
Abstract
Background/Objective:
Tobacco use remains the leading cause of preventable death in the United States. The most widely available treatment options to assist patients in smoking cessation are limited by side effects and moderate efficacy at best. Acupuncture may be an effective option for smoking cessation. The goal of this study was to establish the need for and interest in acupuncture therapy to potentially assist with smoking cessation from a patient perspective.
Methods:
We conducted a cross-sectional survey study among patients aged 18 years or older whose medical record reported current tobacco use with English as their preferred language. REDCap surveys were administered to patients during office visits and included questions regarding opinions and use of all treatments available for smoking cessation (including acupuncture) as well as perceived barriers to acupuncture treatment.
Results:
A total of 57 surveys were distributed, and 42 (74%) were completed. Most patients reported previous attempts at quitting (76%) and had tried a variety of treatments including nicotine replacement (45%), Chantix (varenicline; 23%), Wellbutrin (bupriopion; 19%), “cold turkey” (65%) and hypnosis (3%). No respondents reported having tried acupuncture for smoking cessation.
Conclusion:
When comparing treatment options, patients reported more interest in acupuncture than other treatment options with a statistically significant difference in the level of interest between acupuncture and bupropion. All barriers (cost, time and effectiveness) were equally rated on a Likert-type scale with a median of 50 on a 101-point scale.
Keywords
Introduction
Tobacco use remains the leading cause of preventable death in the United States.1,2 Smoking cessation has been shown to reduce the financial burden on individuals and the healthcare system, improve quality of life, and add up to a decade of life for some patients.3,4 Most US adults want to quit smoking, yet most do not utilize evidence-based treatments, 5 and quitting often requires multiple attempts.5 –7 Currently approved medications to assist with smoking cessation include nicotine replacement therapy, bupropion (Wellbutrin) and varenicline (Chantix).7,8 These options have limitations in terms of relapse, adverse effects and the potential for abuse with nicotine replacement.6 –8 Therefore, there is a need to expand treatment options for smoking cessation.
Evidence has shown that complementary therapies such as acupuncture may be beneficial for smoking cessation.9,10 Acupuncture improves cessation rates when combined with other treatment modalities 11 and is a safe intervention for which many studies have reported no major adverse events. 10 There may infrequently be bleeding or bruising or, rarely, self-limited symptoms such as dizziness, headache or nausea. 10 Patient opinions regarding acupuncture treatment for smoking cessation have not been well studied.
The goal of this study was to establish patient interest in acupuncture therapy to assist with smoking cessation in the population studied. Specifically, the survey was intended to inform: (1) current smoking status and dependence of the study population; (2) interest in quitting; and (3) interest in and perceived barriers to participation in acupuncture. By providing this evidence, we anticipated that this study would contribute a basis for increased resources to support patients with the difficult task of smoking cessation.
Methods
Population
We conducted a cross-sectional survey study of adult English-speaking patients who were currently using tobacco at OhioHealth Riverside Family Practice Center (Columbus, OH, USA). The survey was distributed to all patients who were scheduled to come into the office for an in-person appointment and met the study criteria during the study period. Charts were reviewed 1 week in advance to identify patients who met the study criteria (current tobacco smoker, English speaking, adult). If a patient met the criteria, their upcoming appointment was labeled for survey distribution, and staff were tasked with giving them the survey when the patient was in their room waiting for the physician. While we could not ensure 100% staff compliance with this process, with our training and follow-up, we operated under a reasonable assumption that this process was followed for most patients. All identified patients were offered a survey upon arrival to their appointment. A brief summary of the purpose of the study was provided at the start of the survey that read as follows:
We are asking you to take part in a research project on acupuncture as a tool for smoking cessation. The project is being done by Kelsey Sicker, MD, from OhioHealth Riverside Family Medicine. The research will help us understand how to best meet the needs of people who are currently smoking and determine interest in making acupuncture services available to help with quitting. If you take part in this research study, it is voluntary and you may stop at any time without penalty or loss of benefit. All you need to do is complete this short survey, which should take about 15 minutes. If you do not wish to take part, simply discard the survey. You can refuse to answer questions that you do not wish to answer. Responses will be completely anonymous and kept confidential; your name will not appear anywhere on the survey.
