
Abstract
Arthur Ferguson MacCallan was an ophthalmic surgeon who undertook his pioneering work in Egypt between 1903 and 1923. He established the Egyptian ophthalmic infrastructure which, on his departure, consisted of 23 operational hospital units, treating 134,000 new patients, having trained some 100 ophthalmic surgeons. He also established the Memorial Ophthalmic Laboratory at Giza which is still operational today.
MacCallan became a world authority on trachoma. He pioneered the ‘MacCallan Classification’ which was the first grading system to standardise the stages of trachoma. He used this grading internally from 1905, continuing his research into trachoma over the ensuing years. In 1952, the WHO adopted the ‘MacCallan Classification’ as its standard.
There has recently been a revival of interest in MacCallan’s work. First, the International Coalition for Trachoma Control (ICTC) inaugurated the ‘ICTC MacCallan Medal’ in 2014 as a contribution towards achieving the WHO’s target date for the Global Elimination of Blinding Trachoma (‘GET 2020’). Second, MacCallan’s work with the military hospitals has been recognised by Moorfields Eye Hospital on their World War I Commemorative History Board. Thus, MacCallan’s pioneering spirit, his humanitarian campaign for the relief of suffering and his accomplishments of over a century ago continue to resonate with the profession today.
Keywords
The ophthalmic campaign in Egypt
I regard the campaign against ophthalmia as one of the most important and useful works undertaken in Egypt since the occupation commenced.
Lord Cromer (British Consul General, Egypt, 1883–1907) in a letter to MacCallan, dated 18 December 1914.
Arthur’s early life
Arthur Ferguson MacCallan (Figure 1) was born on 23 October 1872 at New Basford Vicarage, Nottingham.
1
He was raised in ‘genteel poverty’, with a strong Christian and Victorian work ethic. His father, John (1834–1883), who had moved from Northern Ireland, was, in 1868, the Vicar at St. Augustine’s Church, New Basford. In 1870, he married Elizabeth (nee Danks) (1843–1923). They had two children, Arthur and Gertrude (1874–1933). After John’s premature death in 1883, Elizabeth, Arthur and Gertrude moved into The Gables, Sherwood Rise, in Nottingham which had belonged to Elizabeth’s father (Thomas Danks) who had also died in 1883. Elizabeth coped well with the two children as, according to MacCallan, she was ‘a woman of super-eminent ability’. Their circumstances were constrained by ‘an inadequate income’, but Elizabeth was determined that Arthur receive a good education and had him accepted by Charterhouse, a private boarding school located in Godalming, Surrey, England (1886–1891).
Arthur MacCallan, 1923.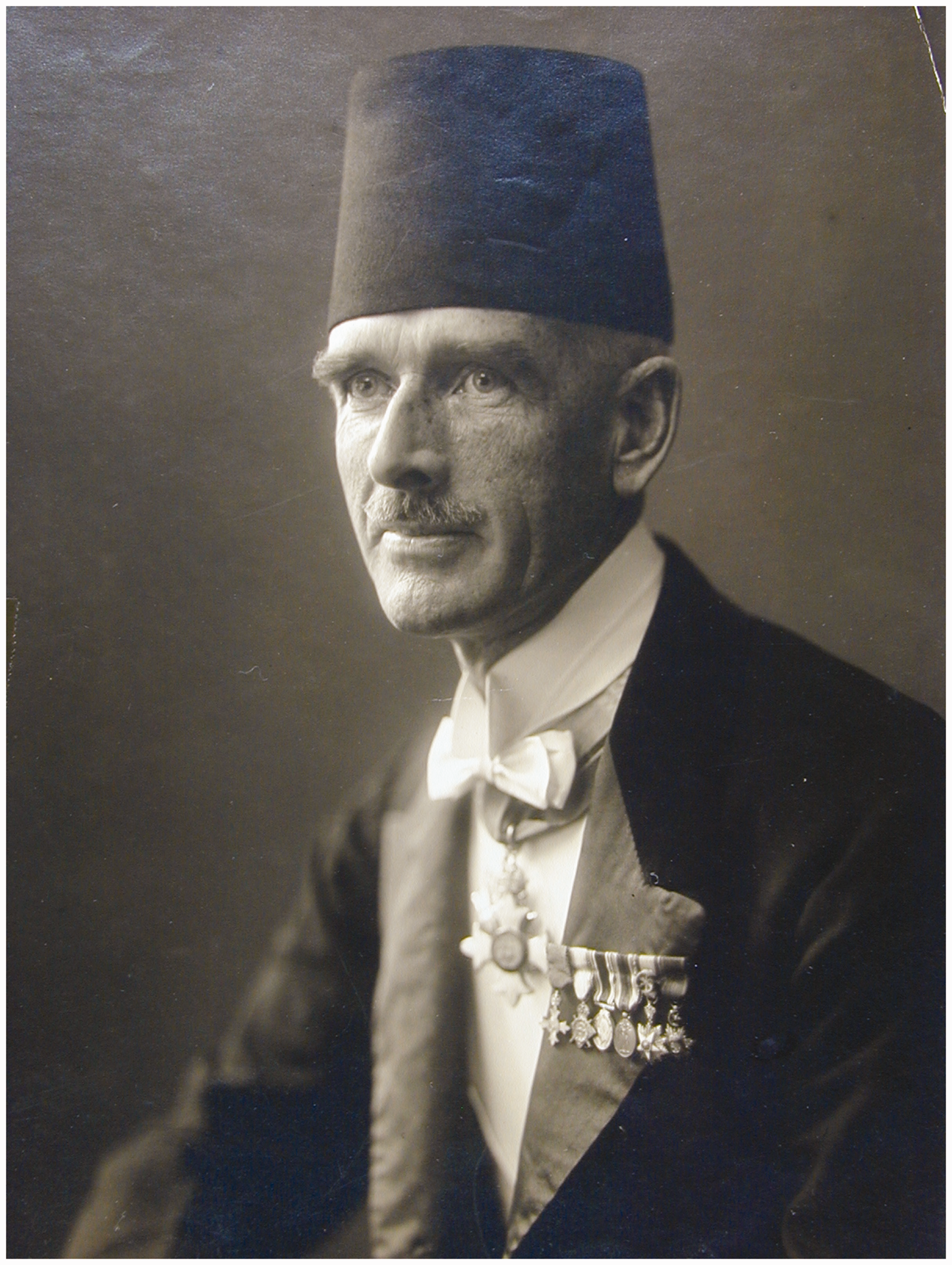
MacCallan then went to Christ’s College, Cambridge (1891–1895). In 1895, he obtained an Entrance University Exhibition to St Mary’s Hospital, London (1895–1900). He developed his bacteriological and pathological work and investigated the micro-organisms found in Enteric Fever for which he won the Darwin Prize at Christ’s College. 2
It was during this time that MacCallan, also acting as a Junior Clerical Assistant at Moorfields Eye Hospital, became interested in ophthalmic surgery, encouraged by Mr Quarry Silcock, surgeon to Moorfields Eye Hospital and general surgeon to St Mary’s Hospital. Silcock suggested that MacCallan should apply for the post of resident house-surgeon at the Royal London Ophthalmic Hospital (Moorfields) which he secured (1900–1903) at an annual salary of £50, with board, lodging and washing.
At the end of his three years’ residency, MacCallan was exhausted. He resigned his post owing to the severe strain of hospital work and the complete lack of social life. He became an unpaid Chief Clinical Assistant thus had no income except £10 for performing a squint operation and a £500 loan from an uncle, intended to establish him in private practice.
