
Abstract
Vancouver General Hospital has a rich neurosurgical history; however, little is documented of the role the institution played in the history of extracranial to intracranial (EC–IC) bypass as a surgical therapy. A review of the literature on the history of cerebrovascular neurosurgery was performed to augment a comprehensive personal interview provided by Dr Sydney Peerless to provide a new insight into the journey towards our contemporary understanding of bypass surgery. Along this timeline, we outline key historic figures and their contributions, as well as document the first small vessel EC–IC bypass at Vancouver General Hospital in western Canada.
Introduction
The first small vessel superficial temporal artery (STA) to middle cerebral artery (MCA), extracranial to intracranial (EC–IC) vascular bypass surgery in western Canada at Vancouver General Hospital (VGH), was performed by Dr Sydney (Skip) Peerless in late October 1969.1,2 This followed a serendipitous series of events that saw the development of the procedure by a number of prominent neurosurgeons. By 1973, Dr Peerless had performed and reported on 50 cases. 3 Patient ‘D’ was the recipient of the first bypass procedure in Canada, a man in his early 50s with 4-vessel occlusion – both carotid and vertebral arteries no longer filled beyond the skull base on angiography and the patient was reliant on collaterals. He had presented with a clinical manifestation of an ischaemic stroke on the background of what his family described as progressive dementia.
Over 2400 years ago, Hippocrates first recognized stroke as ‘apoplexy’, a Greek term that may be translated as ‘to be struck down by violence’. 4 This was followed by centuries of progress in the description of stroke syndromes and, eventually, stroke care as we know it today. The developments in cerebral bypass surgery came at a time when there was effectively no means of evaluating the brain parenchyma for manifestations of ischaemia, and cerebrovascular pathologies relating to cerebral ischaemia were poorly understood. 