The survey questions were self-administered on clinic iPads and could be completed at any time during the appointment and waiting periods in the clinic. The survey was conducted during a time of COVID-related social distancing, so waiting-room places were restricted, providing privacy during questionnaire completion. The survey was presented on REDCap (Research Electronic Data Capture) electronic data capture tools hosted at OhioHealth.12,13 REDCap is a secure, web-based software platform designed to support data capture for research studies that provide an intuitive interface for validated data capture, audit trails for tracking data manipulation and export procedures, automated export procedures for seamless data downloads to common statistical packages, and procedures for data integration and interoperability with external sources. All participants were informed of their rights as research participants by means of an electronic informed consent form that followed the aforementioned survey cover letter. The study was reviewed and approved by the OhioHealth Institutional Review Board.
Measures
Demographic information collected included age, gender, ethnicity, marital status, level of education, and yearly income. The survey also collected smoking history, opinions and use of treatments available for smoking cessation, and barriers to acupuncture as a tool to assist with smoking cessation.
Smoking history was characterized based on questions from the Fagerstrom Test for Nicotine Dependence (FND). 14 Interest levels and perceived barriers to acupuncture were assessed using 101-point Likert-type scales (where 0 indicates minimal interest and 100 indicates maximal interest). Surveys were collected from March 2021 through July 2021. This time frame was predetermined and chosen based on the calculated frequency of encounters with eligible patients.
Statistical analysis
Data analysis was completed using SAS v9.4. Surveys were considered completed if the patient clicked through all the questions, thus marking the survey as “complete” in the electronic survey system (even if they had skipped questions). Fifteen questionnaires were started but stopped before the patient got through all the questions; these were not included in the statistical analysis. We were unable to collect information on how many patients declined to start the survey. Nicotine dependence of the population that completed the survey was based on averaging the total score from the FND questions. Results for interest in quitting, perceived barriers and nicotine dependence were compared by each demographic variable collected. Statistical analysis was performed by Michelle Secic, MS.
All study data were summarized with descriptive statistics. Continuous variables were summarized with means and standard deviations or medians and ranges depending on data distribution. Categorical variables were summarized with counts and percentages. Data were summarized overall and separately by acupuncture interest groups (yes/no/don’t know). The chi-square test or Fisher’s exact test, as appropriate, were used to compare acupuncture interest groups. Interest scores were compared between treatments using Wilcoxon rank sum tests. No adjustments for multiple comparisons were planned. Results with p < 0.05 were considered statistically significant.
Results
A total of 57 surveys were distributed, and 42 (74%) were completed. Most respondents were female (57%) and non-Hispanic (97%). The most commonly reported highest level of education was a high school diploma or equivalent (81%). Annual income levels varied, with most being less than $30,000 (62%). Full demographic information can be found in Table 1, broken down by acupuncture interest groups (yes/no/don’t know). Only “completed” surveys were used for the data analysis. Some of the completed surveys had incomplete/unanswered questions, making “n” different throughout the table.
Demographics.
