
Abstract
Robert Lawson Tait was an original thinker, a surgical innovator, a controversialist and an iconoclast. He made important contributions to surgery, was an eloquent supporter of Darwinian evolution and women in medicine and opposed vivisection. He is probably best remembered for his high-profile opposition to Listerian antisepsis which continued until his death. While Lister went on to receive the country's highest honours and was lauded throughout the world, Tait received much more modest honours and little subsequent recognition by historians. Yet it could be argued that Tait's system rather than Lister's was the basis of modern aseptic surgery. Tait never changed his views on asepsis over his lifetime and relied on surgical cleanliness, which, combined with his extensive clinical experience, enabled him to achieve outcomes as good or better than with antisepsis. By contrast, Listerism evolved over 30 years, claimed to be based on laboratory data and adopted the new discoveries of the germ theory of disease as they emerged. We compare the systems of Tait and Lister, explore the basis of Tait's opposition to Listerian methods and conclude that Tait's thinking underlies modern surgical practice and that he should receive greater acknowledgement for his contribution to the prevention of surgical infections.
Keywords
Introduction
Robert Lawson Tait (1845–1899), an innovative surgeon who made a series of notable contributions to gynaecological surgery, was a controversial figure in his lifetime. At a time when obituarists tended to use coded euphemisms to describe less favourable character traits, his obituary in the British Medical Journal candidly described him as ‘unconventional … aggressive … a born fighter who revelled in the joys of conflict’ and noted his ‘want of respect for age or authority’. 1 He was a prolific writer of articles and of letters, exchanging some 120 letters with Charles Darwin (1809–1892) alone and writing almost weekly to medical journals. Tait became one of the most vociferous opponents of Lister's antiseptic system, relying instead on absolute cleanliness and haemostasis to achieve his impressive results.
Lister achieved almost messianic status while Tait received little in the way of honours in his lifetime and little credit for his achievements after his death. 2 Yet in many respects, it was Tait's principles, system and thinking rather than Lister's that led to the aseptic surgical practice still in use today.
The aims of this article are to compare the techniques of Tait and Lister, explore the basis of Tait's opposition to Listerian methods, to examine the evidence for his alternative approach and to compare these to the aseptic techniques subsequently adopted and in use today.
Tait's early life and influences
Tait's life has been extensively documented elsewhere.3–6 He was born in Edinburgh, gained a bursary to George Heriot's School and went on to matriculate at the University of Edinburgh in 1859 at the age of 14, a common age for bright students to enter universities in Scotland at that time. The following year he transferred from Arts to Medicine and in 1862 transferred again to the Edinburgh Extramural School of Medicine, whose courses led to the Licentiateships of the Edinburgh Medical Royal Colleges. Tait was taught by the Professor of Surgery James Syme (1799–1870) and would later recall his respect for Syme's surgical dexterity and his clean and meticulous surgical technique. 7 In 1866 Tait qualified LRCSEd, LRCPE, the dual Collegiate Licentiateships, (Figure 1) then spent a year as an assistant in a country practice in Bathgate, almost certainly recommended by the Professor of Midwifery James Young Simpson (1811–1870), who kept close contact with the West Lothian town of his birth. 6 Tait made much of his early association from student days with Simpson, although this may have been exaggerated. 8 Tait's publications from this time included a paper in which, newly qualified and aged only 21, with characteristic tartness, he suggested that Colles’ description of the wrist fracture bearing his name was wrong and that the fracture was ‘not entitled to have Professor Colles name attached to it’. 9 In 1867 Tait was appointed resident surgeon to the small Clayton Hospital in Wakefield, the year Lister published his first articles on antisepsis.
