
Abstract
The law on healthcare decision-making in Ireland is in a period of transition and will be enhanced with the full commencement of the Assisted Decision-Making (Capacity) Act (ADMC Act) 2015. The legislation is intended to empower a person to make decisions relating to their healthcare and personal affairs where they lack or may in the future lack the capacity to make their own decisions. This is especially relevant for the older person in terms of planning for future healthcare decisions. This article reports on quantitative and qualitative research which examined the exercise of autonomy by the older person in Ireland in the context of healthcare decision-making. The research compared the lived experience of healthcare decision-making with the existing legal and policy framework. The research sought to identify what is currently understood about the ADMC Act and awareness of the changes it will bring about in decision-making for the older person. These data assist in identifying strengths, such as a feeling of involvement, and weaknesses, such as an asymmetry of information, in the operation of the current decision-making framework while also identifying potential hurdles to the meaningful implementation of the 2015 Act.
Introduction
The 2016 Census indicated that the population of Ireland has continued to grow older since the 1980s with 637,567 people older than 65 years. 1 This is a 19.1% increase since 2011. 2 The Health Service Executive 3 and government departments 4 forecast the continuation of this demographic change over the coming years. While such figures represent a societal success in healthcare provision, they also raise challenges relating to the health and care of the older person. Older persons tend to account for a greater number of interactions with healthcare professionals. 5 This may in part be explained by the prevalence of chronic disease, a doubling of obesity levels, as well as steps taken to facilitate greater access to General Practitioners in Ireland. 6 This underlines the need to ensure that the rights of the older person are effectively recognised and protected across law, policy, and practice. 7
The experience of healthcare can be daunting, and this is perhaps especially true for the older person. 8 To improve the experience, healthcare services increasingly adopt a person-centred care approach. Key elements of this are service user involvement and health literacy which necessitate clear communication, informed consent, and respect for an individual’s autonomy. In this way, service users are placed at the centre of healthcare delivery. The Health Information and Quality Authority (HIQA) 9 has emphasized the human rights dimension of person-centred care 10 while also recognizing that healthcare and social care practitioners and organizations have found it challenging to ‘translate human rights principles into day-to-day practice and service delivery’. 11 This article details quantitative and qualitative research which examined how the exercise of autonomy in practice is facilitated for the older person in Ireland. The combination of these methods allowed for certain themes to be explored and drawn out in greater detail. Such analysis is significant, given the limited empirical research in Ireland at this juncture. The research examined the experience of contemporaneous decision-making and engagement with advance care planning. As part of this, the empirical research gauged perceptions on the exercise of autonomy, identified aspects of healthcare decision-making which raise the greatest concern for the older person, and assessed whether there is a lack of understanding surrounding certain aspects of the legal framework for healthcare decision-making.
The empirical research occurred at a point of transition in the Irish legal framework for healthcare decision-making. The article is therefore presented against the background of the current legal and policy framework while also examining the changes that will accompany the full commencement of the Assisted Decision-Making (Capacity) Act (ADMC Act) 2015. 12 As of September 2021, the majority of this legislation remains to be commenced. The article is divided into four main sections. The first section outlines the law and policy on autonomy and decision-making. The second and third sections address research methodology and research findings, while the fourth section discusses key themes. By considering this evolving framework, the article draws attention to constraints on the exercise of autonomy, including an asymmetry of information (between the healthcare professional and the older person) which can restrict the scope of self-determination and which may pose a significant challenge to achieving the aims of the ADMC Act 2015.
Autonomy and the older person
Autonomy is a fundamental concept for healthcare decision-making in liberal democracies. The term ‘autonomy’ is derived from the Greek words ‘autos’ and ‘nomos’ meaning self-rule or law; originally describing the self-government of Greek city-states, over time it has come to represent the will and preferences of the individual. 13 Under the liberal conception of autonomy, as associated with JS Mill, an individual’s autonomy is to be respected due to the benefits which it can bring about for the individual and society alike. 14 Individual benefits for the older person in exercising autonomy may include an increase in the quality of life, 15 as well as improved health and well-being. 16 In this respect, the World Health Organization has expressly recognized the importance of ‘optimizing opportunities for health, participation and security in order to enhance the quality of life as people age’. 17
The right to autonomy has strong foundations in law and is recognized and protected in common law, the European Convention on Human Rights, 18 the Charter of Fundamental Rights, 19 the Irish Constitution, 20 and legislation. 21 The legal endorsement of autonomy allows for reliance on and enforcement of ethical principles in individual situations. 22 This may involve relying on negative or positive rights as provided for by the liberal interpretation of autonomy. Such rights are reflected in the principles of non-interference and in the requirement for consent to an intervention.
A person must therefore provide informed consent before a treatment can be administered. Such consent is to be based on the healthcare professional having informed the person of the risks, benefits, and any alternatives so that the person can weigh up the information and arrive at an informed decision. 23 This reflects a person-centred approach to the information required in respect of a decision. 24 The provision of sufficient information and the involvement of the person is an essential aspect of treatment and, from a legal perspective, is not to be dispensed with because the person is considered to be in a vulnerable condition. 25 A person’s age should not restrict or limit their involvement. Nonetheless Barken has observed that ‘[w]ithin youth-oriented Western cultures, older people are often disadvantaged by age relations and are the frequent targets of ageism (i.e. discrimination on the basis of age).’ 26
Under Irish law, there is a presumption that an adult patient has the capacity to make a healthcare decision. 27 If there is a concern as to whether a person has the capacity to make a particular healthcare decision, this is to be determined on a functional basis, namely, whether the person can comprehend and retain the treatment information, believe the information, and weigh it up in arriving at a decision at that time. 28 If a person is deemed to lack the capacity to consent or refuse a particular treatment, then the decision is to be made in the person’s best interests. 29 Best interests seek to balance a number of potentially competing interests, including best clinical interests, the person’s wishes and preferences, and their beliefs and values. 30 Therefore, if a person has particular views about future treatment in the event of a potential loss of capacity, advance care planning may be an appropriate way to protect their autonomy.
Advance care planning
The options for advance care planning have however traditionally been somewhat limited in Ireland. For example, under the Powers of Attorney Act 1996, while it is possible to create a power of attorney over personal care decisions such as where the donor would live and with whom, it is not possible to create a power of attorney that will cover healthcare decisions. An advance healthcare directive is therefore currently the only formal mechanism for ensuring a person’s input in future healthcare decisions. After a period of tenuous recognition of advance healthcare directives,
31
the decision of Baker J in Governor of X Prison v McD (P)
32
brought legal clarity to the issue. Baker J in McD (P) stated, I consider that as a matter of law . . . a person may make a freely stated wish in regard to their future care and that this ought to be, and can in an appropriate case be, respected by those with care of that person.
33
While the judicial recognition of advance care directives brought welcome legal clarity, it did not provide detail as to the formalities that may be required to ensure the validity and applicability of a directive. This is provided for in the ADMC Act 2015, however, these are among the provisions yet to be commenced.
