
Abstract
Background:
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are a healthcare burden. Acupuncture improves dyspnea in patients with chronic obstructive pulmonary disease (COPD) but, to the best of our knowledge, has not been tested in AECOPD. Here, we evaluated the efficacy and safety of true acupuncture added to standard of care (SOC), as compared with both sham procedure plus SOC and SOC only, for the treatment of AECOPD among inpatients.
Methods:
This double-blinded randomized sham-controlled trial was set in a tertiary hospital in Israel. Patients with a clinical diagnosis of AECOPD were assigned to true acupuncture with SOC, sham procedure with SOC or SOC only. The primary outcome was dyspnea improvement as measured daily by the validated modified Borg (mBorg) scale. Secondary outcomes included improvement of other patient-reported outcomes and physiologic features, as well as duration of hospitalization and treatment failure. Acupuncture-related side effects were evaluated by the validated Acup-AE questionnaire.
Results:
Seventy-two patients were randomized: 26 to acupuncture treatment, 24 to sham and 22 to SOC only arms. Baseline characteristics were similar in the three groups. A statistically significant difference in dyspnea intensity was found from the first day of evaluation after treatment (p = 0.014) until day 3 after treatment. Similar results were found for sputum production, but no statistical significance was found when comparing physiologic features between the three arms. Acupuncture was not associated with adverse events.
Conclusion:
Acupuncture seems to be efficacious in the treatment of AECOPD among inpatients hospitalized in internal medicine departments.
Trial registration number:
NCT03398213 (ClinicalTrials.gov)
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a major health problem. Its prevalence varies between countries and has recently reached 25% of the adult population aged 40 and older in developed countries.1–3 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is defined as an event in the natural course of the disease characterized by a change in the patient’s baseline dyspnea, cough, and/or sputum that is beyond normal day-to-day variations, is acute in onset, and may warrant a change in regular medication in a patient with underlying COPD.
3
AECOPD leads to quality of life impairment and increased frequency of hospitalizations. According to the global initiative for chronic obstructive lung disease (GOLD), treatment of AECOPD involves inhaled bronchodilators, oral corticosteroids, antibiotics for cases of clinical airway infection and non-invasive mechanical ventilation for complicated cases with severe respiratory acidosis.3,4 Such treatments have been shown to be highly effective for the treatment of AECOPD. 3 However, side effects (mostly of systemic corticosteroids and antibiotics) are frequently encountered.
The addition of other therapeutic approaches may permit a reduction in dosing of currently used therapies, shorter time-to-recovery and duration of hospitalization and/or fewer complications. For instance, acupuncture, a complementary medicine technique, has been shown to be safe, including during hospitalization.5–7 It seems to improve clinical symptoms of stable COPD when added to standard of care (SOC) or compared to sham acupuncture.8–14 Moreover, acute dyspnea improved after acupuncture in conditions such as cancer, chronic bronchitis or asthma.5,15–17 A pilot study of nine patients with AECOPD has shown some encouraging results with acupuncture as compared to sham acupuncture, although no conclusion could be obtained from that study due to its low sample size. 18 A review summarizing clinical studies of acupuncture in the treatment of respiratory diseases in China in the past 10 years has shown promising results for the management of AECOPD, but the included studies were mainly low-quality trials. 19 To the best of our knowledge, no larger study has evaluated the efficacy and safety of acupuncture for treatment of AECOPD during hospitalization.
Due to the healthcare burden and serious implications of this condition, as well as the adverse effects of currently used therapies, our aim was to evaluate the efficacy and safety of true acupuncture as compared with both a sham procedure added to SOC, and SOC only, for the treatment of AECOPD among inpatients.
Methods
Study design
This was a three-arm (1:1:1) randomized controlled trial evaluating the efficacy and safety of the addition of acupuncture to SOC as compared to a sham procedure added to SOC (sham arm) and to SOC only (SOC arm) for treatment of AECOPD in patients hospitalized in internal medicine departments. The study protocol was reviewed and approved by the Institutional Review Board (IRB) in accordance with the Declaration of Helsinki (ethics approval no. 0108-17-BNZ) and prospectively registered at www.clinicaltrials.gov (NCT03398213) on 12 January 2018. Trial methods and results were reported according to the Consolidated Standards of Reporting Trials (CONSORT) 2010 guidelines 20 and acupuncture treatment was reported according to the Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines. 21
Participants
Patients hospitalized in internal medicine departments with a previous diagnosis of COPD 3 were evaluated by department physicians. Inclusion criteria included a previous diagnosis of COPD and a current clinical diagnosis of AECOPD as defined by the GOLD criteria. 3 Exclusion criteria included hemodynamic instability, a platelet count below 20 × 109/L, expected respiratory deterioration requiring mechanical ventilation in the next 24 h, or inability to provide informed consent. Primary sociodemographic (age, gender, comorbidities) and medical (smoking status, Charlson comorbidity index (CCI), COPD severity, pulmonary hypertension severity (based on mean pulmonary artery pressure (mPAP) and classified as mild if 25–40 mm Hg, moderate if 41–55 mmHg and severe if >55 mm Hg), number of hospitalizations for COPD exacerbation, Acute Physiology and Chronic Health Evaluation (APACHE)-II score, and current COPD treatment) data were recorded and compared between the three study groups.
Setting
The study was set in internal medicine departments of Bnai Zion medical center, a tertiary hospital in Haifa, Israel.