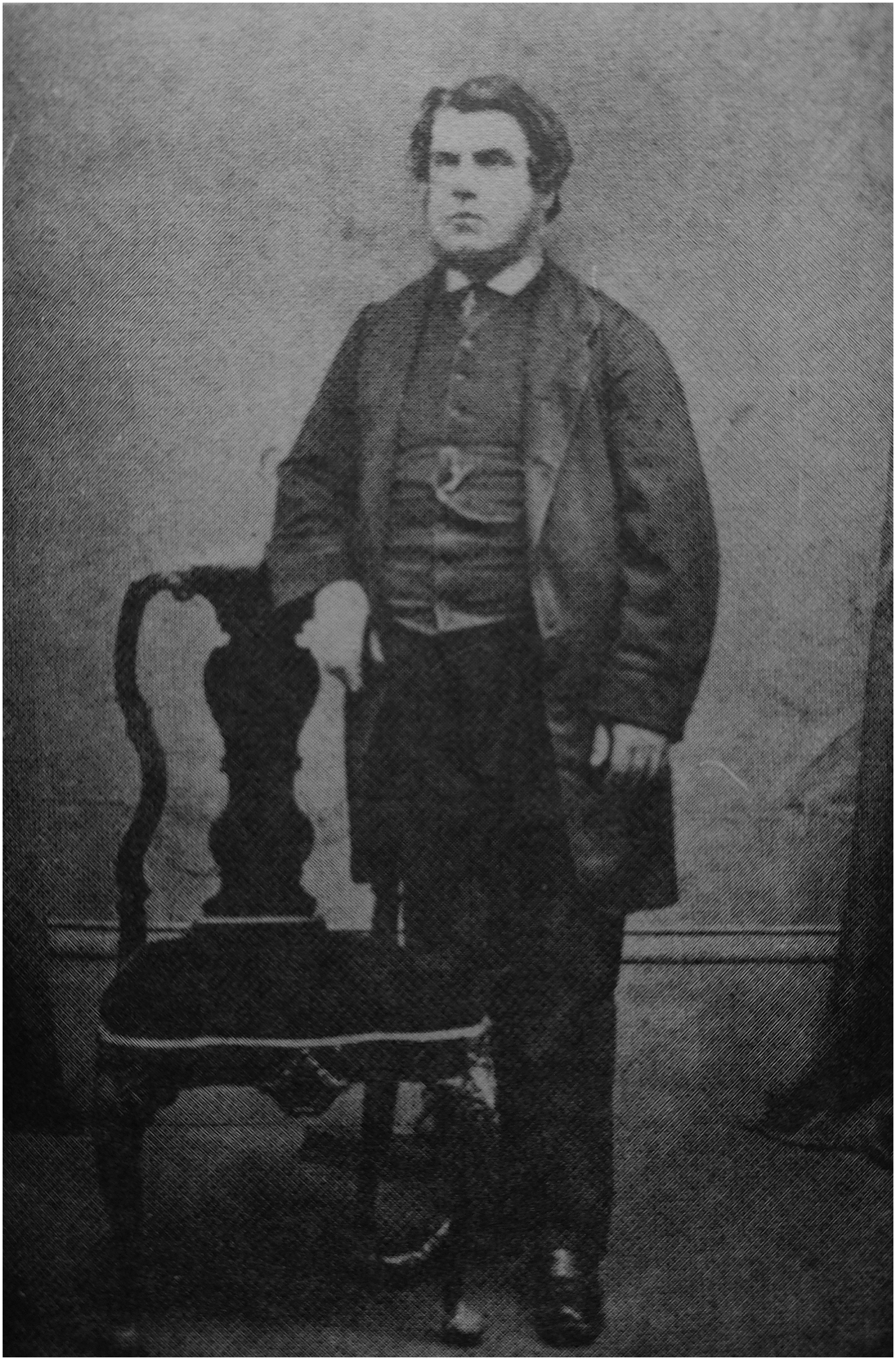
Lawson Tait as a student in Edinburgh c.1866.
The influence of James Syme – cleanliness and cold water
While Syme did not directly address the issue of pre-operative preparation in articles or in his textbook Principles of Surgery, 10 his long-term assistant Alexander Peddie (1810–1907) recorded that he was ‘most strict in the observance of cleanliness as regards instruments, sponges and hands’. 11 Tait would later recall that Syme ‘was always washing his hands. I think I may say he washed them every time he touched a patient. His assistants had to be like him, and his old-fashioned nurses were noted for their tidiness and cleanliness everywhere’. 7 Syme's practice of surgical cleanliness and meticulous haemostasis to prevent infection was taken on to spectacular effect by another of his pupils who would in turn influence Tait. Thomas Keith (1827–1895) had been Syme's house surgeon and had adopted his cleanliness regimen and went on to achieve very low mortality after ovariotomy. 12 Syme could be regarded as the progenitor of the ‘cleanliness and cold water’ school of surgery. Yet Syme's later advocacy of Listerian antisepsis caused Tait, with customary acerbity, to denounce him as ‘a profoundly unscientific surgeon, whose researches were as badly conducted as they were useless …’. 2
The influence of James Young Simpson – Haemostasis, hygiene and hospitalism
By far the greatest influence on Tait from his student days onward was, James Young Simpson, who had introduced chloroform into clinical practice and enjoyed international status in his speciality. Tait attended his lecture course in 1863 and Simpson thereafter took a keen interest in this bright, enthusiastic student, and became a lifelong, loyal supporter through all the controversy which Tait would generate. In 1865, while still a student, Tait published the results of his first and only animal experiments, which were on acupressure, a technique of surgical haemostasis advocated by Simpson. 13 Simpson believed that meticulous, absolute haemostasis was an important factor in the prevention of surgical fever, as blood left in the operative field or wound could lead to infection. He reasoned that acupressure, a technique of compressing blood vessels with needles, could achieve this without using ligatures which were known to cause local inflammation. Tait's animal experiments supported this and concluded (wrongly as it turned out), that acupressure was safe and effective. 13 While Tait abandoned acupressure, he continued throughout his career to strive for careful haemostasis, one of the factors in his later surgical success.