Assisted Decision-Making (Capacity) Act 2015
The ADMC Act 2015 was enacted on 30 December 2015. The genesis of the legislation can be traced back to the 2006 Law Reform Commission (LRC) Report on Vulnerable Adults and the Law. 34 The Report followed on from the LRC Consultation Papers on Law and the Elderly, 35 and Vulnerable Adults and the Law: Capacity. 36 A key catalyst for the introduction of the 2015 Act was the need to support Ireland’s compliance with obligations established under the UN Convention on the Rights of Persons with Disabilities (CRPD). 37 Article 3 of the CRPD requires States to respect the ‘inherent dignity, individual autonomy including the freedom to make one's own choices, and independence of persons’. 38 The CRPD also recognizes the equal right to legal capacity for all persons with disabilities 39 and requires States to ‘take appropriate measures to provide access by persons with disabilities to the support they may require in exercising their legal capacity’. 40 The ADMC Act is a step towards delivering on these obligations. 41
The stated aim of the ADMC Act 2015 is ‘to provide a modern statutory framework that supports decision-making by adults and enables them to retain the greatest amount of autonomy possible in situations where they lack or may shortly lack capacity’. 42 It aims to do this both through creating a set of principles that govern decision-making and by the creation of decision-making supports. These supports include the possibility of appointing a decision-making assistant or a co-decision-maker. The functions of a decision-making assistant include obtaining information and supporting the person to make and express a decision, while the role of a co-decision-maker involves making the decision jointly with the appointer. The structure of these supports is grounded in the socially embedded and interdependent nature of the individual. In circumstances where a person’s capacity is or may shortly be in question, the Act, therefore, provides a framework for support that can empower a person in their healthcare decision-making. Yet, the effective functioning of these supports requires a person to have close social contacts, as well as a willingness to openly discuss matters relating to their healthcare. These points are not easily resolved, as the empirical research demonstrates.
The ADMC Act 2015 also provides for the court appointment of a decision-making representative in circumstances where a person lacks capacity. As part of this process, the court is to have regard for the terms of any advance healthcare directive or enduring power of attorney made by the relevant person. Moreover, there is a preference towards appointing a decision-making representative who has a close relationship with the person. 43 This familiarity would assist in the performance of functions, as the decision-making representative is to ascertain the will and preferences of the relevant person and assist them in communicating these. 44 The scope of the decision-making representative’s authority is framed by the court order as well as general restrictions under the Act. This includes a restriction on authorizing the refusal of life-sustaining treatment. Donnelly and O’Keefe note that ‘[t]his leaves open the question of how such decisions should be made. . . . judicial clarification regarding when and whether an application to court is required would be helpful’. 45
The ADMC Act 2015 also re-affirms the common law presumption of capacity, 46 codifies the functional test for capacity, 47 and sets out a number of guiding principles to be followed in decision-making. 48 The nine guiding principles are intended to apply in situations where anyone is interacting with a person who has difficulties with their decision-making capacity. 49 It is notable that the Act does not use the term ‘best interests’ but instead establishes a requirement to give effect to a person’s will and preferences. This shift in perspective has since been reflected in case law 50 and statutory instruments. 51 It is not, however, possible to fully appreciate the significance of this change until the Act is applied in practice.
The Act provides for reform of the Ward of Court or adult guardianship system, 52 extends powers of attorney to healthcare decisions, and defines the formalities that must be complied with in drafting an advance healthcare directive. 53 The circumstances in which an advance healthcare directive will be applicable are quite specific. Provided the formalities are satisfied, a directive that refuses treatment is to be complied with if ‘at the time in question the directive-maker lacks capacity to give consent to the treatment’; ‘the treatment to be refused is clearly identified in the directive’; 54 and ‘the circumstances in which the refusal of treatment is intended to apply is clearly identified in the directive’. 55 The directive is not applicable to the refusal of life-sustaining treatment unless the directive-maker expressly states this to be the case. 56 It is notable that in addition to a refusal of treatment, the Act also recognizes the possibility that a person may request a specific treatment. Although such a request is not legally binding it is to be taken into consideration during a relevant decision-making process. 57 This process may also be shaped by the appointment, under the advance healthcare directive, of a designated healthcare representative who has the power to ensure that the terms of the directive are adhered to. 58 The directive-maker may confer on the designated healthcare representative the power to advise and interpret the appointer’s will and preferences regarding treatment and/or ‘the power to consent to or refuse treatment, up to and including life-sustaining treatment, based on the known will and preferences of the directive-maker’ as determined by the representative by reference to the directive. 59 This underlines the significance of discussions on advance care planning so there can be congruence between a person’s will and preferences and the medical treatment provided. 60 While there are a range of benefits associated with engaging in advance care planning, 61 there are considerable challenges and barriers which prevent people from effectively engaging in the process. Examples of both internal and external barriers to advance care planning were identified in the empirical research and will be discussed later in this article.
At the time of writing (September 2021), the Act is only partially commenced and codes of practice to guide the application of the legislation are being drafted. 62 Lawyers and healthcare professionals have, however, been conscious of this legislation for in excess of five years. As a result of this long lead-in time, the Act has come to occupy a rather unusual position in Irish law. Although not fully commenced, the Act is referenced in professional codes of conduct, healthcare standards, and guidance documents. Principles within the Act appear to have filtered through to practice without the formal step of commencement having occurred.
Embedding patient autonomy in professional standards and healthcare policy
In addition to legislation and jurisprudence, healthcare professionals are guided by professional codes of conduct, health service policies, and national standards. The abstract nature of the rights contained in the legal framework comes to be reflected and embedded in everyday practice and interactions between healthcare professionals and the older person through these policies and standards. It follows that the manner in which the older person experiences and participates in their medical care and treatment can draw out strengths and weaknesses in the relationship between clinical practice and the law, particularly in the context of healthcare decision-making.
Guidance on healthcare decision-making is set out by the Health Service Executive (HSE) 63 in the ‘National Consent Policy’. 64 The principles contained in the policy are intended to apply to ‘all interventions conducted by or on behalf of the HSE on service users in all locations’. 65 It includes sections on valid and genuine consent, ensuring consent is voluntary, and the assessment of capacity. Standards and guidance on autonomy in healthcare have also been produced by the Health Information and Quality Authority (HIQA). 66 This is an independent authority that has the aim of promoting the quality and safety of care for people using healthcare and social care services in Ireland. 67 Of relevance for the care of the older person in a residential care setting are the ‘National Standards for Residential Care Settings for Older People in Ireland’. 68 The standards were first published in March 2009 and revised in 2016. More recently, the HIQA has sought to bridge the divide between the high-level reference to human rights in such standards and the need to guide staff in the practical implementation of human rights. This is demonstrated by the publication of ‘Guidance on a Human Rights-based Approach to Health and Social Care Services’. 69 Significantly, this guidance document explicitly recognizes the relationship between a human rights-based approach, person-centred care, and support for the purpose of promoting autonomy. 70
Professional standards and codes of conduct are issued by the Irish Medical Council,
71
the Nursing and Midwifery Board of Ireland,
72
and CORU (the statutory regulator for healthcare and social care professionals).
73
The professional standards address the contemporaneous exercise of autonomy and extend to forms of advance care planning.
74
For instance, the Irish Medical Council, ‘Guide to Professional Conduct and Ethics’ includes a section on advance healthcare plans or directives.
75
In this section, it provides that: Sometimes patients want to make plans for their medical treatment which will come into effect if they lose capacity in the future. Plans may include advance refusals of medical treatment or requests for specific procedures. You should do your best to help and support patients who ask for your assistance in writing an advance healthcare plan. You should ask patients with long-term conditions likely to result in their death or mental incapacity in the foreseeable future, if they have made an advance healthcare plan or directive.
76
The obligation of the doctor to enquire as to whether patients with long-term conditions have made advance care plans is effectively part of the management of an existing long-term condition, where the person has some experience of the condition and is therefore better able to make an informed choice on their future care. The tentative nature of the guidance offered outside a long-term condition reflects that advance care planning can be a complex process for both doctor and patient. 77
Research methodology
This article reports on two research studies that examined the experience of healthcare decision-making for the older person in Ireland. The first study relied on quantitative research methods, namely, a self-administered questionnaire. 78 The research was undertaken as part of a funded collaborative project between the researcher and Age Action Ireland. Age Action is an independent national organization for ageing and older people. 79 The research was shaped by three core objectives:
To explore the older person’s understanding of autonomy in healthcare, familiarity with decision-making practices, and awareness of forthcoming decision-making supports.