Randomization
Patients meeting inclusion/exclusion criteria were randomized to SOC with acupuncture (acupuncture arm), SOC with sham procedure (sham arm) or SOC only (SOC arm) using a 1:1:1 permuted block randomization list generated with Microsoft Excel software. To guarantee allocation concealment, randomization was done by an independent research assistant who did not participate in any other parts of the research and assigned the group code to each participant according to the randomization list. The list was preserved in an Excel table and concealed with passwords on both the Excel file and personal computer of the independent research assistant, who was blinded to the meaning of the group code.
Interventions
The intervention protocol was based on a literature review and Delphi process. A panel of eight acupuncturists of at least 5 years of experience in treating hospitalized patients were consulted. The experts were asked to review and analyze the literature regarding traditional Chinese medicine (TCM) and COPD, delineate relevant TCM syndromes and associated “critical” traditional acupuncture point locations and treatment frequency. Their suggestions were based on literature data and their professional experience. Finally, three cycles of stepwise anonymous discussions were taken to obtain a consensus on the treatment approach. The conclusion was to assign the patients into three groups for four daily consecutive treatment sessions and a 4-day follow-up.
SOC only
Patients received SOC for AECOPD according to a standard protocol based on the GOLD guidelines. 3 Such therapy included supplemental oxygen to maintain oxygen saturation (SaO2) around 90%, inhalations (both inhalers and nebulizers), antibiotics and systemic corticosteroids for 5 days. Non-invasive or mechanical ventilation was added depending on the severity of the AECOPD, as determined by clinical evaluation and blood gases.
True acupuncture + SOC group
The acupuncture was performed in a TCM style. During the Delphi process, a list of traditional acupuncture point locations historically used for acute lung conditions was determined and associated with different TCM syndromes. Practitioners systematically documented syndrome diagnosis according to TCM reasoning and used only points appearing in the list and corresponding to the TCM diagnosis (Supplemental Appendix 1). During the treatment, the acupuncturists used 75% alcohol pads to cleanse the skin at the planned needling sites. Subsequently, an average of five (range: 3–7) Eco FDA-approved sterile disposable needles (Maanshan Bond Medical Instruments CO. LTD, Maanshan, Anhui Province, China) of 3 cm length and 0.22 mm diameter were inserted. The puncture depth varied by anatomical location and ranged from 0.5 to 1 cm. Manual needle stimulation was performed, but de qi sensation (e.g. a sensation of dullness, sourness, heaviness and/or tingling around the needle) was not consistently achieved during the acupuncture sessions. Four consecutive daily sessions (15–20 min each day) were administered. Patients in this group also received SOC as described above. No other complementary medicine therapies were added. Explanations were given to patients regarding potential benefits and side effects of acupuncture and treatment was administered only after they signed informed consent.
Sham procedure + SOC group
Department physicians underwent a short training session on the placement of 0.5 cm × 0.5 cm medical sticking plasters (Leukoplast BSN medical) at three traditional ear acupuncture point locations that have no perceived relevance to lung conditions. Manual stimulation of the plasters was strictly avoided. The points were given names that provided some context relevant to the treatment (Zero, Sympathetic and Lung; Supplemental Appendix 2); however, they did not correlate with auricular acupuncture maps or “true” microsystems point terminology. During this training, physicians were taught that they were actually treating patients by ear stimulation and that the aim of the study was to compare the efficacy and safety of acupuncture administered by an experienced acupuncturist compared to verum acupressure administered by inexperienced medical staff after a short training. Patients were also told they were receiving therapeutic ear stimulation. Therefore, this study arm was intended to be double-blinded. The retention time was similar to that in the acupuncture group (15–20 min). SOC was administered as well, as described above.
Primary outcome
The primary outcome was dyspnea intensity pre- and post-treatment in the 4 days of follow-up. It was measured daily, before and 1 h after treatment (for acupuncture and sham groups) or after first evaluation (for SOC group), via the modified Borg (mBorg) scale, which is a validated scale that has been used to evaluate the degree of dyspnea (0 = no dyspnea, 10 = worse dyspnea) in both stable COPD and AECOPD.22,23 Dyspnea intensity was chosen as the primary outcome, since it has been shown to predict clinical outcomes in AECOPD. 24
Secondary outcomes
Variation of clinical symptoms
This included cough intensity and sputum production associated with AECOPD, as evaluated on a visual analogue scale (VAS) from 0 (no symptoms) to 10 (maximally symptomatic), throughout the 4 days of evaluation.
Variation of physiologic features
Venous blood gases (pH and partial pressure of carbon dioxide (pCO2)) and SaO2 were measured before the intervention and daily on the four evaluation days. Respiratory rate (RR) was measured daily, before and 1 h after treatment (for acupuncture and sham groups) or after first evaluation (for SOC group).
Treatment failure
This was defined as death during hospitalization or need for non-invasive or mechanical ventilation. The incidence of treatment failure was evaluated and compared between the three groups.
Duration of hospitalization
This was evaluated and compared between the three study arms.
Safety
Acupuncture-related side effects were systematically evaluated after treatment in the acupuncture group via the validated Acup-AE questionnaire, which was administered to the patient by the acupuncturist immediately after the treatment. 24
Sample size estimation
In a previous study evaluating the efficacy of acupuncture versus sham acupuncture in 68 patients with chronic COPD (34 patients in each group), a 3.6 ± 1.9 unit improvement in dyspnea (on the mBorg scale) was found in the acupuncture arm, compared with a 0.4 ± 1.2 unit improvement in the sham acupuncture arm. 8 According to these data, using analysis of variance (ANOVA) with alpha of 0.05 and 80% power, we calculated a minimal sample size of 66 patients (22 in each group) would be required for this study.
