
Abstract
Non-therapeutic medical interventions on the bodies of children born with disorders of sex development (DSD)/intersex variations have been subject to increasing critical scrutiny. In response to recent criticism directed at the United Kingdom, and early moves to consider reform, we report on a freedom of information exercise that sought to evaluate whether National Health Service England is meeting international standards on optimal clinical management of DSD/intersex variations. The study explored what medical protocols are being followed to help inform potential reform, particularly with regard to non-therapeutic surgery. While the exercise revealed limited examples of promising practice, current protocols in the majority of Trusts appear unlikely to meet the complex needs of these children. We identify areas where significant improvement is needed, including data management, consistency in guideline use, composition of multidisciplinary teams and addressing disciplinary hierarchies within teams. These concerns sharpen criticisms of the lack of recognition of children’s rights in this context.
Introduction 1
International law and civil society have become increasingly critical of non-therapeutic medical interventions on the bodies of children born with intersex variations. This has been provoked by evidence of the harms occasioned by such surgery and increasing awareness of the children’s rights. 2 In the last decade, condemnation has come from the Council of Europe Commissioner for Human Rights; United Nations (UN) Special Rapporteur on Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment; UN Committee on the Rights of the Child; and the UN Committee on the Rights of Persons with Disabilities. 3 In light of such criticism, and the work of activist and patient organisations, Malta, Portugal and now Germany have prohibited such interventions until the intersex individual is able to provide informed consent and a growing number of other states are considering similar reforms. 4 The focus on informed consent accords with the growing awareness of children’s rights, particularly their rights to bodily integrity and to meaningfully participate in decisions that affect them. 5
Within the national context, in 2016 the UK Government responded to criticism from the UN Committee on the Rights of the Child by characterising intersex issues as solely the responsibility of the National Health Service (NHS). 6 It is arguable that this fails to acknowledge Convention obligations as a signatory state and signalled an unwillingness to take responsibility for these issues. 7 Subsequently, however, the Government launched a call for evidence to investigate the needs of intersex people, specifically addressing their experiences with the medical profession. 8 Within the NHS, the clinical reference group governing this area falls under the umbrella of ‘specialised endocrinology’. This team is yet to commission any policies despite there being international consensus on the diagnosis and care of persons with intersex variations. 9 A consistent and coherent healthcare approach to intersex variations in the United Kingdom (UK) may, therefore, be lacking. In response, the NHS has developed a specialised commissioning group looking specifically at intersex variations.
This article is provoked by these national and international contexts, and we address current practice in England. NHS England is only one of the four health systems in the United Kingdom. Since 1999, health policy is part of devolved powers and similar exercises are warranted in the other health systems. Currently, there is little to no data on how NHS England manages children with intersex variations. Consequently, it has been difficult to effectively evaluate how far NHS England is meeting current international standards on clinical management, if at all. To address this, we undertook a freedom of information (FoI) exercise which sought to explore what medical protocols, if any, NHS England hospitals are following. Before addressing our methodology and results, the following two sections situate intersex variations within the socio-medico context and consider international guidelines for best practice in this area.
Intersex variations
Intersex is an umbrella term referring to a diverse range of congenital bodily variations that at the chromosomal, gonadal, hormonal and/or anatomical level do not neatly fit into the binary categories of male or female. These variations may become apparent at different life stages – and some may never come to know about their variation 10 – although they most commonly present at birth or during adolescence. While adolescents are often referred by their general practitioners (GPs) to specialists where puberty is delayed, absent, or where unexpected changes occur, infants are typically born in secondary care and identified immediately after birth or at some point within the newborn period as a result of atypical genitalia. 11 The three most common causes of newborn genital variations are hypospadias, where the urethral opening occurs in a place other than at the tip of the penis or above the vaginal opening; XX congenital adrenal hyperplasia (CAH); and partial androgen insensitivity syndrome (PAIS). CAH affects the adrenal gland’s production of hormones. A side effect of this adrenal problem can be the overproduction of testosterone which has a virilising effect on foetuses with XX chromosomes and ovaries. Infants are born with a larger than average clitoris or atypical genitalia. AIS affects individuals with XY chromosomes who are unable to process the androgens (hormones) released by their gonads. While complete AIS results in external female genitalia but no female internal reproductive organs (symptoms often not appearing until puberty), in PAIS there may be some degree of masculinisation resulting in atypical genitalia.
It is difficult to state the exact proportion of the population with an intersex variation. This is largely due to the politics and semantics of what variations are and are not included under the intersex/disorders of sex development (DSD) umbrella as well as inconsistencies in reporting. The most commonly cited figure is 1.7% of all live births, an estimate made by Anne Fausto-Sterling and her research team. 12 Fausto-Sterling notes that this is an order of magnitude estimate taken from a wide variety of populations. This figure has been replicated in many academic and activist texts including the Council of Europe’s ‘Human Rights and Intersex People: Issue Paper’. 13 Some scholars, like Sax, have criticised this figure for overinclusion, contesting the intersex status of genetic variations like Klinefelter syndrome (XXY) and Turner syndrome (X), and other variations including late-onset adrenal hyperplasia and vaginal agenisis. 14 Excluding these variances, Sax estimated a lower figure of 0.018%. 15
Since replacing ‘intersex’ with ‘DSD’ in medical contexts, the inclusion of Klinefelter syndrome, Turner syndrome and late-onset adrenal hyperplasia is considered less controversial. The Chicago Consensus statement, for example, sought to ground the categorisation of DSD in genetic differences, explicitly including both Klinefelter and Turner syndromes. 16 However, controversy remains among DSD scientists as to whether genetic variation or genital anatomy should be the primary factor in defining category membership. Consequently, both Turner and Klinefelter syndromes continue to have a liminal position in relation to DSD categorisation and these categorisations therefore remain a contested and political act. 17 Regarding genital variations, recent medical guidelines, including the ‘Global disorders of sex development update since 2006’ statement, have noted that ‘There are no clear estimates of the incidence rate of subjects presenting with atypical genitalia at birth, and only a proportion of them present a major challenge regarding male or female assignment’. 18 Nonetheless, they rely on Sax to estimate an incidence rate of around 1 in 4500–5500. Of these, Sax draws on Fausto-Sterling’s figures to estimate that AIS occurs in 8 in 100,000 live births and CAH with genital variations also occurs in 8 in 100,000 live births. 19
The inclusion of hypospadias within ‘intersex’ is another point of controversy. Hypospadias and cryptorchidism (one or more undescended testes) are not routinely understood as DSD unless the individual presents proximal (severe) hypospadias (where the urethra opening is at the bottom of the shaft or on the scrotum) and it is accompanied with cryptorchidism. Instead, hypospadias is more likely to be understood as a symptom, rather than a condition, or syndrome, per se. Accordingly, hypospadias is not always medicalised, and, importantly, there is current evidence of disagreements among UK DSD clinicians as to whether and why they should be subject to medical intervention. 20 The 2006 international consensus statement notes that if ‘all congenital genital anomalies are considered, including cryptorchidism and hypospadias, the rate may be as high as 1:200 to 1:300’. 21 Overall, existing debates about the incidence rates of DSD variations tend to assume that healthcare providers have integrated efficient reporting systems into their practice, an assumption we challenge in our discussion.
Regardless of the technicalities of classification, healthcare practitioners construct the presence of atypical genitalia as a state of emergency requiring immediate intervention. 22 In part, this is because the majority of protocols around intersex care and management were based predominantly on patients with XX CAH, which, as we shall shortly discuss, do necessitate elements of emergency care. 23 In some instances, CAH can result in salt-wasting where the newborn requires life-saving hormonal treatment. Accordingly, where a newborn presents with atypical genitalia it is imperative that tests are performed to rule out or treat salt-wasting CAH. Problematically, however, healthcare practitioners have routinely presented ‘fixing’ genitalia as an integral part of treating CAH. 24 Yet, as Garland and Travis note, treatment for salt-wasting and normalising genital surgeries are entirely separate matters and should not be conflated. Salt-wasting requires immediate hormonal treatment, not surgical intervention, while normalising genital surgeries can easily be deferred until the individual is able to take part in the decision-making process. 25 Scholarship has criticised this conflation for enabling the medical profession to frame all intersex variations as discrete emergencies to ‘create a sense of immediacy that does not just justify, but necessitates, medical intervention’. 26
Problematically, much of the approach to intersex management has been extrapolated from experiences of people with CAH. 27 Since the 1950s, standard medical practice has recommended surgical ‘normalising’ procedures typically within the first 12–18 months of life 28 in order to ‘fix’ intersex children and allow them to lead ‘normal’ lives. Yet, these interventions are non-therapeutic and unnecessary as outside of salt-wasting CAH almost all intersex variations are benign. 29 Hypospadias (including proximal hypospadias) and AIS, for example, do not threaten the life or health of the individual, and instead treatment is provided to cure social and perceived psychological anxieties; the need for boys to be able to urinate while standing features as a core concern behind surgical interventions for hypospadias. 30
The need to defer surgeries is supported by evidence that these procedures result in a range of physical and psychological harms. Early surgical intervention can typically initiate a series of follow-up and corrective surgeries for the first 18 years of life with one study finding 89% of genitoplasties (planned as one-stage procedures) required at least one further major surgery.
31
These surgeries can result in scarring, pain, stenosis, dissatisfaction with genital aesthetics and reduction in sexual functioning.
29
Early removal of testes due to perceived cancer risks can lead to reliance on artificial hormones leading to conditions such as osteoporosis.
32
While guidelines recommend preserving fertility, early removal of testes in childhood makes this an impossibility. There is also evidence that the cancer risks associated with intersex variations have been inflated leading to overdiagnosis and unnecessary gonadectomies.
33
As these surgeries remain experimental, the likelihood of indirect negative consequences are also high, including sepsis, infection and death.
34
As with other experimental interventions on children, these risks are rarely acknowledged.
35
Assigning to the wrong sex/gender is also possible with one clinical review finding that children with certain intersex traits changed from their assigned gender in between 39% and 64% of cases.