To identify the priorities, concerns, and needs of the older person around this topic.
To identify any shortcomings between the legal framework and the subjective experience of research participants.
The questionnaire was comprised of 25 questions, set out across four sections addressing ‘demographic and social information’, ‘standard of health’, ‘consent to medical treatment’, and ‘advance care planning’.
Participants were primarily recruited through the network of Age Action but non-members could also participate in the research. Data collection took place between July 2019 and September 2019. In total, 283 respondents completed the questionnaire. Quantitative data were analysed to produce descriptive and bivariate results. Thematic analysis was used to gain insight into patterns of meaning across the 112 open-ended responses that were submitted. Thematic analysis was drawn on due to its ‘accessibility and its flexibility’. 80 The application of this method involved a combination of inductive and deductive approaches to data analysis.
Age Action also acted as a partner in the second research study. 81 Participatory dialogues (or focus groups) were used to explore two areas of interest. First, the qualitative research captured perspectives on a proposed home care scheme. However, these data are not included here due to the focus of this article. Second, the research examined the older person’s involvement in healthcare decision-making, thoughts on advance care planning, and awareness of the changes that will accompany the full commencement of the ADMC Act 2015. Questions linked to healthcare decision-making were directly informed by the earlier quantitative research. The data from this study are therefore primarily drawn upon in order to expand on points raised by the quantitative research.
Five focus groups were held in four locations in Ireland and took place during October and November 2019. The medium of focus group not only permitted dialogue between the researcher and the participants but also between the participants themselves thereby yielding additional data. 82 Each focus group session was no longer than two hours and was broken into smaller segments to allow for comfort breaks. Groups were composed of between 5 and 10 participants with a total of 30 persons participating. Through the use of open-ended questions, participants were encouraged to share their own experience and opinion.
The principal limitation of the research is that respondents in both the quantitative and the qualitative research represented a highly educated and relatively healthy cohort of older people. As a result, their ability to exercise their autonomy in healthcare decision-making was likely to be more robust than for the majority of older people in Ireland. However, the research findings may serve to underline particularly intransigent issues surrounding healthcare decision-making which need to be addressed.
Research findings
Overview
In the quantitative study, data were collected on the perceived involvement in healthcare decision-making, the last interaction with a healthcare professional, discussion of end-of-life care, and knowledge of advance care planning. A majority of the respondents, 74.91%, felt they were involved in making decisions about their medical treatment. This is a high response and may be influenced by subjective conceptions of what involvement means, as was subsequently evidenced by the qualitative study. Over half of the respondents had not discussed their wishes for end-of-life care with anyone. In situations where a discussion had taken place, it was suggested that these tended to be brief and not especially detailed. A failure to grasp the nettle of healthcare planning was again illustrated by responses to questions on advance healthcare directives. Participants demonstrated low levels of awareness and knowledge of advance healthcare directives. It follows that the responses also indicated a low level of awareness of the ADMC Act 2015.
All participants in the qualitative research reported being as involved as they wanted to be with regard to their current healthcare decision-making. Views varied with regard to the level of involvement that participants wanted, with some participants happier to rely on the advice of their general practitioners (GPs), while others wanted to take full responsibility for decisions. The qualitative research also demonstrated a low awareness among participants of how decisions are made if a person is not in a position to do so themselves. Most if not all participants incorrectly believed their next-of-kin had the authority to make decisions for them in the event of potential incapacity. ‘Next-of-kin’ typically refers to a person’s closest relative or the person to be contacted in an emergency. It is important to note that next-of-kin cannot give or refuse consent on behalf of an adult patient or have access to a person’s medical information unless they have the specific legal authority to do so. Despite this, the status of next-of-kin is often misunderstood. There was also misunderstanding in respect of planning for the future and what, for instance, a power of attorney covered and how it differed from an advance healthcare directive. Of the participants who were aware of the ADMC Act 2015, few felt that they understood how it would affect them.
Demographic, social and health information
The quantitative study captured data on demographic, social, and health information. In all, 38.3% of respondents were more than 80 years old, 21.28% were in the 75–79 year grouping, while 20.92% of respondents were aged between 70 and 74 years. A little over two-thirds of respondents identified as female. 83 The response group was highly educated as just under half of the respondents indicated that they had completed some form of third level education. 84 Secondary school was the highest level of education for 40.21% of respondents. 85 By way of contrast, in the general population 18.9% of persons aged 65 and above possess a third-level qualification. 86 Among the respondents, 53.71% indicated that they live alone, 37.46% live with a partner or spouse, 5.30% live with a family member, and 1.06% are in long-term residential care.
The quantitative study also explored engagement with healthcare services. 94.7% of respondents attended a healthcare professional for a health-related problem at some point in the previous year. In all, 28.21% of respondents indicated that they had been in hospital in the previous 12 months. When asked whether they are being treated for a chronic health problem, 51.09% answered in the positive. This figure is low when compared with broader population data and suggests that this data set represents a relatively healthy population. 87 It follows that over 70% of respondents categorized their standard of health as ‘excellent’ or ‘good’. Just 7.09% considered their health to be poor. The combination of these factors must be taken into account when considering subsequent responses. 88 On this point, Donnelly et al. stated, ‘[d]ecision making becomes more complex for older people with multiple health and care needs as the capacity to self-manage is affected by the cumulative effect of long-term conditions’. 89 It might therefore be expected that a healthier cohort would be better placed to manage and make decisions relating to their healthcare.
The qualitative study did not record data on demographic, social, and health information.
Involvement in decision-making
Section three of the quantitative research inquired about respondents’ involvement in medical treatment and multiple questions were posed about the respondent’s last interaction with a healthcare professional. Responses were generally positive as 74.91% felt involved, 22.91% were of the opinion that they were somewhat involved, and 2.18% did not feel involved in making decisions about their medical treatment. Persons who had completed some form of third-level education, persons who had discussed their wishes for end-of-life care, and persons who completed an advance healthcare directive were shown to report a high level of involvement in such decisions. 90 These are respondents who are actively engaging in a range of healthcare decisions so it is not surprising that these respondents would feel involved.
Persons who did not feel involved in decision-making were asked to consider the reason(s) for their lack of involvement. The question was not applicable to a majority of respondents. However, 8.92% of respondents indicated that they were not provided with the opportunity; 1.88% were perceived not to have capacity by others; 1.41% did not wish to participate; and 4.23% identified communication difficulties as the barrier to their involvement. In all, 3.76% of respondents indicated another reason for their lack of involvement. From these responses, issues of timing, communication, and a sense of paternalism in healthcare emerged: Not given sufficient time for in-depth discussion. Some health grades dictate that no one question their decisions. Medical team knows what should be done – when lying in a bed with others listening there is no time to ask questions and probably not as alert due to worry.
Nonetheless, respondents viewed involvement as being especially important and noted that people should not be distanced from their care.
The subject should always be listened to and their wishes taken seriously, not discounted, ignored or overridden. Patients should be fully involved in their healthcare decision making for best outcomes. Patients should have choices of care if they wish.
Involvement in healthcare decision-making was also identified as a key theme emerging from the focus groups. These participants reported being as involved as they wished to be in their healthcare; that is to say, those who wanted to make their own healthcare decisions were fully supported in so doing. For others, they wished to trust the expertise of the healthcare professional in making the decision: I would be happy with the GP, I always say, I used to be a mechanic and if you brought your car to me, I’ll fix it. So I reckon the GP knows all my cogs and bits and pieces and so he’s the expert and so what he decides is right.