Blinding
Data collectors, department physicians, physicians administering the sham procedure and the statistician were blinded to the group allocation status. Acupuncturist blinding is clearly not possible; however, contact time with patients was the same in both acupuncture and sham arms (15–20 min). Patients receiving both true acupuncture and the sham procedure were told they were being treated for their respiratory condition by acupuncture/acupressure. The group allocation status was only revealed after completion of the study.
Statistical analysis
Demographic and clinical data were analyzed at baseline to measure the balance among the study groups. Quantitative variables were described using mean ± standard deviation or median and 25th–75th percentiles (quartile (Q)1, Q3) depending on their distribution. Qualitative variables were described using frequency and percentage distributions. Next, we showed that our variables distributed equally between the study groups. To compare normally distributed variables between study groups, we used ANOVA. To compare variables that did not distribute normally between study groups, we used the Kruskal–Wallis test with adaptation to pairwise comparison. To compare qualitative variables between study groups, we used the independent chi-square test and Fisher exact test. Bonferroni adjustment was used for multiple comparisons for each independent comparison of acupuncture versus sham, acupuncture versus SOC and sham versus SOC groups. Since the variation of dyspnea intensity between day 1 and day 2 had a normal distribution, a multivariate linear regression analysis was performed after collinearity, interaction and confounding analysis, in order to neutralize the effect of the different sociodemographic and medical covariates on the primary outcome in the three study arms. Adjusted unstandardized regression coefficients were reported with confidence interval (CI), while p < 0.05 was considered statistically significant. Data analysis was performed using IBM’s Statistical Package for the Social Sciences (SPSS) version 22 (SPSS Inc., Chicago, IL, USA). Of note, both per-protocol and intention-to-treat analyses were planned, but since there was no patient cross-over, there was no need to differentiate between the analyses.
Results
Baseline patient data
A total of 104 patients were screened for eligibility. Among them, 72 met inclusion criteria and were recruited between 14 January 2018 and February 2020. Twenty-six of them were assigned to the acupuncture arm, 24 to the sham arm, and 22 to the SOC arm. Baseline demographic and clinical characteristics were similar in patients from the three study arms, as shown in Table 1. Of note, all patients randomized (regardless of group allocation) completed treatments per-protocol (Figure 1).
Baseline characteristics.
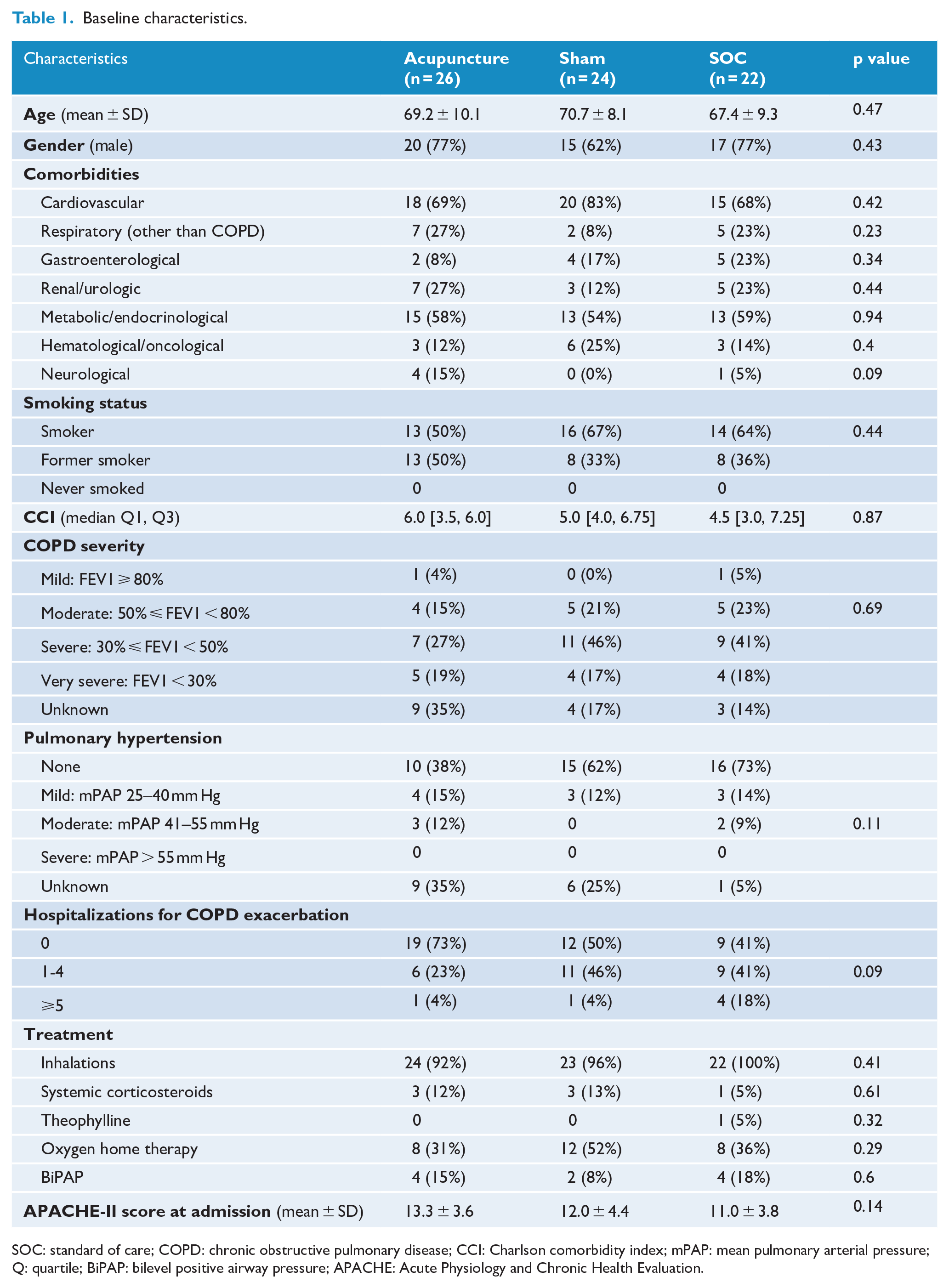
SOC: standard of care; COPD: chronic obstructive pulmonary disease; CCI: Charlson comorbidity index; mPAP: mean pulmonary arterial pressure; Q: quartile; BiPAP: bilevel positive airway pressure; APACHE: Acute Physiology and Chronic Health Evaluation.