Simpson had an early interest in the causes and prevention of puerperal fever and surgical infection. He was familiar with the 1795 Treatise on Puerperal Fever, by the Aberdeen man-midwife Alexander Gordon (1752–1799), 14 who had clearly shown in a careful epidemiological study that puerperal fever could be transmitted from patient to patient by their medical attendants. He reasoned that it was a ‘specific contagion or infection’ transmitted by ‘putrid particles’ and that transmission could be lessened by burning the clothing and bedding of affected patients. ‘I had evident proofs of its infectious nature’ he wrote in 1795 ‘and that the infection was as readily communicated as that of smallpox, or measles’. Crucially Gordon advised that medical attendants should wash and fumigate their clothing after treating an infected patient.14,15 Simpson was also aware of the work of Ignaz Semmelweis (1818–1865) in Vienna, whose study, first published in 1847, had suggested that washing hands in chlorinated water could reduce transmission of puerperal sepsis. 16 Simpson was struck by the similarities between puerperal and surgical sepsis. In an 1850 article, he observed that of those surgical patients who died, the majority did so, not from an operative error or blood loss, but from a post-operative febrile illness. 17 He went on to suggest that this was caused by a specific ‘morbid agent’ similar to smallpox and measles, which entered through the surgical wound and could ‘poison’ the bloodstream. This led Simpson to embark on what would be the last of his great causes ‘hospitalism’. In 1869 he published the first of a series of papers in which he argued that overcrowding and poor hygiene in large hospitals resulted in greater hospital infection. 18 To test this hypothesis he carried out a survey of mortality after amputation of over 2000 patients in British teaching hospitals and compared them to the results of amputations performed in country practice. He found that in the rural group only one out of nine patients had died compared to one out of three in the urban hospitals. 18 Simpson (Figure 2) began a campaign to have hospitals built smaller, with greater spacing between beds and wards to reduce overcrowding. 18 That idea would later be given further impetus by the Victorian Sanitary Movement and by Florence Nightingale (1820–1910). But the surgical world at that time was more interested in another series of papers on preventing surgical infection published just two years earlier. These were destined to bring antisepsis into surgical practice but generated controversy and sparked Lawson Tait's lifelong opposition. The author was Syme's son-in-law, the newly appointed Professor of Surgery in Glasgow, Joseph Lister (1827–1912).
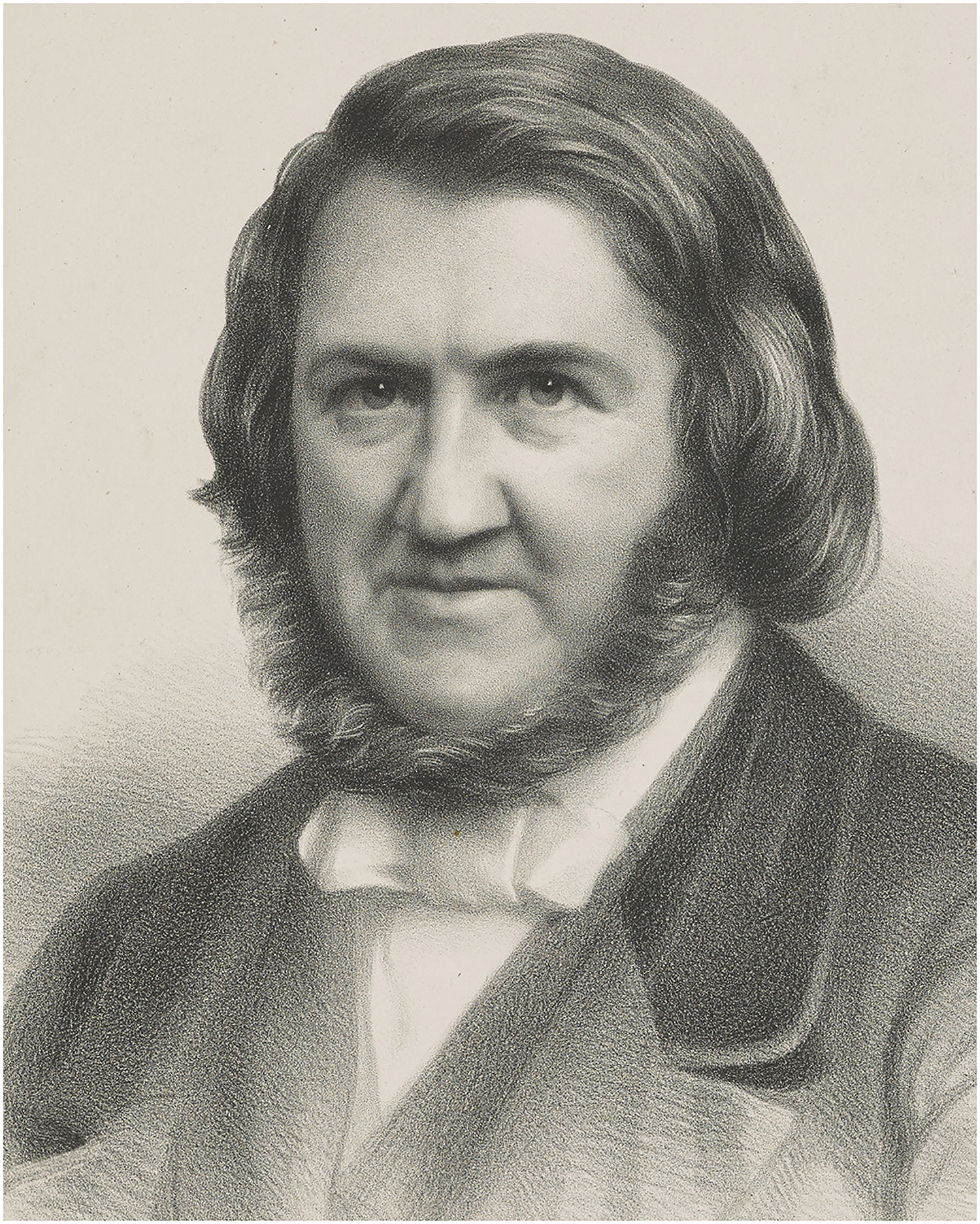
Sir James Young Simpson. Image courtesy National Galleries of Scotland.