Some respondents however recognized the active role of the healthcare professional in promoting and facilitating autonomy: The chap I go to, he would get you involved, you’d make the decision yourself. He’d offer alternatives; you’d say what you wanted.
A common theme among the participants in the focus group was that GPs who were perceived as being younger or more recently qualified were more likely to encourage people to take responsibility for their own healthcare decisions. This is demonstrated by the comments of one of the focus group participants: The younger doctor coming out is asking questions as well into the bargain and I found at one stage I was being grilled. And I went home that night and I thought about it and I said crikey he’s right. And I honestly believe that my own wellbeing has improved as well into the bargain, I don’t mind a bit. As well but if there’s something niggling at me now I’ll go and get it looked after, I wouldn’t before.
Respondents in the quantitative study were next presented with a multi-part question that asked them to reflect on their last interaction with a healthcare professional regarding medical treatment. The questions were directly shaped by the HSE National Consent Policy and sought to draw out the various elements in the patient–healthcare professional interaction such as listening to the patient, providing sufficient information, and allowing sufficient time to consider and process the information provided; all of which are necessary elements in facilitating a person’s autonomy. The questions and responses are listed in the table below.
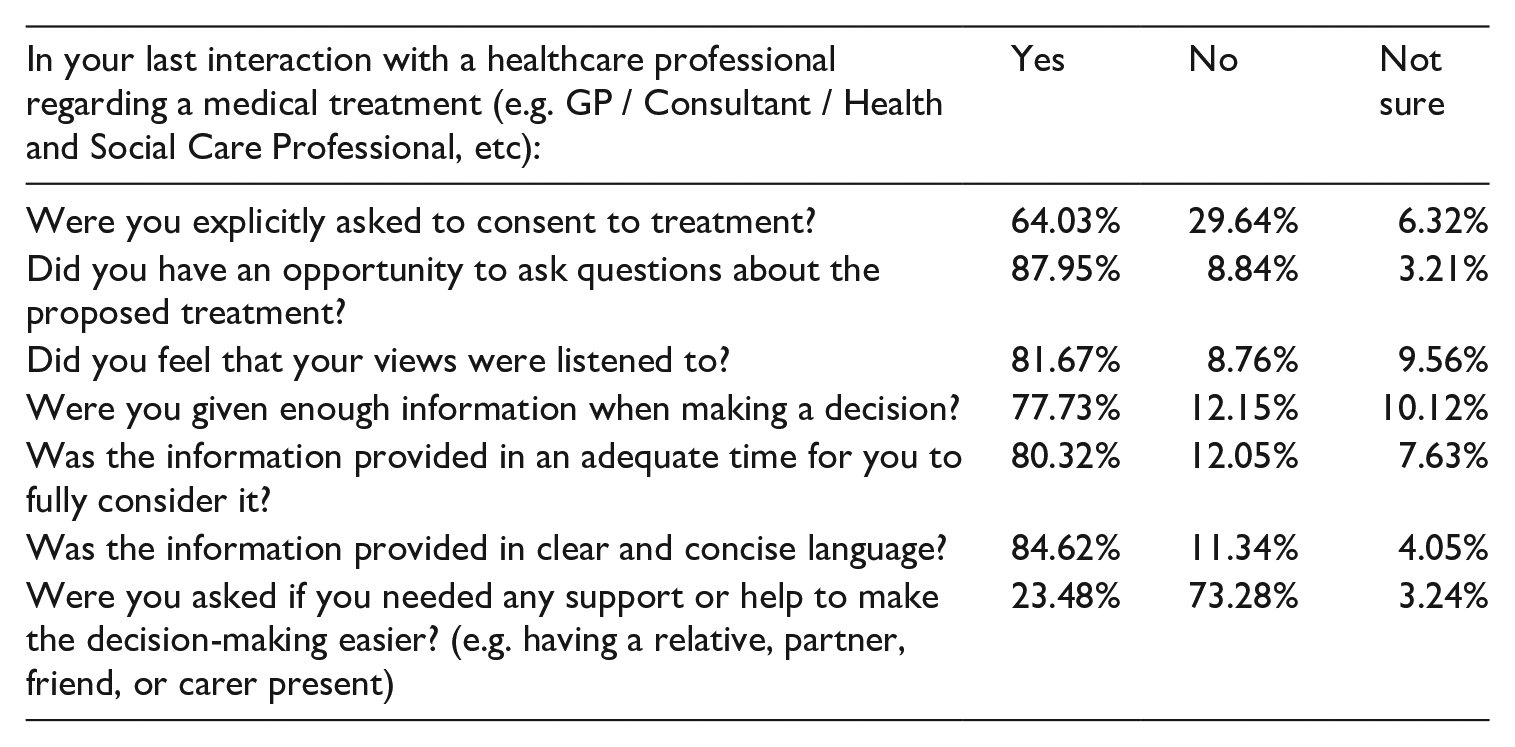
The responses to this series of questions suggest that the consent process is being adhered to in a majority of interactions, although the seeking of explicit consent appears to occur less often as demonstrated by the 29.64% negative response. While it is good practice to secure explicit consent, it may be that implied consent is being relied on in many instances.
The response to the final question relating to decision-making support can be teased out in further detail. Overall, 23.48% of respondents indicated that support was offered. The response to this question varied depending on whether the respondent was male or female. In all, 37.5% of male respondents were offered support or help but this only applied to 16.7% of female respondents. Additional research and attention to this are required particularly as the ADMC Act 2015 provides for a number of decision-making support roles. If such supports are not made available on an equal basis, then it could limit the impact of the legislation.
Advance care planning
The area of advance care planning will be re-shaped with the full commencement of the ADMC Act 2015. The research therefore sought to gauge awareness of the legislation, the extent of discussions about end-of-life care, the knowledge of advance healthcare directives, and the respondent’s thoughts on advance care planning.
The quantitative research indicated that 18.8% of respondents were aware of the ADMC Act 2015. 91 Given the characteristics of this respondent group, a lower level of awareness might be expected among the general population. 92 It could be suggested that if a person is unaware of the legislation, it may be that they are also unaware of the various advance decision-making options that are provided for under the new Act.
Research participants in the quantitative study were asked whether they had discussed their wishes for end-of-life care with someone. The majority of respondents, 54.78%, had not discussed their wishes with anyone. This lack of discussion can create problems for future healthcare decisions and may lead to a second-guessing of a person’s thoughts and preferences. Respondents who had discussed their wishes for end-of-life care most commonly engaged with a family member 39.34%. In all, 18.01% of respondents spoke with a solicitor 93 and 4.41% spoke with their general practitioner. The level of discussion with solicitors is particularly high and several respondents indicated that they had spoken with their solicitor about drafting a will. Although estate planning is undoubtedly important, the focus on this issue may be indicative of some uncertainty about what a discussion on end-of-life care might entail. Respondents indicated that when a discussion had taken place, these tended to be brief and had not explored their wishes and preferences in detail. There was a notable difference in response between people who live alone and those living with a partner or spouse. While 50% of respondents who live alone had not discussed their wishes for end-of-life care, the figure for persons living with a partner or spouse rose to 65.35%. It may be the case that people assume that their partner or spouse will inevitably know what care and treatment they would want and would be in a position to shape those healthcare decisions should they themselves lack capacity.