As the foundations for MacCallan’s future career were laid in Egypt a century before, some background is given to the British involvement there.
The British in Egypt
Britain had been involved in Egypt since before the start of the nineteenth century; it was the gateway to their trading Empire in India and the Far East. Thus, when Napoleon invaded Egypt in 1798, Britain was quick to send its own troops to protect its interests. This led to the defeat and withdrawal of the French troops in 1801, followed by the repatriation of the British troops in 1803.
The highly contagious nature of ophthalmia, which had plagued the local population for centuries, was observed by both the French 3 and British 4 who reported the devastating effect of ‘Egyptian’ or ‘military’ ophthalmia on the troops. This disease was carried back to their respective home countries on the troops’ return. In Britain, this led to the opening, in 1805, of the dispensary for Curing Diseases of the Eye and Ear (Moorfields).
Britain’s further involvement in Egypt increased from 1882, to protect its interest in the Suez Canal in which it had acquired, in 1875, a 44% interest in the Company for £4m from the Khedive, Ismail. However, it was not until the late 1890s that the financier and philanthropist, Sir Ernest Cassel (1852–1921), became involved in the project to build the first Aswan Dam (1898–1902). During its construction, Cassel was shocked at the extent of eye disease amongst the workforce of some 15,000 people. To address this chronic situation, he established a Trust Fund of £E40,000 (Egyptian pounds, equivalent then to £41,000 sterling) with the objective of teaching ‘the principles of ophthalmic surgery to Egyptian Surgeons’. To gauge the magnitude of the Trust Fund, it would have been sufficient to cover the building costs of between six and eight permanent ophthalmic hospitals at that time. In monetary terms, it is approximately £4m/US$6m today.
The trustees of the Cassel Fund, chaired by Lord Cromer, decided to use the interest (£E2000) on the principal to fund an initial, experimental, travelling ophthalmic hospital (TOH) along the lines of those operating in Russia. However, they needed someone to organise and administer the TOH and train local doctors in ophthalmic surgery. Dr EC Fischer, the oculist at Kasr-el-Aini Hospital and a trustee, approached his alma-mater (Moorfields Eye Hospital) to find a competent ophthalmic surgeon to fill the post.
Moorfields, 1903
By a stroke of good fortune, a Ward Sister overheard two doctors discussing the appointment in Egypt and volunteered ‘why don’t you ask Mr MacCallan?’ MacCallan was delighted and recorded that this was ‘the glorious opportunity of being independent with £500 a year and the opportunity for foreign travel [which] seemed to transcend even my dreams’. Using some of his uncle’s money to pay for his passage and collecting the necessary instruments from Weiss & Co, MacCallan set sail on the SS Caledonia and docked at Port Said, Egypt, at the beginning of July 1903.
MacCallan’s early days in Egypt and the first TOH
MacCallan had to establish his reputation with his professional colleagues. As he was unfamiliar with trachoma operations, his appointment caused resentment. However, he rose to the challenge and quickly surpassed the skills of his ophthalmic colleagues, one of whom referred to MacCallan as the ‘god of ophthalmology’, according to a letter from Arthur to his mother (undated, 1903).
MacCallan’s initial instructions were to familiarise himself with local conditions. To do this, he toured the Egyptian Delta area to assess the extent of ophthalmia amongst the local population.