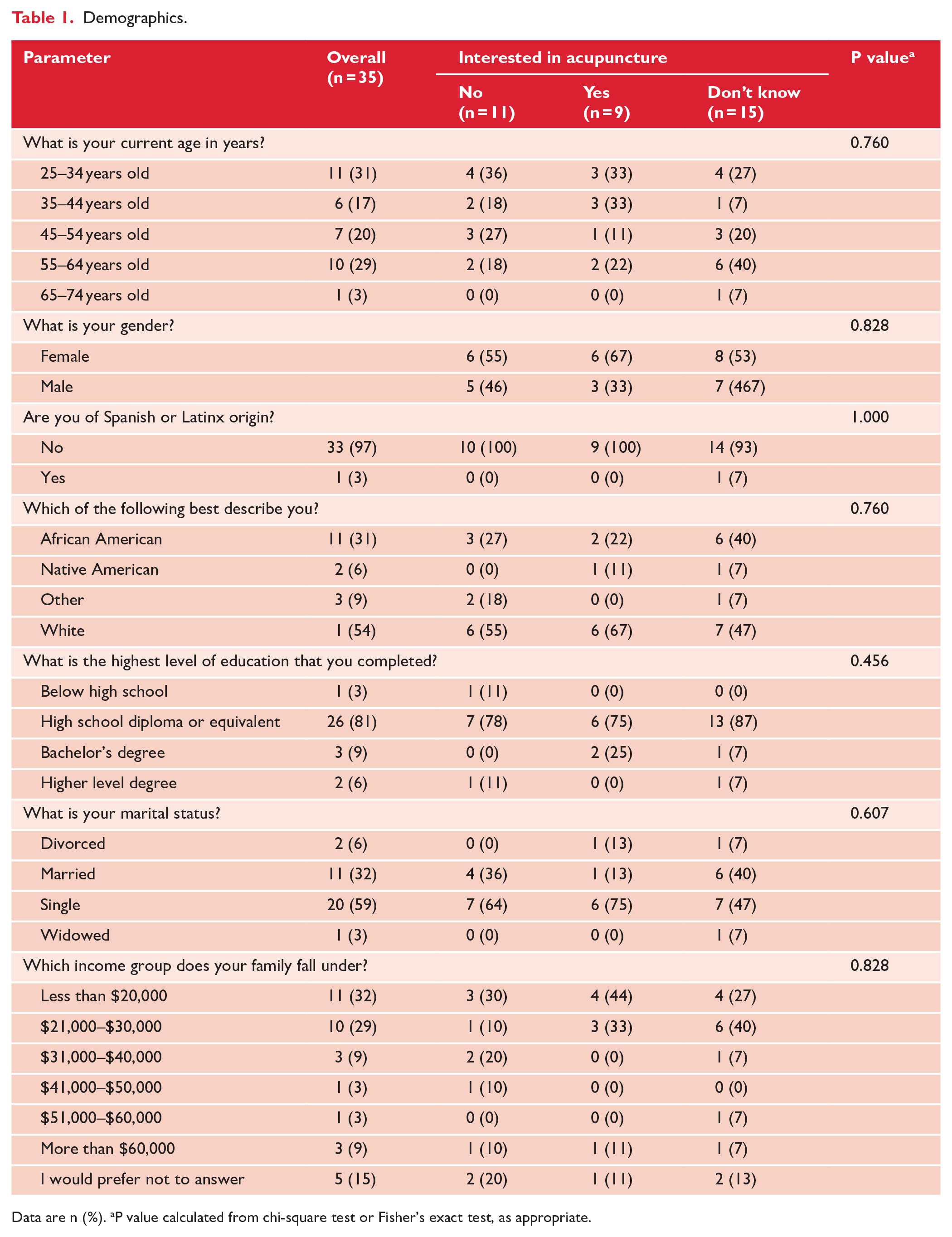
Data are n (%). aP value calculated from chi-square test or Fisher’s exact test, as appropriate.
Most surveyed patients reported daily cigarette smoking (83%). Based on the FND scoring system, the average score was 3.83 (95% confidence interval (CI): 3.43–4.23) which corresponds to a low level of dependence. Most patients reported previous attempts at quitting (76%) and had tried a variety of treatments including nicotine replacement (45%), varenicline (23%), bupropion (19%), “cold turkey” (65%) or hypnosis (3%). No respondents reported having tried acupuncture for smoking cessation. Of the 42 responders, 31 were at least somewhat interested in quitting including 13 (31%) who marked themselves down as “very interested.” Only 6 (14%) were not at all interested in smoking cessation.