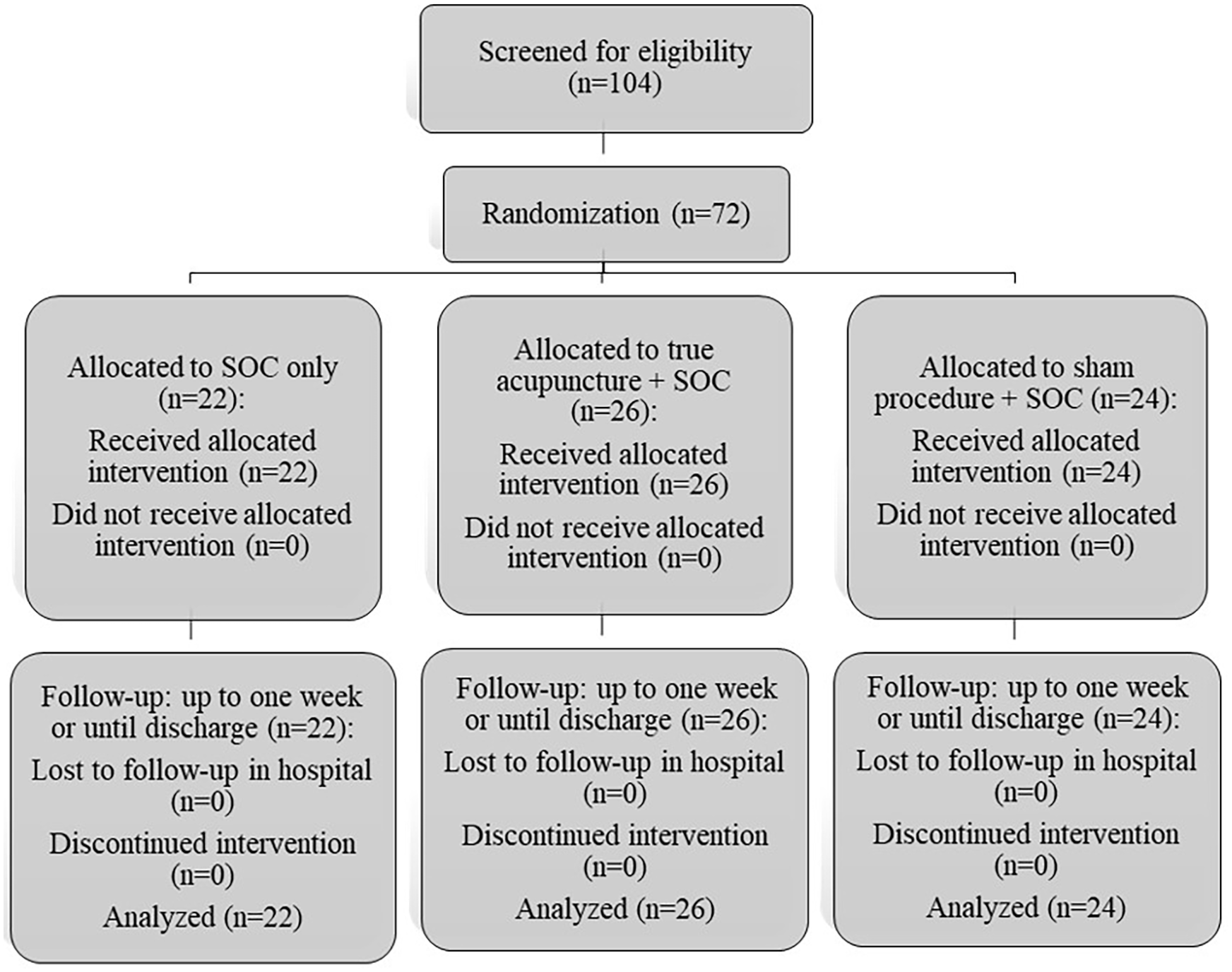
Flow chart of the trial. SOC: standard of care.
Primary outcome
Baseline dyspnea was similar in the three groups. A statistically significant reduction between the three groups in dyspnea intensity, reflected by lower mBorg scores (median Q1, Q3) was found from the first day of evaluation after treatment in the acupuncture group (5.0 (4.0, 5.0)) compared to both sham (6.0 (4.25, 7.875), p = 0.031, effect size d = 0.98 (large to very large)) and SOC (7.5 (5.5, 8.0), p = 0.014, effect size d = 2.07 (very large)) with no significant difference between sham and SOC (p = 0.34) until day 3 after treatment (Table 2). After adjustment for covariates in a multivariate linear regression analysis, the association of study arm with improvement of dyspnea from day 1 to day 2 remained statistically significant (Table 3).
Comparison of continuous data between the three study groups.
