
Abstract
Sir William Osler espoused a particularly idealized medical life that included the patient in the physician's worldview. Disease is not considered a monolith, only a reflection of one's broader health. Death, too, is configured as a part of one's being, not as a thing apart from life. The wholesomeness that characterized Osler's practice is well known—however, his long discussions and thoughts on death have not been sufficiently analyzed. His clinical views have been hinted at and numerous medical historians have noted that Osler's worldview on death was avant-garde for its time, one in which he described finality not as a time of suffering and anguish, but as “singularly free from mental distress.” This essay contends with this simple view. This straightforward understanding becomes complicated when delving into such primary resources as Osler's Study on Dying cards, his writings on other medical conditions, and personal reflections following the personal losses of his sons Edward Revere Osler and Paul Revere Osler. This essay contends that the loss and the death he imagines is not one of peace, but rather, of horror and terror. Furthermore, the primary sources show Osler not as the paragon of flawless clinical acumen and reasoning, but a man of personal beliefs that were in conflict with views he espoused more publicly. The essay therefore reconceptualizes the common understanding of a stoic Osler, determines how death prefigures into Oslerian thought, and challenges the idea of an Oslerian simple death.
Keywords
Introduction
The Principles and Practice of Medicine by Sir William Osler (1892) is a testament to a mode of living. In between descriptions of individual diseases and the pillars of bedside skills that revolutionized medical practice, Sir William Osler espoused a particularly idealized medical life that necessarily includes the patient in the physician's worldview. 1 Disease is not considered a monolith, only a reflection of one's broader health. Death, too, is configured as a part of one's being, not as a thing apart from life. Against the backdrop of a burgeoning biomedicine and an exposition on the state of late 19th century medicine, the book details the end of life as not simply a pathological and physiologic process of dying, but a lifestyle of each illness and its course.
The wholesomeness that characterized Osler's practice is well known—however, his long discussions and thoughts on death have not been sufficiently analyzed. His clinical views have been hinted at and numerous medical historians have noted that Osler's worldview on death was avant garde for its time, 2 one in which he described finality not as a time of suffering and anguish, but as “singularly free from mental distress.” 3
This essay contends with this simple view. This straightforward understanding becomes complicated when delving into such primary resources as Osler's Study on Dying cards, his writings on other medical conditions, and personal reflections following the personal losses of his sons Edward Revere Osler and Paul Revere. Osler, known for his pin-point accuracy and calm demeanor, seems helter-skelter in bereavement when consumed by pain and anguish, and displays an unprecedented vulnerability. This essay contends that the loss and the death he imagines is not one of peace, but rather, of horror and terror. Furthermore, the primary sources show Osler not as the paragon of flawless clinical acumen and reasoning, but a man of personal beliefs that were in conflict with views he espoused more publicly. The essay therefore reconceptualizes the common understanding of a stoic Osler, determines how death prefigures into Oslerian thought, and challenges the idea of an Oslerian simple death.
Victorian conception of death
The 19th century saw major changes in western conceptions of death. Romanticized views were popular in the 18th century and death was considered “familiar and tamed,” 4 something that was “the true goal of existence.” 5 This transition coincided with the growth of heavy industry and consequent shifts in understanding. Stanley Reiser's Medicine and the Reign of Technology maintains that by learning about the patient's body through technology, the patient became abstracted, operationalized, and technically centered. 6 Physiology translated into “the language of machines” and the doctor became an “operator.” 7 While this shift away from a romantic abstraction of death to a specific, observable locus of disease vastly increased the capabilities of therapeutics and diagnostics, medicine, and altered the language it used, it separated the body from the person. Medicine became an act of elucidating specific symptoms by viewing the aberration of clinical signs and values compared with the norms and averages.
This culture of mechanization meant that death was something to be averted, particularly by medical means. It became a fearful event, a taboo dealt with through euphemism and indirectness. 8 The physician's role therefore reflected this larger culture. Where the physician was once described religiously—“as a minister of health” and “steward of the body”—he became secularized, cold, and calculating. 9 The same can be said of the discourse surrounding the dying patient, who, as H. S. Berliner noted, was “for the use of statistical assumptions” and scrutinized by paradigmatic thinking which saw humans unrelated to their surroundings, as objects to be manipulated by instruments, even in death. 10 There was to be a “good death,” 11 one that would be fought against, and if not, assuaged from its horror. Thus, the language of biomedicine and death became neutralizing in its vocabulary, explanatory in its use, and distancing in its conception of humanity.
Osler's antithesis of fear
Osler was born into a minister's family. His father, Featherstone Lake Osler, served as an Anglican missionary, and Osler himself studied divinity at Trinity College for a year. Much of this religiosity surfaces in Osler's writings, for example, describing medical work as “the missionary spirit with a breadth of charity.” 12 He further saw scientific medicine as a single component of a larger equation of life and death, one where religion prefigures but does not necessarily dominate:
He cannot but feel that the emotional side to which faith leans makes for all that is bright and joyous in life. Fed on the dry husks of facts, the human heart has a hidden want which science cannot supply; as a steady diet it is too strong and meaty, and hinders rather than promotes harmonious mental metabolism. 13
It is this “hidden want” and understanding that “science cannot supply” that sees Osler define disease and death differently from the common conceptions of his century. By means of both science and arts, as a humanist of deep reading and constant curiosity, Osler considers medicine's ultimate goal to deter an “iciness” he saw in oncoming residents both at John Hopkins and Oxford in the late 19th century. 14 In his openness to medicine's expansive domains in art and the humanities, Osler expressed a belief that medicine was, as Erasmus stated, a “divine science.” 15 It requires a total compassion, an intricate belief in care and hope.