4 Computed tomography only came to the fore through Sir Godfrey Hounsfield's work in the early 1970s. 5 Magnetic resonance imaging followed shortly behind in 1974 through the Nobel prize-winning work of Paul Lauterbur and Peter Mansfield. 6 Additionally, the best medical care was essentially supportive, and evidence for antiplatelet therapy and other acute interventions would not arrive on the scene for more than 20 years. 7 In 1951, Fisher outlined that a major cause of patients' presentation with ‘apoplexy’ may be an unsuspected carotid artery occlusion. 8 Given the lack of available investigations, angiography gained prominence in the evaluation of patients presenting with stroke and a means by which blood could be delivered to the distal territory affected by a symptomatic atherosclerotic lesion was sought.
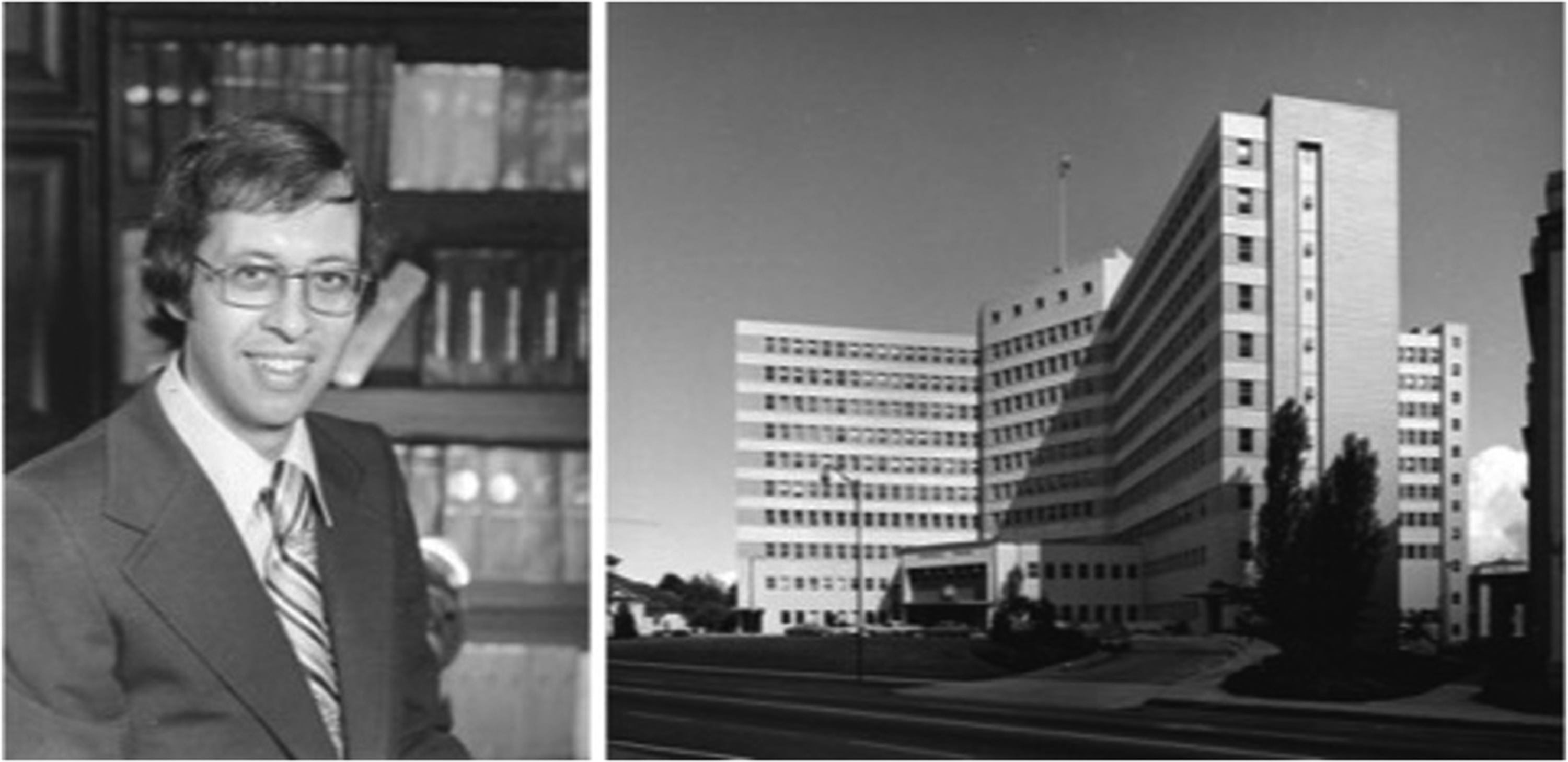
Dr Sydney Peerless was born in Pioneer Mine, British Columbia during the great depression. Eventually raised in the Kitsilano/Dunbar area, he attended Lord Byng Secondary School and subsequently went on to the University of British Columbia for undergraduate and medical studies. He entered his internship year at VGH with a significant interest in cardiothoracic surgery after significant work in medical school focused on developing bypass techniques on the coronary arteries of dogs under the supervision of Drs Peter Allen and Phillip Ashmore. His interest in a pursuit to improve perfusion to the heart was borne out of witnessing a close family member falling ill with cardiovascular disease. However, serendipitously, his first rotations as an intern at VGH were with the Neurosurgery service under the tutelage of Frank Turnbull, Gordon Thomson, Ian Turnbull, Peter Moyes, and Peter Lehmann. 9 Having been treated well by the neurosurgery group, Peerless took a sharp turn into the discipline of neurosurgery and, with the group's assistance, made arrangements to attend residency training at the University of Toronto with the plan that he would take ownership of the paediatric neurosurgery at UBC upon his eventual return (Figure 1).