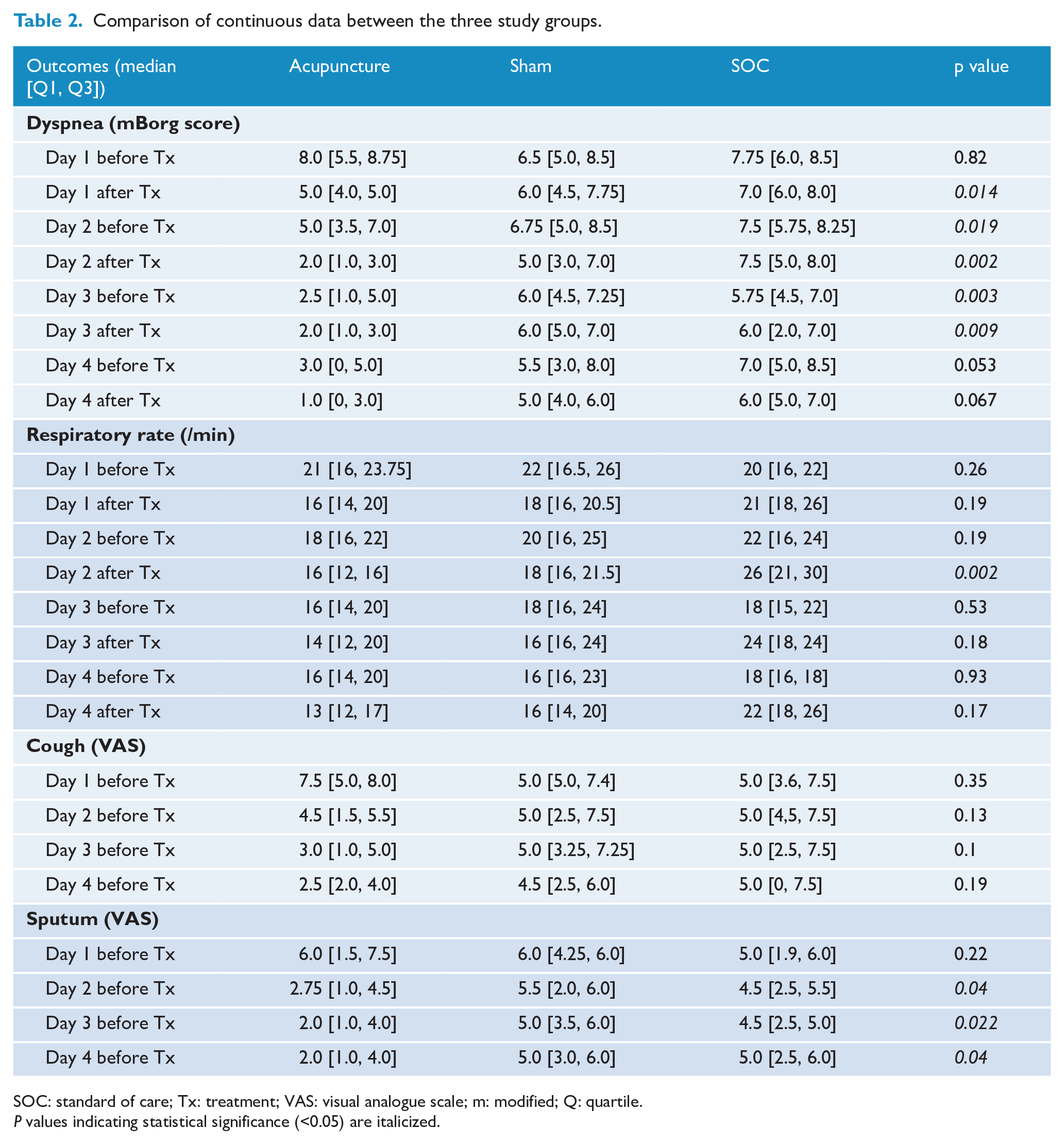
SOC: standard of care; Tx: treatment; VAS: visual analogue scale; m: modified; Q: quartile.
P values indicating statistical significance (<0.05) are italicized.
Multivariate linear regression analysis on variation of dyspnea from day 1 to day 2.
