
Abstract
Background
Acupuncture in Asian countries (and now worldwide) is common and normally quite safe. 1 Hemiplegic patients have been treated using oriental medicine involving acupuncture needles. 2 There have been sporadic cases of migration of acupuncture needles, including to the bladder, heart, lung and even the medulla oblongata. 3 Migration of the acupuncture needle into the lung parenchyma is believed to be a truly rare event and, to our knowledge, has been reported only once previously, alongside four other cases of migration into the lung. 4 Here, we report a case of chronic empyema that occurred after migration of an acupuncture needle into a patient’s left lower lobe.
Case presentation
A 38-year-old man had visited the outpatient clinic of our rehabilitation center 2 years earlier, which was 3 years after the onset of intracerebral hemorrhage of his pons with the sequela of quadriplegia.
A computerized tomography (CT) scan of his neck taken a year prior incidentally revealed a 2 cm nodule in his right upper lobe. In the meantime, he had undergone daily treatment with acupuncture for 1 year. A follow-up chest CT taken in March 2023 confirmed disappearance of the previously demonstrated nodule in his right upper lobe but demonstrated migration of a missing acupuncture needle into his left lower lobe (Figure 1(a)). Unfortunately, the presence of the acupuncture needle on CT scan was overlooked by both the radiologist and the rehabilitation specialist at this time. Meanwhile, he had spent time at a local rehabilitation hospital and had developed symptoms suggestive of pneumonia in his left lower lobe. Antibiotics were given, but his condition worsened and he developed aggravated symptoms of coughing, copious sputum and chest pain over the course of a week. He was sent to the emergency room at our center and admitted to our department of thoracic and cardiovascular surgery. A follow-up chest CT scan with enhancement revealed chronic empyema (Figure 1(b)). He then underwent an emergency closed thoracostomy and was scheduled for thoracoscopic decortication and foreign body removal.
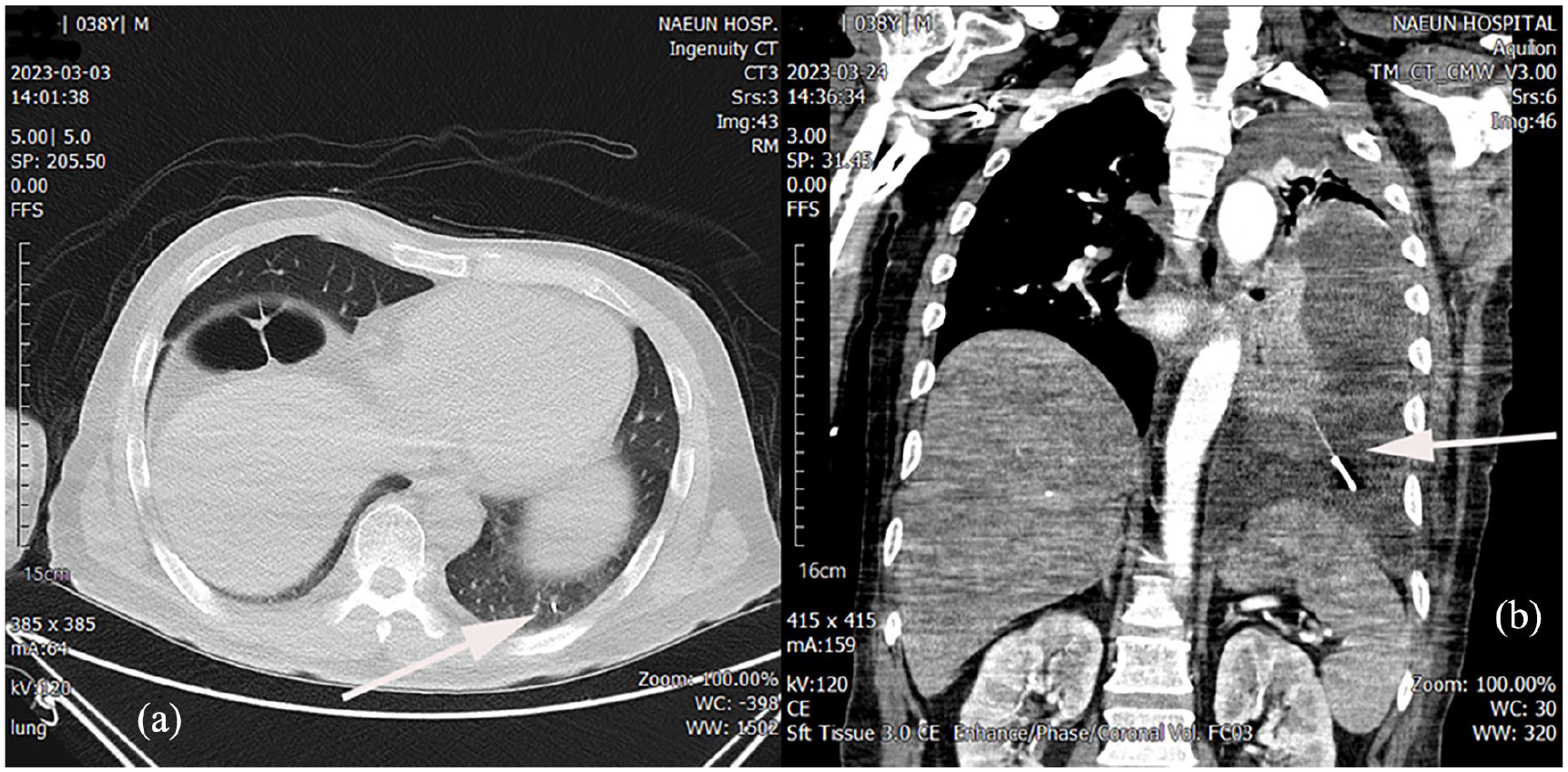
(a) Initial computerized tomography (CT) scan of the patient 2 weeks before symptoms of chest pain and coughing developed, with needle recognized only in retrospect (white arrow). (b) Follow-up CT scan of the patient with signs of empyema in addition to retention of acupuncture needle within thorax (white arrow).