A subsequent question asked respondents whether their GP should raise the issue of advance care planning with them. Despite 4.41% of respondents speaking with their GP about end-of-life care, over half of the respondents wanted their GP to raise the issue of advance care planning with them. 94 This question prompted a relatively high, 35.47%, don’t know response. Based on the key themes arising in the quantitative and qualitative research, it may be that the ‘don’t know’ response was in part motivated by a lack of information. This information may relate to the appropriate timing of such a conversation, what it might entail, and what purpose it would serve. 95 In the absence of such details, the respondent could not be expected to independently raise questions about end-of-life care or advance care planning.
The focus groups revealed that where persons had engaged in some form of advance planning, there was still a deal of confusion over what exactly had been planned for. Of the participants who had created a power of attorney, all who expressed an opinion incorrectly believed that this legal instrument applied to all healthcare decisions. Other participants thought they had signed a Do Not Resuscitate order with their solicitor. Some people were familiar with an advance healthcare directive (or living will as they expressed it) but less clear on what that involved or how it might be created, and in what way it differed from an enduring power of attorney. These points were also reflected in the quantitative study where 60.53% of respondents did not know what an advance healthcare directive is, and 17.29% were not sure. Yet, 8.15% of respondents indicated that they had completed an advance healthcare directive. This is not wholly positive as subsequent comments suggest that some respondents may have instead completed a power of attorney and not an advance healthcare directive. If people are to engage in appropriate advance care planning it appears that much more information is required.
Open-ended comments on advance healthcare directives in the quantitative study related to effectiveness, practical steps, and the relationship with an enduring power of attorney. On the matter of effectiveness and applicability, the presence of an advocate was viewed as essential: Later down it is very difficult to know if your opinions will be carried through if you are not able to stand up for yourself. Advance care directive depends on who is looking after your affairs and has an interest in seeing that you are cared for properly.
This quote echoes the concern identified by Bramley et al. who noted that in the context of advance care planning, ‘[t]he experience of loss of autonomy and self-determined choice left participants questioning whether ACP would actually have any influence on their care’.
96
In Ireland, this concern may, in part, be addressed by the option of appointing a designated healthcare representative as provided for under Section 87 of the ADMC Act 2015.
97
Greater information may therefore encourage more engagement with advance care planning and could reduce some of the confusion surrounding legal instruments in this area: I would certainly consider completing such a directive but would need a lot more information in order to reach an informed decision. It would be helpful if a practitioner discussed the above. Also, I am confused about Enduring Power of Attorney. Have to be continuously pro-active in my own health care. If an advanced healthcare directive is an enduring power of attorney – yes I have done that.
The facilitation of advance care planning has the potential to better define and clarify a person’s will and preferences. In turn, this can support the designated healthcare representative in performing their duties thereby reducing the potential for divergence between perceived and actual will and preferences.
Desire for greater information and support
The theme of information more generally arose at several points in the open-ended responses to the survey. This included a desire for more open communication with healthcare professionals as well as opportunities to ask questions about the information provided: I think if your doctor knows the information they should discuss when it being obvious that a patient needs it.
Responses also set out that the information should be provided in a way which is clear and understandable. In effect, it should not be communicated using clinical terms but should be in terms that can be readily understood by the older person: Should be all in plain English, not a series of medical jargon. Make sure information provided is clear, understandable to even the least educated. Make sure the client is totally au fait with what's available and where it can be sourced. Information needs to be in plain English . . . sometimes hospitals and GP's speak in medical terms known only to medics.
The availability of information for the next-of-kin was also an issue identified by respondents.
As next-of-kin to someone recently in hospital, I felt that decisions were not fully explained and doctors were not accessible enough.
While next-of-kin may want information, it is important to remember that next-of-kin do not have the right to access a person’s medical information unless they have been given specific legal authority. Nor can they give or refuse consent to treatment on behalf of another person in the absence of specific authority. In the qualitative study, it was noted that most if not all participants believed their next-of-kin had the authority to make decisions for them in the event of potential incapacity. Greater healthcare planning may take place if more people were made aware of this and knew that next-of-kin would have a limited role in shaping any future healthcare decisions.
Personal support and the lack thereof arose in several responses. These comments underlined the various forms that support may take and the challenges that are experienced when support is lacking. Several respondents drew attention to a lack of family or social supports if they live alone and the pressures this places on them: Don't have any relatives to help. Hospital staff find this incredible and get annoyed when I can't give them a ‘next-of-kin’ for their forms. Feel I have to be so proactive in my own health care to get satisfactory results. Not easy when on your own, and in pain and consequently unable to drive.
Time pressures were highlighted by respondents who felt their experience with healthcare professionals was dictated by timing: When I go to the GP I feel as though I am on a conveyor belt that she does not have time to listen, and therefore does not have a comprehensive view of the presenting problems. More time with professional would be great, when making decisions. I don't like asking questions as I feel the consultants time is too valuable plus I feel silly not knowing the answers.
Such experiences are not conducive to the provision of information and appropriate support. Instead, these time pressures may exacerbate challenges in healthcare decision-making for both the healthcare professional and the patient.
The manner in which support and information is provided is also an important consideration. For example, availability and ease of access must be kept in mind: As we're nearly all living longer help should be offered re health and aging. Everything now seems to be 'online' forgetting those who can’t cope online–even after ‘getting started’ courses.
Respondents referred to the importance of information being available in hard copy, while no respondent asked for additional material to be made available online.
Discussion: the experience of healthcare decision-making
Contemporaneous healthcare decision-making is marked by several factors which shape the older person’s experience. In particular, the empirical research identified personal factors in addition to the role of the healthcare professional in facilitating a person’s autonomy. The experience of contemporaneous decision-making appeared to be largely positive from the quantitative responses, with 74.91% of respondents reporting being involved in making decisions about their medical treatment, and therefore supported in exercising their autonomy. The qualitative data yielded a more nuanced picture which suggested that the level of involvement depended very much on the degree to which the person wanted to be involved. In effect, this assessment of involvement was, in part, framed by a subjective understanding or expectation of what involvement means. It did however demonstrate that healthcare professionals were responsive to the needs of the individual patient, reflecting a person-centred approach to healthcare in practice.
Factors such as physical health and educational attainment were shown to increase reported involvement in healthcare decision-making. In line with this, research by Hwang et al. has shown that the higher the level of education, the greater the level of perceived autonomy. 98 These are elements that contribute to a person’s independence and, in turn, allow them to engage closely in their healthcare. 99
The level of involvement is not a rigid concept but can be altered through the provision of appropriate information. This moves away from limited ideas of autonomy as non-interference and instead imposes a positive obligation ‘to ensure adequacy of choice’. 100 This can in part be achieved through the actions of the healthcare professional and begins to frame autonomy in terms of empowerment. Certainly, reports on the previous interaction with a healthcare professional were largely positive and suggest that policy is being translated into good practice surrounding consent. Additional support may therefore further facilitate the autonomy of the older person. 101 Respondents demonstrated a desire for additional information across the spectrum of healthcare decisions. Such information can allow the older person to take a more active role in their healthcare and, accordingly, can contribute to an increased quality of life 102 and can protect human rights such as the right to life, autonomy, and bodily integrity. 103
Challenges facing advance care planning
Although a majority of respondents reported feeling involved in current healthcare decision-making, this did not reflect the levels of engagement in advance care planning. It can be suggested that respondents adopted a myopic approach to decision-making whereby day-to-day healthcare decisions were given greater attention than long-term planning. In effect, respondents did not connect advance care planning or discussions about end-of-life care with their level of involvement in healthcare decision-making. The failure to engage with advance care planning represents a lost opportunity to extend a person’s autonomy and ensure that their voice can inform healthcare decisions where they might subsequently lack capacity. The low level of engagement is not indicative of laissez-faire or disinterested attitude. Indeed, the empirical research demonstrated a significant lack of information and/or understanding among participants as to what the current legal position is in Ireland, and a good deal of confusion around what steps could be taken to plan for future healthcare decisions and how the various legal instruments differed from one another. Literacy surrounding the tools and resources for advance care planning must therefore be a priority if these challenges are to be addressed.
