
Abstract
Following COVID-19, good governance of public health is self-evidently a priority. Those who have governance responsibilities should act with integrity, and public health interventions should be both effective and ethically sound. In this context, this article focuses on the work recently undertaken by the UK National Screening Committee (NSC) in reviewing how it engages with and resolves the ethical questions raised by health screening. The article sketches the context for this review and the challenges faced; it describes the review process and the principal review outputs (including the ethical framework); and it reflects on a number of issues that are provoked by the ethical framework. Given the post-pandemic re-organisation of public health, the importance of embedding ethics in screening practice is underlined. If the United Kingdom is to be a standard-bearer for world-leading screening, it is essential that the NSC sustains its commitment to the ideals of good governance.
Introduction
For medical lawyers and bioethicists alike, it is axiomatic that humans need, and should value, good governance of health. Without good governance of clinical medicine, patients are at risk; and, without good governance of healthcare research, not only might participants be at risk, but there is also a risk that potentially beneficial treatments might not be developed. 1 However, following the COVID-19 pandemic, it is also clear that, without good governance of public health, we are all at risk: quite simply, the integrity and sustainability of the conditions that conduce to healthy populations should not be taken for granted. To the extent that public health has previously had a relatively low profile in the medical law and bioethical communities, 2 the pandemic has changed all that: the good governance of public health is now a top priority. Moreover, it is a priority both locally and globally.
That said, we should recognise that the concept and articulation of good governance is contested, 3 as is the question of how much of it is for the law and how much for bioethics. Nevertheless, in an indicative way, we suggest that, for medical lawyers as for bioethicists, the aspiration is for governance that has integrity; for fair, open, and inclusive procedures; for compliance with the ideals of legality and the Rule of Law; for interventions that are effective; and for positions and practices that are legitimate and defensible in the sense that they are compatible with the fundamental values and ethics of the community. Of course, even if we accept that good governance has this kind of scope, this is just the beginning of the conversation and contestation: each component in this aspirational list is itself open to interpretation.
Where we detect or fear shortcomings relative to these desiderata, we can expect there to be expressions of concern – as, indeed, various kinds of concern have been expressed by both lawyers 4 and ethicists 5 in relation to governance during the pandemic as well as post-pandemic. So, for lawyers and ethicists alike, the challenge now is to articulate a regime of good governance, nationally and globally, for public health – good governance not only for the exceptional circumstances of a pandemic but also for the unexceptional, but essential, public health processes and provision on which communities rely.
Arguably, within the broad field of public health, the law and ethics of publicly funded population-wide screening has been somewhat neglected. Yet, the governance of screening is potentially significant in times both unexceptional and exceptional, and in places both local and global. Moreover, governance of screening is likely to be contested. For, whatever the time and the place, there will be pressure to undertake screening programmes that promise to be in the collective interest but also pressure to give due consideration to the interests of the individuals who are to be screened. 6
Against this background, the focus of this article is on recent governance developments at the UK National Screening Committee (NSC) 7 —the NSC being responsible, inter alia, for making recommendations to the government as to the adoption and implementation of new screening programmes. In particular, the focus is on the ethical framework for screening that, following a review of its practice, the NSC has recently published. 8 The publication of this framework is not only timely but it is a significant public declaration of the NSC’s commitment to take ethics seriously; and, by specifying the principles to which its ethical reflections will be orientated, the NSC has also demonstrated its commitment to transparency and accountability for the decisions and recommendations that it makes. While the ethical framework speaks only to the NSC’s view of good governance, it is likely to be of interest to public health lawyers and ethicists internationally. Indeed, the way in which the NSC articulates its commitment to both evidence-based and ethical practice is potentially a point of reference for the screening community worldwide.
This article has four principal parts. First, we describe the context in which the UK NSC has engaged so explicitly with ethics and, implicitly, with good governance; and we also indicate the scale of the challenge faced by the NSC in articulating its guiding values and principles. This is followed, second, by a short account of the review process that led to the adoption of the framework. Third, we set out three key outputs generated by the review, namely: (1) the five organisational values to which the NSC is committed; (2) the four guiding principles that constitute the ethical framework; and (3) a process for ethical analysis. Fourth, we consider several issues that are provoked by the ethical framework – for example, questions relating to potential tensions between the principles, to the principles themselves, their interpretation and their applications, and to the resolution of disagreements on the part of committee members.
Finally, by way of introduction, we should say that, in those parts of the article that are largely descriptive, we are writing from, so to speak, an inside perspective as participants in the review and co-authors of the outputs. By contrast, in those parts of the article, including in this introduction, where we are writing more discursively and with reference to the larger picture of the governance of public health, then we are adopting a perspective that also has an external dimension. Accordingly, and in order to avoid any misunderstanding, we should make two things clear. First, in those parts of the article where we are writing as insiders, we are writing purely on our own account and not for others who were also part of the review process. Second, with regard to the discursive parts of the article, we should emphasise that the review process was not set up explicitly as an exercise in good governance and nor was it presented (or, as far as we know, perceived) in those terms. Of course, the review was undeniably an exercise in self-governance by the NSC; and it was explicitly about making the NSC’s ethical commitments more explicit; from which it follows that it was about ethical governance. Nevertheless, it would be a leap to suggest that those who undertook the review perceived it as an exercise in good governance – and, even though we will from time to time refer to good governance in the context of the review, this is not a leap that we are making.
The context and the challenge
In this part of the article, we set the scene for our description of the review process and its outputs, speaking to the context in which the UK NSC operates and then to the challenges facing a body that seeks to articulate an ethical framework for screening.
The context
The UK NSC, hosted for many years by Public Health England but now part of the Department of Health and Social Care, is not a statutory body. 9 In its role as a scientific advisory committee, the NSC advises ministers and the National Health Service (NHS) in the four UK countries about all aspects of population-wide health screening and it supports implementation of screening programmes. While some of these screening programmes relate to adult health, others relate to foetal and maternal health (including screening of the newborn).
Over the past 25 years, the UK NSC has had a profound impact on health screening in the UK, as well as being a respected international leader in this area. According to the 2021 official review of the NSC’s achievements, the NSC has ‘recommended screening programmes that have saved tens of thousands of lives, prevented huge amounts of serious illness, and helped millions of people make better informed decisions about their health’. 10 Of course, it should not be thought that the NSC does not have its critics. On one side, critics will argue that the mediation of the NSC leads to under-screening so that we fail to optimise the health benefits that we could capture by more extensive screening, 11 but, on the other side, there will be critical voices arguing that the NSC needs to be more careful about the risks of over-screening. Indeed, it was criticism from this latter side by the Nuffield Council of Bioethics (in its report on the ethics of non-invasive prenatal testing (NIPT)) that was one of the prompts for the NSC’s ethical review. 12
Given the nature of its remit, though, it is surely not surprising that the NSC has its critics. The work of the Committee is not always straightforward. For example, the NSC can be required to make recommendations in areas which are socially contested, where evidence is lacking, where the balance of benefit and risk/harm is unclear, or where there are competing and conflicting ethical approaches and positions. 13 In these cases, analysis of the scientific evidence does not provide all that is needed for the NSC to arrive at a recommendation. Furthermore, the approaching era of genomic screening as well as screening that is enabled by artificial intelligence (AI) is likely to extend the range of questions for the NSC and, at the same time, make ethically difficult issues all the more common. 14
During the last dozen years, the NSC has considered a handful of ethically problematic cases – for example, concerning the administration of antibiotics for Group B Streptococcus during the late stages of pregnancy 15 and with regard to preconception genetic testing 16 – and there has also been some reflection on the ethics of offering screening for abdominal aortic aneurysm where, following a positive screen, a small number of patients will not survive preventive surgery. 17 However, none of this was guided by a settled ethical framework for screening decisions.
Accordingly, in order to place itself in the best possible position to tackle such questions, in 2020/2021 the NSC undertook a review of how it engages with and resolves the ethical questions raised by health screening. Any recommendation that hinges on ethical considerations needs to provide a reasoned and rigorous justification for the recommendation, and a clear account of how that recommendation was made. Therefore, the review was concerned both with the ethical principles that the NSC might take into account in its consideration of health screening programmes, and with the organisational values and processes that should underpin its work.
The challenge
The challenge involved in articulating an ethical framework for public health screening should not be underestimated. We say this for at least five reasons.
First, there is no self-evident and authoritative reference point for an exercise of this kind. Of course, we have Wilson and Jungner’s classic criteria as the starting point for any principled practice of screening, 18 but we do not have a generally recognised set of ethical principles specifically designed for population screening decisions. 19 Moreover, although criterion 12 of the 20 criteria that the UK NSC applies to appraise the viability, effectiveness and appropriateness of a screening programme 20 states that programmes should be ‘ethically acceptable to health professionals and the public’, this neither gives a substantive steer nor an indication of the NSC’s own ethical principles. This is all work that remains to be done.