To put the scourge of ophthalmia into context, when MacCallan commenced his work in Egypt, it was recognised that over 90% of the fellaheen (Egyptian natives) suffered from ophthalmia. 5 Arthur himself estimated that over 7% of the population were blind in one or both eyes. Indeed it was considered by Dr Max Meyerhof as the ‘twelfth plague’ of Egypt. 6 Unfortunately, there were only four eye hospitals in Egypt at the time, performing some 1300 operations annually. 5 Given the scarcity of trained surgeons and resources, many eye operations were performed by ‘quacks’ with ‘disastrous results to their [the patient’s] eyes … many were incurable’. 7
In this environment, MacCallan concluded that the success of the TOH scheme was assured 8 given the overwhelming demand for, and local doctors’ lack of knowledge of, ophthalmic treatment; however, given the potential number of patients, one TOH would be insufficient to cope. From an early stage, MacCallan believed that the extension of the TOH scheme throughout the country would bring significant economic benefits. He concluded that ‘the number of inefficient workers, due to the ravages of trachoma, is enormous and every child who now obtains relief at the camps is a worker saved from the ban of efficiency’. 7
The first TOH was located at Menouf as it was one of the most populous towns in the Nile Delta. An acre of land was hired at the outskirts of the town and was enclosed by a rough cotton-stalk fence. The camp was established towards the end of 1903 and began treating patients, free of charge, on 10 January 1904. This camp comprised 11 tents, the largest of which was ‘a lofty tent of the Swiss Cottage pattern with a small portion partitioned off to act as a dispensary. It was floored with concrete so as to be easily cleaned’. 7 The other tents were used for examinations, out-patient care, staff and kitchen. There was a staff of nine persons, including MacCallan and both a male and female hospital attendant. In April 1904, when it became too hot to work under canvas, mat huts were erected to replace the tents.
New initiatives can take time to be accepted. Initially, some of the fellaheen were suspicious; MacCallan was even considered a ‘freak’ by others. However, this prejudice was soon overcome by the empathy, skill and professionalism with which MacCallan organised and treated his patients; they could literally ‘see’ the benefits of his operations. Soon the demand grew rapidly as more people clamoured for more treatment; indeed such clamouring in the early days led to unruly crowds of patients which necessitated MacCallan having a police guard to maintain order, as well as implementing a ticketing system to control and organise patients. In any event, MacCallan soon became established and his reputation and credibility grew rapidly.