Therefore, Osler's conception of death became equally holistic. Aging was a “slow descent into dull oblivion,” 16 and rather than dichotomize, he integrated death as a peaceful transition, both in clinical means and endings. “We speak of death as the King of Terrors,” he says in Canadian Medical and Surgical Journal, “yet how rarely does the act of dying appear to be painful, how rarely do we witness agony in the last hours.” 17 Furthermore, even in his earliest clinical encounters at the Montreal General Hospital, he displays this holistic paradigm:
About 12 o’clock I heard him muttering some prayers, but could not catch distinctly what they were God the Father, Son and Spirit. Shortly after this he turned round and held out his hand, which I took, & he said quite plainly, Oh thanks. These were the last words the poor fellow spoke… From 12.30 he was unconscious, and at 1.25 a.m. passed away, without a groan or struggle. 18
Osler is a familiar figure here: a man of equipoise and careful consideration. He sees the patient totally, and watches life in its totality as well. His religiosity is evident, as is his view on death as a part of life, one that goes “without a groan or struggle.” Death is calmly intimate, symbolic, where there is sincere concern for the centrality of human value at the end as necessitating dignity, worth, and empathy. It is not a fearful thing to be combated, but rather, slipped into naturally as an often quickly experienced, lasting sleep. As Osler simply summarized, “call no man happy until he dies.” 19