Second, while the ethics of public health tend to prioritise collective goods, 21 the direction of travel across the broad sweep of health ethics has been towards the rights of individuals (whether as patients or research participants or simply as ‘consumers’) and, concomitantly, towards supporting individual informed choices. 22 In some screening contexts, particularly where the screening relates to foetal and maternal health, the tension between the traditional (collectivist and utilitarian) approach to public health and the modern (patient-centred and rights-based) approach to clinical ethics is striking. 23
Third, compounding the tension highlighted by the second point, with some pressure on the NSC to extend its reach from population screening to more targeted or stratified screening, it remains to be seen whether it can sustain its traditional distinction between (public health) ‘screening’ and (clinical) ‘testing’ – and, indeed, whether the ethics that are applied to the former are also applicable to the latter.
Fourth, as we have already mentioned, we live in an era of rapid technological development, much of which has potential applications in healthcare, including screening. 24 Good governance needs to be flexible and agile in such conditions. Currently, with AI in the spotlight, there is pressure on governance to ensure that technologies are applied only in ways that are ‘human-centric’. But, how are we to understand ‘human-centricity’: is it about not harming humans, or about humans being in control, or about not de-centring humans? 25 Whatever we make of human-centricity, it will surely translate into some heavily contested red lines to be expressed and enforced by governance. So, the context in which public health screening is undertaken, and particularly the technologies available to screeners will be constantly changing, as a result of which even high-level ethical principles will need to be applied to situations that have not been contemplated. It follows that we cannot reasonably expect an ethical framework to be future-proof.
Last but by no means least, we might detect a lack of confidence, even a crisis, in the bioethics community in relation to precisely the kind of declaration of ethical principles contemplated by the NSC’s review. It is one thing to commit to transparent and inclusive processes (to good governance in a procedural sense) but it is quite another matter to run a set of substantive ethical principles up the flagpole. Strikingly, Sarah Franklin has claimed that, among bioethicists, there is a ‘sense of ethical bewilderment’; and, that ‘[b]ioethics, once a beacon of principled pathways to policy, is increasingly lost, like Simba, in a sea of thundering wildebeest’. 26 More than one diagnosis for this bioethical bewilderment might be advanced. For example, some might see the plurality of ethical approaches and theories as the problem. To the extent that bioethicists seek to stand on consensus and convergence, the plurality frustrates their methods. 27 Or, the diagnosis might be quite the opposite, namely that bioethics needs to articulate a critical vantage point from which to interrogate consensus and traditional views and the problem is that it cannot convincingly identify such a vantage point. 28 Or, again, taking a global view, the diagnosis might be that, while we recognise that bioethics has to address the line between cosmopolitan (non-negotiable) values and local ethics that are optional, we are not confident that it can do so. In other words, we are not confident that bioethics can convincingly determine which of its principles are non-negotiable (and why so) and which are optional. 29
In any event, whichever diagnosis we accept, the prognosis is not great: the challenge of articulating an ethical framework for screening that will command respect should not be underestimated.
The review process
The review was led by the authors, Professor Anne-Marie Slowther at Warwick Medical School and a subset of members of the NSC and its reference groups, which represented a broad range of expertise and experience. A series of workshops were held in 2020, where members discussed the work and experiences of other organisations with an interest in health screening or public health ethics, including the National Institute for Health and Care Excellence, Genomics England Ltd, and the Nuffield Council on Bioethics. Members also reflected upon the ethical issues that had arisen in recent screening proposals considered by the NSC, such as the introduction of NIPT in the NHS foetal anomaly screening programme. Following these discussions, proposals were developed for a set of organisational values for the NSC, an ethical framework for screening, and a process for carrying out an ethical analysis. The proposals were then tested and refined through consideration of two screening case studies.
The first case study focused on a proposal for a child–family cascade screening programme for familial hypercholesterolemia (FH), which was to be piloted through a service evaluation by NHS England and Improvement and several Academic Health Science Networks. The NSC set up an ethics task group to carry out an analysis of the ethical issues raised by the proposal, many of which apply to childhood screening programmes that involve genomic testing more broadly. These include questions about how the benefits of screening for the wider family should be taken into consideration in decisions about childhood genomic screening; and whether it is acceptable to have a significant time delay between a childhood screening test and the age of eligibility for effective interventions.
The ethics task group included people with expertise in law and ethics, medical psychology and sociology, medicine and clinical genomics, and a patient representative. The group’s discussions were informed by existing international guidance on childhood genomic screening and a series of meetings with people with a professional and personal interest in FH screening, including people with FH and parents of children with FH. The group reached a number of conclusions, including that the primary aim of screening for FH in childhood should be to confer health benefits during childhood to children with FH, and that screening ideally should take place as close as possible to the point and time at which effective interventions can be initiated in screened individuals. A report of the ethics task group’s work and findings is available on the UK NSC website. 30
The second case study considered ethical dilemmas posed by the restoration of adult screening programmes in the context of COVID-19 in early 2021. There were harms and benefits associated with different strategies. For example, increasing screening invitation rates could reduce the invitation backlog more quickly and incentivise diagnosis and treatment services to increase capacity. However, if follow-up services could not keep up, this could result in people with a positive screening result experiencing long, anxious waits for diagnosis and treatment.
At the request of Public Health England’s screening division, the NSC facilitated a discussion to explore the ethical issues using its draft ethical framework as a guide. A meeting took place in January 2021 of NSC members (including technical experts and patient and public voices), patient charities and advisors from the four countries of the United Kingdom. The issues were also discussed by the Government’s Moral and Ethical Advisory Group in February 2021. The resulting independent report included an encouragement for screening teams to be open and honest with people about potential delays in the pathway to help them to make informed choices about a screening during the restoration period. 31
These discussions helped the review team to refine and improve the ethical framework for screening. For example, in the original version, the second of the four principles focused on enabling people to make autonomous, informed decisions about screening. Considerations of a childhood screening programme for FH highlighted the need for the framework to encompass situations where screening is offered to people who are not able to make choices for themselves, and for the views of those affected to be taken into account. As a result, the second principle was broadened to cover the wider aspects of how the design and implementation of screening programmes should show respect for people.
Revised proposals for a set of organisational values for the NSC, an ethical framework for screening, and a process for ethical analysis were adopted by the NSC in June 2021. 32 These outputs of the review are summarised in the following sections.
The key outputs
Three key outputs were produced by the review process, namely: (1) the five organisational values to which the NSC is committed; (2) the four guiding principles that constitute the ethical framework; and (3) the process for ethical analysis. In this part of the article, we summarise these outputs; and, in the next part, we will look more carefully at some aspects of the ethical framework and its guiding principles.
Before we speak to these outputs, however, we should say that no particular significance was attached to designating some of the NSC’s commitments as ‘values’ and others as ‘principles’. To be sure, the organisational values are separated from the principles of the ethical framework but this simply reflects a difference in focus: whereas we can read the former as being focused on matters pertaining to the integrity of NSC members and its procedures, we can read the latter as being the guiding considerations for its recommendations and decisions. Further, although as we emphasised in our introductory remarks, the review process was not explicitly perceived or presented as an exercise in good governance, if we do take the perspective of good governance in viewing the process outputs, then it is easy to relate the values to matters of integrity and procedure and the principles to the alignment of recommendations and decisions with community values and ethics.
Organisational values
A need to articulate the values that underpin the NSC’s work was identified early in the review process. A committee that upholds and works by important organisational values can expect to receive trust and cooperation from its stakeholders or ‘customers’. This is highly important if moral or ethical judgements are to be made. Organisational values should encompass what should be expected in terms of the quality of the committee’s work, the qualities and behaviour of its constituent members, and the way it engages and communicates with others.
We found that values were already explicitly and implicitly described in the NSC’s Code of Practice, 33 and in other codes of conduct that the NSC adheres to, such as the Principles of Public Life (the ‘Nolan Principles’), the NHS Values, and the Principles for Scientific Advice to Government. From these, five broad values that are specific to the NSC were drawn (see Box 1).
UK National Screening Committee values.