The patient underwent video-assisted thoracoscopic surgery under general anesthesia 3 days later. A lung abscess rupture site was seen and the extruded acupuncture needle was evident, surrounded by pus (Figure 2(a) and (b)). Extensive decortication was needed but fortunately the needle was easily removed. Two chest tubes were inserted due to air leakage. The anterior chest tube was removed on the third postoperative day and the posterior chest tube was removed on the seventh postoperative day. His postoperative course was uneventful and he was discharged a week later following the removal of sutures.
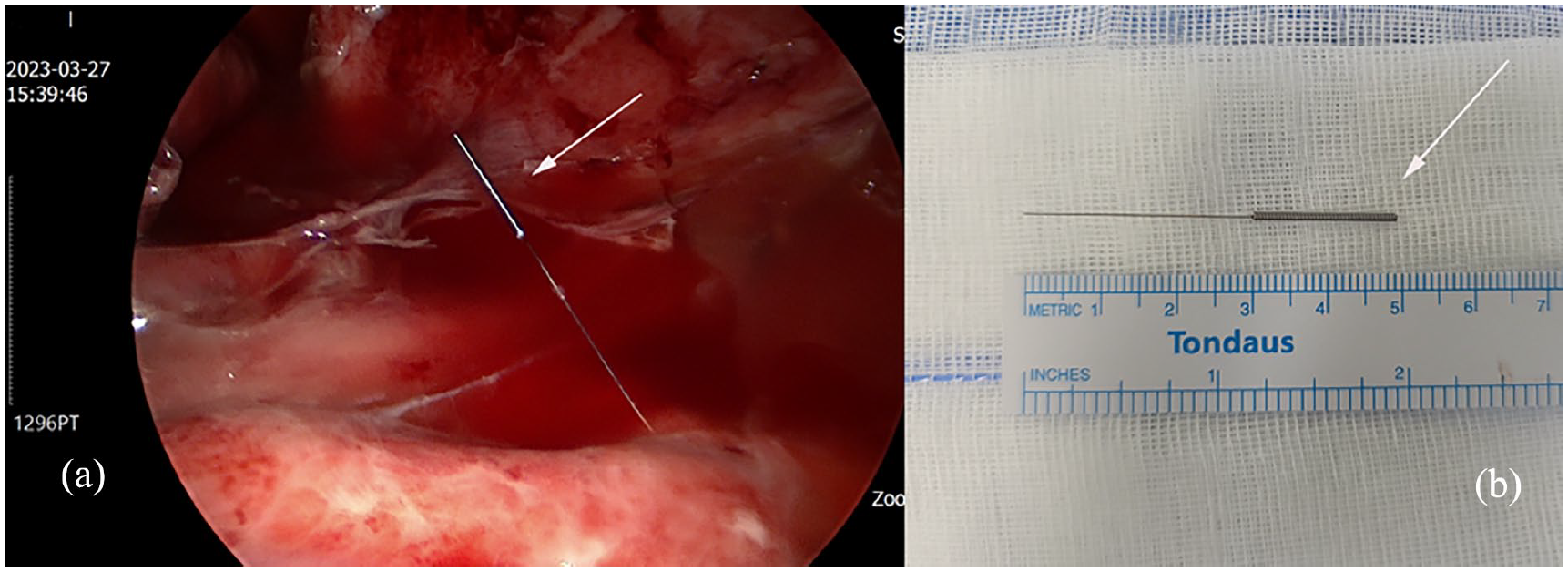
(a) Intraoperative view of the acupuncture needle (white arrow) seen extruded out into the pleural cavity. (b) Photograph of retrieved acupuncture needle (white arrow).
Comment
Acupuncture is being used for various indications—not just for pain but also commonly for the treatment of paresis following stroke or as a sequela of intracerebral hemorrhage. Patients with hemiplegia or quadriplegia do not always experience normal induced pain sensations and thus may frequently not notice a retained or missed acupuncture needle. Theoretically, a missed needle may be pushed further into a patient’s subcutaneous tissue and eventually into his or her pleural cavity. It seems less likely that the needle would have advertently been placed so deeply into the patient’s thoracic cavity at the time of the initial treatment, although there have certainly been many cases of pneumothorax occurring after acupuncture. 5 To our knowledge, there have been four other such cases of migration and penetration of the lung reported in the literature. 4 All of these cases involving an acupuncture needles penetrating the lung have induced infection and resulted in empyema. As suggested by Kim and his colleagues, if there is a missing needle after acupuncture treatment, or if symptoms such as a fever or dyspnea develops after acupuncture, meticulous radiologic examination using simple X-rays or CT should be performed and, if the needle is found, prompt attempts at early removal should be made immediately. 4 Early surgical removal may potentially prevent development of empyema and the need for a major decortication operation.