Osler's clinical contradictions
Close readings of Osler's work provide some counterpoints to this somnolent, artful death. In lectures on Angina Pectoris and Allied States, he states that “a man in full health, in the prime of life, may be seized… and die within a few hours,” later adding that “for no man suffers the anguish of a severe paroxysm of angina without a consciousness of the nearness of the Angel of Death.” 20 He further adds that the agony is terrible, where one is “unable to stir until the agony has passed off.”
Other conditions such as pneumonia, to which Osler himself succumbed, is described by Osler near his death as, “encouraging… no actual pain.” 3 However, this is similarly complicated by his greater clinical work. While originally called “a friend of the aged,” Osler notes that pneumonia includes “cold gradations of decay” that are “distressing to himself and his friends.” 21 Even in his own death, he faced some conflict where, between painful bouts of coughing, he wished to “shunt the whole pharmacopoeia, except opium… what a comfort it has been.” 22
These conflicts are plainly highlighted in his Study of Dying cards. Done at John Hopkins Hospital in 1900–1904, the cards make observations of 486 dying patients.23,24 While there is no consensus on why the cards themselves were begun, there is opinion that they were started because Osler disagreed with the poet Maurice Maeterlink. Maeterlink, like many at the time, discussed death as a thing of great anguish and physical pain. 25 Meanwhile, Osler worked in the ideals of humanism as a means to ameliorate fear and loathing of the dead and dying.