Refining small vessel bypass techniques
At the Toronto General Hospital, Peerless met Dr William (Bill) Lougheed and was quickly captivated by his work at the Best Institute on microvascular reconstruction. Lougheed recognized the advantages of a microscope in surgery and eventually developed a manoeuvrable, double-headed diploscope to use in both his procedures and lab work.12,13 He is touted as Canada's first microneurosurgeon and eventually performed the first long vein EC–IC bypass in a human in 1971. However, in the 1960s, as Lougheed's experiments with Peerless were underway, the equipment had not yet caught up to the vision. The technique to perform the bypass was relatively straightforward, though success relied heavily on the appropriate equipment. The finest sutures available were 6-0 or 7-0 sutures being used by ophthalmologists and were far too large for the vessels <1 mm undergoing anastomosis. In the animal experiments, hair was often used as a tool and threaded onto needles by hand. Given the lack of appropriate clips that would not injure blood vessels when applied, tourniquets were contrived from polyethylene tubing and fine suture material to encircle and obstruct vessels during the anastomosis. Peerless worked with Lougheed to perfect these instruments for use in microneurosurgery specifically for bypass and surgical treatment of arteriovenous malformations, aneurysms, and tumours of the skull base. This work led to significant collaboration with industry to develop and refine microsurgical instruments, suture material and the microscopes through which these procedures are possible today (Figure 2).
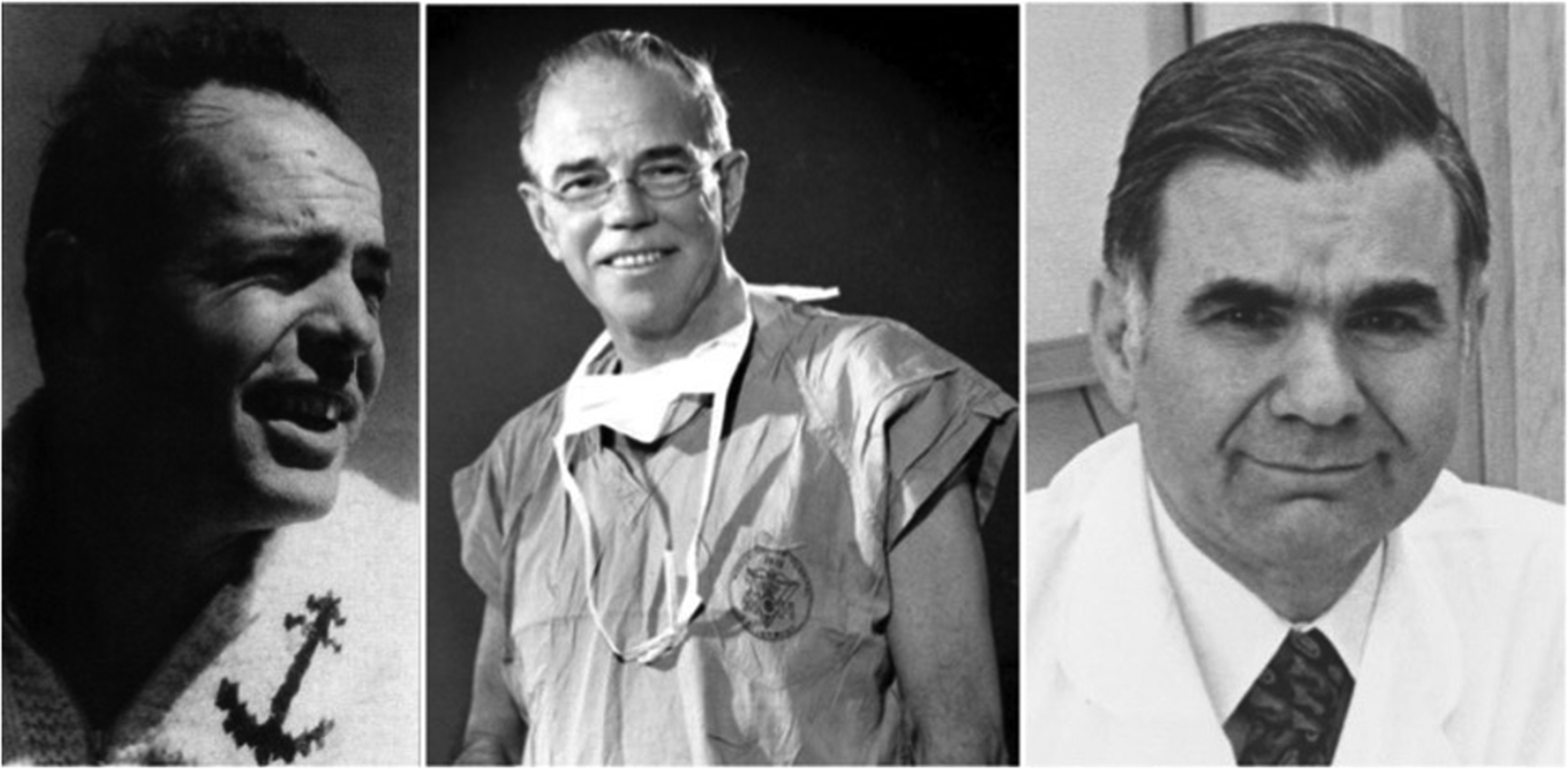
Dr Raymond M.P. (“Pete”) Donaghy worked as a neurosurgeon at the University of Vermont and was a close friend to Lougheed, sharing a common interest in microvascular reconstruction and microneurosurgery. 16 Donaghy, too, was Canadian, born in East Mann, Quebec, but moved to Plainfield, Vermont in his youth. He returned to Canada to initiate his neurosurgical training at the Montreal Neurological Institute where he was mentored by Dr Wilder Penfield, eventually completing his training in Boston at the Massachusetts General Hospital under the mentorship of Dr John Mixter. After his training, Donaghy worked closely with Littmann in Vermont to refine instruments, needles and suture material at the time. 17 Peerless was introduced to Donaghy by Lougheed and travelled to Vermont during his residency training in 1967–1968 to perform further work on small vessel anastomosis in animals with these novel tools. From there, Peerless was introduced to Dr M Gazi Yasargil, who was the first to perform an STA to MCA bypass in dogs during a brief period working in Vermont. 