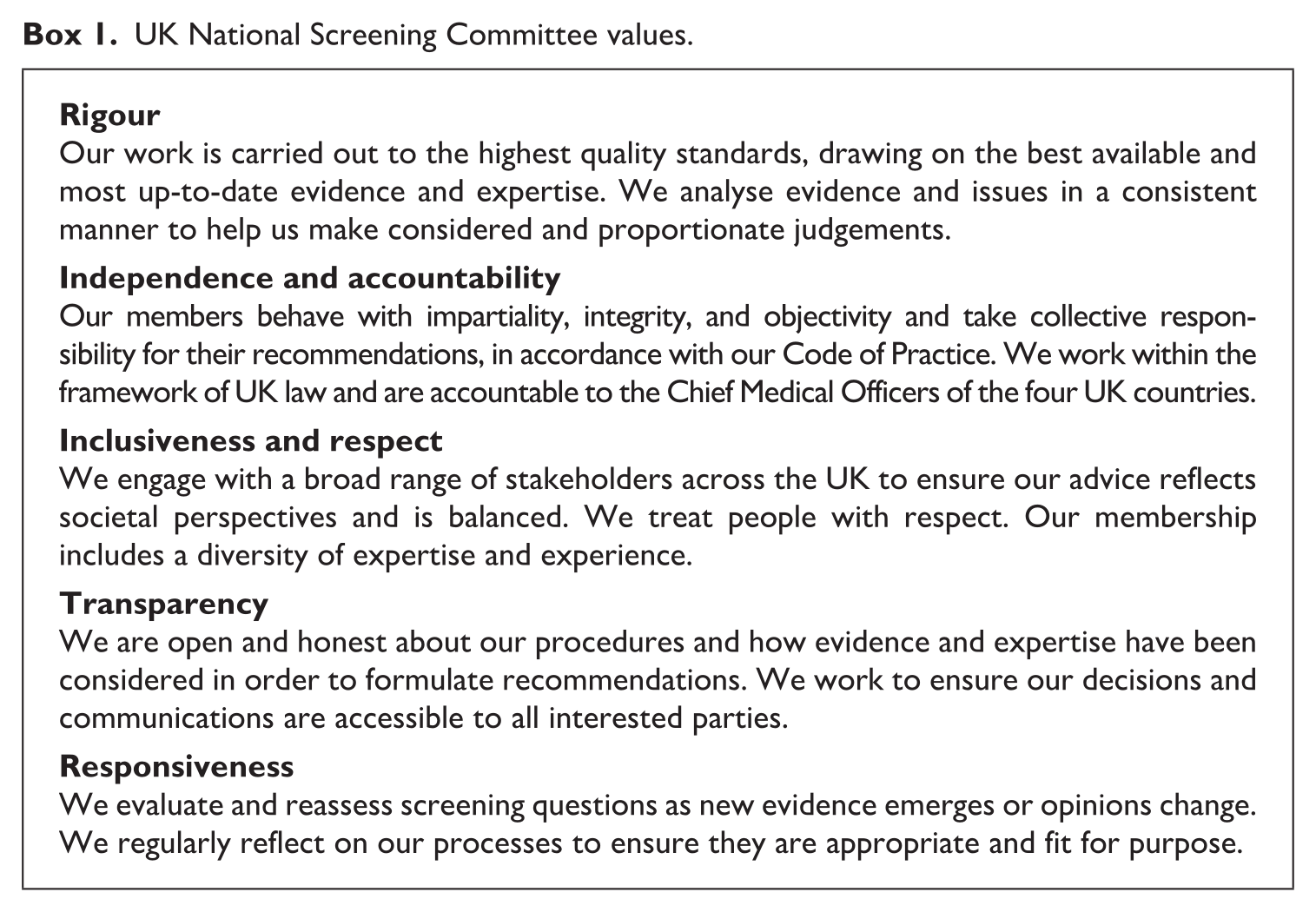
This process highlighted some areas for improvement in the way the NSC was conducting its work. For example, although all members of the NSC must declare any conflicts of interest, these were not publicly available, which might appear to be contrary to the value of transparency. A register of the financial, non-financial, and indirect interests of members of the NSC and its subgroups is now on the Gov.uk website. 34 In addition, the NSC recognised that it would be timely to review how it involves stakeholders and the public in its work to ensure it is meeting the value of inclusiveness. 35
Ethical principles
There is more than one way of characterising the overarching objective (or goal) of public health policy: at minimum, it can be expressed in terms of improving the infrastructure for the health of a population or it can be put more ambitiously in terms of improving the health and well-being of those humans who form the population. 36 The more that public health tends towards the latter, the more that its policy will invite interventions in individual lives and lifestyles. Screening lies somewhere between the minimum and the ambitiously interventionist. The availability of publicly funded screening is an essential infrastructural feature; its voluntary (opt-in) character is non-interventionist; but, there is a significant practical ‘nudge’ in the setting of targets and the normalising of screening pathways and programmes. 37 While this kind of policy is necessarily in the background, the review process sought to articulate foreground ethical principles that would always be relevant considerations that would function to constrain how and to what extent the background policy could be justifiably served by public health screening.
Four principles were identified as salient and these together form an ethical framework for screening (see Box 2). The principles are accompanied by a brief description of how they interact with each other, highlighting that they can be in tension and that the interpretation and application of the principles is a judgement that the NSC must make.
The UK NSC ethical framework for screening.
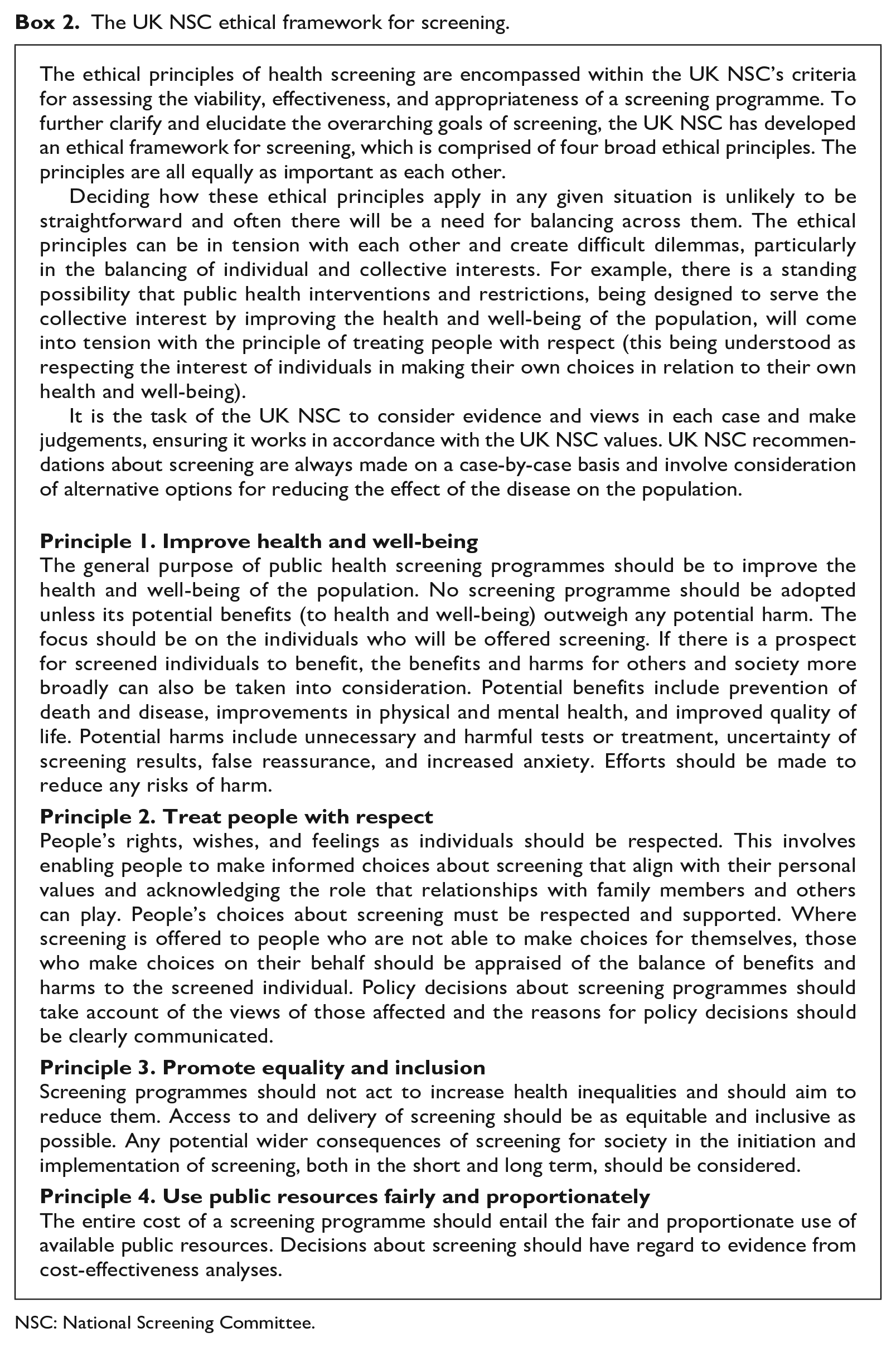
NSC: National Screening Committee.
Clearly, there is much more to be said about these four principles. As we have already indicated, in the next part of this article, we will revisit the ethical framework with a view to sharpening our understanding of the particular weight and importance of the principles, their interaction, and their application.
Ethical analysis process
While the ethical framework sets out the four principles that would guide the UK NSC in making its recommendations in response to proposals for new or modified screening programmes, it also needed a process that would enable it to examine, identify, and assess the ethical issues raised by particular screening proposals or practices. Accordingly, an ethical analysis process was developed and trialled on a case study on a child–family cascade screening programme for FH. The process sets out:
The purpose of an ethical analysis process – broadly, this is to advise the UK NSC on the ethical issues raised by a screening proposal. These should be considered alongside other factors, such as scientific evidence, economic modelling, and NHS delivery considerations.