The cards themselves note the act of dying, with “coma or unconsciousness before death,” and whether “there is any fear in body, mental, or spiritual.” 24 Osler gave reports on the findings, as well as the tallies, to staff at the hospital, and there was a separate official spreadsheet accounted in the Hospital itself. Mueller notes that the majority were signed by nurses (258, 60%), with none signed by Osler himself.
Still, there are non-subtle discrepancies. 340 (70%) deaths were recorded by Osler as sudden. Yet discomforts (such as physical, mental, or spiritual) were lower when recorded by Osler (104) versus when analyzing the cards primarily (157). Additionally, Osler did not note any discomfort in a second domain, compared to Mueller who noted 29 s domain pains recorded when analyzing the cards themselves. 23
Furthermore, analyzing the fonds (Figures 1 to 5) themselves show a death that is hardly “without groan or struggle.” 18 People “call out loudly,” 16 they “suffer from shortness of breath,” 26 they have “extreme tenderness of entire body,” 27 they die in agonal breathing with “gasps of respiration,” 28 they suffer from “dyspnea,” 28 “severe bodily pain,” 29 and a fear of death permeates, where in terror, patients ask “Am I dying?” 28
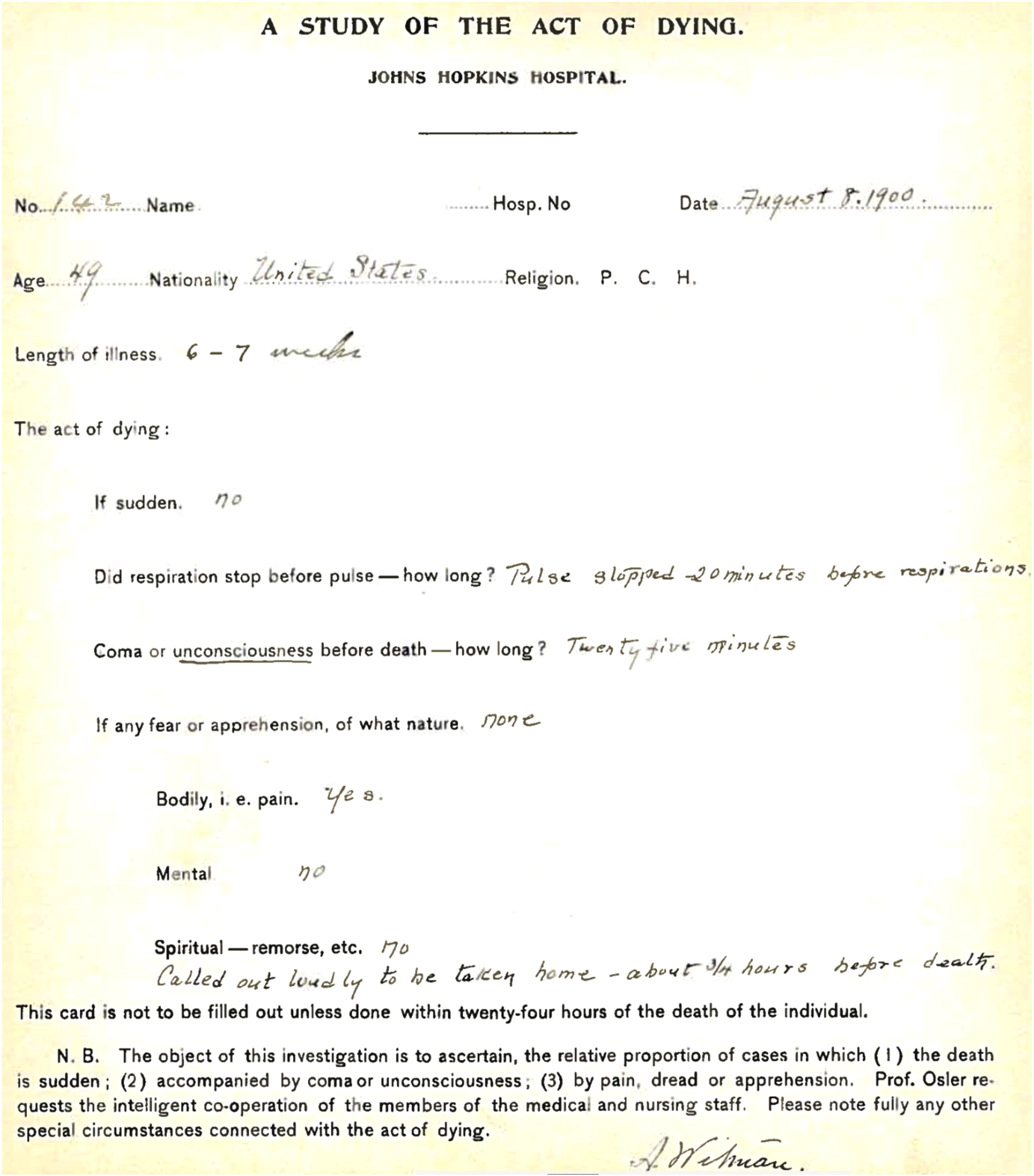