Joseph Lister – antisepsis and controversy
Lister had come to Edinburgh as a young surgeon in 1853 to study under Syme, intending to stay for only a few weeks but remaining for seven years (Figure 3). Lawson Tait began medical studies in Edinburgh as Lister left for the surgical chair in Glasgow and there is no evidence that they ever met. 6 As Syme's house surgeon and assistant Lister would have been exposed to Syme's cleanliness regimen, yet he does not emphasise cleanliness or hand washing in his early papers on antisepsis. Stimulated by Louis Pasteur's (1822–1895) flask experiments, which concluded that fermentation of beer, wine and milk was caused by micro-organisms in the air, Lister repeated them and reasoned that suppuration, putrefaction and animal and human infection might also be caused by ‘septic germs’ in the air. 19 Although at this stage there was no laboratory, or indeed any scientific evidence to support this in humans, Lister and his supporters made much of this ‘scientific basis’ on which ‘the germ theory of putrefaction’ and antiseptic practice had been founded. Yet the only conclusions that could be drawn from Pasteur's 1864 experiments and Lister's repetition of these the following year, was that germs in the air could ferment wine, beer and milk. Although the laboratory proof that microbes caused putrefaction was still to come, Lister in 1868 described ‘the germ theory of putrefaction’. 20
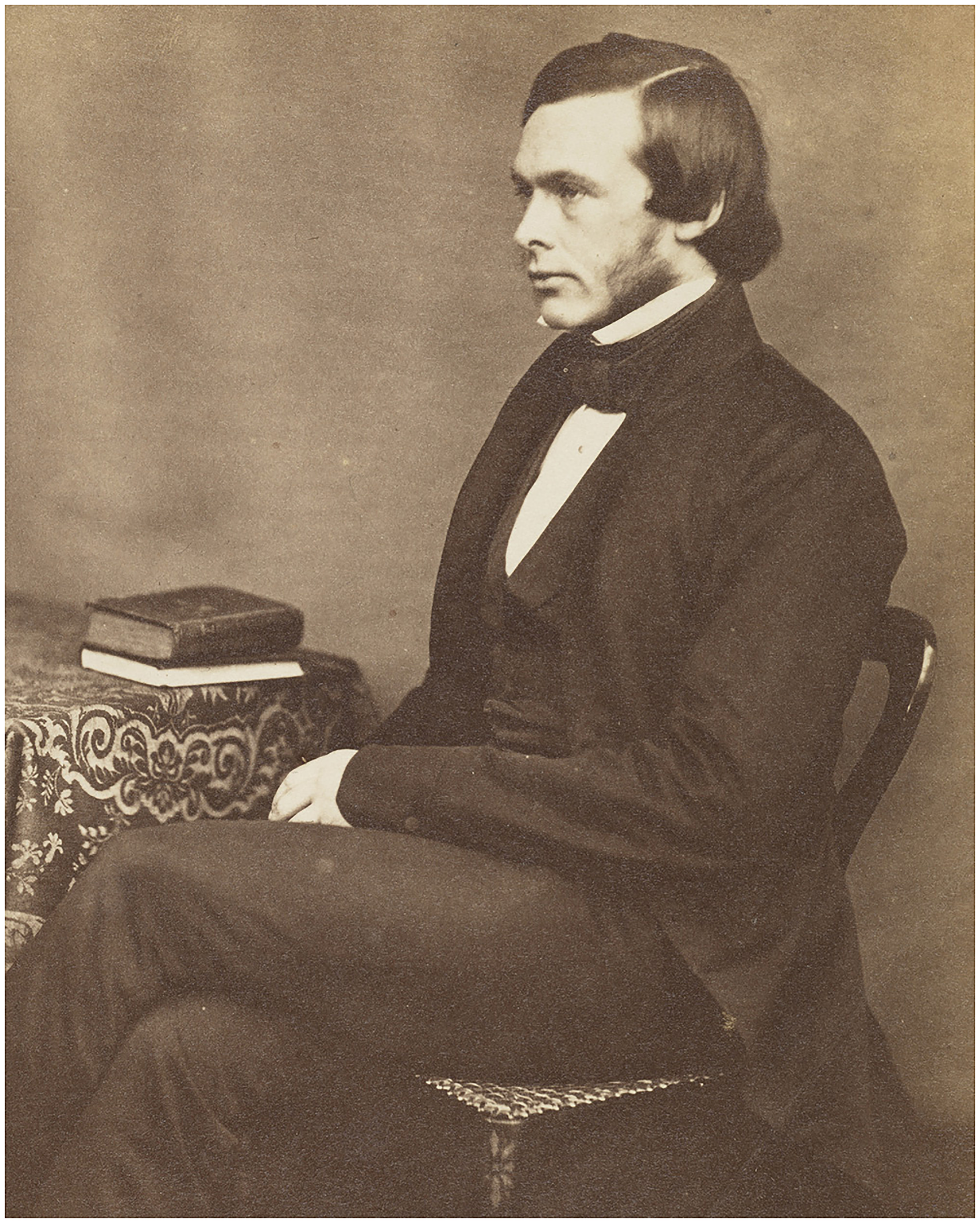
Joseph Lister as a young surgeon in Edinburgh c1855. Image courtesy National Galleries of Scotland.
Lister's goal was to kill the germs in abscesses, compound fractures and amputation wounds and he aimed to achieve this ‘by applying a dressing of material capable of destroying the life of the particles’. Lister used carbolic acid (phenol), a derivative of coal tar, after this was suggested to him by Thomas Anderson (1819–1874), Professor of Chemistry at Glasgow University. Lister later applied carbolic acid to surgical wounds, with the aim of preventing germs in the air from reaching the wound, by means of a multi-layered carbolic dressing. As the technique evolved, he experimented with dilutions of carbolic acid and with various wound coverings to retain the antiseptic liquid or paste in situ and reduce evaporation. These included lint, oiled silk, gutta percha, thin lead sheet, block tin, lacquer and plaster, resulting in dressings with up to eight layers.20,21 In January 1868, Syme gave a powerful endorsement of Lister's system calling it ‘the most important improvement in surgical practice in recent times’. 22 Lister's ‘system’ continued to evolve with the antiseptic spray (abandoned after some ten years) and the addition of wound drapes soaked in the carbolic solution. 23
Lawson Tait – An early critic of Listerism
Lawson Tait was among Lister's early critics, reporting that ‘in twelve compound fractures … the only cases where suppuration did occur were two in which I employed the acid paste exactly as recommended by Mr Lister’. 24 He later wrote that in his early years ‘Lister had no more faithful disciple, no more devoted follower … I spent my days with my hands soaked in carbolic oil, making carbolic putty … I carried it [Listerism] out more scrupulously than the master himself’. 25 Tait's alternative approach was based on the cleanliness advocated by Semmelweis and by Simpson. ‘Destroy the germs on the hands of those who attend parturient women, and the women are safe’ Tait wrote ‘let the physicians and students … wash hands and instruments in a solution of corrosive sublimate [mercuric chloride] each time before touching the patients, and these women seem to be absolutely free from danger’. 26 Sir John Eric Erichsen (1818–1896), Professor of Surgery at University College, had employed a young Joseph Lister as his dresser and went on to write extensively about antisepsis. Erichsen saw this handwashing and cleanliness in obstetrics as the origin of aseptic surgery. ‘Surgery is most indebted to obstetricians for great improvements in general surgery’, he wrote ‘for it is to them we owe the great precautions which independently of Listerian or antiseptic method, tended to lower the mortality of surgical cases’. 27