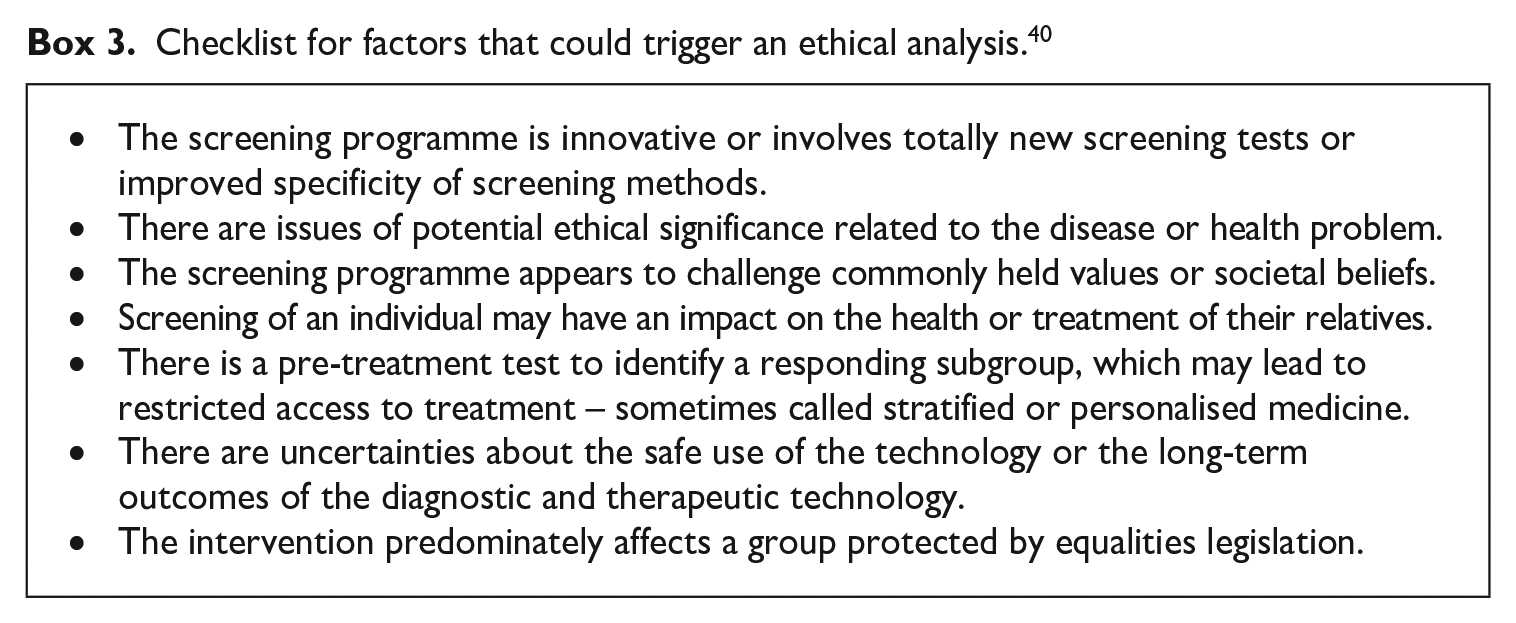
What would trigger an ethical analysis – drawing on the European Network for Health Technology Assessment ‘HTA Core Model for Screening Technologies’, 38 we created a checklist of the features of a screening proposal that could trigger an ethical analysis (see Box 3). Given the potential resource implications, only those programmes that raise significant and/or complex ethical issues would be taken forward for an ethical analysis.
At what point an ethical analysis should be undertaken – the UK NSC’s process for assessing screening proposals follows a number of steps. 39 Typically, the ethical analysis would not be undertaken during the first three steps (assessment of relevance, triage, and rapid review). In other words, it would only be at step 4, following a thorough review of the research evidence, that the ethical analysis would begin.
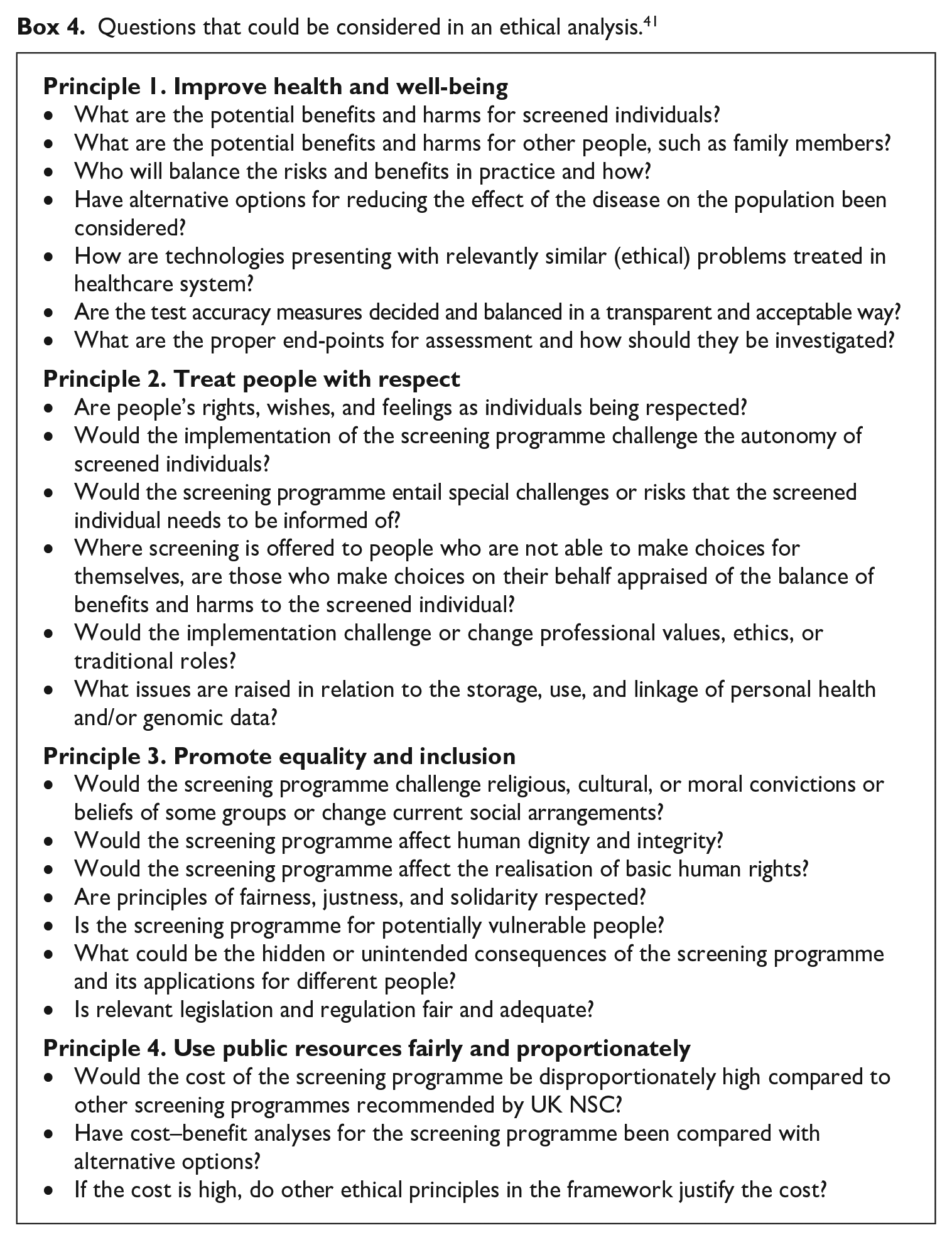
What questions would be considered in an ethical analysis – drawing again on the HTA Core Model but adapting it for the UK NSC, a list of questions was developed with reference to the four principles of the ethical framework (see Box 4). The list should be regarded as an indicative guide and not exhaustive.
What activities should be undertaken – it was recommended that a case-by-case approach be taken to deciding on the activities that should be undertaken to address the questions in hand. Options include establishing an ethics task group to oversee the process, as we did for the case study on child–family cascade screening for FH, reviews of the literature, and expert and public engagement. The kinds of questions that would be examined in an ethical analysis are likely to require stakeholder input, particularly clinical opinion and patient experience.
Checklist for factors that could trigger an ethical analysis. 40
Questions that could be considered in an ethical analysis. 41
Issues provoked by the ethical framework
The ethical framework adopted by the NSC is a reference point for the NSC itself, but it also speaks to both the general public and the screening community. Although the NSC will develop its own jurisprudence as it employs the framework case-by-case, it might also be considered for adoption by other screening groups. However, the framework is still in the nature of a work in progress and there is scope for refining our understanding of the scheme.
In this part of the article, we start by sketching the implications of the NSC recognising that its decisions and recommendations give rise to a burden of ethical justification that needs to be discharged. Then, we consider how the NSC’s framework-guided ethical reflections relate to the general public health objectives of screening; how the burden of justification might be discharged where the principles themselves, or their application or interpretation, are contested; how the NSC might resolve its differences; and how the bottom-line ethical judgement should be expressed.