Study of Dying Card 142: “Called loudly.” 16
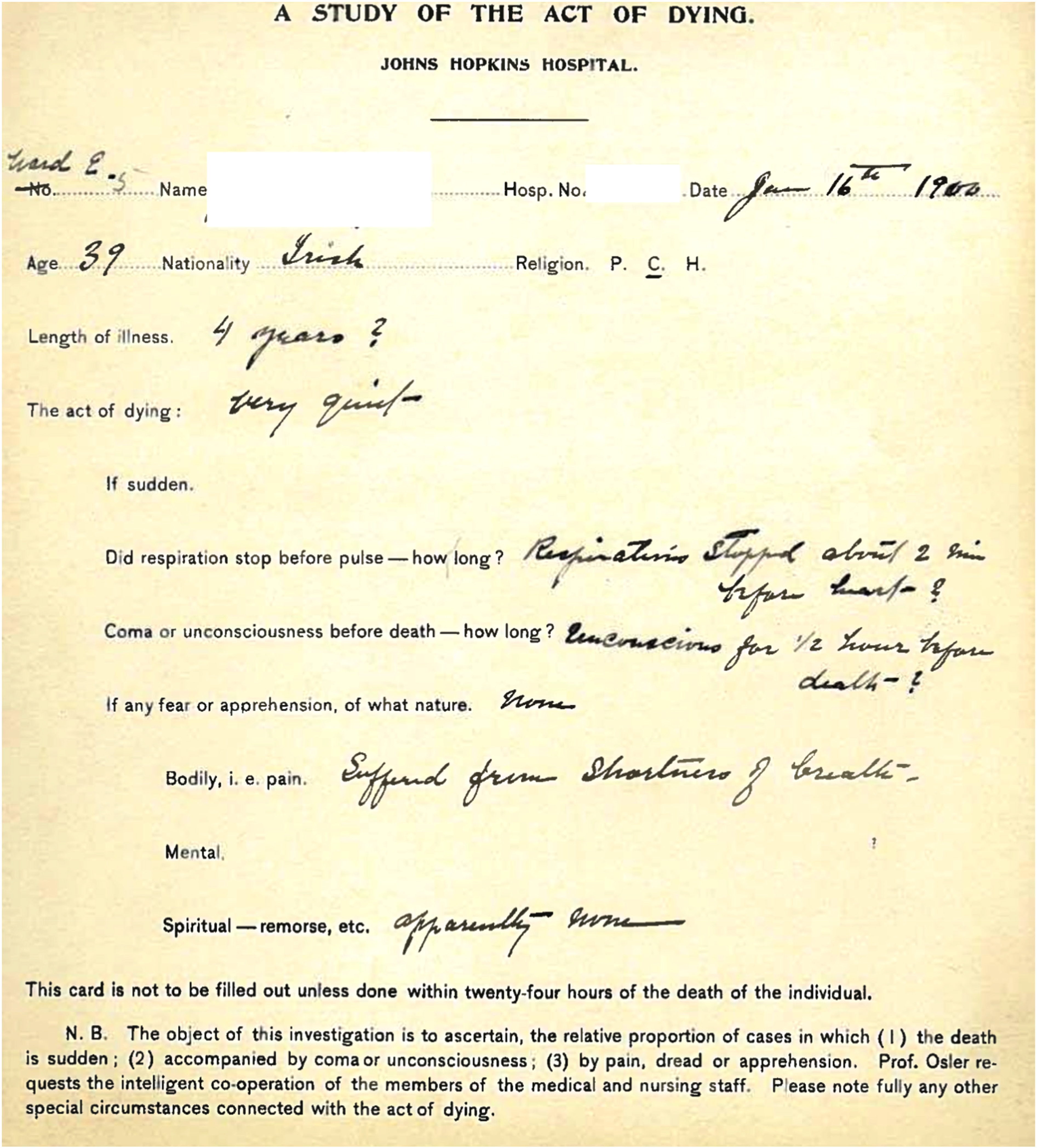
Study of Dying Card 5: “Called loudly.” 26
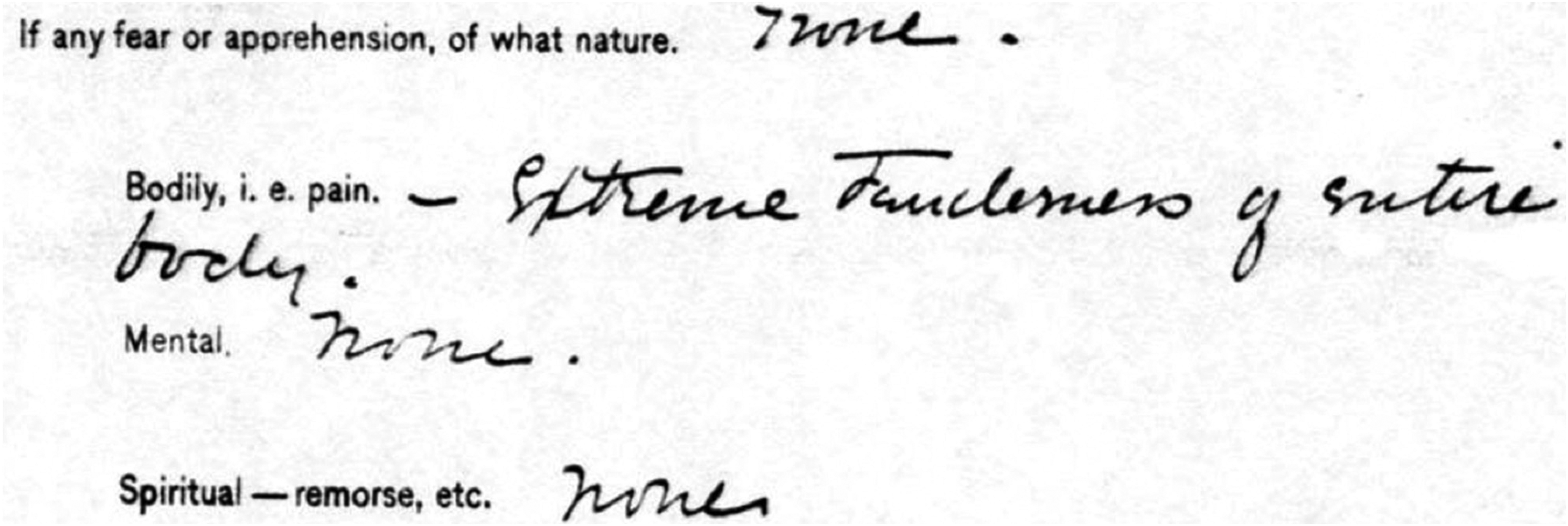
Portion of Study of Dying Card 21: “Extreme tenderness of entire body.” 27
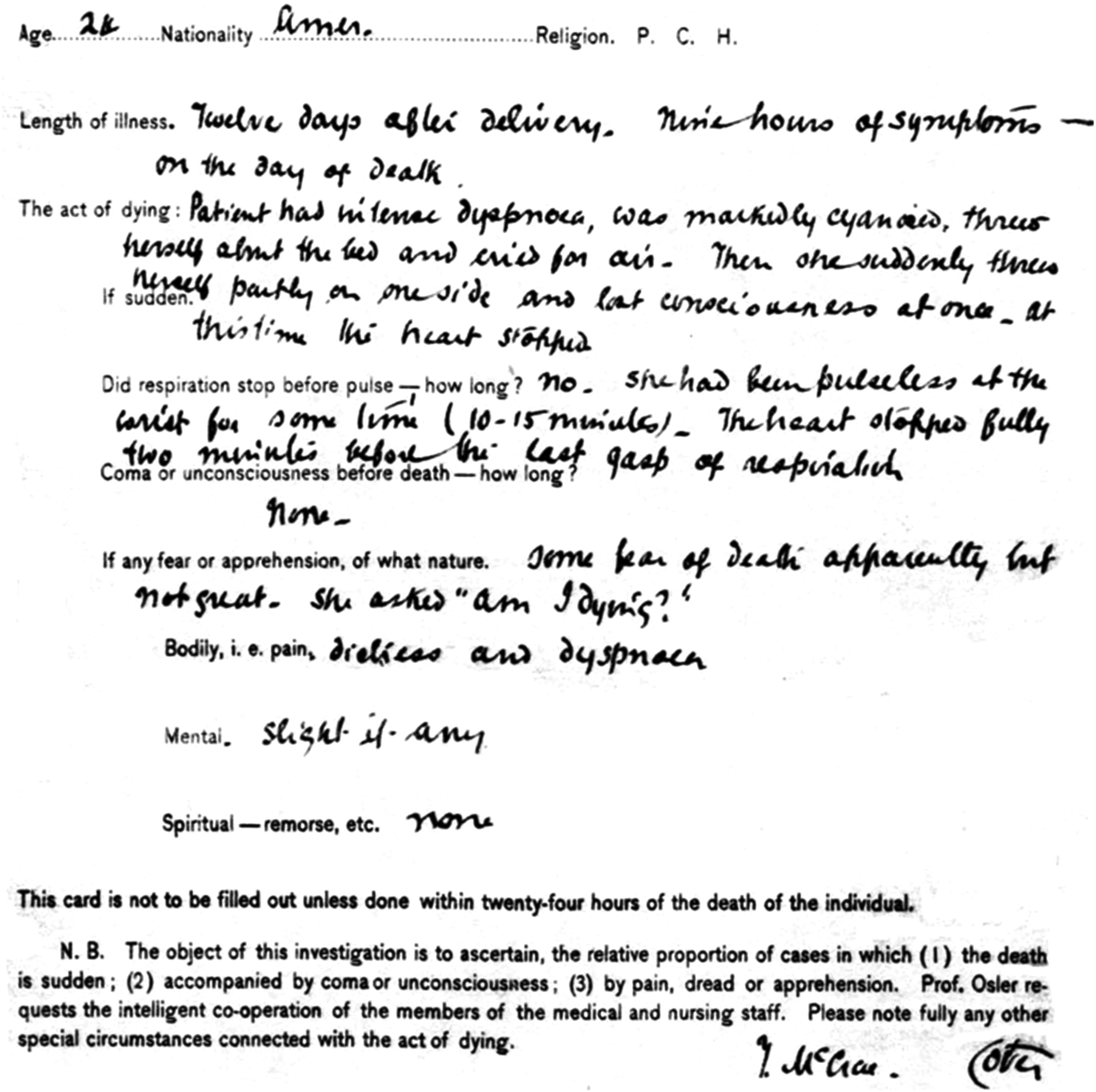
Study of Dying Card 26: “Gasps of respiration,” “Dyspnea,” “Am I Dying.” 29
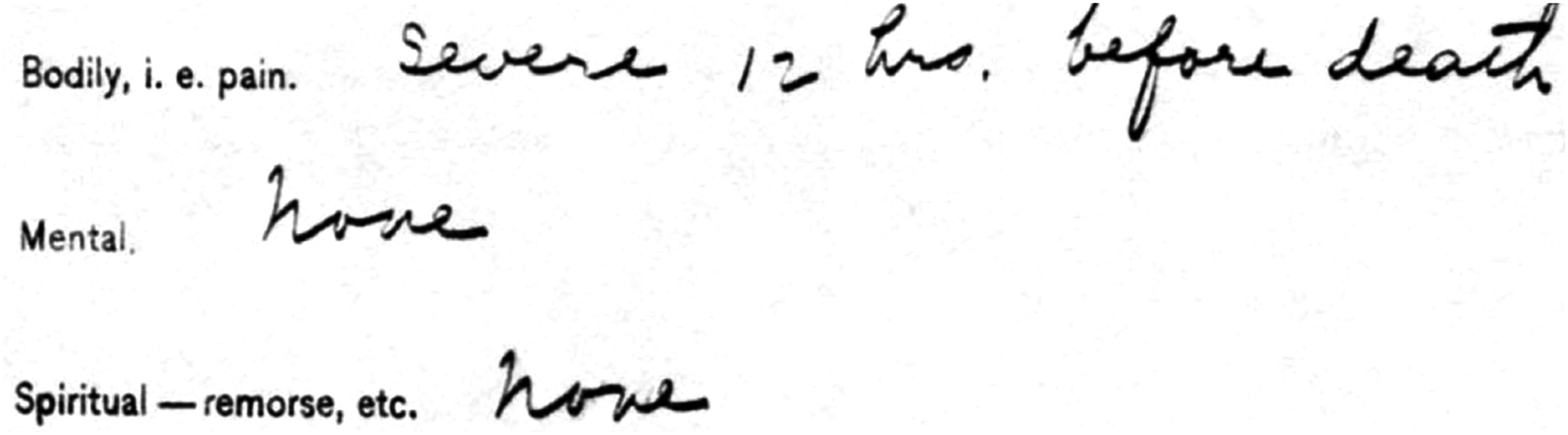
Portion of Study of Dying Card 48: “Severe.” 29
Osler never published the results, and many consider the lack of time as the reason.30,31 This essay, however, suggests another motive: Osler's own findings stand in contradiction to the death he clinically advocated for, one that is calm, painless, and a form of relief and forgetting.
Osler's conception of death unraveled
This struggle becomes especially evident when looking at Osler's own personal losses. For the most part, this period is not discussed in the Oslerian legacy of history of medicine. There is little focus on when Sir William Osler was not focused—where he drifted to and from himself to find forgotten, submerged, and somewhat frightful aspects of the self. Although Osler was one to “urge the advantages of an early devotion to a peripatetic philosophy of life,” 32 his personal experiences of death re-examines his clinical coolness. Rather than “acquire the art of detachment,” 33 used whimsically to mean a clinician who seeks evidence over all, detachment is brutally forced upon him with the loss of those he loved.