The lack of clarity shown among respondents was not entirely surprising as the law itself has not been especially clear. For instance, there was tenuous judicial recognition of advance healthcare directives in the mid-1990s 104 but it was not until 2015 that there was a clear pronouncement on legal status. 105 The divide between the legal framework and people’s perceptions of decision-making was further highlighted by the qualitative research which suggested that many respondents believed that their spouse or next-of-kin would have the legal authority to make decisions if and when required. Misunderstandings of this type can only be remedied through the provision of information and this may prompt people to take a more active role in planning for their future care and medical treatment.
Towards the full commencement of the ADMC Act 2015
The provision and availability of information will become ever more important upon the full commencement of the ADMC Act 2015. The legislation presents a unique opportunity to commence a new dialogue with the public on matters of healthcare decision-making. As Ní Shé et al. wrote, The commencement of ADM provides an opportunity to redefine the provision, practices, and priorities of healthcare in Ireland to enable improved patient-centred care. To facilitate implementation of ADM, it is therefore critical to identify and provide adequate resources and work towards solutions to ensure a seamless commencement of the legislation.
106
By way of comparison, the experience of the Mental Capacity Act 2005 in England and Wales suggests that delivering on the empowering ethos of an act, such as the ADMC Act 2015, depends heavily on effective implementation. 107 In England and Wales, notwithstanding that the Mental Capacity Act 2005 was regarded as a most sensitive and far-reaching piece of legislation at the time, and accompanied by a widely praised Code of Practice, 108 the experience was that implementation of the Act remained a major problem. 109
In terms of the specific challenges to implementation that the Mental Capacity Act faced, that may equally apply to the ADMC Act, the House of Lords Select Committee found that the ‘[t]he Act has suffered from lack of awareness and a lack of understanding’, 110 both with the general public and the professionals who were required to implement it. 111 A lack of information available to the public in accessible form was highlighted as a major concern. 112 The empirical research underpinning this article suggests that the potential for a similar information deficit or asymmetry will be a key point to address as part of an effective implementation of the ADMC Act.
The Health Service Executive set up an Assisted Decision-Making Steering Group in May 2016. 113 The role of the Steering Group is to develop draft guidance for healthcare and social care professionals and to develop education and training, implementation, and communication plans. 114 It is necessary that the older person and the public more generally be factored into plans for communication. The point about ‘online’ literacy is an important one for the older person. Nonetheless, it can be expected that the healthcare professional will be best informed about the intricacies of this legislation. This may result in an asymmetry of information between the healthcare professional and the older person. A cleft in information and awareness of the legal framework could exacerbate existing inequalities as it makes it more difficult for patients to shape their experience of healthcare through contemporaneous and non-contemporaneous decisions. In such situations, the healthcare professional may have to adopt the role of ally and educator in order to best support the older person’s involvement in healthcare decision-making. In this way, the level of empowerment and engagement may be enhanced in the future.
Conclusion
The research set out to compare the lived experience of healthcare decision-making with the existing legal and policy framework and to identify what is currently understood about the ADMC Act and the changes it will bring about in decision-making in terms of advance care planning.
In contemporaneous healthcare decision-making, the picture was positive and the evidence was that policy is being translated into good practice surrounding consent. Respondents reported as being overwhelmingly ‘as involved as they wanted to be’ in their healthcare decisions. This reflects both the existence of support for the exercise of autonomy and a person-centred response on the part of healthcare professionals to meeting a person’s individual needs and requirements. This is encouraging as it suggests that notwithstanding concerns about translating human rights into practice this is being achieved.
The picture in respect of advance care planning is a great deal less positive. There has been a distinct lack of engagement with advance care planning. There are two principal reasons for this. The first is the persistent misconception that a person’s next-of-kin has the authority to make a decision for a person in the event of incapacity and therefore that there is no particular need to make plans for the future. The second is that the law itself is only now being expanded upon and clarified, meaning that a great deal of uncertainty has persisted thus far as to what can be planned for, and how. If people realized that their next-of-kin could not make decisions, the research suggests that there would almost certainly be a far greater interest in powers of attorney and in creating advance healthcare directives, particularly those that appoint a designated healthcare representative. It behoves the appropriate authorities therefore to use the unique opportunity that the imminent commencement of the Act presents to ensure that comprehensive and accessible information in terms of advance care planning is available to everyone who needs it. The protection and promotion of autonomy are not simply about the protection of a human right in isolation. Instead, this right can influence the quality of life and can strengthen physical and social abilities in a way which represents a success in ageing. 115
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The quantitative research was funded by an Irish Research Council New Foundations award. The qualitative research was funded by an Irish Human Rights and Equality Commission award.
1.
2.
Op. cit.; Eurostat, Ageing Europe: Looking at the Lives of Older People in the EU (Luxembourg: Publications Office of the European Union, 2019), p. 9. Older people are defined as those aged 65 years or over by the Eurostat report.
3.
B. Smyth, P. Marsden, F. Donohue, et al., Planning for Health: Trends and Priorities to Inform Health Service Planning 2017 (Dublin: HSE, 2017), p. 6. Adults 65 years and above will increase by up to 21% (131,000) by 2022. There will be 16,100 additional people aged 85 years and above by 2022. The HSE provides all of Ireland's public health services in hospitals and communities across the country.
4.
Department of the Taoiseach, National Risk Assessment 2019: Overview of Strategic Risks (Dublin: Government of Ireland, 2019), p. 40. ‘The share of population aged 65 and over is projected to increase from one in eight to one in six by 2030, and the number of people aged 85 and over is projected to almost double.’
5.
Smyth et al., Planning for Health, p. 19. A person aged 65 years and over attends a General Practitioner practice an average of seven times a year.
6.
Op. cit., p. 27.
7.
S. Donnelly, D. Ó Coimín, D. O’Donnell, et al., ‘Assisted Decision-Making and Interprofessional Collaboration in the Care of Older People: A Qualitative Study Exploring Perceptions of Barriers and Facilitators in the Acute Hospital Setting’, Journal of Interprofessional Care 35 (2021), pp. 852–862. ‘Decision making becomes more complex for older people with multiple health and care needs as the capacity to self-manage is affected by the cumulative effects of long-term conditions.’
8.
S. Abdi, A. Spann, J Borilovic, et al., ‘Understanding the Care and Support Needs of Older People: A Scoping Review and Categorisation using the WHO International Classification of Functioning, Disability and Health Framework’, BMC Geriatrics 19 (2019), p. 195.
9.
The Health Information and Quality Authority (HIQA) is an independent authority established to drive high-quality and safe care for people using the health and social care services in Ireland.
10.
Health Information and Quality Authority, Guidance on a Human Rights-based Approach in Health and Social Care Services (Dublin: HIQA, 2019), p. 8; Health Information and Quality Authority, Supporting People’s Autonomy: A Guidance Document (Dublin: HIQA, 2016), p. 10. ‘Respect for autonomy is important in the context of health and social care, as it is central to person-centred care.’
11.
Health Information and Quality Authority, Guidance on a Human Rights-based Approach in Health and Social Care Services, p. 4.
12.
Full commencement is expected to occur in mid-2022. Mary Donnelly and Caoimhe Gleeson, The Assisted Decision-Making (Capacity) Act 2015: Personal and Professional Reflections (Dublin: HSE, 2021).