Recalling our introductory remarks, while the questions that open the conversation in this part of the article reflect our insider perspective, our responses incorporate a certain amount of external reflection.
Recognising and discharging the burden of ethical justification
The exercise undertaken by the NSC recognises that screening committees bear the burden of justifying their decisions, including justifying the ethical basis of their decisions. Moreover, as we have said, the scheme identifies four principles – principles that are said to be of equal importance – to guide ethical decision-making and relative to which justificatory reasons should be offered. Nevertheless, it is not entirely clear how this burden is to be discharged relative to the proposed principles.
Borrowing from the thinking that is characteristic of the legal process of judicial review, we can say that the scheme identifies four relevant ethical principles, each of which must be given serious consideration through an ethical analysis process like the one outlined above. Having done that, the screening committee will have, so to speak, an ethical profile in relation to the proposal under consideration. The profile might be perfectly clear in showing the proposal to be ethically problematic or unproblematic, in which case the overall judgement to be made by the committee is straightforward. However, in some cases, the profile might be unclear in some respect as a result of which the judgement to be made will be less straightforward.
Nevertheless, in all cases, whether the profile is perfectly clear or much less clear, the judgement made should be one that is guided by ethical principles and that, as a result, can be legitimately put forward as being compatible with good governance. It is implicit in this, of course, that the judgement should not be irrational (in the sense that it conspicuously fails to serve public health purposes) and nor should its application of the ethical principles be wholly unreasonable (in the sense that no reasonable person could possibly so judge). This is not to say that the ethical judgement has to be such that no one dissents or that no one could reasonably disagree with it. 42 For a screening committee to discharge its burden of justification, for a judgement or recommendation to be ethically defensible, it is enough that the Committee has been guided by the right considerations (the four principles), that it has not taken into account irrelevant considerations, and that the decision is neither irrational nor wholly unreasonable.
Put in these terms, the scheme leaves plenty of room for screening committees to exercise their discretion in making their ethical judgements. In an attempt to further clarify how the scheme might be operationalised, we can speak to four questions, namely: how the general public health objectives of screening relate to the four ethical principles, how screening committees should proceed where the application of one of the principles is unclear or contested, how committees might resolve their differences, and how committees should frame or express the outcome of their ethical deliberations.
How do the general public health objectives of screening relate to the four ethical principles?
Given that the general purpose of screening and screening committees – unlike, say, committees whose raison d’être is to promote equality or to ensure value for money and efficiency – is to improve the conditions for, or the actual level of, public health, it is tempting to think that, in practice, the first ethical principle (improve health and well-being) will assume more importance than the other principles. However, this is not necessarily so. While the fact that screening is designed to improve public health will surely shape background thinking around what would be a sound and justifiable recommendation, it does not follow that the first principle will be more important than the other principles in the specifically ethical part of the process.
To clarify our thinking about the strength of the principles and the tensions between them, we can start with clear cases before considering more challenging hypotheticals, and then a possible two-stage approach. While we assume a degree of flexibility in handling the tensions that might arise between the principles, we also assume that the commitment to this framework entails that each of the principles is taken seriously.
Clear cases
To start with the clearest of cases, let us suppose that a screening committee judges that a particular proposal clearly fails all four of the ethical principles. In other words, it judges that: (P1) the proposed screening would clearly cause more harm than benefit; (P2) it would clearly fail to respect persons; (P3) it would clearly fail to promote equality and inclusiveness; and (P4) it would clearly not be fair or proportionate to commit the level of resource required. While this is an easy case, and the ethical profile is clear, it does not tell us whether the failure under P1 was more or less important than the failure in relation to the other principles.
Conversely, let us suppose that a screening committee judges that a particular proposal clearly satisfies all four of the ethical principles. In other words, it judges that: (P1) the proposed screening would clearly produce more benefit than harm; (P2) it would clearly respect persons; (P3) it would clearly promote equality and inclusiveness; and (P4) it would clearly be fair and proportionate to commit the level of resource required. Again, this is an easy case, a straightforward profile, but it does not tell us whether passing muster relative to P1 was more or less important than satisfying the other principles.
Hypothetical scenarios
A more promising test case would be if a proposal satisfies P1 but fails to pass muster relative to the other principles; or, conversely, if a proposal fails to pass muster relative to P1 but satisfies the other principles. In either case, if the decision were to follow the indication given by P1, the contraindications given by the other principles notwithstanding, then this would suggest that P1 is indeed more important than the other principles. However, we need to look more carefully at these hypothetical scenarios.
The former scenario is that a positive recommendation is made for the screening proposal on the basis that it satisfies P1 and notwithstanding that it does not satisfy the other principles. This certainly suggests that P1 is the dominant principle but the scenario lacks plausibility if we allow that an ethics committee could so easily override a finding that P2 is violated (e.g. if it could dispense with the requirement that submission to screening should be free and informed). After all, for many ethics committees, it would be axiomatic that persons should be treated with respect. 43 This simply does not comport with the commitment to take each of the principles seriously.
That said, an ethics committee might want to operate with a proviso for emergencies or other exceptional cases. If so, and to make this scenario plausible, we have to assume that the net benefit under P1 is so great or so responsive to the urgent need, or something of this kind, that the committee is prepared to override other principles to which it is committed. In other words, we have to assume that the context is one of grave emergency or catastrophe. On this analysis, it would be correct to say that, in ‘ordinary’ circumstances, the four principles are treated as being of equal importance but that, in ‘extraordinary’ circumstances, P1 is dominant where screening would be hugely beneficial. 44
Turning the scenario around, we are asked to imagine a negative recommendation being made where a screening proposal fails to satisfy P1 (showing net harm) despite the proposal passing muster relative to the other principles. But, without qualification, this would mean that if, say, P3 has no weight against P1, then attempts to level up access to screening (or to redistribute resources under P4) could be vetoed by P1. Again, if an ethics committee is to honour its commitment to take each of the principles seriously, we have to suppose that the context for the decision is exceptional and that the facts fall within a proviso that the committee believes it can in good faith apply.
A two-stage approach
In our hypothetical scenarios, we have imagined all four principles being on the table, and the committee being presented with a tension between P1 and one or more of the other three principles. Allowing that P1, having being balanced against the other principles, inclines the committee towards a positive or negative recommendation as the case might be is one thing; but, for P1 to operate as a kind of override, we have suggested that a special case proviso needs to be recognised. However, there might be another way of structuring the principles and processing any tensions that might arise between P1 and the other principles.
Many years ago, Mary Warnock suggested that we should assess the ethics of new biotechnologies (particularly genetics) in two stages. 45 In the first stage, the question would be whether a technology promised to produce a net benefit over harm. If the judgement was that no such benefit would be produced, then it would not be ethical to proceed. However, if the judgement was that there would be such a benefit, then the assessment should move to a second stage. At the second stage, the question would be whether, the promised benefit notwithstanding, considerations of human rights and human decency indicated that it would be unethical to proceed. In other words, at the second stage, we should ask whether ‘even if the benefits of the practice seem to outweigh the dangers, it nevertheless so outrages our sense of justice or of rights or of human decency that it should be prohibited whatever the advantages’. 46 Applying this approach, the considerations identified as relevant at the second stage would operate as constraints that would qualify and limit the pursuit of benefit.
Now, if a screening committee were to understand the relationship between the principles in this two-stage way, it might treat P1 as the guiding standard at the first stage and then P2, P3, and P4 as the relevant considerations and constraints at the second stage. On this basis, so the argument would go, each of the four principles would be taken seriously. What should we make of this?
If P1 is satisfied at the first stage, a positive recommendation is indicated. However, Warnock’s main point is that we might decide at the second stage, and by reference to counter-principles, that it would be unethical to proceed. Applying this to the ethical framework means that, where P1 prima face indicates a positive recommendation, we might still end up with a negative recommendation because of the counter-considerations relative to P2, P3, and P4. Here, although the initial question is whether P1 is satisfied, serious and potentially determinative weight is attached to the other principles. That is fine.
If, however, P1 is not satisfied, matters are a bit less clear. If a failure to satisfy P1 is conclusive, then the other principles are not taken into consideration and this simply will not do – or, at any rate, it will not do unless this is an extraordinary case that engages a special case proviso. So, to keep faith with its commitment to take each of the principles seriously, the committee should treat the negative recommendation indicated by P1 as no more than prima facie. Even where P1 is not satisfied, there has to be a second stage discussion and the possibility that the final decision, all principles considered, will be for a positive recommendation.
How should screening committees proceed where the application of one of the principles is unclear or contested?
Thus far, we have been looking at cases where the ethical profile is relatively unproblematic. To be sure, some of these cases suggest a tension between the principles (between, say, P1 and one or more of the other principles) but at least the bearing of each principle is clear. However, there might be cases where it is not clear whether one or more of the principles is satisfied.