His first son, Paul Revere, was born when Osler was 43 years old in 1893, a year after marrying Grace Osler. She had already had two stillbirths, and was, as Osler said, “taking the rough with the smooth,” 34 a week later, Paul died of meningeal hemorrhage, a painful, horrible death for an infant. As Osler described to Lafleur a year later, “Though the birth was an exceedingly easy one, he was a little asphyxiated, and I suppose there was slight meningeal hemorrhage, and subsequent clotting in the veins or sinuses.” 35
Osler wrote a letter to his wife, titled “Paul Revere Osler” as a means to deal with the grief (Figures 6, 7(a) and (b)). 36 In it, Osler shows death distracted, away from the horrors of the clinical reality of his son's early end. Addressed from “Heaven,” Osler states, “I got here safely with very little inconvenience.” 37 Much of the letter then deals with divisions of heaven, based on age and experience. The letter, though, shows “[Heaven as] the exact counterpart of earth so far as its dwellers are concerned.” 38 It is a “lovely green spot, with fountains and trees and soft couches and such nice young girls to tend to us.” Moreover, Paul later meets Emma Osler, the sister of William Osler, who similarly died horribly young while Osler himself was a child. She is not featured in death, but rather, she “had been sent to make [Paul] feel happy and comfortable.” 38
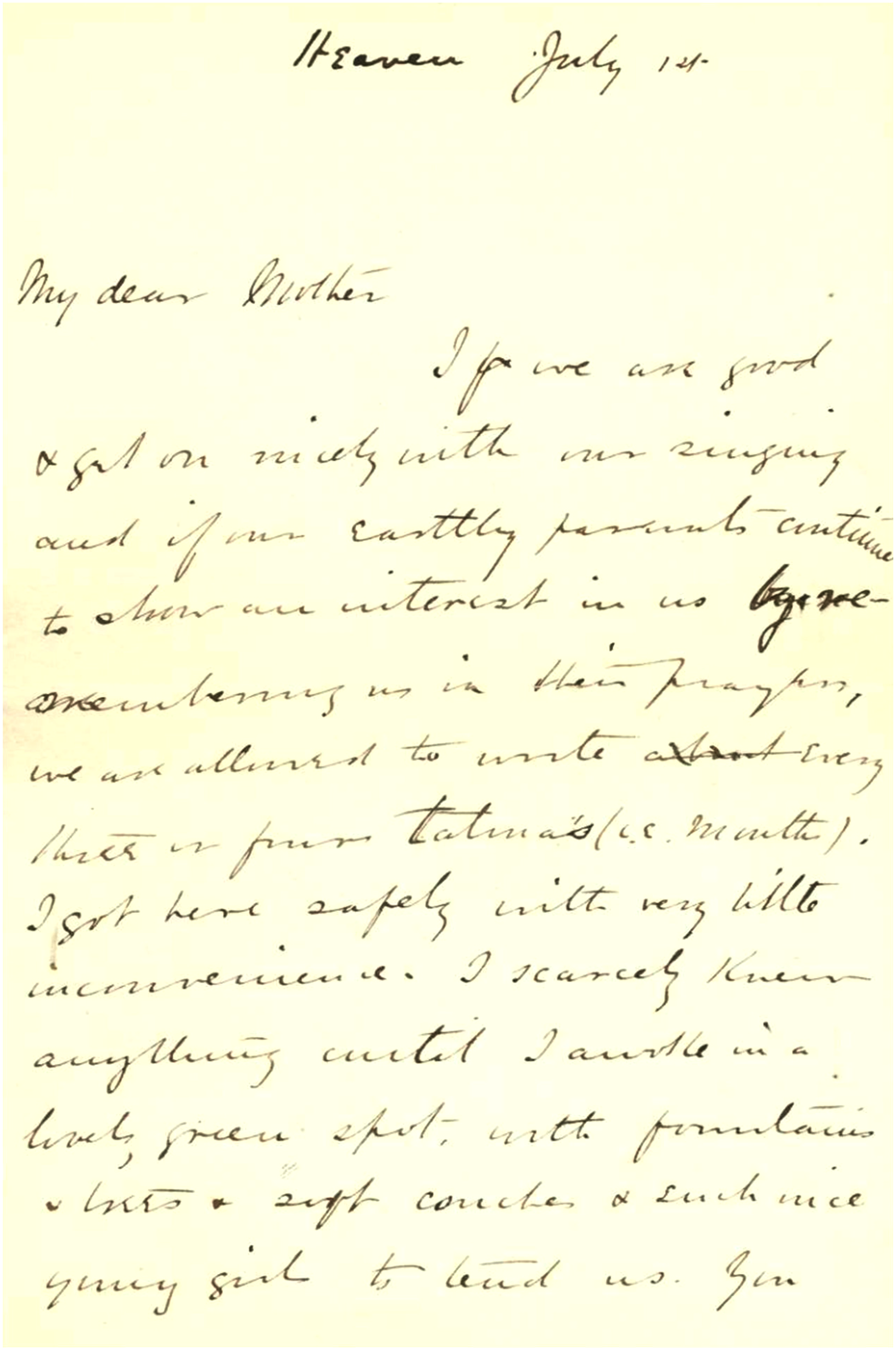
Posthumous letter from “Paul Revere Osler” to his mother, Grace Osler, page 1.

(a) and (b) Posthumous letter from “Paul Revere Osler” to his mother, Grace Osler, pages 2–3.
Such a discontinuity between the reality of death as an occasional “king of terrors” and Osler's purported public view of the quiet death is further shown with the loss of his second son. 39 Edward Revere Osler, known as Revere, was born in 1896. Worried about a similar outcome as Paul, and likely still traumatized, Osler did not allow himself to kiss the infant until day five. 40 No incidence occurred, and the childhood was a happy blossoming. Pictures (Figure 8(a) to (c)) show a joyful family, one of love and contentment. 41

On 30 August 1917, however, this idyll ended when Revere was killed in battle in the Great War. Osler was intimately crushed, writing to H. S. Birkett on 1 September that, “Our dear laddie has been taken!” 42 This vulnerability was in contrast with the accepted emotionality of the period. It shows Osler, who rarely used exclamations, as bruised deeply by the loss of his second son. “Taken” is used, suggestive of a sudden, brutal kidnapping of a life that could have been lived. Rather than discreet, then, death is exclaimed.