On the other hand, Lister, if he was aware of the writing of Alexander Gordon (1752–1799), of Oliver Wendell Holmes (1809–1894), or even of Semmelweis, did not include them in his ‘system’. Lister wrote in great detail about the minutiae of the dressings, their composition and handling and the timing of dressing changes as his system evolved. By contrast, he gave little mention to hand, instrument or skin washing. Lister continued to operate in the traditional soiled frock coat and, in marked contrast to the cleanliness school, he did not seem particularly concerned with ward cleanliness. Indeed in 1870, as a result of the success of antisepsis, he had ‘relaxed my former vigilance regarding the wards’. 28 He went on to abolish the annual cleaning of his wards, proudly claiming that ‘it is now three years since any cleaning took place on these wards of mine’. 28 Lister wrote in 1871 ‘If we take cleanliness in any other sense than antiseptic cleanliness, my patients have the dirtiest wounds and sores in the world’. 29 Thomas Schlich comments that this shows that Lister was totally committed to the concept of the germ theory and that neither improved ventilation, nursing hygiene nor hospital cleanliness were relevant because it was antisepsis that had reduced the rate of pyaemia, erysipelas and hospital gangrene. Everything else was of trifling consequence compared to antisepsis. ‘This opinion of the vital importance of Listerism’ wrote Schlich ‘helps to understand why so many British surgeons rejected Lister's conceptual switch and criticised his narrow views’. 30
Ovariotomy: Paving the way for surgery of body cavities
While controversy continued about the effectiveness of Listerism, another contentious operation was emerging which would further focus arguments between chemical antisepsis and cleanliness. Giant ovarian cysts were debilitating and life-changing and early attempts to excise them had resulted in high mortality. Thomas Spencer Wells (1818–1897) began performing the procedure in 1858 in the small Samaritan Hospital in London and laid great importance on ‘thoroughly cleansing, painting, and lime washing the wards’. 31 He believed, like Simpson, that surgery in small hospitals resulted in reduced mortality and he emphasised good ventilation in wards and theatres. Wells also advised that observers in theatre be kept to a minimum, that these should not have been in contact with infectious patients and there should be little talking during operations. Although his first hundred ovariotomies had a 34% mortality rate, Wells persisted and after 500 cases his mortality had reduced to 21%. 32
Encouraged by Simpson, Thomas Keith (1827–1895) in Edinburgh began performing ovariotomies in 1862 having seen the technique used by Spencer Wells. By keeping detailed records of each patient, Keith produced accurate results, recording the lowest mortality published to date in the world literature. 33 Keith was very much of the cleanliness and cold water school, although initially he also used antiseptic wound dressings, firstly the tar bags used by Spencer Wells and subsequently Listerian antiseptic dressings, which he later abandoned, reverting to ‘boiled water and soda’.12,34 From the outset Keith published detailed case reports in the Edinburgh Medical Journal 34 and summaries in The Lancet of every 50 cases, each with a table of the outcome in individual patients. His mortality rate progressively fell from 22% in the first 51 operations to 19% after 101 procedures, with a further fall to 18% after 150 operations 35 and he eventually reported a 4% mortality. 12 J. Marion Sims (1813–1883), a leading American gynaecologist, visited Keith and attributed his success to cleanliness of the operative field, meticulous haemostasis and lavage of the peritoneal cavity with water. 36