MacCallan’s volume of work in these early days was enormous; during the first three months of 1904, at Menouf, he treated 6157 patients and performed 615 operations (Figure 2).
9
These operations were ‘mostly for malposition of the eyelids as a result of trachoma (Granular lids) or as a result of badly performed operations by quack-doctors’.
8
Where anaesthetics were required, opium, cocaine or chloroform were used; in some cases, where no anaesthetics were available, patients might still insist that the appropriate operation be performed, so great was their desire for treatment. This was, of course, the era before antibiotics.
MacCallan operating in the desert, Menouf, 1904.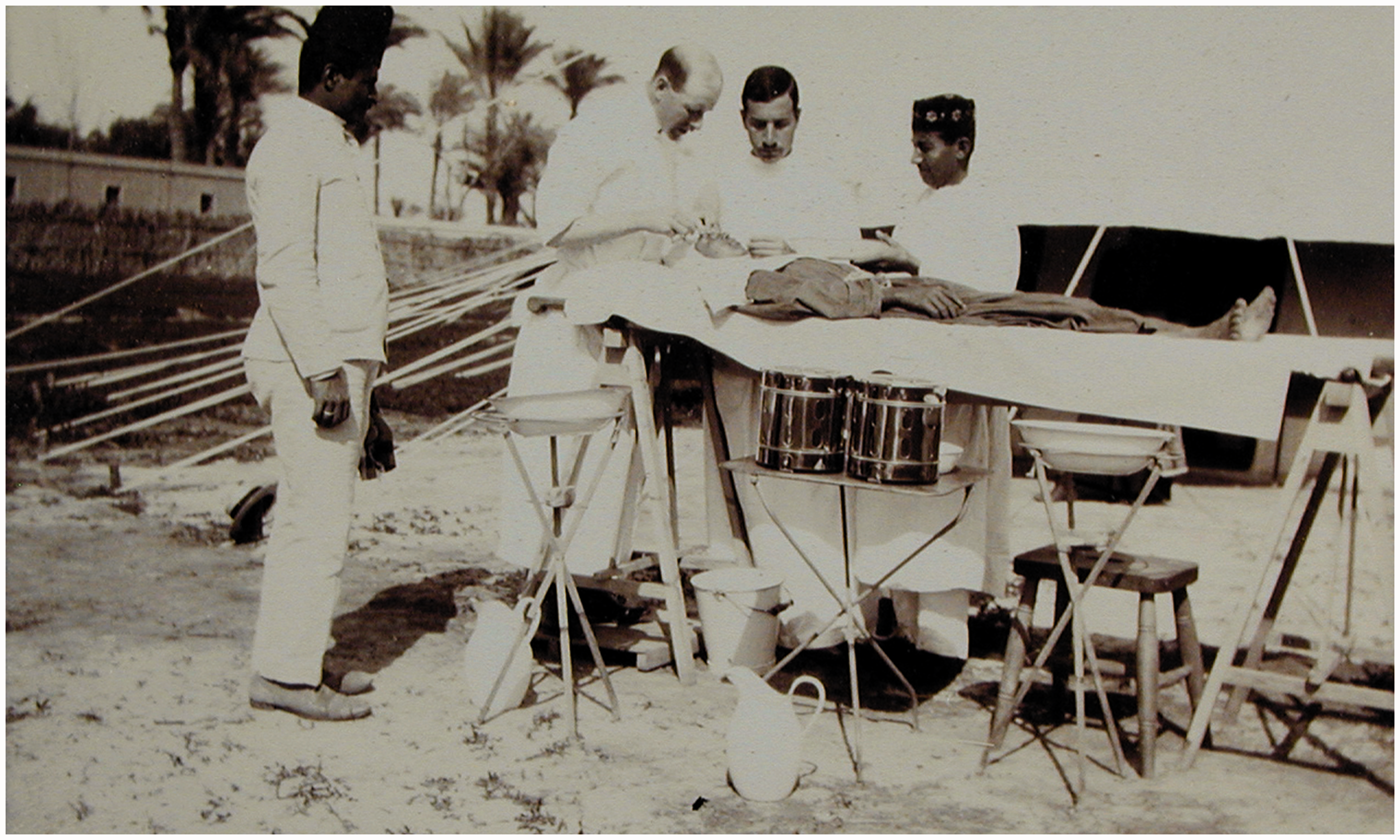
To give a sense of the challenges facing MacCallan, an extract is given from a letter to his mother, dated 10 February 1904: The number of patients goes on increasing and the work is now very onerous. I feel as if I should like to go to sleep for a fortnight. I still go out into the mob of waiting people every morning on horseback, hunting crop in hand (Figure 3) and wearing a bloody (from operating) galabia [a long-sleeved, closed garment reaching the ground] and choose out patients. But now I have a list prepared and post it up the day before. It does not make much difference to the mob however. They come now from all parts of Egypt. Alexandria, Behers, Cairo, Kap el Faqal etc. I really have not the heart to refuse to see them. Many of them who come such a long distance are blind and incurable. It is astonishing the calm way in which they take the news when one tells them that their case is hopeless.
MacCallan choosing patients, Menouf, 1904. The horse is ‘Saladin’.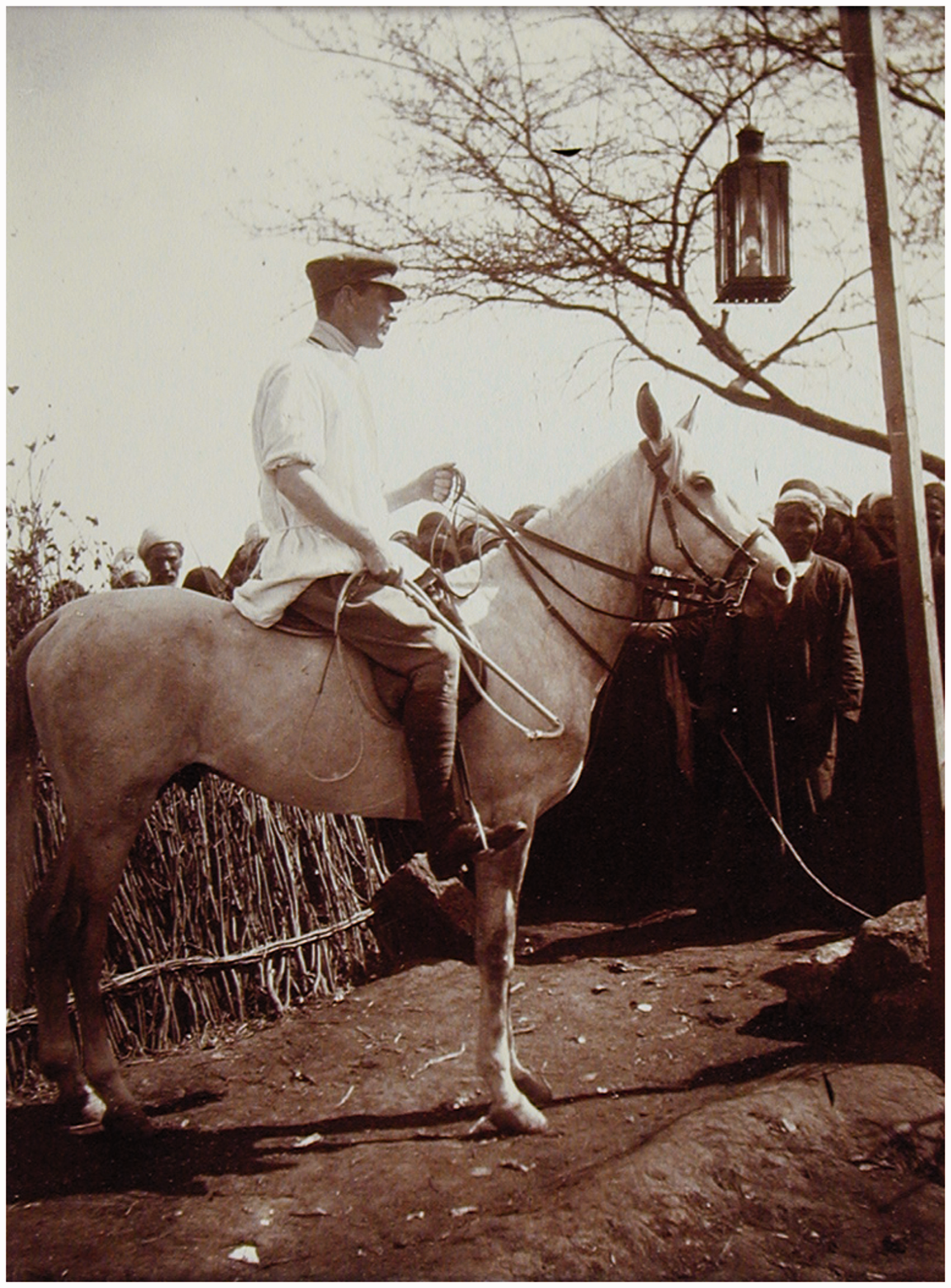
MacCallan’s solutions for eliminating trachoma
These early experiences reinforced MacCallan’s conclusion that, even with two TOHs, the treatment available was ‘only a drop in the ocean’. Thus, something both fundamental and bold had to be implemented. To address this, MacCallan planned, first, to ‘create a stable central ophthalmic administration with the best possible clinical and scientific teaching adjuncts’ 10 ; this included the training of doctors’ in ophthalmic surgery. Second, that at least one permanent ophthalmic hospital should be established in each of Egypt’s 14 Provinces. Third, in order to reduce the incidence of ophthalmia, particularly at schools, it was necessary to introduce an educational programme on ophthalmic hygiene.