13.
M. Donnelly, Healthcare Decision-Making and the Law: Autonomy, Capacity and the Limits of Liberalism (Cambridge: Cambridge University Press, 2014), p. 10; J. Lombard, ‘Autonomy’, in N. Emmerich et al. eds., Contemporary European Perspectives on the Ethics of End of Life Care (Cham: Springer, 2020).
14.
J.S. Mill, On Liberty (London: JW Parker and Son, 1859), p. 207.
15.
C. Edwards, S. Staniszewska and N. Crichton, ‘Investigation of the Ways in Which Patients’ Reports of Their Satisfaction with Healthcare Are Constructed’, Sociology of Health and Illness 26 (2004), p. 159.
16.
A.C. Moller, R.M. Ryan and E.L. Deci, ‘Self-Determination Theory and Public Policy: Improving the Quality of Consumer Decisions without Using Coercion’, Journal of Public Policy and Marketing 25(1) (2006), pp. 104–116.
17.
18.
Pretty v United Kingdom (2002) 35 EHRR 1, [63]. ‘In the sphere of medical treatment, the refusal to accept a particular treatment might, inevitably, lead to a fatal outcome, yet the imposition of medical treatment, without the consent of a mentally competent adult patient, would interfere with a person's physical integrity in a manner capable of engaging the rights protected under Article 8 § 1 of the Convention.’
19.
Charter of Fundamental Rights of the European Union, Article 7.
20.
Bunreacht na hÉireann (the Irish Constitution), Art. 40.3; Re a Ward of Court [1996] 2 IR 79.
21.
See Assisted Decision-Making (Capacity) Act 2015.
22.
M. Donnelly, ‘The Right of Autonomy in Irish Law’, Medico-Legal Journal of Ireland 14 (2008), pp. 34–40.
23.
R. Faden and T.L. Beauchamp, A History and Theory of Informed Consent (New York: Oxford University Press, 1986), p. 274; T. Grisso and P. Appelbaum, Assessing Competence to Consent to Treatment: A Guide for Physicians and Other Health Care Professionals (New York: Oxford University Press, 1998), p. 6.
24.
Fitzpatrick v White [2007] IESC 51.
25.
Lombard, ‘Autonomy’, p. 162.
26.
Rachel Barken ‘“Old Age” as a Social Location: Theorizing Institutional Processes, Cultural Expectations, and Interactional Practices’, Sociology Compass 13(4) (2019), pp. 12673–12692.
27.
Fitzpatrick and Another v K and Another [2008] IEHC 104.
28.
Op. cit.
29.
30.
Op. cit., Re a Ward of Court.
31.
See also Re a Ward of Court [1996] 2 IR 79; JM v St Vincent’s Hospital [2003] 1 IR 321; Fitzpatrick and Another v K and Another [2008] IEHC 104.
32.
[2015] IEHC 259 at [57]; See also JM v St Vincent’s Hospital [2003] 1 IR 321. See Re a Ward of Court; Fitzpatrick v K.
33.
Governor of X Prison v McD(P) [2015] IEHC 259, [126].
34.
35.
36.
37.
UN Convention on the Rights of Persons with Disabilities.
38.
UN Convention on the Rights of Persons with Disabilities, Article 3.
39.
UN Convention on the Rights of Persons with Disabilities, Article 12(1).
40.
UN Convention on the Rights of Persons with Disabilities, Article 12(3).
41.
M. Donnelly and C. Gleeson, eds., The Assisted Decision-Making (Capacity) Act 2015: Personal and Professional Reflections (Dublin: Health Service Executive, 2021), p. xiii; See also M. Donnelly, ‘The Assisted Decision-Making (Capacity) Act 2-15: Implications for Healthcare Decision-Making’, Medico-Legal Journal of Ireland 22(2) (2019), pp. 65–74.
42.
43.
Assisted Decision-Making (Capacity) Act 2015, s.38(5).
44.
Assisted Decision-Making (Capacity) Act 2015, s.41
45.
M. Donnelly and S. O’Keefe, ‘Who Decides?: Consent, Capacity and Medical Treatment’, in M. Donnelly and C. Gleeson, eds., The Assisted Decision-Making (Capacity) Act 2015: Personal and Professional Reflections (Dublin: Health Service Executive, 2021), p. 43.
46.
Assisted Decision-Making (Capacity) Act 2015, s.8(2) ‘It shall be presumed that a relevant person . . . has capacity in respect of the matter concerned unless the contrary is shown in accordance with the provisions of the Act.’
47.
Op. cit. s.3(1).
48.
S.8.
49.
The Decision Support Service describe the nine guiding principles as follows: ‘Presume every person has the capacity to make decisions about their life; Support people as much as possible to make their own decisions; Don’t assume a person lacks capacity just because of an unwise decision; Only take action where it is really necessary; Any action should be the least restriction on a person’s rights and freedoms; Give effect to the person’s will and preferences; Consider the views of other people; Think about how urgent the action is; Use information appropriately’ Decision Support Service, ‘Legislation’. Available at ![]() (accessed 12 April 2022).
(accessed 12 April 2022).
50.
A v Hickey & Ors [2021] IEHC 318, [74].
51.
Medicinal Products (Prescription and Control of Supply) (Amendment) (No. 7) Regulations 2020, SI No. 698/2020.
52.
Assisted Decision-Making (Capacity) Act 2015, s.53-57.
53.
Part 8.
54.
S.84(1)(b).
55.
S.84(1)(c).
56.
S.85(3).
57.
S.84(3)(a).
58.
S.88.
59.
Assisted Decision-Making (Capacity) Act 2015, s.88.
60.
C. Duffy, ‘Mind the Gap: Practical Considerations with Regard to the Assisted Decision-Making (Capacity) Act 2015 from the Perspective of Family Carers’, in M. Donnelly and C. Gleeson, eds., The Assisted Decision-Making (Capacity) Act 2015: Personal and Professional Reflections (Dublin: Health Service Executive, 2021), p. 100.
61.
M. Zwakman, L.J. Jabbarian, J.J.M. can Delden, et al., ‘Advance Care Planning: A Systematic Review about Experiences of Patients with a Life-Threatening or Life-Limiting Illness’, Palliative Medicine 32(8) (2018), pp. 1305–1321.
62.
Donnelly et al., ‘Assisted Decision-Making’, p. 2; C. Davies, F. Fattori, D. O’Donnell, et al., ‘What Are the Mechanisms That Support Healthcare Professionals to Adopt Assisted Decision-Making Practice? A Rapid Realist Review’, BMC Health Services Research 19(1) (2019), p. 960.
63.
The HSE provides all of Ireland's public health services in hospitals and communities across the country.
64.
Health Service Executive, National Consent Policy (Dublin: Health Service Executive, 2019).
65.
Op cit., p. 20.
66.
Health Information and Quality Authority, National Standards for Residential Care Settings for Older People in Ireland (Dublin: HIQA, 2016); Health Information and Quality Authority, Supporting People’s Autonomy: A Guidance Document; Health Information and Quality Authority, Guidance on a Human Rights-based Approach in Health and Social Care Services. (Dublin: HIQA, 2016).
67.
The Health Information and Quality Authority is provided for under the Health Act 2007.
68.
Health Information and Quality Authority, National Standards for Residential Care Settings for Older People in Ireland.
69.
Health Information and Quality Authority, Guidance on a Human Rights-based Approach in Health and Social Care Services.
70.
Op. cit., p. 47.
71.
Medical Council, Guide to Professional Conduct.
72.
73.
74.