Tait's technique and results
With characteristic boldness, Tait began to perform the procedure of ovariotomy in 1868, while still a house surgeon, though his first patient died of peritonitis. Undeterred he continued, reporting a mortality rate of 38% in his first 50 operations, performed ‘with the [carbolic] spray and full antiseptic precautions’.25,26 After abandoning Listerism, Tait embraced meticulous cleanliness as described in an editorial in The Lancet in 1922:
‘He cleansed the skin of the patient with soap and water, and in dirty cases with turpentine; he boiled his instruments and his ligatures; he surrounded his wounds with laundried towels; he took the greatest possible care in the preparation of his sponges; and, above all things, he took the most minute precautions to avoid infection of his hands, and was accustomed to allow some days to elapse after dealing with any septic case before performing an abdominal operation. Indeed, he was a striking example of that super cleanliness which we now know to be the secret of a successful surgery – an aseptic surgeon long before asepsis was generally practised, or the meaning of the term was even understood’. 37
To this Tait added Keith's technique of peritoneal lavage with large quantities of water to ‘cleanse the peritoneum’. In 1886, he was able to report one of the most remarkable series in the history of surgery, 139 consecutive ovariotomies without a single death. 38 He attributed this to small incisions, absolute cleanliness and haemostasis, ligation rather than clamping of the ovarian pedicle, along with copious peritoneal lavage with water. Indeed, his anonymous biographer in Plarr's Lives of the Fellows felt that ‘Perhaps the most original and at the same time most valuable innovation which surgery owes to Lawson Tait is the washing of the peritoneum after an operation’, although credit for this really belongs to Thomas Keith. 39 In recent years, however, doubts have been cast on the effectiveness of this technique. 40
But Tait made other valuable contributions (Figure 4). In 1870, he set up in private practice in Birmingham, with hospital appointments at the small Birmingham and Midlands Hospital for Women and the West Bromwich Hospital and spent the rest of his career in Birmingham. Buoyed perhaps by his early ovariotomy success he felt confident enough to open the abdomen for sepsis, draining a tubo-ovarian abscess in 1872 and performing his first hysterectomy the next year. In 1877, he became the first surgeon to carry out salpingectomy for the disease of the Fallopian tubes (known as Tait's operation). From this developed what many regard as his greatest contribution, emergency laparotomy for ruptured tubal pregnancy, a procedure which has saved countless lives. 41 By 1879, confident enough to expand into other areas of the abdomen, he performed what appears to be the first successful cholecystostomy in 1879, describing it as ‘cholecystotomy’. 42 He was among the first surgeons to perform appendicectomy for acute appendicitis, describing in 1889 the successful removal, on two occasions, of a ‘thickened, swollen and suppurating’ appendix. 43 Tait was a true pioneer of abdominal surgery. William J Mayo (1861–1939) went so far as to suggest that ‘the cavities of the body were a sealed book until the father of modern abdominal surgery, Lawson Tait carried the sense of sight into the abdominal cavity’. 44

Lawson Tait at the peak of his career c.1888. Image © National Portrait Gallery, London.