17 Upon completion of his residency, Peerless received a McLaughlin Fellowship grant that allowed him to travel to Zurich to work with Yasargil and Hugo Krayenbuhl, where he applied himself thoroughly in learning the STA to MCA bypass procedure, performing the surgery on numerous dogs from 1968 to 1969. During his time with Yasargil and Krayenbuhl as a fellow at the Konstonsspital Zurich, he spent considerable time in the operating theatre learning from the masters and travelled around Europe to propagate the use of the microscope and microsurgical tools in neurosurgery. Given the massive advances shared by both Donaghy and Yasargil on the development of the small vessel EC–IC bypass, they elected to perform the procedure at the same time in their first human patients with the goal of bypassing occluded carotid arteries. The procedures took place on 30 October 1967 in Zurich, and 31 October 1967 in Vermont and both bypasses remained patent with patients in neurologically stable condition.18,19 The bypass performed by Donaghy remained open until the patient's death 11 years later from complications of heart disease and that performed by Yasargil on a 20-year-old man with Marfan syndrome remained open as confirmed with a good palpable pulsation of the STA years later. Not only did this result in Donaghy being the first to perform a small vessel bypass, but he was the first Canadian to do so. Later on, Yasargil also went on to perform the first bypass for Moyamoya disease in a 4-year-old boy in 1972 with an excellent clinical and radiographic result. 17
After completion of his residency, Peerless planned to return to Vancouver as an attending neurosurgeon, though now with an impressive armamentarium of experience in clinical cerebrovascular and microneurosurgery. Upon his return to VGH in August 1969, Peerless continued practicing STA to MCA bypass on animals in the lab and rapidly sought the tools necessary to instigate the dissemination of microneurosurgery at the institution. He initially borrowed the otolaryngology operating microscope to operate on aneurysms, arteriovenous malformations and vestibular schwannomas, but subsequently acquired a dedicated neurosurgical microscope at VGH in late 1969. As Peerless built out the surgical tools available at VGH, he began working with Dr Stanley Hashimoto to search for an appropriate patient with a carotid occlusion as a potential candidate for small vessel EC–IC bypass. Patient ‘D’ was identified and underwent direct vertebral and carotid punctures for cerebral angiography, as was standard practice at that time. He was found to have 4-vessel occlusion and was ultimately recommended to undergo bilateral STA–MCA bypass, with the left-sided EC–IC bypass performed in October 1969 at VGH and the right side performed 2 weeks later. Peerless fondly recalls that post-operatively, patient ‘D’ no longer experienced transient ischaemic attacks and his cognitive status improved remarkably. His post-operative angiographic studies demonstrated patent bypasses and he ultimately went on to live many years longer. After word of this success spread, Peerless was visited by many patients seeking out small vessel EC–IC bypass as treatment for their cerebrovascular disease.