36
There is evidence that clinicians do acknowledge some of these risks in their consultations, but they concomitantly fail to discuss the possibility that ‘these early genital surgeries may also produce suffering, social alienation, and trauma later in life’.
37
Accordingly, such surgeries raise serious ethical and legal concerns. These concerns are heightened when they are performed for non-therapeutic reasons. As the UN Special Rapporteur on Torture stated: …genital-normalizing surgeries [performed] under the guise of “reparative therapies”…are rarely, if ever, medically necessary, lead to severe and life-long physical and mental pain and suffering and can amount to torture and ill-treatment.
38
Current international guidelines on optimal clinical management
In 2006, over 50 international paediatric endocrinologists met to review the management and long-term outcomes of ‘intersex disorders’.
39
The result of this Conference was the ‘Consensus Statement on Management of Intersex Disorders’ which sets out clear general concepts of care for children born with ‘Disorders of Sexual Development’, the preferred terminology of the Consensus Statement.
40
In particular, with regard to optimal clinical management, it states: gender assignment must be avoided before expert evaluation in newborns; evaluation and long-term management must be performed at a centre with an experienced multidisciplinary team (MDT); all individuals should receive a gender assignment; open communication with patients and families is essential, and participation in decision-making is encouraged; and patient and family concerns should be respected and addressed in strict confidence.
41
Most importantly, the Consensus Statement emphasises that the complex needs of children with intersex variations require an MDT comprised of experienced ‘pediatric subspecialists in endocrinology, surgery and/or urology, psychology/psychiatry, gynecology, genetics, [and] neonatology’. The Consensus Statement also stated that, if available, MDTs should include social work, nursing and medical ethics, although it acknowledged that the team would reflect ‘DSD type, local resources, context, and location’. 42 The significance of the disciplines is illustrated by the duties they are responsible for, as detailed by Gomez-Lobo in Table 1.
Members of the MDT and their roles. 43
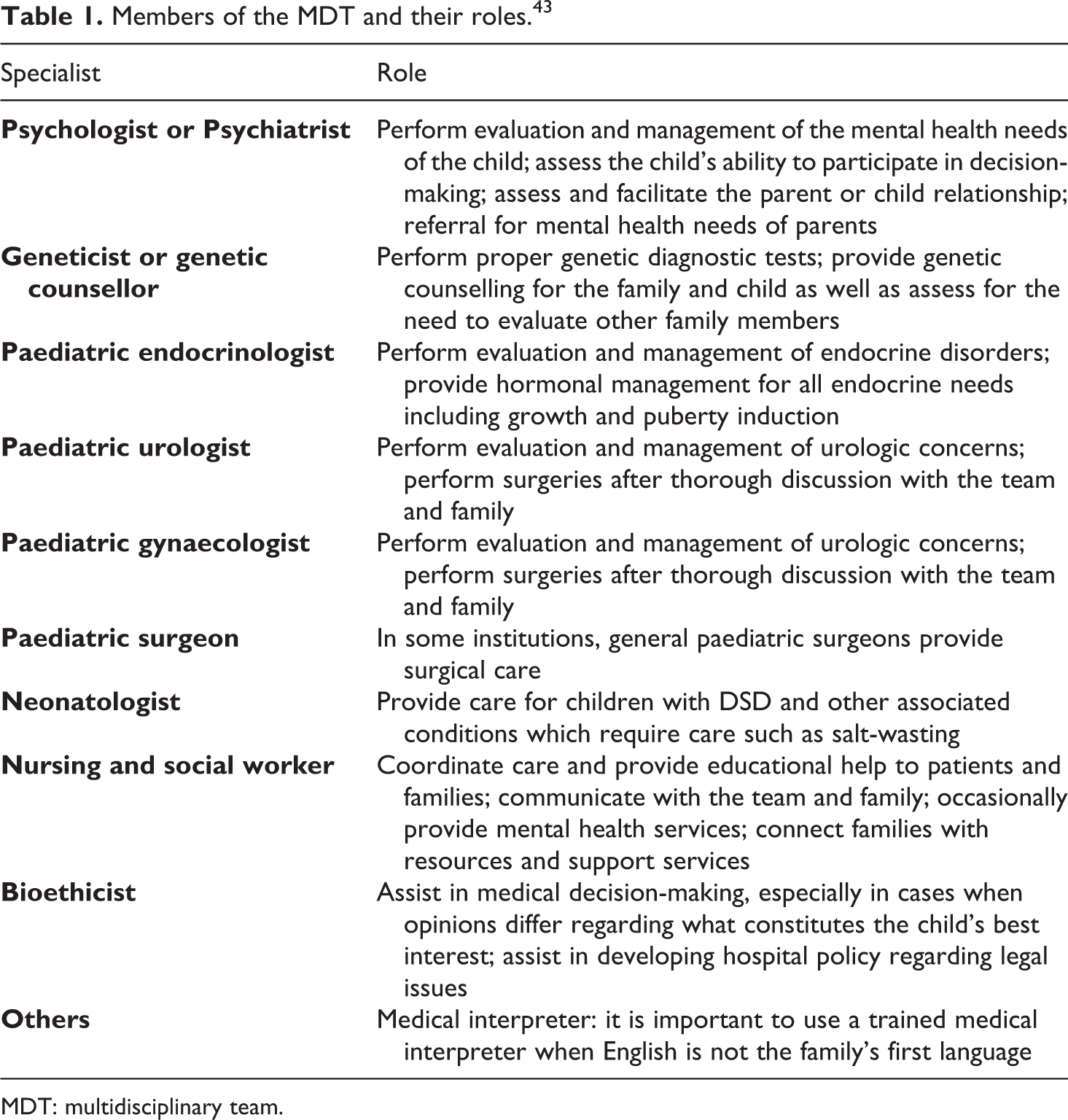
MDT: multidisciplinary team.
The Consensus Statement also stresses the importance of ongoing communication with the individual’s GP, and that ‘Psychosocial care provided by mental health staff with expertise in DSD should be an integral part of management to promote positive adaptation’. 44 When updated in 2016, it was added that ‘education and psychological support was needed…to [allow individuals to] make sense of the condition, relate to their community and establish relationships’. 45 Notably, psychosocial support is considered crucial for the child and their family to ensure ‘the best possible set of decisions [are reached] in the circumstances’. 46 Recently, one of the UK’s leading providers of intersex healthcare, Great Ormond Street Hospital (GOSH), was criticised over failures to provide psychological support to patients. We would expect NHS England to have learnt from and engaged with this psychosocial need. The 2016 update also emphasised the need for MDTs to engage with peer support. 47
While the Consensus Statement recommends deferring non-therapeutic medical interventions, it also points towards a body of literature suggesting that ‘surgery…performed for cosmetic reasons in the first year of life relieves parental distress and improves attachment between the child and the parents’. 48 It also states that ‘systematic evidence for this belief is lacking’. 49 Nevertheless, non-therapeutic interventions appear routinely recommended and practised, and a recent study found these beliefs persist among many healthcare professionals. 50 These practices have been the focus of the international criticism we have noted and the activities of international activists and support groups.
The Consensus Statement produced thorough guidelines in this area, but in the absence of clear NHS policy, little is known as to whether individual NHS England hospitals are adhering to the Consensus Statement’s General Code of Practice. A number of organisations including the Society for Endocrinology UK (SEUK) 51 and the British Society for Paediatric Endocrinology and Diabetes (BSPED) 52 have each developed UK-specific guidance in this area, but it is unclear whether these are being followed in place of international guidelines or at all. Moreover, while these guidelines affirm the need for an MDT, there are some problematic differences in their composition (as we address below) that could limit the extent to which the United Kingdom can be viewed as delivering optimal care. To address this gap in knowledge and explore how children with intersex variations are managed, we conducted an FoI exercise to map out medical practice in this area. Such an evaluation is important and timely given that the UK Government and the NHS are considering medical standards and that controversial management strategies are a potential source of considerable stress for patients and families. 53 The findings presented here provide important evidence for reform considerations in this area. They also have significance for other jurisdictions as the ethics and legality of early management – specifically non-therapeutic surgery – is the focus for increased national and supranational scrutiny.
Methods
FoI requests are an increasingly important methodological tool particularly in healthcare, as ‘data obtained from multiple NHS trusts can provide a rich corpora of data swiftly’ that are not readily available within the public domain.
54
This allows researchers to engage in a wider consideration of the scope of the NHS and to access information that prior to the Freedom of Information Act 2000 would have been difficult to access.
55
While this process is cost-effective both in terms of time and resources, research has shown that FoI requests also have a better response rate than other forms of data collection such as questionnaires or letter-based requests.
56
This section follows Fowler et al.’s proposed methodological checklist to enable the research community to develop a more standardised process of data collection through the use of FoI requests.
57
Fowler et al. recommend that methodological sections should include the following information: Which body/bodies data were requested from How many and what questions were asked The rate and time frame or responses Reasons given when data were not released Amount of data received
58
For our study, FoI requests were sent in July 2018 to 134 NHS bodies: all 131 acute NHS Trusts, and 3 specialist children’s trusts as acute Trusts were unable to respond on their behalf. One hundred and twenty-eight responded (95.2%), with 91.8% answering in full. Reasons given for partial responses included that the cost exceeding the statutory limit or that the data may make individuals identifiable. In some instances, there was no justification. Thirty-one Trusts exceeded the 20 working day statutory time limit for responses, with 6 failing to respond at all. Trusts were asked: Who provides expert evaluation of gender assignment in children with DSD? Does the Trust use an MDT that deals with the evaluation and long-term management and needs of patients with DSD? What specialties are represented on the MDT? When dealing with DSD, what guidelines, if any, do decision makers follow? How many people have been referred to this team per year for the last 5 years?