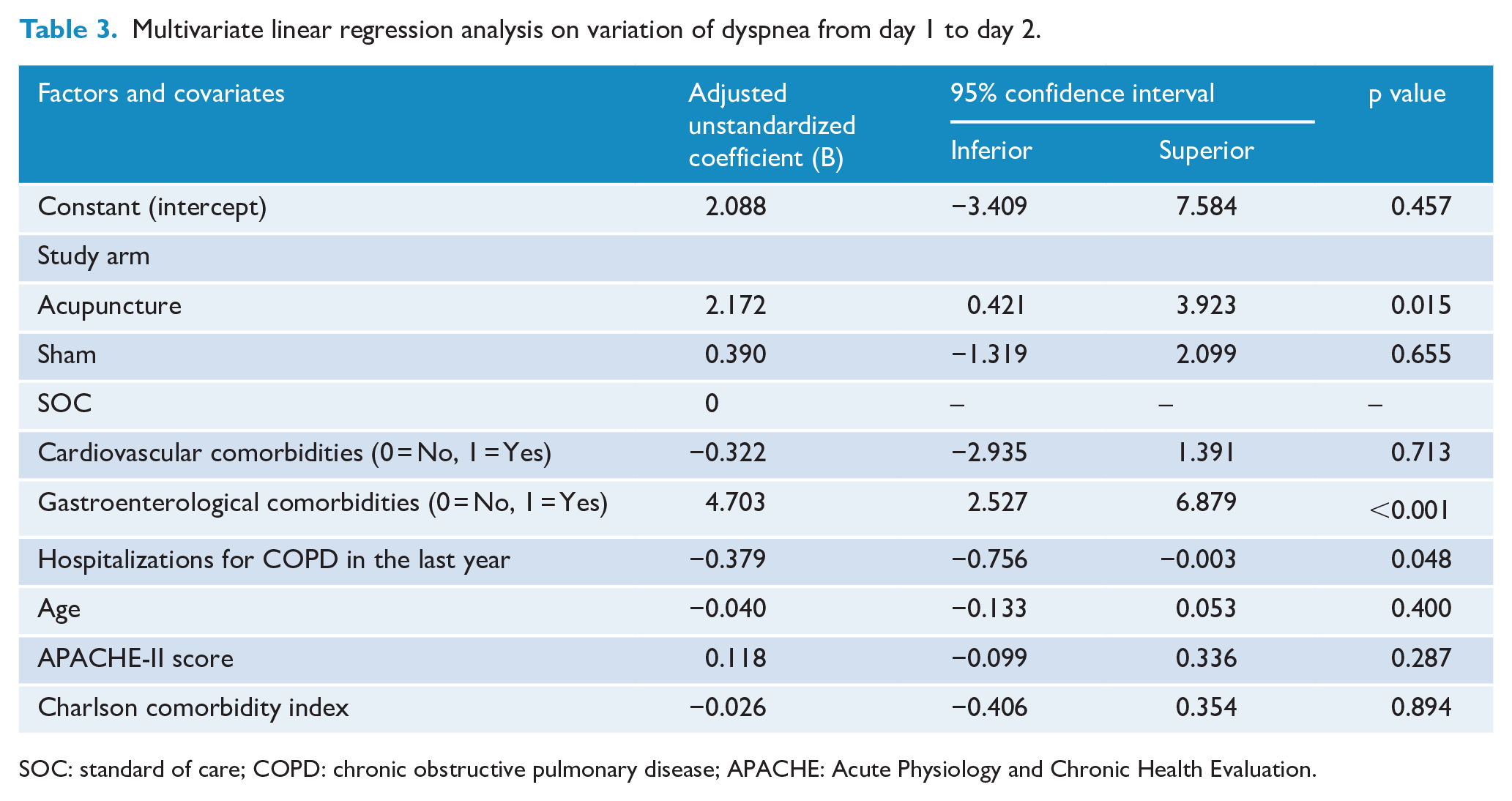
SOC: standard of care; COPD: chronic obstructive pulmonary disease; APACHE: Acute Physiology and Chronic Health Evaluation.
Secondary outcomes
Patient-reported outcomes
Baseline VAS scores for cough and sputum intensity were similar in the three study arms (Table 1). No statistically significant difference in cough intensity was observed between the three study arms throughout the 4 days of follow-up (Table 2). However, a statistically lower level of sputum production was observed in the acupuncture arm compared with sham and SOC from day 2 (p = 0.04; Table 2). Post hoc analysis showed a statistically significant difference between acupuncture and sham on day 2 (p = 0.024, effect size d = 0.70 (medium to large)), day 3 (p = 0.010, effect size d = 0.74 (medium to large)) and day 4 (p = 0.018, effect size d = 1.03 (large to very large)). A significant difference between acupuncture and SOC was only observed on day 2 (p = 0.044, effect size d = 0.70 (medium to large)), and there were no statistically significant differences between sham and SOC groups.
Physiologic assessment
Baseline physiologic data were similar in the three groups. A statistically significant difference was observed in RR at day 2 after treatment (p = 0.002), with significant differences both between acupuncture and sham groups (p = 0.005, effect size d = 1.09 (large to very large)) and between acupuncture and SOC groups (p = 0.003, effect size d = 2.18 (very large)), but not between sham and SOC groups (p = 0.050). All other RR measurements were statistically similar between the three arms throughout the 4 day follow-up (Table 2).
Concerning pH, a statistically significant difference between the three groups was observed at day 4 (p = 0.048), although post hoc analysis did not show any statistical significance when comparing groups head-to-head (Figure 2(b)).