Consider, for example, the proposal for an FH ‘service evaluation’ to which we have already referred. 47 Here, parents taking their 12-month-old children to the clinic for their routine immunisation visit would also be offered an FH screening test for the child. When the UK NSC’s ethics task group considered this proposal, one question was whether the proposed screen was designed to be of benefit to the child, the child’s parents, or the wider family. In the event of a positive screen, and employing a reverse cascade, there could be several beneficiaries. But, applying the first principle, would it matter if the child did not benefit but the child’s parents or members of the family (who, unlike the young child, could be prescribed statins) did benefit? According to P1, screening should be designed to improve (and have the effect of improving) the health and well-being of the population, the focus should be on the individual who is screened, and benefits for others can also be taken into account. This is open to interpretation. However, the ethics task group took the view that this principle should be read as requiring that there should be benefit to the child being screened. 48 Moreover, if we refer to the second principle, which underlines the importance of treating people with respect, this reading of the first principle seems to be reinforced.
At all events, having read the first principle this way, a critical question now becomes whether screening the child could be for its benefit. Putting aside the question of whether it would be beneficial to screen when the overwhelmingly likely outcome would be a negative result, how would the child benefit when the screen was positive? Because the child would not be prescribed statins until some years later, the treatment would be largely dietary in nature. Whether or not dietary regimes and a raised awareness in the family of the need for a healthy lifestyle actually are of benefit to the child is, currently, hard to say. When the NSC reviewed the evidence on FH screening in childhood in 2019/2020, it found limited evidence of long-term benefits. 49 FH families have compelling stories to tell about how well children have fared with dietary regimes and about how much support they have received, but healthcare professionals have worrying stories to tell about the harmful effects of this kind of intervention. Accordingly, the ethical profile for this proposal has a large question mark alongside the first principle. We simply do not know whether in general, let alone in any particular case, FH screening for young children would be of more benefit than harm to the child (including the possible harm that parents might be put off bringing their child into the clinic for the routine immunisation visit). 50
Another example of the uncertain application of a principle, this time the second principle, has been encountered in relation to the use of NIPT in the screening pathway for pregnant women, in particular, for the identification of babies with Down’s syndrome. There are several ethical dimensions to this development 51 but, relative to the NSC’s ethical framework, the headline question concerns the tension between the second principle (treating pregnant women with respect by enabling them to make informed choices) and the third principle (taking an inclusive approach specifically by being sensitive to the interests of people with Down’s syndrome and the concerns of their families). Beyond this headline question, however, there is a further question about how and when NIPT is to be offered to pregnant women. This concerns a choice between a two-stage recall approach and a one-stage ‘reflex’ approach, where a blood sample is taken at the same time as the first screen and automatically sent for NIPT analysis if the first screen indicates a higher chance result. To state the matter shortly, it is arguable that the former is superior to the latter in enabling women to make an informed choice about using NIPT, but, for the former to deliver on its promise, it does require a significant investment of resources (allowing for a consultation and conversation specifically about the benefits and risks associated with NIPT). 52 Faced with this particular uncertainty, the NSC recommended that the recall approach should be piloted and evaluated, and this is now underway.
This example of uncertainty, and the NSC’s response, takes us to two other questions. One is the question of how, in practice, an ethics committee should proceed where the application of the framework or particular principles is problematic in the ways just indicated; but, first, what if it is the framework principles themselves that are challenged?
Rejection of the framework principles
We should not expect all members of an ethics committee to arrive at the same conclusion. Members might reasonably disagree about the interpretation or balancing of the principles, or about the relevance and significance of the evidence that they have, and so on. However, what if a member disagrees with the principles themselves? In other words, what if a member rejects the principles that constitute the ethical framework?
In principle, a member of a screening committee might argue that the recognised ethical framework does not highlight the right principles. For example, it might be argued that, say, human dignity or solidarity or vulnerability should be explicitly highlighted and directly considered. No doubt, such an argument merits serious consideration, but, as we indicated in our discussion of the challenges facing the review, there is no easy way of resolving this kind of dispute. 53
In this scenario, the NSC having set out its stall, now finds itself challenged in the most fundamental of terms. Does the onus of justification lie on the NSC or the challenger? And what is the burden of justification? In the current state of bioethics, it seems unlikely that either the NSC or the challenger can come up with an argument that shows that it would be wholly unreasonable (or incoherent) to come up with any other ethical principles than the ones adopted or proposed. Arguably, to find such an apodictic demonstration, we have to drill all the way down to the generic conditions that make it possible for humans to exist on planet Earth, to form communities, to develop their capacity for agency, and to debate ethics and good governance. 54 Because these conditions are generic, they are neutral between the rival ethical views that are characteristic of particular communities and, thus, unhelpful to protagonists of particular ethical principles. 55 Moreover, the requirement that all humans should respect the generic conditions entails only that ethical governance should be compatible with those conditions, and it does not rule out the possibility that more than one scheme of good governance might meet this compatibility test.
If the protagonists do not drill down this deep but limit their arguments to their own particular communities, then the dispute is likely to centre on whether the NSC’s or the challenger’s principles fit most convincingly with the plurality of principles espoused by some reference group (whether the screening community, the public health community, the larger community, the community of right-thinking persons, and so on). Unless the principles that the NSC has adopted are so obviously unreasonable relative to these reference groups, the challenger should give way.
This is not to say that the ethical framework should never be reviewed and revised. Far from it. But, we do not think it is appropriate for a screening committee charged with applying an agreed ethical framework to revise the framework on the hoof. Arguments of this fundamental kind need to be conducted elsewhere and, for our purposes, we can focus on those cases where the differences between committee members concern the interpretation or application of the published framework principles.
Disagreements as to the interpretation or application of the framework principles
We can consider now how the NSC might proceed where differences arise among members who do accept the framework principles but who disagree about their interpretation or application. Even by limiting our discussion in this way, we can anticipate occasions when members will have different views about the appropriate ethical judgement to be made. Where the difference lies within the range of tolerance, where members agree that it is reasonable for others to have a difference of opinion, there should be no need for any further action; the majority view will prevail. However, what about those occasions where the differences go deeper and where the minority is not prepared to yield to the majority? We imagine that these will be rare occasions, but anticipating this possibility the NSC has provisionally agreed on a process by which such differences might be resolved (see Box 5).
Summary of the process for working through disagreements between UK NSC members.
NSC: National Screening Committee.
This process, it will be noted, does not attempt to suppress differences, and it is not about avoiding the expression of differences. Indeed, although it aspires to arrive at a consensus, it is not just about finding common ground; differences need to be squarely confronted. It is imperative that all voices are given equal consideration. Of course, this does not guarantee that the committee will be able to arrive unanimously at a particular view and, where divisions remain, the process recognises that a majority decision will prevail. 56
How should screening committees frame the outcome of their ethical deliberations?
In principle, if we ask a committee to assess the ethics of a screening proposal, we might expect that the overall judgement to be returned will be that the proposal is (1) ethically required, (2) ethically prohibited, or (3) ethically permitted. In practice, the question might be put to the ethics committee in a way that requires a ‘yes’ or ‘no’ answer – for example, the question might be ‘Would it be unethical to proceed with this proposal [which otherwise meets all the screening criteria]?’ or perhaps ‘Is there any reason, ethically speaking, to have reservations about making a positive recommendation in relation to this proposal?’ Nevertheless, it should be possible to translate the ethical profile into an overall judgement to the effect that the proposal should be rejected as ethically prohibited or recommended as ethically required or ethically permitted.
Where the ethical profile is straightforward, then translation also seems straightforward. If the profile is entirely unproblematic, the judgement must be that a positive recommendation is at least ethically permitted and even ethically required; and, conversely, if the profile is comprehensively problematic, then the judgement must be that a positive recommendation is ethically prohibited.
Where, however, the ethical profile is not straightforward, the committee’s own process for resolving disputed applications and interpretations of the framework principles might enable it to make a decisive overall judgement. That said, a more nuanced judgement might be more appropriate. For example, there might need to be a proviso attached to an overall judgement that a positive recommendation is ethically permitted. In such a case, what the proviso might flag up is that the implementation of the programme (e.g. whether to implement NIPT by adopting a recall or a reflex approach) should be attentive to the ethical principles; and this might indicate that a pilot or an evaluation (such as that undertaken with NIPT) might be the practical (and fully ethical) way forward.
As with all the questions of further refinement, screening committees will need to learn from their experience of using the ethical framework.
Conclusion
To return to where we started, it bears repeating that the good governance of public health is a priority; and, in our view, no matter how evidence-based and effective governance might be, it cannot be good governance unless ethics is taken seriously. Moreover, with the shake-up of public health following COVID-19, this is the perfect opportunity to show that all the governance lessons have been taken.