The term ‘DSD’ was used instead of ‘intersex variation’ as this is the terminology used by NHS Trusts. Our analysis accordingly refers to ‘DSD’. This does not mean, however, that we approve of the term. 59 While FoI requests were most suitable for this exercise, this methodology has inevitable limitations. FoI requests cannot answer why particular practices are adopted nor ascertain their wider impact: such questions require further research. Moreover, ensuring consistency across the Trusts in terms of how they gather information is problematic. The authors acknowledge these difficulties, particularly given the lack of external corroboration of data. 60 Nevertheless, the methodologies employed by the Trusts displayed a logical internal consistency, producing detailed information about the practices of the Trusts. Ultimately, this FoI was designed to initiate and inform discussions regarding medical standards in this area and the exercise generated data appropriate for this.
Results
Of the 128 responses, we identified 15 Trusts that provide care, with 105 Trusts referring patients to these ‘hub hospitals’. 61 It is a concern that eight Trusts claimed they had no engagement with the issues raised, or no guidelines on where to refer patients. 62 Our subsequent analysis focuses on the hub hospitals that provide care for children with intersex variations. While this may seem like a small sample size, it captures all of the MDTs working with children with intersex variations in England. All 15 are listed in Table 2 with the number of hospitals referring patients to them and also the number of patients that had been referred to the hub hospital’s MDT (Q5).
Number of referrals to hub hospitals.
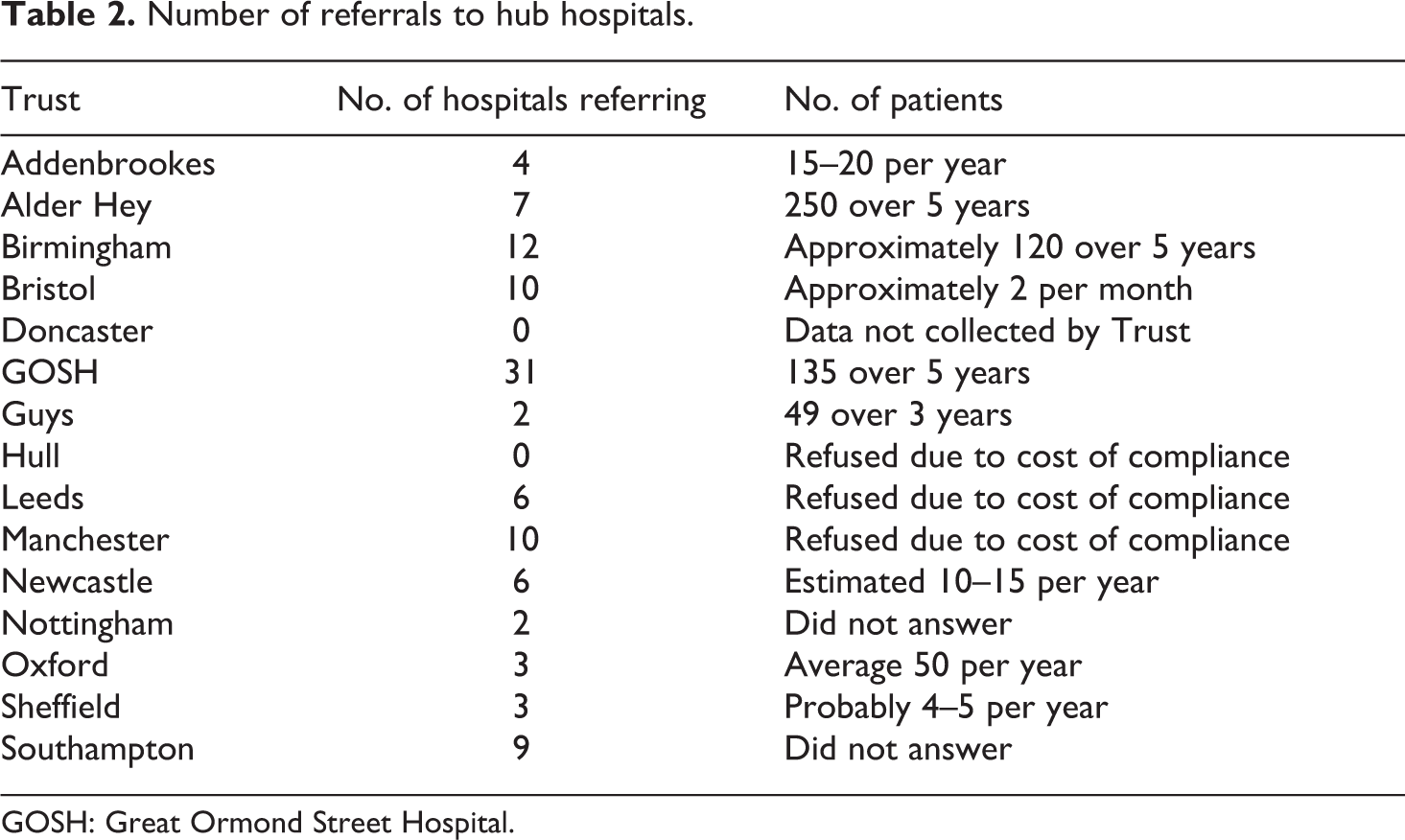
GOSH: Great Ormond Street Hospital.
Of the 15 Trusts, only 9 gave full answers to Question 5 (number of patients referred). Three refused due to the cost of compliance, two gave no reason for the unanswered question and one acknowledged the data are not collected by the Trust. The data from Table 2 also evidence insufficient record-keeping by the Trusts, with only four giving answers not indicated to be an estimate. This limits the value of the data and comparability of results. However, based on only the 9 hubs that responded (which, including referring hospitals, account for 87 of the 120 Trusts who responded, 72.5%), there is an average of between 220 and 227 MDT patient referrals a year. It is highly likely that the number of patient referrals is greater given that six hub hospitals, predominantly located in the North, did not respond. Twenty-seven hospitals refer patients to these six hubs meaning that altogether, we have no figures for 33 out of 120 NHS Trusts (27.5%).
In terms of MDTs, all except three hub hospitals stated that an MDT was responsible for the expert evaluation of gender assignment in children with DSD (Question 1). Newcastle, Doncaster and Bassetlaw, and Hull and East Yorkshire instead indicated that a paediatric endocrinologist would be responsible for this evaluation. Newcastle elaborated stating that expert evaluations are primarily provided by paediatric endocrine consultants and newborns are ‘usually examined at a joint appointment with a consultant paediatric endocrine and a consultant clinical geneticist and if possible a paediatric surgeon who will see the family at the same appointment’.
In response to Questions 2 and 3 (the use and composition of MDT), all hub hospitals – bar Hull and East Yorkshire – confirmed they relied on an MDT, although the disciplines reflected on these specialist teams were subject to significant variance. Table 3 provides details of the composition. Hull and East Yorkshire stated that ‘there is not a specific team, but access to paediatric endocrinologist, paediatric urologist, visiting regional geneticist, paediatric endocrine specialist nurse is available. The long-term management is through the paediatric endocrine specialist clinic’. Hull’s specialisms are included within Table 3. Nottingham declined to answer what specialisms were involved in their MDT.
Composition of MDTs.
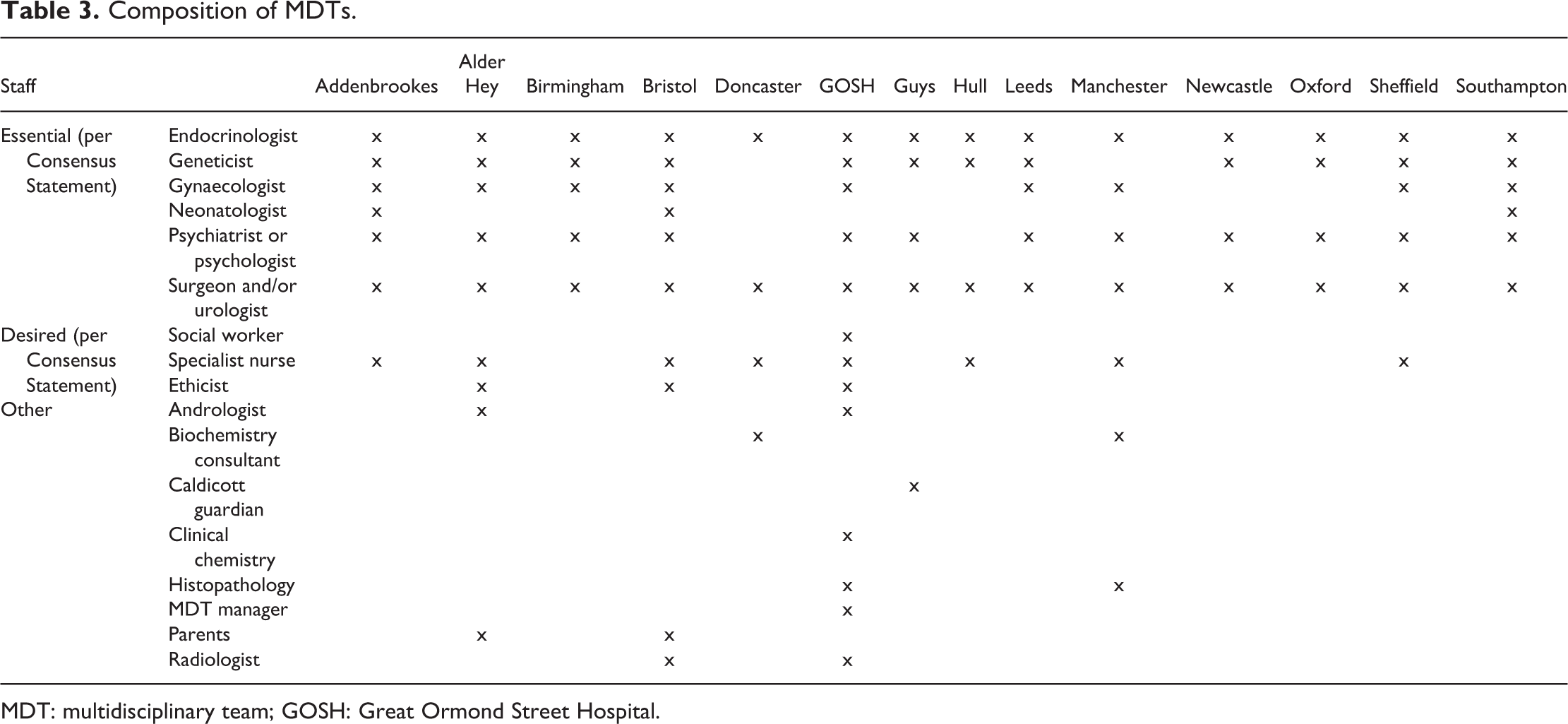
MDT: multidisciplinary team; GOSH: Great Ormond Street Hospital.