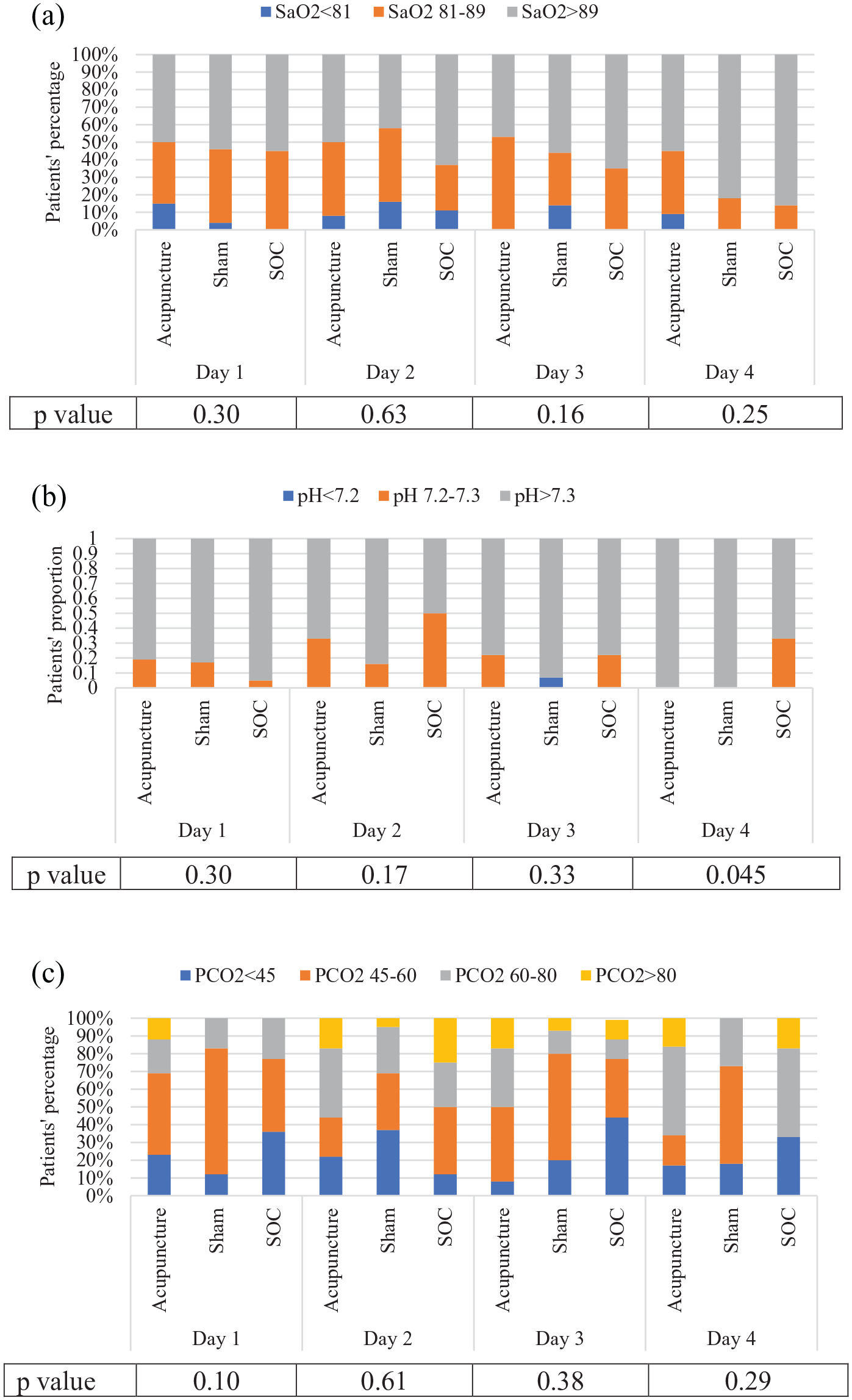
Between-group comparison of qualitative variables. SOC: standard of care; pCO2: partial pressure of carbon dioxide; SaO2: oxygen saturation.
No statistically significant difference was observed when comparing other physiologic measures between the three study groups (Figure 2).
Treatment failure
No death or mechanical ventilation occurred in the study participants during follow-up. However, there were a total of four treatment failures, all of which were non-invasive ventilations, occurring in two patients (8%) in the acupuncture arm, one (4%) in the sham arm and one (5%) in the SOC arm (p = 0.83).
Duration of hospitalization
No difference was noted in terms of duration of hospitalization between the three study arms (5.5 ± 2.3 days for acupuncture vs 6.0 ± 2.9 days for sham and 6.3 ± 2.9 days for SOC, p = 0.05).
Safety
No side effects of acupuncture were reported during the study period, as assessed by the Acup-AE questionnaire.
Discussion
The addition of acupuncture to usual care seems to be effective and safe in the treatment of AECOPD in internal medicine departments, judging by the improvements in patient-reported outcomes. However, physiologic features did not seem to be impacted.
This study was a three-arm randomized controlled trial. This design was chosen to assess both specific (acupuncture vs sham) and non-specific (sham vs SOC) effects of acupuncture in the treatment of AECOPD. In order to reliably evaluate both of these effects, a sham procedure must be credible, defined as both indistinguishable from true acupuncture, as evaluated by patient-filled questionnaires,18,25 and inactive (defined by some as not producing a typical acupuncture needle sensation), as verified by expert opinion. 26 In this study, we chose not to reveal to patients and sham providers that one of the study arms was sham-based. We designated the sham intervention “non-penetrating acupuncture point stimulation” to achieve two goals, the first of which was directed toward patients, allowing the non-specific effects of the sham procedure, and the second of which was to enable an authentic treatment scenario by the medical staff who believed they were providing a credible intervention. Moreover, contextual factors (including provider intent, ceremonial aspects and attention) were similar in acupuncture and sham groups. For these reasons, although credibility could not be systematically evaluated via validated questionnaires, we consider our procedure to have been credible, allowing comparability of both interventions for non-specific effects.
While a statistically significant effect of acupuncture on patient-reported outcomes of AECOPD was achieved, one may wonder whether these results are clinically significant. In a manuscript reviewing the different breath-related scores, the minimally clinically important differences in both VAS and Borg scales were determined as one unit, 27 which was reached in this study from day 1 after treatment for median dyspnea as compared to control groups.
While this study shows positive specific effects of acupuncture on patient-reported outcomes in AECOPD, it does not appear that acupuncture influences physiologic features (e.g. oxygen saturation, blood gases). Former studies do not support our findings, as a meta-analysis of the effects of acupuncture on stable COPD recently showed improvements in both functional/quality of life and physiologic parameters (pulmonary function), although most of the reviewed studies were low quality. 11 Another study focusing on mechanically ventilated patients showed improvement in respiratory indices after acupressure treatment. 28 This discrepancy may be related to the fact that most of the patients recruited in this study were hospitalized in internal medicine departments and not intensive care units (ICUs), so the severity of AECOPD was generally mild-moderate, and the desaturations and respiratory acidosis that were observed were not generally different from patients’ baselines, so significant physiologic improvement might not be expected. On the other hand, the relative respiratory stability of our participants allowed us to evaluate patient-reported outcomes more reliably (via scales that may be difficult to administer in the ICU). Another explanation may be related to the fact that patient-reported outcomes and physiologic features reflect different aspects of AECOPD; both measurements have limitations and are only mildly correlated.29,30 For these reasons, and following the positive endpoints in patient-reported outcomes and safety delineated in this study, a future separate study should concentrate on the specific physiologic effects of acupuncture on critically ill patients with AECOPD.