Between 1872 and 1890 Tait wrote at least 13 articles on antisepsis, which became increasingly critical of the system. 45 He bore no personal animosity towards Lister, describing him as ‘a man who has exercised an enormous influence for good on the progress of surgery during the last, twenty years’ 46 but he derided the theory of Listerian antisepsis. ‘The Listerism of twenty and fifteen and twelve and ten years ago is dead’ he wrote in 1891. ‘Each wave of altering principle and different detail killed the wave in front of it until the only logical conclusion of the whole business, the spray, has been denounced by its inventor … Those of us who protested … have seen these germicides given up and the success of our "simple cleanliness" admitted on all hands. But then we see the "germicidians" coolly turn round and say "our germicides were only a joke; it was cleanliness we meant all the time"’. 47 In one of Tait's last papers he would claim that ‘at my hands there was no Listerism, no chemical antiseptics, nothing but soap and water’. 48 Tait accepted the existence of microbes, and he accepted Pasteur's work as far as it applied to dead material in the laboratory. Like his mentor Simpson, he advocated small hospitals, kept meticulously clean and well-ventilated with spacing between patients.
But Tait never really changed his original ideas and adhered to the principles of cleanliness advocated by Gordon and Semmelweis in obstetrics and developed in surgery by Simpson, Syme and Spencer Wells. On the other hand both the concept and detail of Listerism changed significantly over the years, by abandoning the carbolic spray, by incorporating the discoveries of Louis Pasteur, Robert Koch (1843–1910) and Rudolf Virchow (1821–1902), and by adapting from the concept of the germ being the cause of putrefaction to the revelation that the germ was the cause of surgical infection.
Lister was criticised by his contemporaries for poor use of statistics in his results. Lister the scientist preferred the application of his laboratory work to clinical practice as recorded in detailed single case histories. In marked contrast Tait collated his results from large numbers of operations, systematically compiling statistical tables and charts. Lister's views however followed that of Claude Bernard (1813–1878), founding father of modern experimental physiology who wrote that statistics ‘revealed absolutely nothing about the mode of action of medicine’. 49 Tait prioritised his clinical experience over that of laboratory evidence produced by Lister and relied on probabilities, including the variation in patients; such as their condition, nutritional status, the environment and whether the patient suffered from other medical conditions. 30 Tait's contemporaries of the cleanliness school also produced their own modifications. Notable among these was George Callender (1830–1879) at St Bartholomew's Hospital London, who advocated a system of what he called ‘clinical precision’. Callender considered a multiplicity of causes for septic complications, recognising patient risk factors such as extremes of age, prior illness, co-morbidity and malnutrition. He aimed to improve the patient's pre–operative state with nutrition, iron and tonics. This has been re-emphasised in the twenty-first century as ‘pre-optimisation’. His local wound management consisted simply of cleanliness and irrigation with water or dilute chloride solution, backed up by gentle tissue handling, precise approximation of tissues and absolute haemostasis. In 1878, he reported a remarkable 3.4% mortality for all operations in the hospital.50,51
Subsequent development of aseptic surgery
The progression to asepsis was a gradual one with several individuals making contributions. William Macewen (1848–1924) in Glasgow wore a laundered gown, devised instruments made from single pieces of steel and boiled these in a fish kettle, gradually discarding carbolic completely.
Curt Schimmelbusch (1860–1895) in Berlin ‘sterilised’ dressings and towels in water heated under pressure in what was a forerunner of the steam autoclave. Gustav Neuber (1850–1932) in Berlin introduced the surgical cap and sterile gown and designed operating theatres in a way that allowed the walls and floors to be washed down. In 1889 William Halstead (1852–1922) in Baltimore introduced surgical gloves, initially to protect the hands of surgeons and nurses from the irritating effects of carbolic acid or mercuric chloride used to sterilise operating instruments. In 1897 in Germany Johannes von Mikulcz-Radecki (1850–1905) started to wear a face mask. A study of photographs of surgeons in theatres showed that by 1923 more than two-thirds wore masks and by 1935 most did. 52 The principles of aseptic surgery have continued to evolve. Ventilation in theatres improved following the seminal work by Blowers in 1968. 53 The role of sterilisation in the operating theatre was updated by Kelsey in 1969 54 and the introduction of clean air systems by John Charnley (1911–1982) further reduced the risk of intraoperative infection.55,56 These developments have relied almost exclusively on physical rather than chemical methods.