When comparing treatment options, patient preferences were highest for “cold turkey,” followed by acupuncture, as shown in Figure 1. There was significantly more interest in acupuncture compared to bupropion (median interest scores 50 vs 1.5, respectively, p = 0.013). There was also a statistically significant greater level of interest in “cold turkey” compared with both bupropion and nicotine replacement. Other differences were not statistically significant.
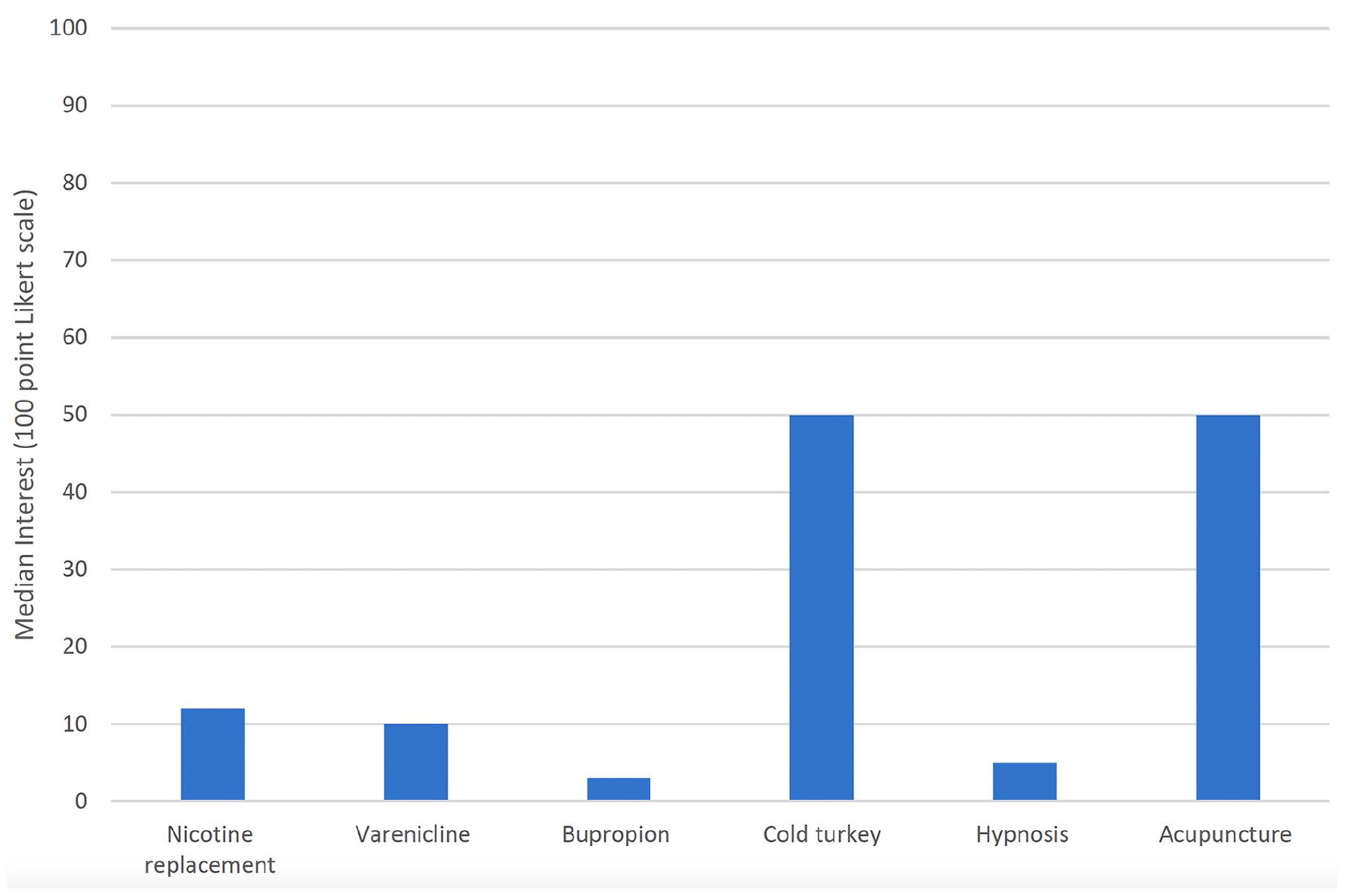
Interest in therapies for smoking cessation among patients who currently smoke cigarettes. Participants were asked to rate their level of interest in each therapy used for smoking cessation based on a 101-point Likert-type scale with higher scores indicating greater interest.