Op. cit., ‘You Should Respect and Individual’s Advance Healthcare Directive If You Know They Have One.’
75.
Medical Council, Guide to Professional Conduct, section 16.
76.
Op. cit., section 16.
77.
78.
The research was supported by an Irish Research Council, New Foundations award. Ethical approval was granted for this research project by the [. . .] Research Ethics Committee, reference 2019-04-20-AHSS.
79.
Age Action has a broad stakeholder base with a membership of over 3,000 older people; 800 volunteers; and over 100 employees.
80.
V. Braun and V. Clarke, ‘Thematic Analysis’, in H. Cooper et al., eds., APA Handbook of Research Methods in Psychology, Vol. 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological (Washington, DC: American Psychological Association, 2012), pp. 57–71.
81.
The research was supported by the Irish Human Rights and Equality Grant Scheme 2019. Ethics approval was secured from the [. . .] Research Ethics Committee (reference 2019-09-01-AHSS).
82.
‘Focus groups are a form of group interview used to yield data through communication between research participants.’ Jenny Kitzinger, ‘Qualitative Research: Introducing Focus Groups’ British Medical Journal (1995) 299, at 311.
83.
67.02% of respondents were female, 32.62% male.
84.
49.47% of respondents indicated that they had completed some form of third-level education.
85.
National school was the highest level of education for 9.61% of respondents. Only two respondents, 0.71%, had not completed any level of schooling.
86.
87.
B. Hernández, R.B. Reilly and R.A. Kenny, ‘Investigation of Multi Morbidity and Prevalent Disease Combinations in Older Irish Adults Using Network Analysis and Association Rules’, Scientific Reports 9 (2019), p. 14567. ‘only 9.08% of the population do not have any of the 31 diseases studied.’
88.
S. Cullati, D.S. Courvoisier, A.I. Charvet-Bérard, et al., ‘Desire for Autonomy in Health Care Decisions: A General Population Survey’, Patient Education and Counseling 83 (2011), pp. 134–138.
89.
Donnelly et al., ‘Assisted Decision-Making’, p. 1; F. Bunn, et al., ‘Supporting Shared Decision Making for Older People with Multiple Health and Social Care Needs: A Realist Synthesis’, BMC Geriatrics 18(1) (2018), p. 165.
90.
77.7% of respondents who had completed some form of third-level education felt involved in making decisions about their medical treatment; 82.54% of respondents who discussed their wishes for end-of-life care considered themselves to be involved in decision-making. In all, 88.14% of persons who completed an advance care directive felt involved in making decisions about their medical treatment.
91.
73.68% of respondents were not aware of the Assisted Decision-Making (Capacity) Act 2015. In all, 7.52% of respondents selected ‘not sure’.
92.
The level of awareness was lower among persons who had not completed some form of third-level education. In all, 27.41% of respondents who completed some form of third-level qualification were aware of the Act. The figure was much lower for persons who completed secondary school at 8.82%, while awareness among persons who had completed national school was 14.81%.
93.
L. Bramley, et al., ‘Perspectives on Autonomy and Advance Decision-Making: A Qualitative Study based on Older People Living with Frailty and Their Carers’, Medical Law International. Epub ahead of print 26 June. Available at ![]() (accessed 8 September 2021). ‘Where certainty did exist, participants had often made plans and this was particularly relevant in relation to their post-death arrangements.’
(accessed 8 September 2021). ‘Where certainty did exist, participants had often made plans and this was particularly relevant in relation to their post-death arrangements.’
94.
Should your General Practitioner raise the issue of advance care planning with you? Yes 52.45%, No 12.08%, Don’t know 35.47%.
95.
T. Eynon, M. Lakhani and R. Baker, ‘Never the Right Time: Advance Care Planning with Frail and Older People’, British Journal of General Practice 63(615) (2013), pp. 511–512.
96.
Bramley et al., ‘Perspectives on Autonomy’, p. 26.
97.
Assisted Decision-Making (Capacity) Act 2015, s.87.
98.
H.L. Hwang, H.S. Lin, Y.L. Tung, et al., ‘Correlates of Perceived Autonomy among Elders in a Senior Citizen Home: A Cross-Sectional Survey’, International Journal of Nursing Studies 43(4) (2006), pp. 429–437; A higher desire for autonomy has previously been observed among persons considered to be more educated. See K.E. Flynn, M.A. Smith and D. Vanness, ‘A Typology of Preferences for Participation in Healthcare Decision Making’, Social Science & Medicine 63 (2006), pp. 1158–1169; K.E. Flynn and M.A. Smith, ‘Personality and Health Care Decision-Making Style’, The Journal of Gerontology, Series B: Psychological Sciences and Social Sciences 62 (2007), pp. 261–267.
99.
T. Moilanen, M. Kangasniemi, O. Papinaho et al., ‘Older People’s Perceived Autonomy in Residential Care: An Integrative Review’, Nursing Ethics 28(3) (2021), pp. 414–434.
100.
Donnelly, Healthcare Decision-Making and the Law: Autonomy, Capacity and the Limits of Liberalism, p. 41.
101.
Moilanen et al., ‘Older People’s Perceived Autonomy in Residential Care’; See V. Grow Kasser and R. Ryan, ‘The Relation of Psychological Needs for Autonomy and Relatedness to Vitality, Well-Being, and Mortality in a Nursing Home’, Journal of Applied Social Psychology 29(5) (1999), pp. 935–954.
102.
C. Ferrand, G. Martinent and N. Durmaz, ‘Psychological Need Satisfaction and Well-Being in Adults Aged 80 Years and Older Living in Residential Homes: Using a Self-Determination Theory Perspective’, Journal of Aging Studies 30(1) (2014), pp. 104–111.
103.
Moilanen et al., ‘Older People’s Perceived Autonomy in Residential Care’, p. 424. ‘Autonomy was considered as a sign of respect, dignity and human value and how they were regarded as an individual. Older people said that their autonomy promoted their well-being, subjective vitality and mental health. They also felt that it decreased stress levels, depression and apathy, and improved their quality of life and satisfaction.’
104.
See Re a Ward of Court [1996] 2 IR 79; JM v St Vincent’s Hospital [2003] 1 IR 321; Fitzpatrick and Another v K and Another [2008] IEHC 104.
105.
Governor of X Prison v McD(P) [2015] IEHC 259.
106.
É. Ní Shé, D. O’Donnell, S. Donnelly, et al., ‘“What Bothers Me Most Is the Disparity between the Choices that People Have or Don’t Have”: A Qualitative Study on the Health Systems Responsiveness to Implementing the Assisted Decision-Making (Capacity) Act in Ireland’, International Journal of Environmental Research and Public Health 17(9) (2020), p. 3924, [5].
107.
108.
109.
House of Lords Mental Capacity Act 2005: post-legislative scrutiny.
110.
‘Poor implementation appeared to be a function of low awareness combined with poor understanding of the Act.’ Op. cit., p. 23.
111.
This was also found to be the case in Scotland where the Mental Welfare Commission observed in respect of Adults with Incapacity (Scotland) Act 2000 that, ‘[t]oo often guardians, care staff etc. don’t know the principles exist or what they mean.’ Mental Welfare Commission for Scotland Adults with Incapacity (Scotland) Act 2000 – Proposals for Reform Scottish Government Consultation Response. Available at ![]() (accessed 7 September 2021).
(accessed 7 September 2021).
112.
House of Lords Mental Capacity Act 2005: Post-Legislative Scrutiny, p. 162.
114.
Op. cit.
115.
L. Hansen-Kyle, ‘A Concept Analysis of Healthy Aging’, Nursing Forum 40(2) (2005), pp. 45–57.