Over the next 20 years, MacCallan worked tirelessly to achieve his self-imposed goals. Thus he found himself bearing the mantle of ‘ambassador’ in promoting this cause in which role, over the years, he persuaded both local notables and Government to provide significant funding and other support for the development of the ophthalmic hospital infrastructure.
Establishing the ophthalmic hospital infrastructure: Travelling ophthalmic hospitals
The success of the first two TOHs was evident. However, in order to give treatment to as many people as possible, they were relocated every six months. The actual number of TOHs depended on circumstances and available funding at the time. In 1904, for example, the two TOHs treated patients at Menouf, Fayoum, Damietta and Calioub. By the end of 1906, Zagazig, Damanhur, Beni-Suef and Assiut had been added. 11
One beneficial consequence of these travelling hospitals is that they acted as ‘roving advertisements’ for the ophthalmic campaign as they brought the hospital to the people. As the benefits in relieving suffering were so evident, it encouraged private donations to be made by wealthy individuals, both of money and land, some of which were significant. By 1909, for example, more than £E10,000 had been subscribed, equivalent to over £1m today.
Tent hospitals were also used to respond to an initiative by Lord Kitchener, British Consul 1911–1914. This led to MacCallan establishing travelling hospitals to fight ankylostomiasis (hookworm). Given their flexibility, these hospitals were also used to great effect in 1915, during World War I.
Permanent ophthalmic hospitals
The purpose of providing buildings as ophthalmic hospitals was to enable treatment to be carried on throughout the year; this was not possible in tent hospitals during the hot weather. Initially, incorporating an ophthalmic unit in some of the existing hospitals was considered. However, this idea was discarded as there was neither available accommodation nor any building land nearby. More significantly, the large number of patients, often 500, attending the ophthalmic section daily would entirely disorganise the arrangements of the general hospitals. 11
Thus it was decided to construct separate permanent hospitals. In recognising the imperative nature of this initiative, the Egyptian Government took over the administration of the Cassel Fund in 1905 and started providing more finance for the treatment of ophthalmia. MacCallan was delighted and noted that ‘the national importance of the struggle against ophthalmia has thus been recognised and must henceforth take its place amongst the measures essential to the prosperity of the country.’ 12
The first permanent ophthalmic hospital was based at Tanta; Government funding was approved in 1906 but, due to financial difficulties of the contractor, it was not opened until 1908. A second hospital was opened at Assiut in 1910. These, and other, permanent hospitals were funded by a combination of local and Government finance and, in many cases, included generous donations of both land and money from wealthy individuals.
On MacCallan’s departure in 1923, there were 23 ophthalmic hospital units, including five TOHs, and a further two planned hospitals. The Memorial Ophthalmic Laboratory at Giza (now known as the Giza Memorial Institute for Ophthalmic Research) was then under construction. Many of these hospitals are operational today; indeed Fayoum celebrated its centenary in 2015. Significantly, MacCallan had established an infrastructure that could continue to develop even after his departure. The success of this may gauged in that, by 1937, there were 63 permanent ophthalmic hospitals, 15 travelling hospitals and treatment centres in 38 Government schools. 13
Training ophthalmic surgeons
The training of ophthalmic surgeons was a requirement of the original Cassel Trust Fund. These qualified surgeons were also essential to staff the increasing number of both permanent and travelling hospitals. MacCallan was a keen advocate for training and research, and at his leaving tea party in December, 1923, he proudly noted that ‘at the first meeting of the [Egyptian Ophthalmological] Society in 1903, there were 17 members, only 7 of whom were Egyptians. Now there were 96 members, the vast majority of whom were Egyptians, and most of them had been his pupils’. Training was of a practical, surgical nature and supported by lectures and examinations. A complete course of post-graduate lectures was also introduced which included clinical pathology and bacteriology.
At the tea party, MacCallan also quoted statistics which recorded the significant growth over 20 years in the number of patients treated (from 3379 to 133,750: 40× increase) and operations performed (from 1268 to 76,035; 60× increase).