Obviously, improving patient well-being and reducing suffering is of great importance in itself. However, diminishing dyspnea may have additional valuable consequences. It has been shown that, in patients with COPD, a high perception of respiratory exertion, that is, increased sensation of dyspnea, reduces the effort exerted to overcome increased respiratory resistance. 31 Apparently, patients adopt a compromise between the drive to increase effort to maintain adequate ventilation and the desire to reduce the negative sensation elicited by this increase in effort. Accordingly, reducing dyspnea is expected to also have a beneficial effect on respiratory activity during AECOPD.
The specific effects of acupuncture delineated in this study do not resonate with findings from preceding studies where the effects of sham acupuncture and verum acupuncture did not differ.32–34 There are two possible explanations for this discrepancy. As opposed to pain syndromes, alleviation of dyspnea may be less responsive to non-specific effects of acupuncture. In addition, our sham procedure involved a non-penetrating approach, which may have triggered fewer and/or weaker mechanical non-specific effects. Future explanatory studies should tease out the various non-specific effects of sham acupuncture procedures.
According to this study, an immediate reduction of dyspnea was observed after each acupuncture session as compared with control groups, with a new increase the following day, before the next treatment session. This may have been related to an immediate short-term effect of acupuncture, as previously described for acupressure in mechanically ventilated patients. 29 However, measurement of acupuncture time-effect should be further evaluated since, as described in a recent review, it has generally not been measured systematically and there are no consistent data on the immediate, post- and total time-effect of acupuncture. 35 Specifically, in the current clinical context, calculating the half-life of the acupuncture effect may determine the need for longer or more frequent sessions, as well as its timing related to conventional therapies that may potentiate possible synergistic effects.
Indeed, positive effects of both conventional and other complementary medicine techniques (reflexology, mindfulness) in the treatment of COPD have been shown in previous studies.36,37 The specific acupuncture outcomes delineated in this study suggest an “at least additive” effect of acupuncture with SOC. However, in this era of integrative medicine, synergism should be evaluated in the combination of acupuncture with conventional or other complementary therapies.38,39 This may allow for the reduction of medications with side effects in patients treated with acupuncture, as shown in most of the studies summarized in a critical analysis on acupuncture in pulmonary conditions. 5
Limitations
The single-center study design may limit the generalizability of our findings, although the population was heterogeneous in terms of sociodemographic and clinical background. Furthermore, the absence of acupuncturist blinding to type of treatment, which is not feasible for now, may have introduced performance bias, which was reduced by using a “sham practitioner,” as well as assessor blinding (to minimize detection bias). Another limitation was the absence of analysis of the potential effect of acupuncture on dose of conventional therapies. Further studies should systematically analyze and compare the types and doses of medications in the study arms to examine for a potential reduction attributable to acupuncture use. Finally, although we achieved the minimal sample size, the relatively low number of patients may limit interpretations of our multivariate linear regression analysis, though the model was statistically significant.
Conclusion
Acupuncture seems to be effective and safe in the treatment of AECOPD among inpatients hospitalized in internal medicine departments, with apparent short-term effects on dyspnea intensity. Further studies should evaluate the time-effect of acupuncture in this setting, as well as its physiologic effects among both critically ill patients and outpatients.
Supplemental Material
sj-docx-1-aim-10.1177_09645284221086293 – Supplemental material for Treatment of acute exacerbations of chronic obstructive pulmonary disease with acupuncture during hospitalization: a three-arm double-blinded randomized sham-controlled trial
Supplemental material, sj-docx-1-aim-10.1177_09645284221086293 for Treatment of acute exacerbations of chronic obstructive pulmonary disease with acupuncture during hospitalization: a three-arm double-blinded randomized sham-controlled trial by Ilana Levy, Yotam Elimeleh, Sagi Gavrieli, Samuel Attias, Ariel Schiff, Arie Oliven and Elad Schiff in Acupuncture in Medicine
Supplemental Material
sj-jpg-2-aim-10.1177_09645284221086293 – Supplemental material for Treatment of acute exacerbations of chronic obstructive pulmonary disease with acupuncture during hospitalization: a three-arm double-blinded randomized sham-controlled trial
Supplemental material, sj-jpg-2-aim-10.1177_09645284221086293 for Treatment of acute exacerbations of chronic obstructive pulmonary disease with acupuncture during hospitalization: a three-arm double-blinded randomized sham-controlled trial by Ilana Levy, Yotam Elimeleh, Sagi Gavrieli, Samuel Attias, Ariel Schiff, Arie Oliven and Elad Schiff in Acupuncture in Medicine
Footnotes
Contributors
IL, SG, SA, AO and ES wrote the study protocol including conceptualization and design. SG and ES performed the acupuncture intervention. IL and YE collected the data. IL, AS and ES analyzed the data. IL and YE wrote the first draft of the manuscript, directed by ES. The manuscript was then reviewed by SG, SA, AS and AO. All authors read and approved the final version of the manuscript accepted for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.