Lister and Tait compared
Despite the accolades received by Lister, antisepsis was widely criticised at the time and was never accepted by some. Yet the principles of asepsis, beginning at much the same time, more radical and more difficult to implement, were quietly accepted into surgical practice with little opposition. 57 Why was this? Absolute cleanliness lies at the heart of modern aseptic technique rather more than chemical disinfection.
Moreover, Tait's view of scientific evidence is arguably more in accord with modern thinking than Lister's. As Greenwood observed ‘The values of visual evidence, exactness, thoroughness, statistical evaluation, and specialisation, all of which Tait fervently insisted his science stood for, are exactly the values embraced by the present concept of science’. 2
So why is Lister revered rather than Tait?
Perhaps the contrasting personalities of the two men was a factor.
Tait was a cigar-smoking bon viveur who loved alcohol, used coarse language, was short tempered, aggressive and iconoclastic. He was a supporter of then controversial causes like specialism in medicine, Darwinism, women in politics and medicine, Irish independence and was a fierce opponent of vivisection. These principles created enemies and may have dissuaded many surgeons from accepting his views on surgical hygiene. As a result of a paternity suit and a libel action later in life, he lost much of his authority, his wealth and influence. 6 Also Tait was an individualist who did not change his views on asepsis over his lifetime nor, unlike Lister, did he inspire a coterie of student followers and disciples.
By contrast, Lister was courteous, quietly spoken and retained the Quaker habit of addressing using ‘thee’ and ‘thou’. 58 He had a large body of admiring followers among former students, dressers and house surgeons who introduced his system around the world. They downplayed asepsis, characterising it merely as a refinement of Listerian antisepsis. 59 Moreover Lister never accepted asepsis, but he adapted his views over the years bringing in the work of Pasteur, Koch and others. In 1908, when aseptic practice had been adopted in many British hospitals, 57 Lister wrote ‘It has grieved me to learn that many surgeons have been led to substitute needlessly protracted and complicated measures [asepsis] for means as simple and efficient [as antisepsis]’. 60
Tait was frequently described as an opponent of germ theory, yet he accepted Pasteur's conclusion that air carries germs which cause putrefaction. His error was that he believed this occurred only in dead tissue, not in living. 26 He believed that before operating the surgeon should not ‘perform any post-mortem examination or dissection, nor handle any patient suffering from purulent infection’. 61 Like Callender he stressed the additional importance of patient and environmental factors in causation of post-operative infection.
Lister rejected the concept of cleanliness in surgery. John Leeson, who worked under him in Edinburgh, reported that his theatre ‘was grimed with the filth of decades. I suppose it was occasionally cleaned, but such process was never in evidence. The operating table looked as if it was never washed …. No one dreamed of washing his hands before starting work’. 58
Koch showed that carbolic acid was not a particularly effective germicide and that mercuric chloride (used by Semmelweis) was better at destroying ‘the most resistant organisms in a few minutes by a single application of a highly dilute solution’. 62 Lister subsequently adopted mercuric chloride as an antiseptic, again depicting his willingness to embrace new developments which would enhance his system.
Some 30 years after Tait's death, reflecting on his contribution, John Harvey Kellogg (1852–1942) and Franklin Martin (1857–1935) in the USA and Leonard Gamgee (1868–1956) in England, all regarded Tait as the true instigator of aseptic surgery. 8 That though may be too simplistic an analysis. Lawrence and Dixey suggest that this surgical revolution came about not ‘from a single surgical innovation engineered by a small group (the Listerians) but as the accumulation of many small deviations from intellectual and practical routine among the surgical community as a whole.’ 63 We would argue that among the most important of these ‘deviations’ were those practised and promoted by Lawson Tait. Tait never changed his views on asepsis and relied on his extensive clinical experience and manual dexterity to achieve his success, and on clinical observation and statistics to support his case. Listerism evolved over 30 years and, based largely on laboratory data, adopted the new discoveries of the germ theory of disease as they emerged.
Perhaps that is why Lister is still revered while Tait, an original thinker and the most accomplished of surgeons, is largely forgotten. If we accept that "antiseptic" means the use of chemicals to destroy bacteria or prevent their growth while "aseptic" defines physical methods to achieve this aim, then Tait, inspired by Gordon, Semmelweis and Simpson, should enjoy greater recognition for his contribution to modern surgical practice.
Footnotes
Acknowledgements
We are grateful to William Dibb and to David Wright who each read over the manuscript and made many helpful comments and suggestions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.