Over the years, MacCallan played a key role in the development of the Egyptian Ophthalmological Society. He was elected President in 1912 and was created an Honorary Member in 1925.
Hygiene awareness in schools
MacCallan believed that ‘the most important work carried out was the institution of ophthalmic treatment in all Government Primary Schools throughout Egypt’. 14
Given that trachoma was highly contagious, particularly in the close environment of the family unit and schools, MacCallan energetically tried to educate people on the benefits of personal ophthalmic hygiene and so prevent the spread of the disease. Indeed, one of his first professional calls in 1903 was to the headmaster of Menouf School with the offer of inspecting the pupils for ophthalmia; he found that 124 of the 133 day-pupils needed treatment.
A further example of the extent of ophthalmia arose whilst MacCallan was inspecting Tanta School in 1906. 15 He found that only 16 pupils, from a total of 485, ‘were free from granular ophthalmia or trachoma’. Typically, he worked tirelessly both to prevent the disease, through education and establishing a programme of formal schools’ inspections, and cure his patients through operations and medicines. One practical approach adopted by MacCallan, in educating people on the importance of facial and ophthalmic hygiene, was to exclude patients with dirty faces!
It is salutary to record that this emphasis on hygiene (clean hands, faces and towels) remains relevant today and is part of the WHO-endorsed SAFE strategy (‘F’ – facial cleanliness).
Ophthalmic research, including ‘MacCallan’s Classification’ of trachoma and the Memorial Laboratory
MacCallan is probably best known among the international ophthalmic profession for his research into and ‘classification of the stages of trachoma’. He analysed trachoma by identifying its component parts in a structured manner which enabled patients’ symptoms to be more readily identified and thus more readily treatable. As Professor Sorsby succinctly noted: ‘his drive, energy and resolution all went into his efforts to convert the … human suffering from trachoma into a concrete scientific and administrative problem’. 16 As early as 1905, he was using his classification internally; this was then published in 1908 and further developed in his books Trachoma and its Complications in Egypt 17 and Trachoma. 18 In 1952, the WHO adopted ‘MacCallan’s Classification’ as its standard.
Ophthalmic research facilities in Egypt were limited. To address this, MacCallan established the first laboratory at Assiut in 1913; by 1918 it had been transferred to Giza where research was conducted in a large tent hospital.
19
Finally, he was instrumental in establishing the permanent ophthalmic research establishment at Giza, then known as the Memorial Ophthalmic Laboratory, whose main functions were to act as a research institute and a post-graduate teaching centre. The funding for this Laboratory was provided by the Imperial War Graves Commission as a Memorial to those men of the Egyptian Labour and Camel Transport Corps who fell during the Great War 1914–1918. The Laboratory was completed in 1925, formally opened in 1926, and is still operational today (Figure 4). In a hand-written note, MacCallan recorded that ‘this laboratory was envisaged by me many years beforehand. I got the site, the money for the building, arranged the endowment, and designed the interior, with all detail’; he also considered this Laboratory ‘as the coping stone of my work’.
Giza Memorial Institute for Ophthalmic Research, 2009.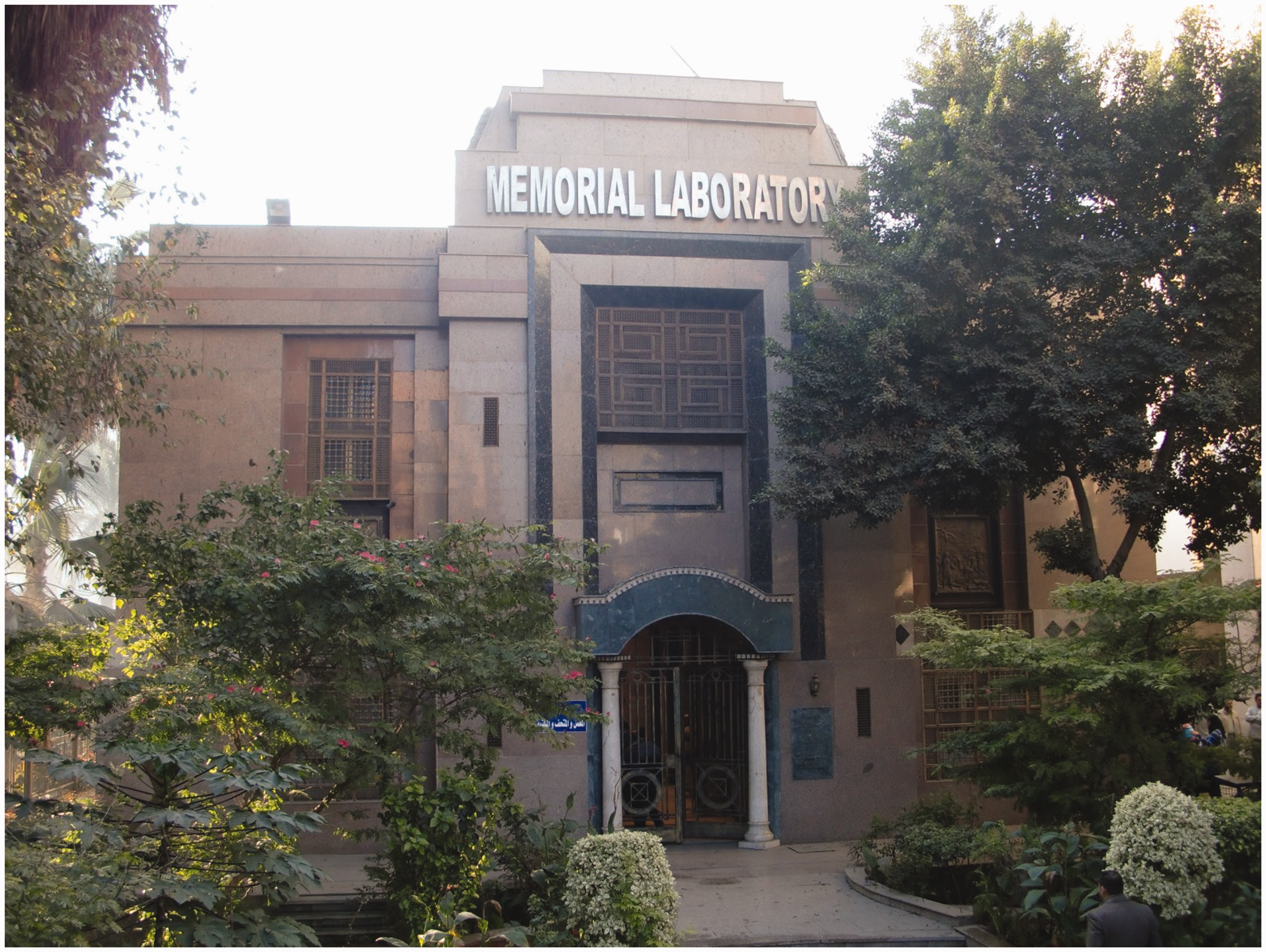