Small vessel bypass and aneurysm surgery
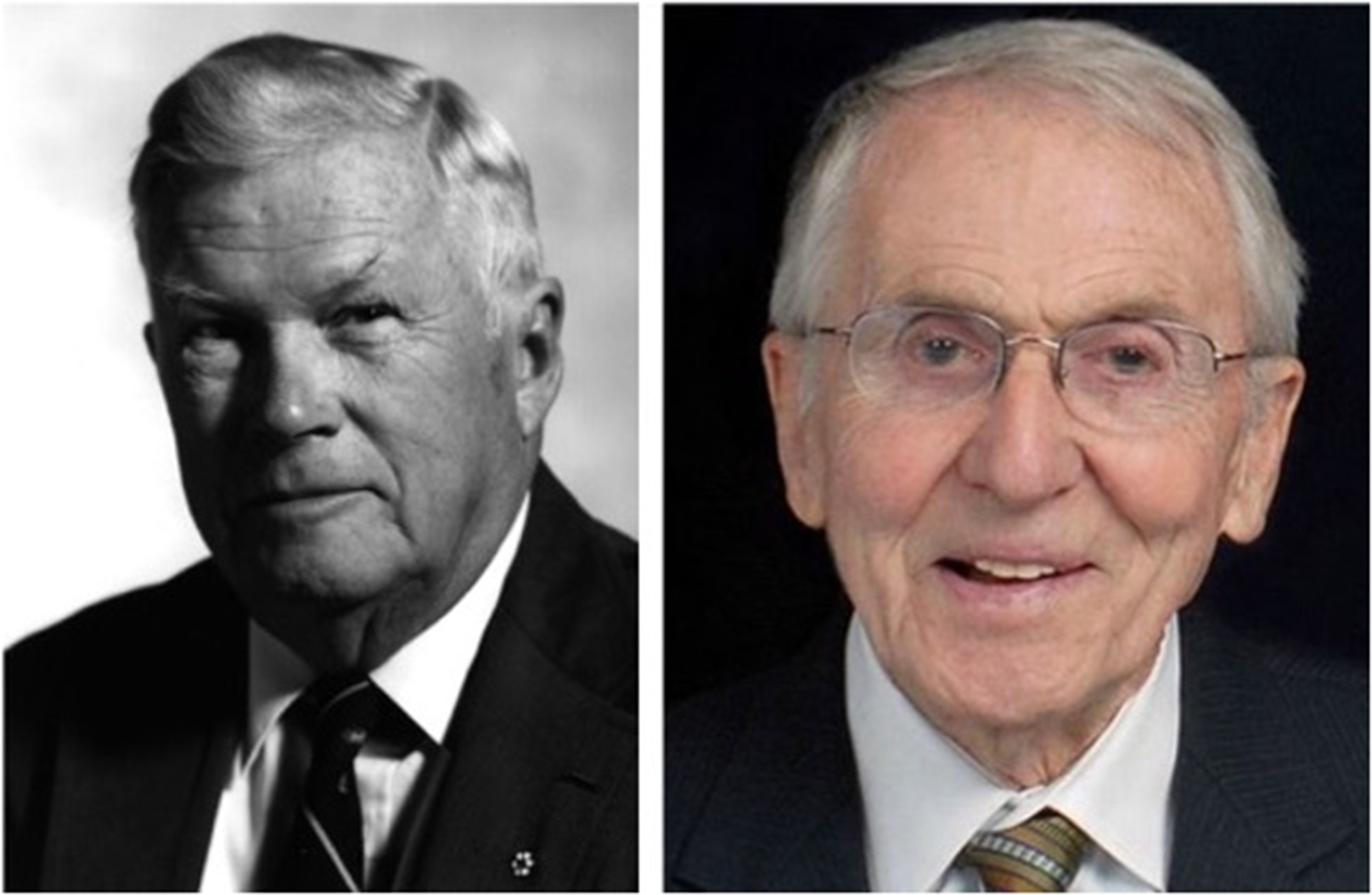
After only a brief tenure at VGH, Peerless was recruited back to the University of Western Ontario in 1975 to work with Dr Charles Drake, a powerhouse of cerebrovascular neurosurgery with a laser focus on the management of posterior circulation aneurysms. The initial focus of his time in London would diverge quite a ways from the management of ischaemic stroke. Within 1 week of arriving in London, Ontario, Peerless and Drake performed a distal EC–IC bypass to the MCA territory with a proximal clip trapping of a giant MCA aneurysm – a technique known as Hunterian ligation.20,21 Peerless and Drake would go on to perform hundreds of these combined procedures for management of both giant anterior circulation aneurysms and even some for posterior circulation aneurysms. The robust patency rates of small vessel EC–IC bypasses performed by Peerless allowed them to revascularize complete territories. Peerless and many other Western-trained neurosurgeons often fondly recount the procedure that married the EC–IC bypass with the Drake microtourniquet, with its first application in 1975. 20 First, a bypass would be performed, and subsequently a microtourniquet would be slung around a proximal vessel intended to be sacrificed for aneurysm treatment, in order to allow precise occlusion to spare branches and perforators. The tourniquet would be fastened through the skin after closure such that a reversible tourniquet occlusion could be performed on the ward. Patients who developed neurologic deficits during the awake vessel occlusion could simply have the tourniquet taken down, or it could remain in situ as a proximal ligation (Figure 3).
Small vessel bypass for ischaemic cerebrovascular disease