Among the post-COVID changes, the UK NSC, having previously been a part of Public Health England, is itself undergoing a considerable overhaul. The Committee will retain its name but it has a new home in the Office for Health Improvement and Disparities (OHID) in the Department of Health and Social Care. 57 According to a recent statement, the remit of the Committee will be extended to include targeted screening for high-risk groups, stratified screening that is more tailored to the individual, and (as at present) average-risk population screening. The Committee will have closer links with research bodies and guideline-making organisations such as the National Institute for Health and Care Excellence (NICE) and Scottish Intercollegiate Guidelines Network (SIGN). 58 Clearly, this is a significant re-organisation and rebooting of the UK NSC; and, at a time when new tools and techniques for screening will present new opportunities but also ethical challenges, it is a space to watch.
The UK NSC has taken the bold, and possibly unique, step of defining and describing the ethical principles that guide its deliberations and recommendations, and it has started to apply them explicitly to specific screening questions. Although we cannot see any obvious reason why the principles should not apply to the wider range of screening programmes that will now fall within the NSC’s new remit, this will need testing. Embedding ethics in future processes and recommendations will be important because, while the NSC needs to have credibility with the scientific community, 59 it also needs to earn the trust and confidence of patients and the general public. World-leading science is necessary but not sufficient for world-leading screening; if the United Kingdom is to be a standard-bearer for the good governance of public health, both its screening decisions and its practice need to be guided by world-leading ethics.
Footnotes
Acknowledgements
In addition to the authors, the staff and members of the UK NSC and its reference groups who contributed to the development of the UK NSC’s ethical framework for screening include Natalie Armstrong, Felicity Boardman, Sunil Bhanot, Louise Bryant, Eleanor Cozens, David Elliman, Jane Fisher, Sharon Hillier, Anne Mackie, John Marshall, Maggie Powell, Anne-Marie Slowther, Bob Steele, and Cristina Visintin. The members of the ethics task group for child–family screening for familial hypercholesterolemia included Roger Brownsword (Chair), Sunil Bhanot, Louise Bryant, Angus Clarke, Sharon Hillier, Katherine Robertson, Graham Shortland, and Anne-Marie Slowther. We would also like to thank the many people who attended stakeholder meetings during the process and reviewed drafts of the output materials.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
1.
See, for example, R. Brownsword, ‘Regulating Automated Healthcare and Research Technologies: First Do No Harm (to the Commons)’ in Graeme Laurie, Edward Dove, Agomoni Ganguli-Mitra, Catriona McMillan, Emily Posten, Nayha Sethi, and Annie Sorbie, eds., The Cambridge Handbook of Health Research Regulation (Cambridge: Cambridge University Press, 2021), p. 266.
2.
That said, public health law and ethics have not been totally overlooked. See, for example, R. Brownsword, ‘Public Health, Private Right: Constitution and Common Law’, Medical Law International 7 (2006), p. 201; A. M. Viens, J. Coggon, and A. S. Kessel, eds., Criminal Law, Philosophy and Public Health Practice (Cambridge: Cambridge University Press, 2013); J. Coggon, K. Syrett, and A. M. Viens, Public Health Law: Ethics, Governance and Regulation (Abingdon: Routledge, 2017); and L. O. Gostin and L. F. Wiley, Public Health Law, 3rd ed. (Oakland: University of California Press, 2016).
3.
See, for example, H. Addink, Good Governance (Oxford: Oxford University Press, 2019). According to Addink, ‘the rule of law, democracy, and good governance are the cornerstones of the modern state’ (p. 3). Precisely, how these cornerstones relate to one another is unclear. Moreover, given the multitude of lists of governance desiderata that have been issued, it is not clear what we should treat as the essence of good governance. Nevertheless, Addink suggests that the following six general principles can be taken to represent the ideal of good governance: properness, transparency, participation, effectiveness, accountability, and human rights. This is not the end of things because, on closer analysis, each of these principles is an umbrella for a number of more specific sub-principles. We should also note Council of Europe, 12 Principles of Good Democratic Governance (2008) (available at ![]() ).
).
4.
See, for example, J. Sumption, Law in a Time of Crisis (London: Profile Books, 2021), pp. 228 and 233; S. Fowles, Overruled (London: Oneworld Publications, 2022), pp. 102–103; and L. O. Gostin, Global Health Security: A Blueprint for the Future (Cambridge, MA: Harvard University Press, 2021), esp. pp. 155–157 and 222–223, arguing that the WHO needs to re-establish its legitimacy and leadership role in developing robust, transparent, and coordinated governance of global health security.
5.
See, for example, the insistence by the European Group on Ethics in Science and New Technologies that ‘The public health emergency must not be abused to usurp power, or to permanently suspend the protection of rights and liberties’ (Recommendation 4 of its ‘Statement on European Solidarity and the Protection of Fundamental Rights in the COVID-19 Pandemic’ (April 2, 2020), p. 4. Available at ![]() (accessed 24 August 2023). Compare, too, for the tip of an iceberg, M. M. Mello and C. J. Wang, ‘Ethics and Governance for Digital Disease Surveillance’, Science 368(6494) (2020), pp. 951–954; V. L. Raposo, ‘Big Brother Knows That You Are Infected: Wearable Devices to Track Potential COVID-19 Infections’, Law, Innovation and Technology 13 (2021), p. 422; and B. A. Kamphorst, M. F. Verweij, and J. A. W. van Zeben, ‘On the Voluntariness of Public Health Apps: A European Case Study on Digital Contact Tracing’, Law, Innovation and Technology 15 (2023), p. 107.
(accessed 24 August 2023). Compare, too, for the tip of an iceberg, M. M. Mello and C. J. Wang, ‘Ethics and Governance for Digital Disease Surveillance’, Science 368(6494) (2020), pp. 951–954; V. L. Raposo, ‘Big Brother Knows That You Are Infected: Wearable Devices to Track Potential COVID-19 Infections’, Law, Innovation and Technology 13 (2021), p. 422; and B. A. Kamphorst, M. F. Verweij, and J. A. W. van Zeben, ‘On the Voluntariness of Public Health Apps: A European Case Study on Digital Contact Tracing’, Law, Innovation and Technology 15 (2023), p. 107.
6.
Compare A. Raffle, A. Mackie, and J. A. M. Gray, Screening: Evidence and Practice, 2nd ed. (Oxford: Oxford University Press, 2019). In his Foreword to the book, at v, Bob Steele (who, at the time, was Chair of the UK National Screening Committee) says of the ethical challenge that ‘it is easy to see screening from two viewpoints, and although it is vital for systematic screening programmes to benefit the population, we must not lose sight of the fact that the end-users are individuals, and their rights to making informed decisions are just as relevant to screening as they are to the treatment of established disease’.
8.
9.
10.
11.
See, for example, D. S. Wald and A. C. Martin, ‘Decision to Reject Screening for Familial Hypercholestrolaemia Is Flawed’, Archive of Diseases in Childhood 106 (2021), p. 525 (leading to a response by some members of the NSC: see, J. Marshall, G. Shortland, S. Hillier, R. Brownsword, and B. Steele, ‘Response to “Decision to Reject Screening for Familial Hypercholestrolaemia Is Flawed” by Wald and Martin’, Archive of Diseases in Childhood 107 (2021), p. 102; and then to a further comment by Wald and Martin at DOI: 10.1136/archdischild-2021-322934).
12.
See, for example, Nuffield Council on Bioethics, Non-Invasive Prenatal Testing: Ethical Issues (London: Nuffield Council on Bioethics, 2017).
13.
As we indicated in our introductory remarks, there is always a potential tension between positions that reflect the collective interest (broadly speaking utilitarian in nature) and positions that are more protective of individual rights. For some particular examples, see the next paragraph in the text and 5.3 below.
14.
Compare (albeit with regard to clinical and research practice rather than screening) R. Brownsword, ‘New Genetic Tests, New Research Findings: Do Patients and Participants Have a Right to Know—and Do They Have a Right Not to Know?’ Law, Innovation and Technology 8 (2016), p. 247.
16.
See Human Genetics Commission, Increasing Options, Informing Choice: A Report on Preconception Genetic Testing and Screening (London, 2011). Notice, this concerned preconception genetic testing, not population wide screening.
17.
See R. Brownsword and J. Earnshaw, ‘Controversy: The Ethics of Screening for Abdominal Aortic Aneurysm’, Journal of Medical Ethics 36(12), p. 827, (2010).
18.
J. M. G. Wilson and G. Jungner, Principles and Practice of Screening for Disease (Geneva: WHO, 1968). The sixth of Wilson and Jungner’s criteria requires that the test should be ‘acceptable to the population’.
19.
For a helpful attempt to synthesise ‘emerging screening criteria proposed over the past 40 years’, see A. Andermann, I. Blancquaert, S. Beauchamp, and V. Déry, ‘Revisiting Wilson and Jungner in the Genomic Age: A Review of Screening Criteria Over the Past 40 Years’, Bulletin of the World Health Organization 86(4), p. 317, (2008). Three conspicuously ethical considerations are included in the criteria, namely, that the programme ‘should ensure informed choice, confidentiality and respect for autonomy’; that it ‘should promote equity and access to screening for the entire target population’; and that ‘the overall benefits of screening should outweigh the harm’ (all at 318).
20.
21.