In 1931, a ceremony was held at Giza to unveil a bust of MacCallan commemorating his 20 years’ dedication to the Egyptian ophthalmic service, funded by his students, patients and colleagues. When this bronze bust was imported in 1930, the Ministry of Finance agreed to waive the customs duty in recognition of the ‘moral significance’ of Arthur’s humanitarian work in Egypt. Today, the bust is located inside the Memorial Institute.
World War 1
MacCallan was in England in August 1914. At the outbreak of war, he was ordered to return immediately to Egypt by Lord Kitchener, then Minister of War, through his aide-de-camp Colonel Fitzgerald. He set sail on P&O Mooltan along with ‘150 generals on board’. Then in December, MacCallan attended the parade when Egypt was declared a British Protectorate.
In early 1915, many of the ophthalmic hospitals, including TOHs, were commissioned by the military to treat the sick and wounded from the campaigns in the Suez Canal, Gallipoli and Salonica. During that time, MacCallan developed a plan to establish a large ‘hospital under canvas’ in Alexandria, the whole area around which was turning into a huge hospital camp. He initially planned for 200 beds, based at Glymenopoulo Bay, but this was expanded later to 650 beds when it transferred to Giza in October, 1915 for the winter months. 20 By January 1916, the military hospitals were able to accommodate the reduced number of sick and wounded and so MacCallan’s hospitals were decommissioned and returned to ophthalmic use. MacCallan was commended by Surgeon-General Ford that his hospital was ‘a model of what a war hospital under canvas should be’ (28 February 1916). Recently, on 11 November 2014, MacCallan’s military hospital work was recognised by Moorfields Eye Hospital on their World War I Commemorative History Board.
In February 1916, MacCallan was posted to Mersa Matruh as a Special Services Officer and Senior Medical Officer at the base, with the rank of Major, RAMC. He was Mentioned in Despatches and demobilised in 1917, returning to ophthalmic administration, teaching and surgery.
However, MacCallan’s war work was not yet finished as, after the capture of Jerusalem in December 1917, Field Marshall Allenby ordered MacCallan to inspect the Ophthalmic Hospital of St. John of Jerusalem. This hospital had been used as an ammunition dump by the Turks and had been badly damaged when the Turks retreated. According to Sir Ronald Storrs, then Military Governor of Jerusalem, ‘it took the best part of a week to clear it [the hospital] of exploded and unexploded cartridges and to summon the expert advice of MacCallan from Cairo’. 21 MacCallan travelled there in February 1918 to investigate. Just a year later, in February 1919, Allenby reopened the reconstructed ophthalmic hospital.
MacCallan’s personal life
MacCallan was dedicated to his ophthalmic work. Given his considerable workload and the amount of travel he had to do within Egypt, he felt he was too old (even in his early 30s) to go to the hotel dances in Cairo. Thus, it was not until 1917 that he met his future bride, Hester Boyd-Carpenter (1893–1960). Hester was the youngest daughter of William Boyd-Carpenter (1841–1918) and his second wife Annie-Maude (nee Gardner, 1854–1915). William had been Bishop of Ripon (1884–1911), Chaplain to Queen Victoria and Clerk of the Closet to Edward VII and George V. Both William and Annie-Maude are buried in Westminster Abbey.
Hester travelled to Egypt during 1916 to stay with her step-brother, HJ Boyd-Carpenter, the Chief Inspector of the Egyptian Government Schools, and worked as a volunteer nurse with the British Red Cross. In mid-1918, MacCallan proposed, despite being 20 years older. They were married on 12 September 1918 and had three children.