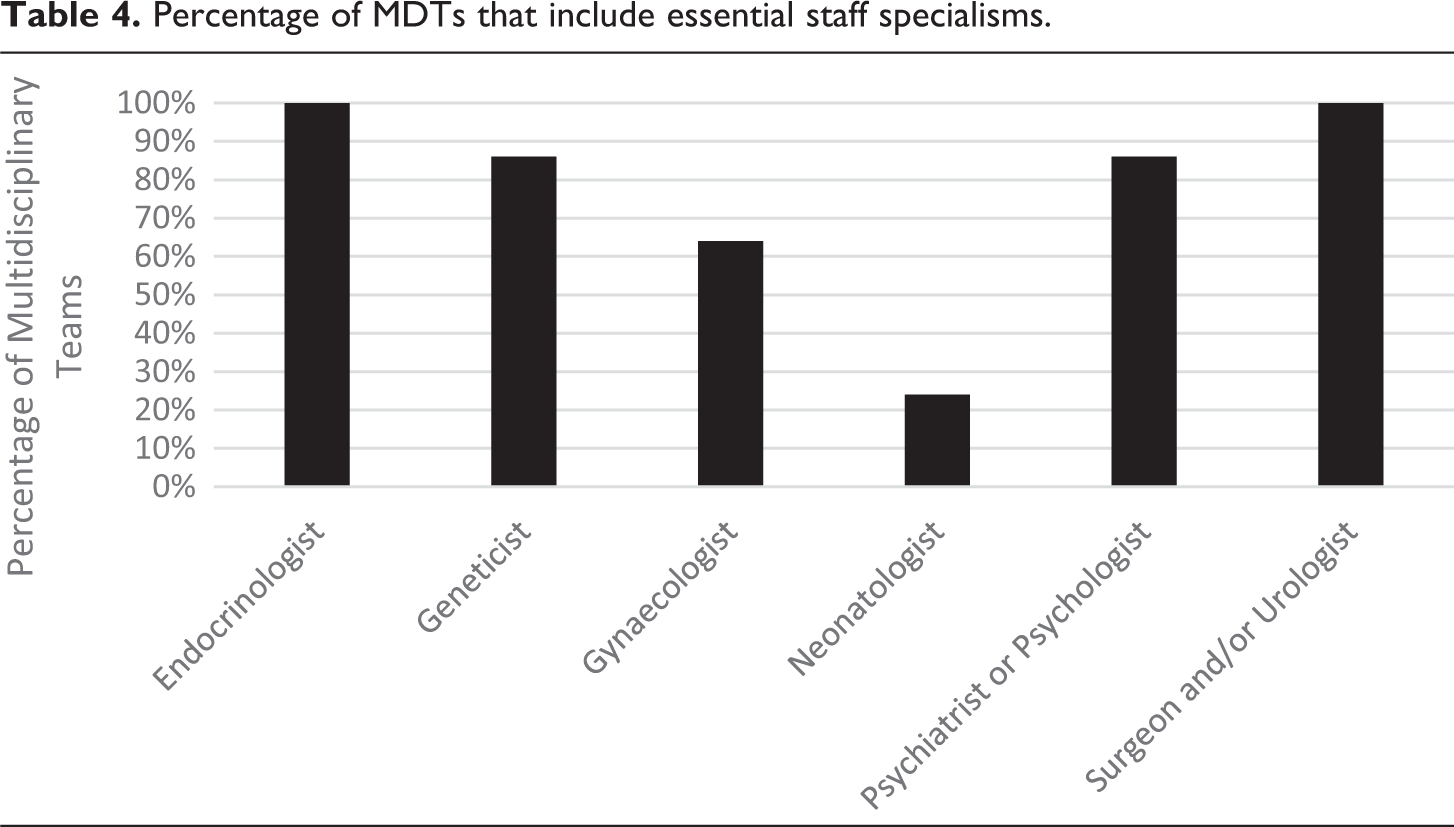
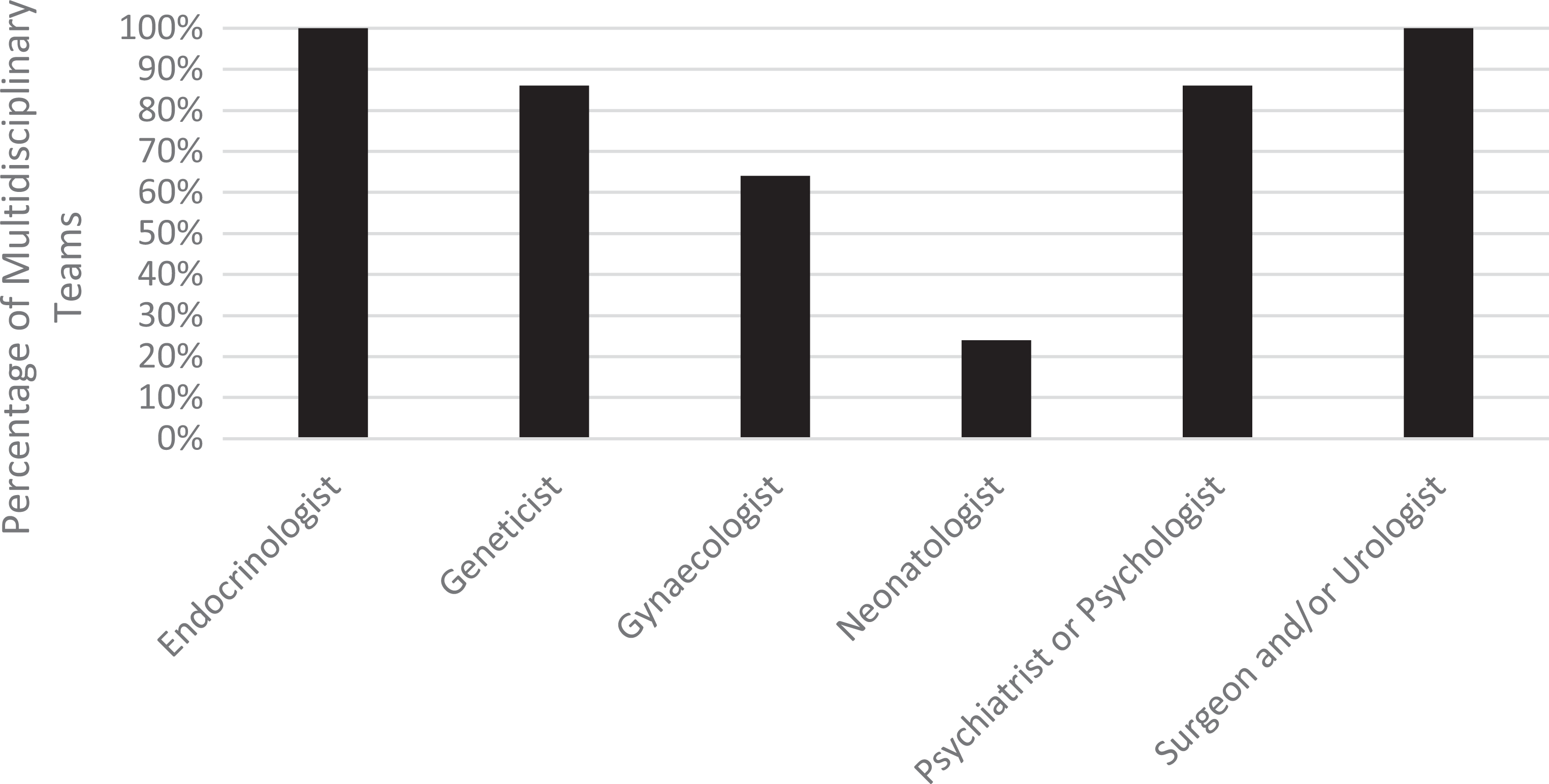
With the exception of Nottingham, Table 4 demonstrates all MDTs have access to an endocrinologist and a surgeon/urologist; 86% have access to geneticists and psychologists; 64% have access to a gynaecologist; and 21% have access to a neonatologist. Accordingly, we can see MDTs in the United Kingdom are not comprised of the staff deemed essential by international guidelines designed to promote optimal care.
Percentage of MDTs that include essential staff specialisms.