Throughout his time in London, Peerless continued work on evaluating the efficacy of bypass for ischaemic cerebrovascular disease in concert with Dr Henry Barnett. Peerless and Barnett felt strongly that procedures in stroke and neurosurgery should be tested and not simply picked up because ‘someone like me goes around saying it's a great operation’, a concept that originated down the highway through David Sackett's work at McMaster University in Hamilton, Ontario. 1 Together, Peerless and Barnett launched an international cooperative study on the use of small vessel EC–IC bypass to evaluate in a randomized controlled manner to determine if a direct revascularization procedure would reduce the rate of subsequent stroke in patients with recent hemispheric or retinal strokes as compared to best medical management (daily aspirin and hypertension management).24–26 After careful design of the trial in concert with David Sackett's group at McMaster, neurosurgeons from far and wide travelled to London to learn small vessel EC–IC bypass for use on patients enrolled in the trial. The procedure was taken up with great enthusiasm; it became so common, with such fixed belief in its efficacy, that it was often being performed in less than optimal patient circumstances. 27 The trial design was considered excellent, 1377 patients were enrolled, and technical execution was monitored, though ultimately the trial was negative and found that the best medical care resulted in fewer strokes than revascularization. The negative results of the EC–IC bypass trial were presented at the World Federation of Neurological Surgeons meeting in Toronto in 1985 to a crowd of surgeons, and significant fallout ensued in the neurosurgical community. 28 The procedure would no longer be covered under insurance along with a firm recommendation against performing bypass for ischaemic cerebrovascular disease.