MacCallan’s recreational activities included riding, shooting, hunting and dogs. In his very early days, he had purchased his first horse, Saladin, and enjoyed the freedom this gave him both as a practical means of transport, as well as for recreation purposes. MacCallan also shot snipe at the Nile Barrier, having purchased a gun in his early days for £10. He developed an interest in hunting, again often conducted around the Nile Barrage area. On one hunt just before Christmas 1904, the pack caught a wolf weighing at least 50 lbs. He also found the presence of a canine friend provided a distraction from the rigours of camp life. His first dog, Jock, a poodle, unfortunately died at Menouf in 1904; given the fellaheen’s great respect for MacCallan, they shared their mentor’s grief by turning out ‘en-masse’ at Jock’s funeral.
Egyptian independence and MacCallan’s decision to leave Egypt
When MacCallan arrived in 1903, Egypt was under the control of the British. However, there had been a constant push by Egyptians to seek independence from Britain and control its own affairs. This move was halted during World War I but, thereafter, there was increasing pressure for independence to be granted and for foreign nationals, employed by the State, to be repatriated.
MacCallan was involved in this process from both a professional and personal aspect. As a means of protecting the interests of British nationals employed in Egypt, the Association of British Officials (ABO) was formed in 1920 with MacCallan being elected as Chairman. In these early days, however, the Egyptian authorities regarded the ABO as a ‘revolutionary organisation’ but due to MacCallan’s tact and negotiating skills, the ABO became the official mouthpiece of the British officials in Egypt.
From a personal point of view, these changing circumstances forced MacCallan to choose to remain in Egypt or return to London. Given MacCallan’s administrative experience, in 1923 the Egyptian Undersecretary of State for Public Health insisted that he should accept the post of Director General of Epidemic Services and of all general hospitals. Professionally, he was not inclined to do so as this would prevent him from continuing his ophthalmic career, particularly on research into trachoma. Thus, MacCallan resigned in 1923 and returned to London in February 1924.
MacCallan’s long and successful career in Egypt had been recognised over the years by both the Egyptian and British Governments. These included the CBE (1920), the Order of the Nile (2nd Class: 1924) and the Order of the Hospital of St. John of Jerusalem (Officer: 1940). On his departure, the then British High Commissioner for Egypt, Lord Allenby, wrote to MacCallan in his letter dated 7 April 1924: The tributes paid by Englishmen and Egyptians alike … to your professional skill, administrative ability and untiring energy, have been as remarkable as they have been well-deserved, and the record of your work, of incalculable benefit to the people of this country, will rank high in the history of British endeavour here.
MacCallan’s personal qualities
MacCallan faced considerable challenges and difficulties throughout his time in Egypt. He met these with fortitude by applying Ovid’s philosophy to ‘steel thy heart and endure: this trouble shall turn to thy vantage’. 22 MacCallan had a clear vision as to what was needed to alleviate the suffering of the local population and was driven by an iron will and his determination to succeed. He had ‘tenacious energy and a wonderful talent for organisation … a high sense of duty, strict control over himself and his subordinates with personal amiability and kindness of heart [which have] won for this man the confidence and affection of his innumerable patients and staff’. 23 He cared deeply about his patients’ welfare and, according to Ghabrial Faraq, Chief Clerk of the Ophthalmic Section, ‘was always just with his staff’.
MacCallan was also a skilled negotiator, which talent he needed to raise funds for the development of the ophthalmic infrastructure. He loathed bureaucracy and was no ‘pampered official’, but recognised that if he were to become part of the official hierarchy, he would have to develop skills in ‘the art of propaganda among all classes of the population’ and despite having to apply ‘myself to the niceties of administrative routine which I hated’. 24
Post Egypt (1924–1955)
On his return to England, aged 51, MacCallan continued his ophthalmic career. He held various appointments including, in 1924, Assistant Ophthalmic Surgeon at Westminster Hospital where he remained until his (official) retirement in 1937; he was then appointed consulting ophthalmic surgeon. He was also Assistant Surgeon to the Royal Eye Hospital, Southwark. He was on the Editorial staff of the British Journal of Ophthalmology and the American Journal of Ophthalmology. Arthur also held a number of committee appointments, including, in 1935, President of the International Organisation against Trachoma, a position he held for some 20 years.
He only returned once to Egypt which was in 1937. This meant he was absent from both the official opening of the Memorial Ophthalmic Laboratory, Giza (1926) and the unveiling of the Commemorative Bust in 1931. However, MacCallan’s personal messages were read out to the participants at both events.
In 1936, MacCallan delivered the Hunterian Lecture at the Royal College of Surgeons of England. 25 That same year, he published Trachoma which updated and developed his earlier works. 18
During World War II, MacCallan was a Captain and Medical Officer in the Home Guard. He was also recalled to Westminster Hospital in 1944 where, for a time, he resumed full clinical responsibility for the Eye Department, until the permanent staff were demobilised. A newspaper reporter recorded that ‘I found Mr MacCallan, now white-haired, but with a hand as firm as a rock, at Westminster Hospital, still doing research work in trachoma … When I called, Mr MacCallan had just diagnosed trachoma in five cases’. 26
MacCallan continued his active research and involvement in ophthalmic affairs and committees for the rest of his life. He died on 31 March 1955 at Westminster Hospital and is buried at the Church (‘Rock’) Cemetery, Nottingham.
Concluding remarks
It is a fitting tribute to MacCallan that his personal attributes, his humanitarian campaign for the relief of suffering and his accomplishments of over a century ago, have recently been revived by both the International Coalition for Trachoma Control and Moorfields Eye Hospital. This demonstrates that his pioneering spirit continues to inspire and resonate with today’s profession as they continue the fight to eliminate blinding trachoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.