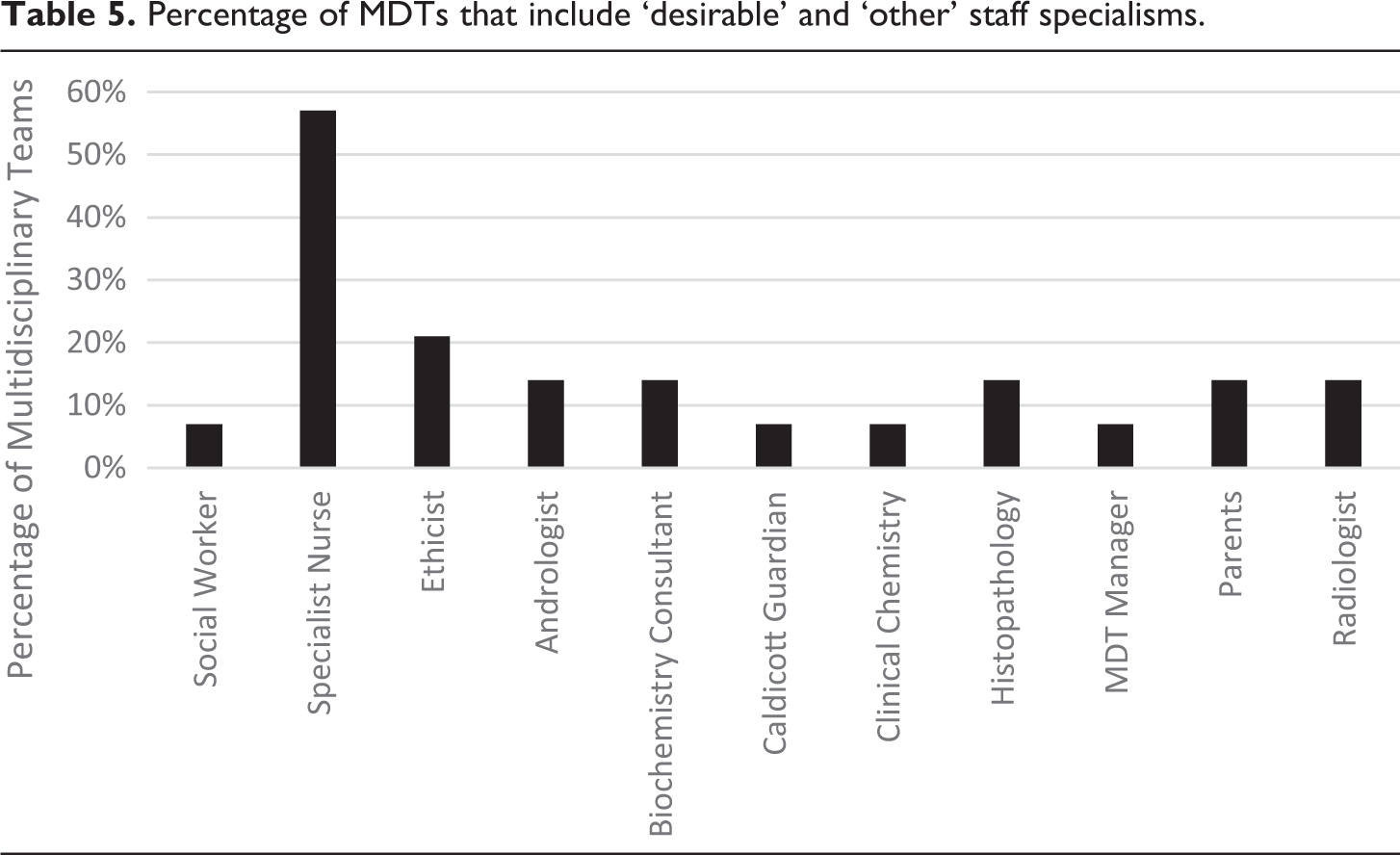
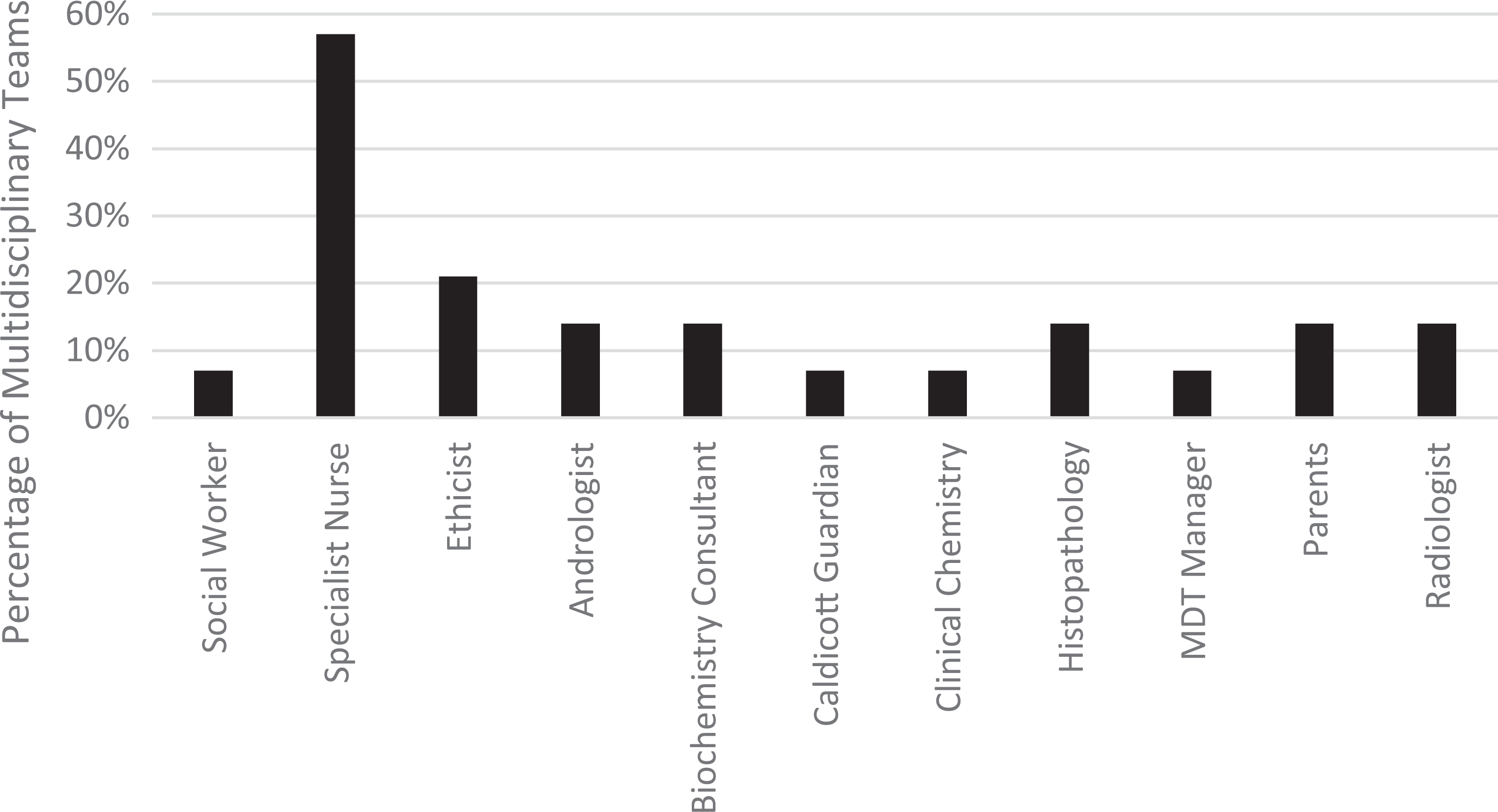
In terms of desired specialisms, as Table 5 indicates, inclusion is much more sporadic. Only 57% of MDTs had access to a specialist nurse. Ethicists were only represented on 21% of MDTs and only one Trust had a social worker. ‘Other’ specialisms are mixed but highlight the greater resources of GOSH – likely because of their dual public and private status, geographic location and the large volume of hospitals that refer on to them.
Percentage of MDTs that include ‘desirable’ and ‘other’ staff specialisms.
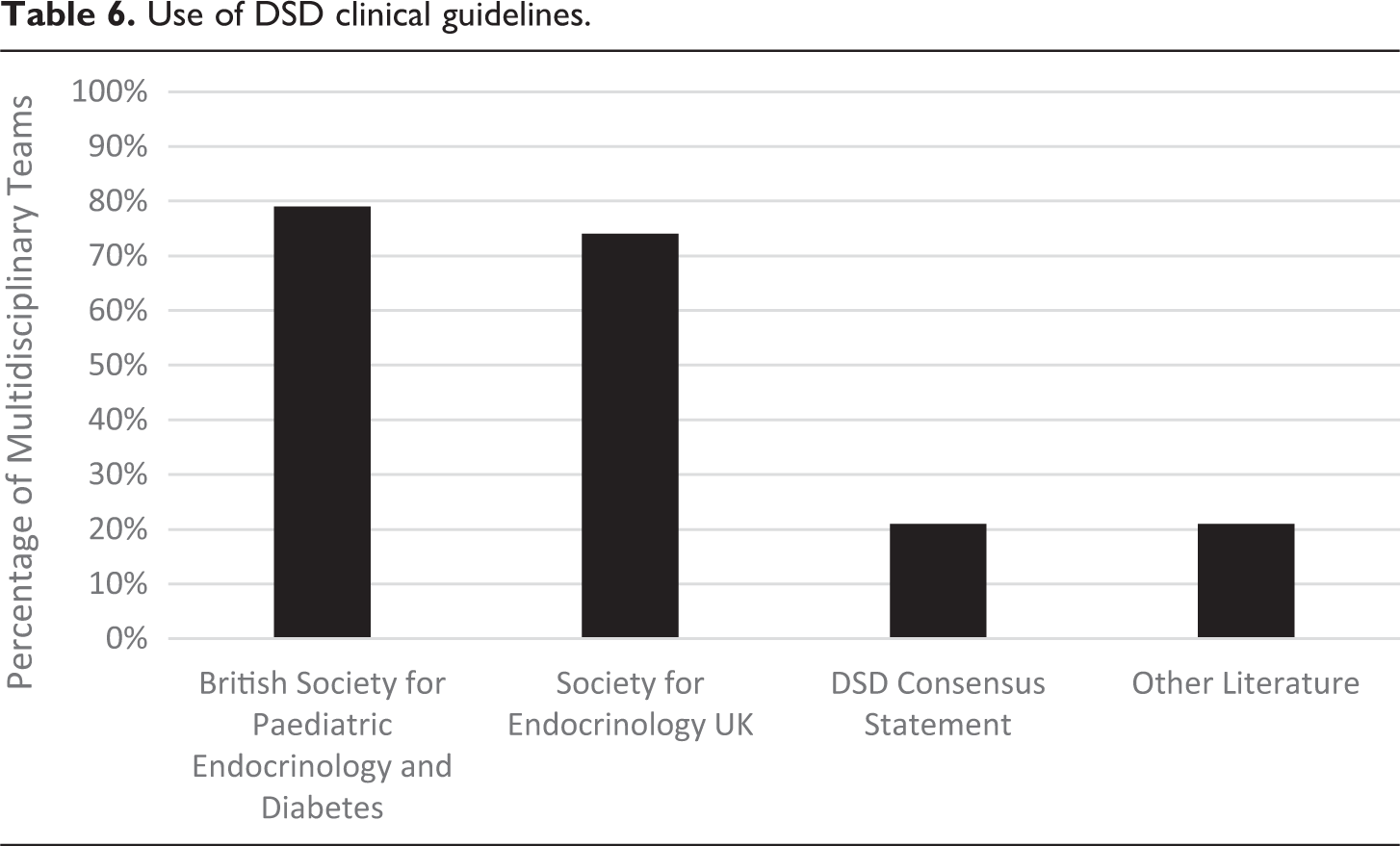
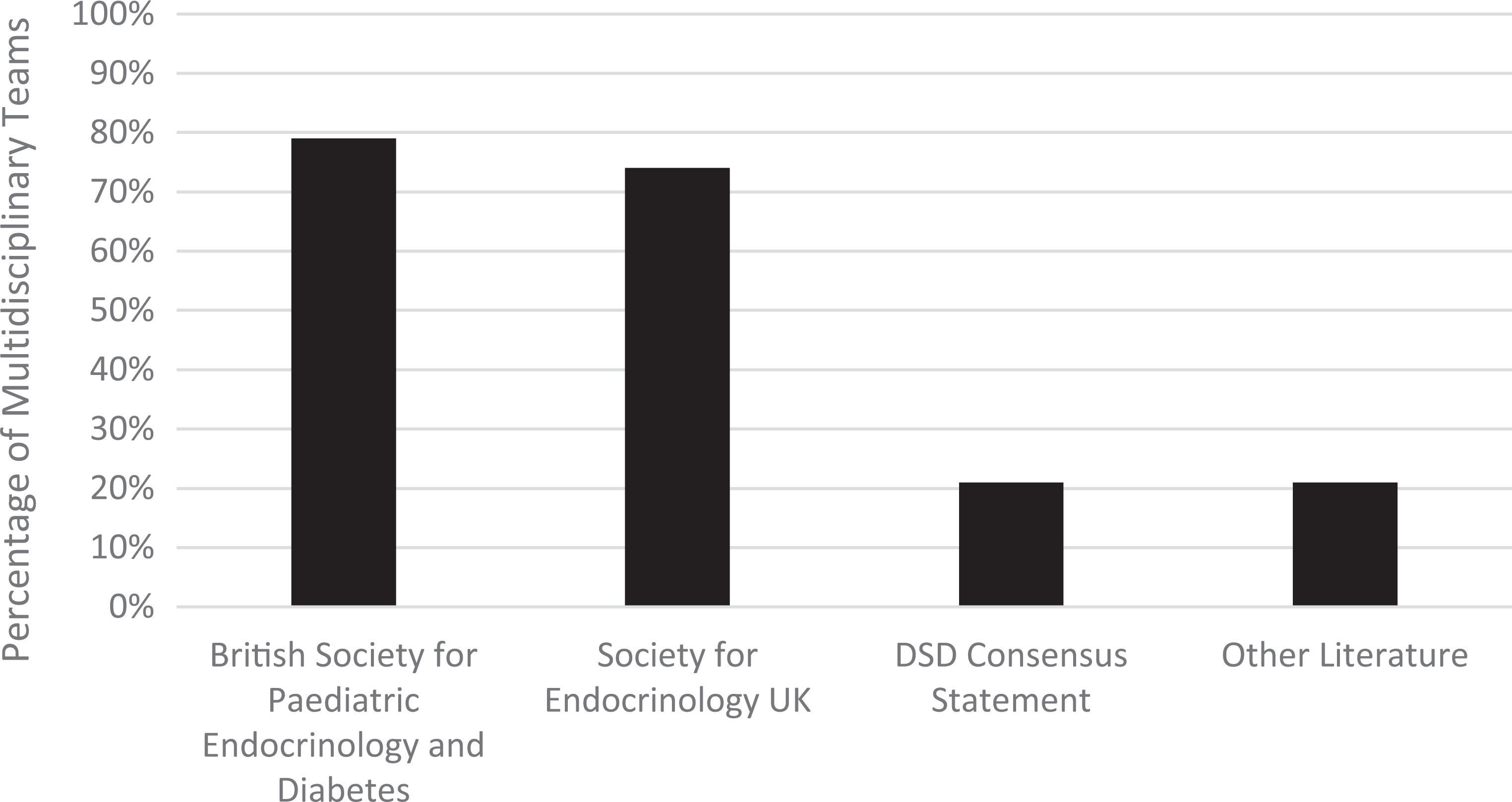
As set out in Table 6, the most frequently used guidelines were the BSPED Clinical Standards and Principles of Management of Disorders of Sexual Development (2017) and the SEUK Guidance on the Initial Evaluation of an Infant or an Adolescent with a Suspected Disorder of Sex Development (Revised 2015): Four MDTs (Alder Hey, Doncaster, Hull and Oxford) do not use the SEUK and three MDTs do not use the BSPED (Addenbrookes, Guys and Newcastle). Only Birmingham, GOSH and Bristol refer to the international DSD Consensus Statement. The examples of other literature provided by Addenbrookes, Bristol and GOSH included the COST Action Working Group’s DSD Consensus Statement, 63 Evaluation and Treatment of Cryptorchidism, 64 undefined literature purely referenced as ‘current’ and their own regional referral guidelines. Once again, Nottingham refused to provide information as to what, if any, guidelines they followed.
Use of DSD clinical guidelines.
Discussion
The data that our exercise generated raise significant concerns regarding clinical record-keeping, geographical variation in MDTs, use of clinical guidelines, the composition of MDTs and professional hierarchies within the health sector. We address these in turn.
Recording intersex variations
Our FoI requests demonstrate inconsistencies in the recording of intersex variations resulting in a significant divergence of incidence rate. This is, to some extent, surprising given the medicalisation of intersex. For example, in Doncaster, the data for the number of DSD referrals were simply ‘not collected by the Trust’. Similarly, two Trusts did not answer the question providing no explanation as to why and three Trusts failed to give the answer due to cost. If the information had been properly and systematically recorded, this would not be a difficult request to comply with. The failure to comply with our requests points to a lack of systematic data collection, suggesting that clinicians are still failing to carefully and systematically record and compile data on these issues. Of the other Trusts, a further three were approximations, again highlighting a lack of precision in data collection.
Improper data keeping is problematic as it challenges current assumptions about incidence rates and therefore the scale of harm in this area. The ‘Global disorders of sex development update since 2006’ statement, for example, notes that ‘Data are not available to determine the exact frequency of specific DSD, while only a small fraction of those with DSD require extensive multidisciplinary assessment to reach a recommendation for gender assignment’. 65 The potential harms of non-therapeutic medical interventions are therefore minimised through appeals to their relative rarity despite the lack of evidence to back up such a claim. Unfortunately, it is not possible to use the FoI data to comment on the incidence rate of intersex variations, particularly given that we do not know which variations are/are not being referred to the MDT (e.g. hypospadias) or exactly when (newborn or adolescence). Nevertheless, our numbers suggest that the referral rate is higher than Sax’s claim of 1 in 4500–5000. 66 Even with the refusal of some MDTs to provide data, our research points to a figure closer to 1 in 3000. Given this figure does not account for 27.5% of Trusts in England, we speculate that it may well be higher but acknowledge that more research is desperately needed. This is compounded by historical evidence demonstrating that families often keep intersex variations a secret from their doctors. 67