See, for example, the Nuffield Council on Bioethics, Public Health: Ethical Issues (London: Nuffield Council on Bioethics, 2007) in which the emphasis is on the ‘stewardship’ of the infrastructure for public health; and, T. Baldwin, R. Brownsword, and H. Schmidt, ‘Stewardship, Paternalism and Public Health: Further Thoughts’, Public Health Ethics 1(2), p. 113, (2009).
22.
See, for example, Andermann et al., ‘Revisiting Wilson and Jungner in the Genomic Age’, (n. 19) at 318 where, speaking of the emerging criteria, the authors note that several ‘reflect broader trends that have shaped both Western medicine and society more generally over the past generation (e.g. increased consumerism, the shift away from paternalism towards informed choice, a focus on evidence-based health care, and the rise of managed care models that emphasize cost-effectiveness, quality assurance, and accountability of decision-makers)’. In the British jurisprudence, this is perhaps most clearly signalled by the decision of the UK Supreme Court in Montgomery v Lanarkshire Health Board [2015] UKSC 11. On which, see R. Brownsword and J. Wale, ‘The Right to Know and the Right Not to Know Revisited’, Asian Bioethics Review 9 (2017), pp. 3–18.
23.
See, further, for example, R. Brownsword, Technology, Governance and Respect for the Law: Pictures at an Exhibition (Abingdon: Routledge, 2023), Ch 9, esp. 77–82 and 91–93.
24.
See, for example, R. Brownsword, ‘Regulating Patient Safety: Is It Time for a Technological Response?’ Law, Innovation and Technology 6 (2014), p. 1, and Brownsword, ‘Regulating Automated Healthcare and Research Technologies: First Do No Harm (to the Commons)’ (n 1).
25.
Compare R. Brownsword, Rethinking Law, Regulation and Technology (Cheltenham: Elgar, 2022), and R. Brownsword, Technology, Humans, and Discontent with Law: The Quest for Better Governance (Abingdon: Routledge, 2023), Ch. 34; and F. Pasquale, New Laws of Robotics (Cambridge, MA: The Belknap Press, 2020). At a global level, we should also note the WHO’s Guidance in World Health Organization, Ethics and Governance of Artificial Intelligence for Health (Geneva: 2021), available at ![]() . While this guidance is about health in general rather than public health in particular, and while within public health it is not specifically about screening, the six ethical principles that are the centrepiece of the report (at 23-30) are of interest. These principles concern the protection of human autonomy; the promotion of human well-being, safety, and the public interest; ensuring transparency, explainability, and intelligibility; fostering responsibility and accountability; ensuring inclusiveness and equity; and promoting AI that is responsive and sustainable. Analysing the possible readings, tensions, and accommodations of these principles, and how they relate to the ethical framework developed by the NSC, would be an exercise for article in its own right. Suffice it to say that, as a first move in comparing these WHO principles to the four principles of the NSC, we should probably set aside those WHO principles that are AI-specific. This would leave us with the protection of human autonomy; the promotion of human well-being, safety, and the public interest; and ensuring inclusiveness and equity.
. While this guidance is about health in general rather than public health in particular, and while within public health it is not specifically about screening, the six ethical principles that are the centrepiece of the report (at 23-30) are of interest. These principles concern the protection of human autonomy; the promotion of human well-being, safety, and the public interest; ensuring transparency, explainability, and intelligibility; fostering responsibility and accountability; ensuring inclusiveness and equity; and promoting AI that is responsive and sustainable. Analysing the possible readings, tensions, and accommodations of these principles, and how they relate to the ethical framework developed by the NSC, would be an exercise for article in its own right. Suffice it to say that, as a first move in comparing these WHO principles to the four principles of the NSC, we should probably set aside those WHO principles that are AI-specific. This would leave us with the protection of human autonomy; the promotion of human well-being, safety, and the public interest; and ensuring inclusiveness and equity.
26.
S. Franklin, ‘Ethical Research―The Long and Bumpy Road From Shirked to Shared’ Nature 574 (2019), pp. 627–630, DOI: 10.1038/d41586-019-03270-4.
27.
See, for example, R. Brownsword, ‘Bioethics Today, Bioethics Tomorrow: Stem Cell Research and the “Dignitarian Alliance”’, University of Notre Dame Journal of Law, Ethics and Public Policy 17 (2003), p. 15, and R. Brownsword, ‘Stem Cells and Cloning: Where the Regulatory Consensus Fails’, New England Law Review 39 (2005), p. 535.
28.
See, for example, Brownsword, Technology, Governance and Respect for the Law: Pictures at an Exhibition (n 23) Ch. 9, and R. Brownsword, ‘“Just Doing Bioethics”: Policy, Principle and Process’ in Erick Valdes and Juan Alberto Lecaros, eds., Handbook of Bioethical Decisions: Volume 2 (Cham: Springer, 2022) Ch. 20. For an important recent defence of an Archimedean vantage point for bioethics, see S. D. Pattinson, Law at the Frontiers of Biomedicine (Oxford: Hart, 2023).
29.
See, for example, R. Brownsword, ‘Migrants, State Responsibilities, and Human Dignity’, Ratio Juris 34 (2021), p. 6.
30.
31.
35.
36.
See, for example, R. Brownsword, ‘Public Health, Private Right and the Common Law’, Public Health 120 (2006), p. 42; and R. Brownsword, ‘Criminal Law, Regulatory Frameworks and Public Health’ in A. M. Viens, J. Coggon, and A. S. Kessel, eds., Criminal Law, Philosophy and Public Health Practice (Cambridge: Cambridge University Press, 2013), p. 19.
37.
Seminally on ‘nudging’, see R. H. Thaler and C. R. Sunstein, Nudge (London: Penguin, 2009); and, for critical assessment in relation to public health, see R. Brownsword, ‘Public Health Interventions: Liberal Limits and Stewardship Responsibilities’, Public Health Ethics (2013), p. 235 (special issue on NY City’s public health programme), DOI: 10.1093/phe/pht030.
38.
40.
41.
42.
On the bandwidth of reasonableness, scope for reasonable disagreement, and unreasonableness, see Brownsword, Technology, Humans, and Discontent with Law, (n 25) Ch. 15–19.
43.
Compare the criteria proposed by Andermann et al. (n 19) and their remarks concerning ‘the shift away from paternalism towards informed choice’ (n. 22). See, too, S. John and J. Wu, ‘“First, Do No Harm?” Non-Maleficence, Population Health and the Ethics of Risk’ Social Theory and Practice 48 (2022), p. 525.
44.
Compare R. Brownsword and J. Wale, ‘In Ordinary Times, In Extraordinary Times: Consent, Newborn Screening, Genetics and Pandemics’, BioDiritto 1(Sp) (, p. 2021)129.
45.
M. Warnock, ‘Philosophy and Ethics’ in C. Cookson, G. Nowak, and D. Thierbach, eds., Genetic Engineering—The New Challenge (Munich: European Patent Office, 1993), p. 67.
46.
Ibid., at p. 67.
47.
See, p. 9 above.
48.
49.
50.
In the end, the evidence presented to the ethics group did not allay its concerns that this risk could be discounted.
51.
See Nuffield Council on Bioethics (n 12); and R. Brownsword and J. Wale, ‘Testing Times Ahead: Non-Invasive Prenatal Testing and the Kind of Community that We Want to Be’, Modern Law Review 81(4) (2018) p. 646.
52.
See, further, J. Wale, ‘Packaging Prenatal Tests and Information for Pregnant Women: Enhancement or Dilution of Informational Interests?’ in M. Borghi and R. Brownsword, eds., Law, Regulation and Governance in the Information Society (Abingdon: Routledge, 2023), p. 181.
53.
See, pp. 8–9 above.
54.
See, for example, R. Brownsword, Law, Technology and Society (Abingdon: Routledge, 2019), R. Brownsword, Law 3.0 (Abingdon: Routledge, 2020) (for the ‘triple licence’), and R. Brownsword, ‘Informational Wrongs and Our Deepest Interests’ in M. Borghi and R. Brownsword, eds., Law, Regulation and Governance in the Information Society (Abingdon: Routledge, 2023), p. 199.
55.
56.
Compare Council of Europe, 12 Principles of Good Democratic Governance (n. 3). In the first of the Council’s principles, which is on ‘Participation, Representation, the Fair Conduct of Elections’, the participatory elements are elaborated in the following five points: ► Citizens are at the centre of public activity and they are involved in clearly defined ways in public life at local level. ► All men and women can have a voice in decision-making, either directly or through legitimate intermediate bodies that represent their interests. Such broad participation is built on the freedoms of expression, assembly and association. ► All voices, including those of the less privileged and most vulnerable, are heard and taken into account in decision-making, including over the allocation of resources. ► There is always an honest attempt to mediate between various legitimate interests and to reach a broad consensus on what is in the best interest of the whole community and on how this can be achieved. ► Decisions are taken according to the will of the many, while the rights and legitimate interests of the few are respected.
58.
59.
As we have already remarked (see text at ns 11 and 12), the NSC is not without its critics.