Moreover, it was unlike Osler to lament to others. Numerous accounts detail a curious, personable, but otherwise expressively constrained person. 43 He did not elaborate on his feelings in the place of facts. Evidence was a stalwart, which was the ultimate reason for writing The Principles and Practice of Medicine—to show how to provide care that was contemporary yet relatable to physicians, considerate of patients yet aware of medical boundaries.
So unique and totally world changing was Revere's death that Osler began to journal his dreams. Much of it is shimmering darkness, patches of ink written and crossed out, circled and reconsidered. One passage starts, “Dreamt of the boy.” Another ends, “They took his face. They took it once more.” 44
These letters were written with Osler's simultaneous reading of Sigmund Freud's The Interpretation of Dreams (1915). At its core, the book deals with the unconscious condensation, which as Osler underlined, “is the royal road to a knowledge … of the mind.” 45 His personal copy is well read, with evidence of being held closely and comfortably (Figure 9). Paratextually, passages are underscored and re-written. With the text, Osler's unconscious contradictions on death are laid bare.
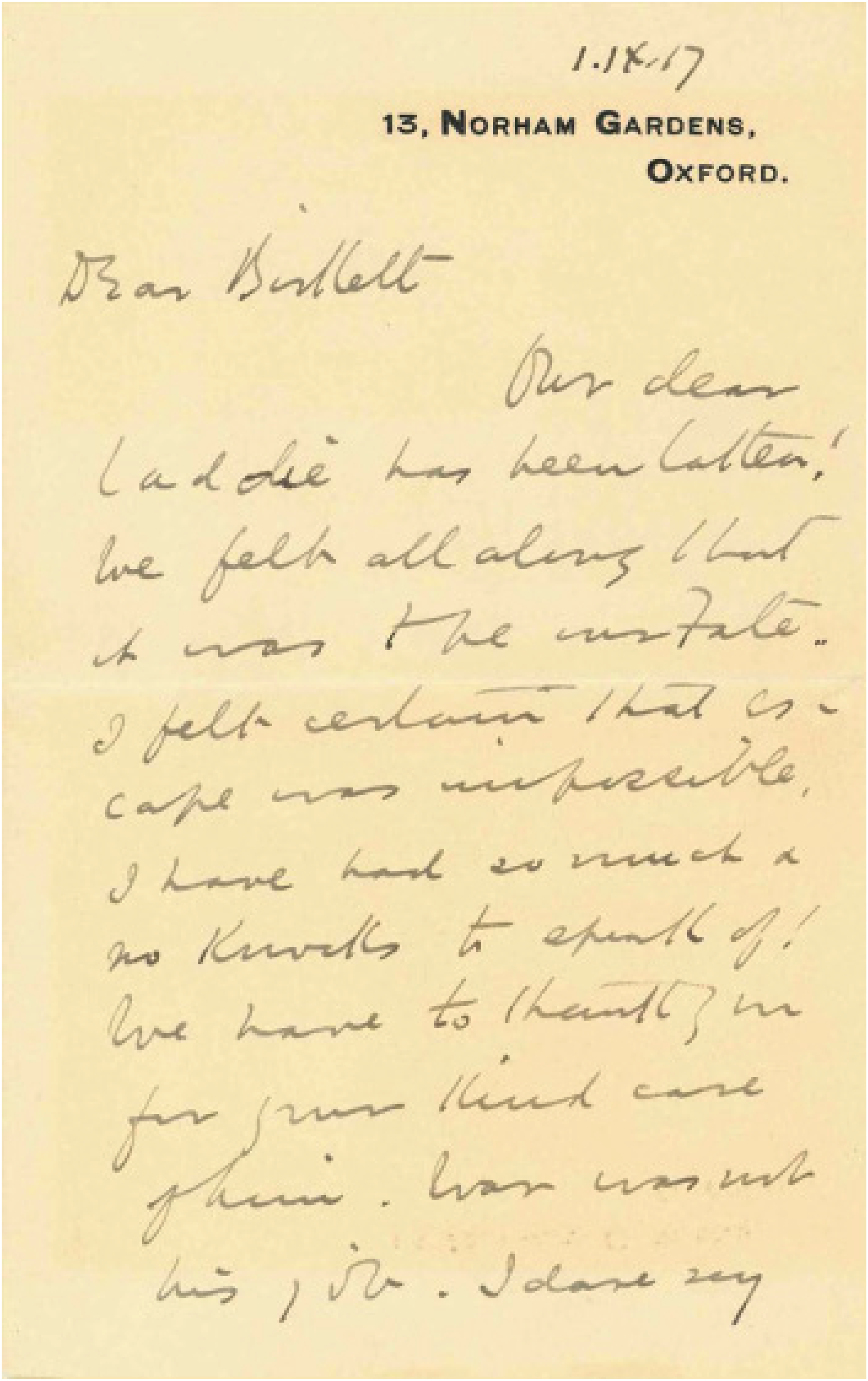
William Osler to H. S. Birkett 1 September 1917: “Our dear laddie has been taken!” 42
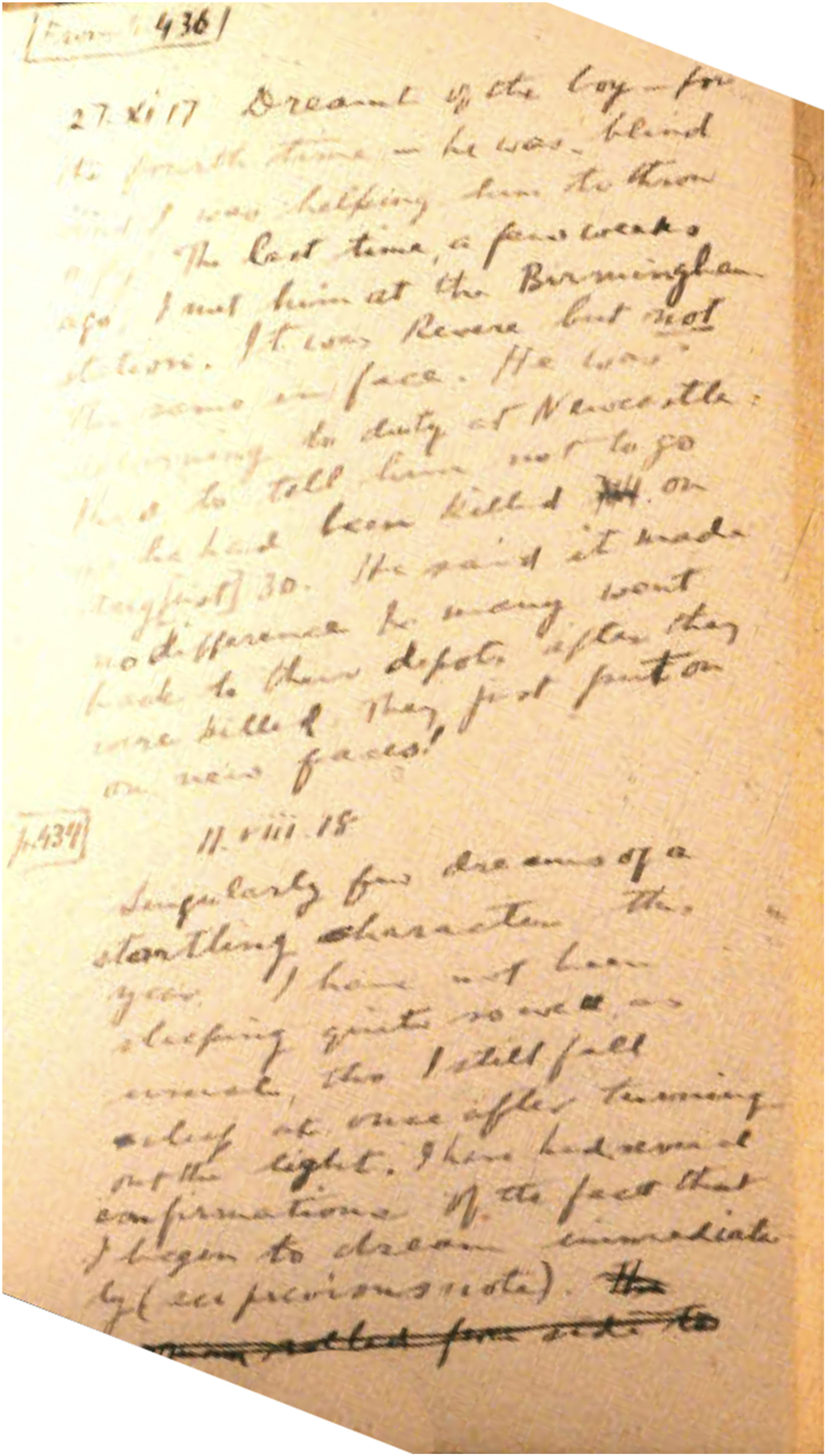
Page from Osler's dream journal.
Osler's dream journal shows evidence of this thoughtful contemplation, with some of these personally strained beliefs on death patched throughout the brief pages. In its uncharacteristic roughness, the journal showcases an unconscious hunger to have his son again, a conscious filtering of a man poised and educated, and a manifestation of them both in trying to realize the dream through the written actualization of it. By producing the notes, “the boy lives again.”35,46