Second, the contested nature of the term ‘DSD’ within medical categorisation means that some instances of non-therapeutic medical interventions on children may not be recorded or are being recorded under a different clinical code. In relation to the NHS, Creighton et al. found that despite the introduction of an international consensus statement recommending deferral of intersex surgeries in 2006, there was nevertheless consistent recourse to gonadectomy, bilateral excision of testes, oophorectomy, operations on the clitoris, vaginoplasty, operations on labia, plastic operations on the penis and hypospadias masculinising operations on children up to the age of 14 between 2000 and 2014. 68 While not all of these may be instances of DSD, they highlight the high levels of surgical interventions on the bodies of children within the context of the NHS, suggesting that the 2006 Consensus Statement has failed to impact medical practice. Other research has similarly suggested that surgical practice in relation to intersex variations have not altered in recent years. 69 Munro et al. use these findings to conclude that there is an ‘implementation deficit regarding the 2006 Consensus Statement Guidelines, which is a matter of pressing concern, given the evidence that early childhood surgical procedures can be harmful and that poor prognosis is common’. 70
A third linked issue arises from these two points. The lack of systematic data collection makes it impossible to evidence how often and when non-therapeutic medical interventions are happening. Medical professionals continue to claim that practices and techniques have improved, that surgical interventions are rare and that anecdotal accounts of harm from intersex activists are therefore not based on current practice. 71 All of this means that it is incredibly difficult to make informed national policy decisions in either the medical or legal sphere. Attempts to improve intersex care to support intersex people are therefore hampered by the lack of systematic data collection.
Guidelines
The results identified two main sources of guidelines: the BSPED and the SEUK guidelines. The BSPED guidelines are brief and refer only to the composition of MDT and key bullet-point recommendations for the care of patients with DSD. In contrast, the SEUK guidelines are more comprehensive and mirror, in many ways, the international guidelines in the field. This is unsurprising given that one of the authors of the SEUK’s guidelines was also an author of the international consensus. Nonetheless, there are some differences in the recommended MDT composition which are unexplained by the text. Moreover, there are differences between the listed MDT composition within the text and the table offered within the SEUK guidelines. 72
One issue raised by MDT reliance on these guidelines is that while they may result in consistent management practices, their primary focus on endocrinology means they are not fully utilising the interdisciplinary potential of MDTs. Indeed, the SEUK guidelines specifically state that ‘the paediatric endocrinologist assumes the role of clinical lead and oversees the timely involvement of other members of the team’. 73 The reliance on these specialisms may further compound the homogeneity of care pathways offered and limit any impact of the non-medical specialisms on MDTs. As Table 7 demonstrates, the BSPED does not contain any reference to additional specialisms while the SEUK guidelines separately recommend that MDTs should have wider links to an MDT team consisting of specialists ‘from adult endocrinology, plastic surgery, gynaecology, clinical genetics, clinical biochemistry, adult clinical psychology and social work and, if possible, to a clinical ethics forum’. 74 It is notable that adult endocrinology and plastic surgery are at the top of this list and a ‘possible’ ethics forum is last. Despite the lead author having been part of the consensus statement drafting, there is no explanation given as to why the UK guidelines should differ so markedly from the international consensus other than ‘some areas [of the consensus statement] were not covered in sufficient detail’. 75 The UK approach in these guidelines problematically places a greater emphasis on an endocrinologist/urologist model and on surgery: unlike the Consensus Statement, the SEUK guidelines do not recommend deferring surgery but rather suggest that psychological support is available for parents so that they can be ‘informed of the controversies around undertaking or withholding early genital surgery’. 76
A comparison of guidelines-suggested essential MDT composition.