After much discussion, the trial was ultimately summarized in the modern neurosurgical literature as having included the wrong patients and possibly the wrong surgeons, which sparked a decades-long search for a suitable target pathology in the category of ischaemic cerebrovascular disease. 29 A significant critique of the inclusion criteria was the lack of robust hemodynamic criteria by which patients would be selected, as this did not allow identification of patients who might benefit from revascularization. The Carotid Occlusion Surgery Study (COSS) was published in 2011 and was designed to rectify the shortcomings of the EC–IC bypass trial by including patients with elevated oxygen extraction fractions on positron emission tomography (PET) in the affected hemisphere – a finding of the St Louis Carotid Occlusion Study (STLCOS) that indicated patients had higher risk of ipsilateral stroke.30–32 Despite an effectively run trial with high bypass patency rates, low treatment cross-over and good patient follow up rates, the trial was halted early for futility. COSS demonstrated a reduction in subsequent stroke events after the perioperative period, though the medical arm had a substantially lower risk of stroke than originally hypothesized. COSS was also criticized for being underpowered and for using a less rigorous PET methodology to identify at risk patients than was used in STLCOS.
The Carotid and Middle Cerebral Artery Occlusion Surgery Study (CMOSS) was published in 2023 with the goal of presenting a further refined patient population with stricter operator selection. 33 The trial reported a 6.2% risk of stroke or death in the 30-day post-operative period but ultimately demonstrated improved long-term protection against stroke than medical therapy. However, due to the significant perioperative morbidity and mortality incurred, authors reported no significant difference between the two trial arms. CMOSS was criticized for including patients with less haemodynamic demand, short follow up time period of 2 years, and combining both patients with MCA and internal cartoid artery (ICA) occlusion. 34 MCA and ICA occlusions are separate entities with different flow replacement requirements and critics argue that using the same bypass strategy in both pathologies may not be appropriate. A CMOSS post hoc analysis demonstrated that the MCA occlusion group that underwent bypass had superior outcomes as compared to the medical arm. Overall, ischaemic cerebrovascular disease is a heterogeneous group of pathologies, and a single surgical strategy may not be applicable to all patients. Thirty years of discourse reveals the importance of two factors in managing these patients: identification of perfusion-dependent ischaemia and technical expertise of the surgical team.
Conclusion
After the results of the EC–IC bypass trial were released, Peerless ceased performing bypass for ischaemic stroke given the negative findings of the trial, but he continued to perform the procedure for aneurysm treatment and Moyamoya disease. He would occasionally travel to distant centres to teach EC–IC bypass, though indications began to wane. Over the years, other trials have attempted to demonstrate some benefit of EC–IC bypass in ischaemic cerebrovascular disease indications. While there is significant ongoing criticism and discourse amongst those in the neurosurgical community, many believe EC–IC bypass for ischaemic indications is a question that remains unanswered.29,33,35,36 Those lucky enough to train with Peerless recount that to observe him performing a bypass was to witness mastery – a refined and complex procedure performed with such composure and modesty as if to imply simplicity. Despite the lack of positive findings within a tremendous body of work, the long history of cerebral revascularization surgery demonstrates that significant contributions to the medical world rarely occur in isolation and often arise through immense personal dedication, creativity, and an interdisciplinary spirit.
Footnotes
Acknowledgements
On 10 April 2024, this manuscript was awarded the 2024 Nis Schmidt History of Surgery Prize and was presented at the University of British Columbia Department of Surgery Grand Rounds. The authors thank Dr Nis Schmidt for his unflinching dedication to surgical history and the generous endowment that has made this annual award possible.
Ethical considerations
Informed consent was not required in the production of this study due to the absence of human subjects.
Author contributions
MAR conceived the project, performed the literature review, and drafted the manuscript. SJP provided a historical interview, contributed to and reviewed the manuscript. GJR supervised the project, contributed to and reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.