians, Review of Gross Negligence Manslaughter in Healthcare (London: Department of Health and Social Care, 2018).
24.
Leslie Hamilton, Independent Review of Gross Negligence Manslaughter and Culpable Homicide (London: General Medical Council, 2019).
25.
Tasker et al., ‘Just Culture’, p. 1.
26.
David Sellu v The Crown [2016] EWCA Crim 1716.
27.
Margot Brazier, Sarah Devaney, Danielle Griffiths, Alex Mullock and Hannah Quirk, ‘Improving Healthcare through the Use of ‘Medical Manslaughter’? Facts, Fears, and the Future’, Clinical Risk 22(5–6) (2016), pp. 90.
28.
30.
Cribb et al., ‘Justice’, p. 327.
31.
Cribb et al., ‘justice’, p. 327.
32.
Cribb et al., ‘Justice’, p. 327.
36.
General Medical Council (Fitness to Practice Rules) 2014.
37.
General Medical Council (Constitution of Panels, Tribunals and Investigation Committee) Rules Order of Council 2015.
39.
Op. cit.
41.
Op. cit.
42.
Op. cit.
43.
Op. cit.
44.
General Medical Council v Simon Bramhall [2021] EWHC 2109 (Admin).
46.
Op. cit.
48.
Elisabeth Mahase, ‘GMC must Focus on “Significant Breaches” only, say Doctors’, British Medical Journal 377(2022), p. 1594.
49.
Merry and Brookbanks, Errors, pp. 103–183.
50.
Merry and Brookbanks, Errors, p. 138.
51.
Michelle Robson, Jon Maskill and Warren Brookbanks, ‘Doctors Are Aggrieved–Should They Be? Gross Negligence Manslaughter and the Culpable Doctor’, The Journal of Criminal Law 84(4) (2020), p. 324.
52.
Merry and Brookbanks, Errors, p. 150.
53.
Op. cit.
54.
Op. cit., p. 389.
55.
Merry and Brookbanks, Errors, p. 108.
56.
Donaldson et al., To Err.
57.
59.
Op. cit.
60.
61.
R v Bawa-Garba (Hadiza) [2016] EWCA Crim 1841.
62.
Ash Samanta and Jo Samanta, ‘Gross Negligence Manslaughter and Doctors: Ethical Concerns Following the case of Dr Bawa-Garba’, Journal of Medical Ethics 45(2019), pp. 10-14.
63.
64.
GMC V Dr Hadiza Bawa-Garba [2018] EWHC 76 at [53].
65.
Bawa-Garba v GMC [2018] EWCA Civ 1879 at [88] and [89].
66.
GMC V Dr Hadiza Bawa-Garba [2018] EWHC 76 at [53].
67.
68.
Bawa-Garba v GMC [2018] EWCA Civ 1879 at [85].
69.
Nathan Hodson, ‘Permission without Direction: Gross Negligence Manslaughter and Erasure following Bawa-Garba’, European Journal of Health Law 26(3) (2019), p. 198.
70.
Op. cit., pp. 183–203.
71.
Op. cit., p. 190.
72.
Op. cit., p. 183.
73.
Op. cit., p. 199.
74.
76.
Op. cit., p. 50.
77.
Op. cit., p. 53.
79.
81.
[2009] EWHC 1923.
83.
Op. cit.
86.
Op. cit.
87.
Merry and Brookbanks, Errors, p. 141.
88.
90.
Op. cit., para [73].
91.
Op. cit., para [64].
92.
Op. cit., para [78].
93.
Op. cit., para [36].
94.
Op. cit., para [78].
95.
Op. cit., para [79].
96.
Op. cit., para [80].
97.
Op. cit., para [81].