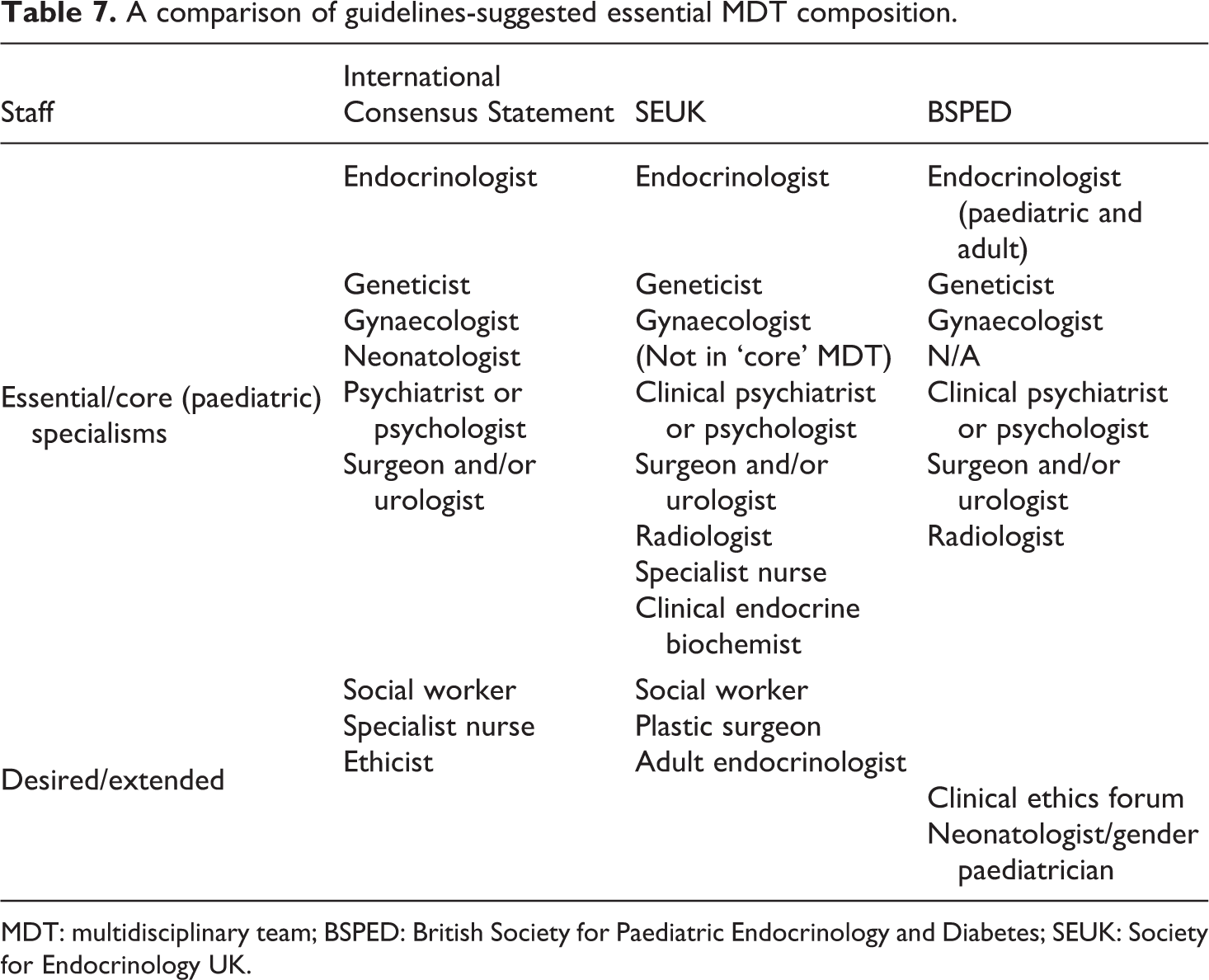
MDT: multidisciplinary team; BSPED: British Society for Paediatric Endocrinology and Diabetes; SEUK: Society for Endocrinology UK.
Furthermore, unlike the international guidelines, neither the BSPED nor SEUK guidelines acknowledge the legal and ethical issues raised by non-therapeutic medical interventions on the body of the intersex child. Although the SEUK guidelines make passing reference to a possible ‘ethics forum’ in wider MDT links, it mentions nothing else in this regard. As already noted, legal scrutiny of this area is intensifying at international level, with the UN making 40 recommendations on intersex issues in its concluding observations since 2013. A number of these recommendations were made before the drafting of the current guidelines. As such, there is a danger that NHS Trusts that rely primarily on the UK guidelines may be falling behind international clinical and ethical standards and, in particular, the Consensus Statement. While some leading UK endocrinologists have rejected the idea that non-therapeutic medical interventions may contravene human rights obligations, 77 we advocate a greater engagement with lawyers, ethicists and patient-activists in order to ensure that international guidelines are appropriately followed.
We would therefore support a shift from the current endocrinologist/urologist-based guidelines to a new interdisciplinary set of guidelines drawing more on psychological, ethical and legal obligations. As Roen states, such a model allows ‘psychological health care [to act as] the foundation upon which other kinds of health care may be built as needed’. 78 This will require a shift in funding from surgical management to a psychosocial framework, 79 something for the newly formed NHS specialised commissioning group to consider. Moreover, it will require new guidelines to be developed in this area.
MDT composition and geographical variation
In general, our results show children with an intersex variation who enter the NHS will be managed by an MDT. This is consistent with the Consensus Statement. However, the meaning of ‘MDT’ is subject to a significant degree of geographical variation. While endocrinologists and urologists are uniformly represented, only three MDTs contain all specialisms considered essential by the Consensus Statement or even UK guidelines. In particular, there is a distinct lack of neonatologists. In the United Kingdom, this could perhaps be explained by the division of neonatology as a distinct branch of paediatric medicine within the NHS. Neonatologists primarily deal with instances of acute care in newborns and so are primarily housed within Neonatal Intensive Care Units. This siloing of medical and professional expertise through the NHS may lead to their lack of representation on MDT and may also explain why some of the UK-adapted guidelines are less prescriptive about having a neonatologist on the MDT. 80 The lack of gynaecologists, however, is less easy to explain and needs further research and assessment.
While it is positive that psychologists are represented in 12 out of 15 Trusts, the inclusion of other specialisms or sub-specialisms desired by the Consensus Statement is extremely limited with nursing, ethics, social work and social care rarely if ever included. This is perhaps unsurprising given the narrow MDT composition within UK guidance. GOSH is an exception in this regard (although this may be due to the media scrutiny it received regarding care in 2017). 81 Bristol is also notable in terms of promising practice. Only two hub hospitals specifically referred to parents either as part of the MDT or consulting with the MDT, and no reference was made by any of the Trusts to peer support groups. While silence does not necessarily indicate that MDTs are not engaging with parents or peer support groups, it is perhaps indicative of a hierarchy between medical specialisms and those constructed as being outside of the MDT. Intersex children and their families are signposted towards peer support instead of this being built into the MDT themselves. Such an approach follows the recommendation of the SEUK guidelines and shows another disjuncture between national and international approaches. Further research is needed to ascertain what level of input such groups are playing at the various hubs, particularly given that they can play an important role in decisions made over care pathways. 82 In terms of variations in MDT composition, Gomez-Lobo found that gaps in disciplinary representation may be due to the result of lack of available expertise. Thus, it is imperative that financial, administrative and technical support is provided to ensure MDTs consist of the appropriate specialisms required to best support children with intersex variations. 83
Perhaps the most concerning aspect of the results is the lack of appropriate psychological support for children and their families in areas served by Doncaster and Hull hub hospitals. There is also emerging evidence that even where psychological support is available it is not centred around the needs and experiences of intersex service users. In the United Kingdom, service users are being referred to Gender Identity Development Services. These services are in high demand and are largely based upon the experiences of trans service users. As a result, intersex children and their parents have reported anecdotally being discharged after one session, as they do not display signs of gender dysphoria. 84 This may confirm Horowicz’s concern that the use of diagnostic criteria in referrals to Gender Identity Development Services are problematic. 85 Moving away from imprecise and limited diagnostic criteria would allow for ‘individually focussed psychological support and monitoring from clinicians across a child’s development. This approach would provide an ongoing developmental commitment, through a positive and proactive approach, to understanding the individual psychological needs of each child’. 86 Taking these points in conjunction with the findings of our study may indicate a lack of continuing support available for intersex children and their families. It may also point towards a need for serious and specific training for psychologists around intersex issues as well as the need for more funding to be made available for these services. While our study focused on the experiences of children, it is worth noting that there is only one MDT available to adults in the entirety of England.
Relatedly, the BSPED and SEUK guidelines recommend that MDTs should include radiologists. This was the case for only two of the Trusts despite most of them following the BSPED guidelines. Consequently, the data highlight significant geographical variation in the make-up of MDTs with subsequent effects on optimal clinical care for intersex children and their families.