All perceived barriers were equally rated on a Likert-type scale with a median of 50 on a 101-point scale. Barriers assessed included cost, side effects, time commitment, and effectiveness.
Discussion
Patient perspectives on available treatments for smoking cessation have not been well studied. This survey study suggests that some patients are interested in acupuncture as an option to help with cessation efforts. The survey study design was specifically chosen in order to quantify patient interests and opinions despite possible limitations as described below.
This study’s generalizability is limited by sample size. Sample limitations were challenged by the COVID-19 pandemic, which limited in-person visits during the time of this study. There is also potential for social desirability bias, given the nature of the questions on a topic that may have strong social ties. The risk of transferability was minimized by allowing for anonymity and by researchers not being present during survey administration. There were no specific relationships between the participants and the researchers other than coincidental patient care in some cases. In addition, these results are at risk for selection bias because the written survey was only available in English, which limited the sample to patients who could read and write in English. By relying on documentation of smoking status in the electronic medical record, there was potential for errors, inaccuracy, or outdated information in patient selection. Patients may also have been rushed or interrupted when completing the survey because it was distributed during an office visit. This likely contributed to multiple surveys not being fully completed.
The survey itself had some limitations as well. An introduction and consent statement at the start of the survey specifically mentioned the goal of the study was to assess acupuncture as a tool for smoking cessation, possibly introducing bias toward acupuncture. The survey included a summary of treatments including known risks and benefits, of which the uncommon nature of adverse events with acupuncture treatments was mentioned and may have introduced some bias. The evaluation of barriers to acupuncture was limited because specific barriers were offered on the survey without the opportunity for patients to identify barriers independently. In addition, barriers to treatments other than acupuncture were not assessed.
The results of this survey show that patients who currently smoke cigarettes are interested in quitting and do have an interest in acupuncture to a degree that is comparable to or even greater than other specific treatment options commonly offered for smoking cessation. When comparing various patient demographics, there was no significant difference between each group’s levels of interest in acupuncture. Thus, the results suggest that patient-centered decision-making for all patients should include discussion regarding acupuncture as a treatment option for smoking cessation, among the other first-line treatment options. There were some perceived barriers to acupuncture treatment, but we anticipate that these results may prompt further resources for patients to learn about and access these treatments.
Conclusion
There was patient interest in acupuncture as an option for smoking cessation in this urban primary-care setting in the midwestern United States, although this interest was not very marked. There are perceived barriers to acupuncture including cost, time and effectiveness. Further studies are needed to expand the generalizability of these results. There is interest in supporting additional resources for acupuncture as a treatment option for smoking cessation.
Supplemental Material
sj-xlsx-1-aim-10.1177_09645284231206145 – Supplemental material for Patient interest in acupuncture for smoking cessation: a survey
Supplemental material, sj-xlsx-1-aim-10.1177_09645284231206145 for Patient interest in acupuncture for smoking cessation: a survey by Kelsey M Sicker, Michelle Secic, Anna Graham and Stephen E Auciello in Acupuncture in Medicine
Footnotes
Acknowledgements
The authors would like to recognize the faculty, residents and staff at OhioHealth Riverside Family Practice for their support and contributions to the completion of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.