In the journal, Osler further describes the horror, the awful death of Revere that is imagined but never seen. Of course, one can argue that this re-imagining and direct contradiction to a death of “sleeping and forgetting” are due to the different nature of the deaths—disease versus war. However, such a rationalization fails to explain his clinical incongruencies, his omissions in the Study of Dying notes, his description of death personally, and his own journaling. Death is not peaceful. In seeming agreement with Maeterlink, it is a being breathing nightmare air, one that Osler encounters in his own personal losses.
Conclusions
In framing these individual tragedies and their effects on Osler's conflicted formulation of death and dying, it could be argued that Osler's idea of total health actually becomes more comprehensive. “The good physician treats the disease,” he states, “the great physician treats the patient who has the disease.” 35 Osler's form of death is similarly individualized; instead of a single philosophy of serene, easy death free from anguish or mental duress which has been suggested in the literature and initially thought to be clinically touted by Osler himself, Osler's actual conception of death is a complicated smorgasbord of pain and dread. The archive of Osler's journals, books, and personal writings—his Study of Dying cards, his diary after Revere's death, and his numerous letters during World War I, as well as full texts like The Interpretation of Dreams—show a conflicted Osler, one who is buffeted and changed by the circumstances of living.
Such texts buoy the work by necessitating it—they illuminate a fuller picture of Osler's life, and ultimately, his own small deaths. Together, these works comprise disappointments, difficulties, seeing family members pass, and how all these add to a life unfulfilled: his two sons. Together, they dissuade from the mythos of Osler, showing him as an evolutionary of ideas, rather than an absolutist. Such a conflicted idea of death and dying suggests Osler as a true advocate of his own ideals that praise the ability for change and flexibility—to live in uncertainty, to move toward a fuller comprehension when one can, and to learn always what life is about, even if that means not being able to live it as peacefully in death.
Footnotes
Acknowledgment
The author thanks Dr Abraham Fuks for helping edit the essay and his careful consideration.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.