MDTs and disciplinary hierarchies
The common presence of a psychologist in MDTs intimates that psychosocial needs are generally seen as an integral aspect of care. However, the inclusion of these specialisms must be taken with some degree of caution: the results cannot reveal how or when the psychologist is involved. Elsewhere, commentators have highlighted a failure to engage in genuine multidisciplinary work so that alternative approaches and frameworks have not been explored. This has been particularly frustrating for the integration of psychology into MDTs. As Liao et al. note, although ‘multi-disciplinary care pathways for…DSDs often allude to the importance of psychological interventions, [they]…are usually set up without due considerations of them’. 87 Liao and Roen conducted interviews with 32 MDT members and found psychologists risk being marginalised as their expertise is seen as peripheral. This can see them working in parallel and separate to the main MDT. 88 As they write, ‘the centrality of a medical process…was taken for granted rather than negotiated. The classification of intersex traits as pathological dictates clinical priorities and hierarchical arrangements, leaving very little space for psychosocial staff to formulate different ideas and solutions’. 89 MDTs often suffer from an absence of leadership that sees them default towards a medicalised approach that favours ‘action’ over deferral of treatment. 90 Of our 15 hub hospitals, only GOSH has an MDT manager and thus any evidence of an MDT organisational structure and, if hub hospitals are following the SEUK guidelines, it is likely these teams are led by paediatric endocrinologists.
Accordingly, we remain sceptical as to how and when psychosocial care is being incorporated into care pathways. Offering alternative care pathways has not been the case under the current endocrinologist-dominated model where clear hierarchies between healthcare professionals persist. This affects the timings of when different specialists are brought into the MDT with research suggesting that psychologists tend to be brought in after surgery has taken place and where there is a perceived psychological problem (such as depression). 91 Newcastle’s response to Question 1 demonstrates the potential for these hierarchies to play out in practice, particularly how surgeons may influence the care management of children with an intersex variation. Newcastle stated that examinations of newborn infants ideally involve a paediatric surgeon who will also be present at the first meeting with the family. The presence of a surgeon at such an early stage means they are well placed to influence the parents’ decision-making process. In Newcastle’s first meeting, there is a notable absence of psychological expertise. While our results do not disclose whether this experience is shared in other Trusts, most responses stated the MDT would provide the expert evaluation, of which the urologist/endocrinologist is consistently a central feature and where an MDT lead is generally lacking. We share Liao et al.’s concerns that although ‘it is obvious that parents affected by DSD first and foremost require sustained psychological support…this does not seem to be the central focus in paediatric management’. 92 Indeed, it may be understood more as an afterthought. The absence of psychologists from initial discussions with families is pronounced given that ‘they are likely to be the only team members with advance training in communication in emotive environments’. 93
The downplaying of psychosocial support within MDTs has important consequences for the ways in which parental concerns are understood and addressed. Timmermans et al.’s direct observations of interactions between healthcare providers and caregivers in DSD clinics found that clinicians frame gender in a biomedical way thus skewing the process of gender assignment. 94 Informed by caregivers’ already preconceived expectations regarding the child’s future gender, clinicians are able to ‘marshal information strategically to make certain decisions seem more appropriate than others’. 95 Clinicians and parents thus co-produce gender using a ‘medical rationale that absolves clinician and parents from making the “wrong” choice’. 96 Other research has raised important concerns over the potential for healthcare professionals to ‘lead’ parents into making certain decisions though the way they frame information. 97 This framing may, in practice, shut down dialogue between parents and medical professionals by presenting information as a single unified collective. 98 As Davis writes, ‘While this model can disperse medical decision-making power, it also can reassert the authority of medical professionals over intersex traits by vesting it in a group, not simply an individual’. 99 Moreover, the lack of MDT representation from psychiatrists, social workers and broader fields such as ethics, bioethics, law, sociology or anthropology may be due to their greater potential to ‘reject essentialist beliefs about sex, gender and sexuality’. 100
The central role of a surgeon/urologist is particularly concerning when non-therapeutic interventions are a primary concern for service users, 101 advocacy groups 102 and the international bodies that are increasingly critical of practice in this area. These are non-medically indicated interventions that can be characterised as socially motivated gender-‘normalising’ or ‘confirming’ surgeries. 103 While each of the guidelines the Trusts refer to acknowledge the merits of deferring surgeries, a recent study shows that healthcare practitioners’ views continue to be shaped by the belief that surgery prevents parental distress 104 despite studies contesting this. 105 Accordingly, many aspects of these surgeries are still practised routinely. This is especially problematic given that international condemnation stems from increasing awareness of the harms occasioned by early non-therapeutic interventions, 106 and the heightened ethical concern generated by their social rather than clinical motivation. 107 This growing attention to harm can be understood as part of a gradual shift in the acknowledgement of children as subjects who have interests and are rights holders. We now consider these non-therapeutic interventions in the context of the right to bodily integrity and a child’s right to participate in decision-making that affects them.
Children’s rights
A number of the concerns raised highlight the continuing limitations of clinical engagement with children’s rights. This may be unsurprising, as at a state level the evolution and adoption of children’s rights has been uneven and, at times, piecemeal. In law, Stalford et al. have argued that courts ‘across all jurisdictions routinely pursue limited, often distinctly disempowering approaches to children’s rights’.
108
In the United Kingdom, it has been argued that courts are still ‘only flirting with the idea that children are rights-holders’.
109
As Stalford et al. note, many courts: …fail to engage with children’s rights issues, confining their adjudication to a factual review of the available evidence rather than a more nuanced understanding of how that evidence might be interpreted in the light of established children’s rights norms and research intelligence.
110
Academic attention has increasingly turned to the importance of bodily integrity as a fundamental ‘psychological need’ 112 and ‘the cornerstone of all other liberties’. 113 Judicial attention too is beginning to acknowledge its importance in underpinning legal rights. 114 In the case of children, the importance of bodily integrity has recently been explored in the context of non-therapeutic interventions. In a series of articles, Fox et al. 115 have argued that in best interest determinations the child’s right to bodily integrity should outweigh other concerns, such as the more amorphous notion of family integrity. In this regard, the authors develop the concept of embodied integrity. This seeks to recognise not only the traditional ‘protective’ functions of bodily integrity doctrine – the injunction to refrain from unwanted interference with the body – but also the embodied nature of human existence.
Attending to embodiment directs us to acknowledge the body as the means through which we interact with and experience the world. Interventions on the body are therefore often biographical, shaping our life experiences and choices. 116 Embodiment helps us to understand the essential role of the body in the developing lives and identities of children and alerts us to the potential impact of non-therapeutic interventions. As Roen writes: ‘The scarring, the aesthetic difference, the changes to sensation are lived continuously. They are necessarily imbricated in the process of an emerging self’. 117 While the approaches of clinicians to their patients clearly differ, 118 where the body is treated as an abstract ‘malleable object’, the role of the body in constituting the emerging subject and selfhood is ignored. 119
The experience of children born with intersex variations who are subject to non-therapeutic gender-‘normalising’ interventions demonstrates the need to respect the embodied integrity of children and young people. While early non-therapeutic surgical interventions are frequently characterised as one-off, they generally result in a childhood and early adulthood marked by additional reparative procedures. Early interventions can also see children assigned to the wrong gender with the significant physical and psychological harms this can entail. Evidence suggests that these risks are being downplayed by clinicians.
120
These unnecessary surgical interventions, motivated by social concerns, are clearly biographical, determining subsequent experiences of child- and adulthood: …surgery does reach beyond the superficial and even beyond the material, enabling a different reality for the emerging self. For those who undergo surgery, the embodied self is necessarily remoulded: surgery is never simply a ‘cosmetic’ endeavour.
121
The kinds of problems that are…left out, or not fully evaluated, concern those issues pertaining to the future desires of the intersex person, or the future political perspective and social opportunities of the intersex person, and issues to do with the complex involvement of the body in the process of becoming.
129
Conclusions
Medical protocols on the management of intersex variations are under increased national and international scrutiny. This is motivated, in part, by the non-therapeutic justifications for many interventions and the significant harm that may follow. Harm to children in the context of cosmetically or socially justified procedures is of particular ethical concern.
134
The UN Special Rapporteur on Torture summarised the direct and indirect impact of such surgery: In many States, children born with atypical sex characteristics are often subject to irreversible sex assignment, involuntary sterilization and genital normalizing surgery, which are performed without their informed consent or that of their parents, leaving them with permanent, irreversible infertility, causing severe mental suffering and contributing to stigmatization. In some cases, taboo and stigma lead to the killing of intersex infants.
135
…there must always be room for the atypically sexed child to imagine and to become, of their own accord, rather than to simply respond to what has already been imagined for them. Early genital surgery dangerously assumes that what was imagined by the adults will be sufficient for, or ought to constrain, the desires of the intersexed child as s/he grows into adulthood.
136
The exercise identified limited examples of promising practice in terms of the composition of MDT. This is seen with GOSH and to a lesser extent Bristol. These were, nevertheless, overshadowed by a widespread failure to include all specialisms that the Consensus Statement set out as essential and desired to meet the complex needs of children with intersex variations. Most notably, non-medical disciplines are problematically absent in a situation that is often experienced as a ‘social emergency’ 138 rather than a pressing biomedical or health concern. Access to specialist treatment and care in this area will be significantly determined by geographical location. NHS England must provide adequate resources and funding to enable MDT to have an appropriate range of specialisms.
Our FoI exercise also found significant problems with record-keeping in this area. There is a severe lack of systematic and comprehensive data collection, and the data that are collected also lack precision. Accordingly, it is difficult to create policy and guidance in an informed manner. We are concerned that this lack of data has been used to justify non-therapeutic medical interventions. Thus, claims that intersex variations and their poor and damaging medical management are ‘rare’ rely upon the medical profession’s own systematic lack of data collection and poor administrative practices.
Our data collection was restricted to NHS England. Practices in the devolved health services require similar investigation. It is also important to address the broader context of health and social care for individuals with intersex variations. This was beyond the remit of the current exercise. However, this must be part of the broader reconsideration of health responses. Further work is required to investigate support practices in the early months and also longer term. 139
Ultimately, our investigation revealed that current practice in English hospitals is lagging behind moves in other jurisdictions to acknowledge the harms of early intervention and the need to respect and promote children’s rights. In this, NHS England hospitals may be out of step with what can be characterised as a developing human rights norm.
Footnotes
Author's Note
Michael Thompson is also affiliated with the University of Leeds as a Professor of Law.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.