
Abstract
Objective:
The aim of this study was to systematically assess the effectiveness and safety of acupuncture for patients with atopic eczema (AE).
Methods:
Two reviewers searched 13 databases from their inception through 31 July 2018 for randomized controlled trials (RCTs) of patients with AE. Dichotomous data and continuous data were analyzed using risk ratio (RR) and mean difference (MD), respectively, with 95% confidence intervals (CIs).
Results:
A total of eight RCTs (with 434 participants) were included. The results of one included RCT showed that acupuncture was better than no treatment at reducing itch intensity measured using a visual analogue scale in patients with AE. The combined results of six RCTs showed that acupuncture was better than conventional medicine at reducing the eczema area and severity index (EASI) (MD: −1.89, 95% CI: −3.04 to −0.75, I2: 78%) and the combined results of seven RCTs showed that acupuncture was better than conventional medicine in terms of global symptom improvement (RR: 1.59, 95% CI: 1.20 to 2.11, I2: 55%) in AE. We had insufficient data to show significant effects of acupuncture on quality of life and AE recurrence rate. No severe adverse events were found related to acupuncture.
Limitations:
The included RCTs had some methodological limitations, and most of the included trials were conducted in China. This analysis only included studies that compared acupuncture alone with no treatment or positive control (conventional medicine), so the specific effects of acupuncture could not be evaluated.
Conclusion:
Acupuncture might be effective at reducing itch intensity and may be more effective than conventional medicine at reducing EASI and improving the global symptoms of AE.
Protocol registration:
PROSPERO CRD42018096261
Introduction
Atopic eczema (AE) is a common inflammatory, pruritic, and chronically relapsing dermatological disease that results in frequent exudates and severe pruritus.1,2 In China, AE is also called chronic eczema (CE). The prevalence of AE is approximately 20% in children and 1%–3% in adults in most western countries. 2 Itching, dry skin, and lichenification are the main symptoms of AE. With regards to disease management, 75% of patients and their caregivers believe that effectively controlling symptoms can improve quality of life. 2 Currently, treatments for AE include emollients and topical corticosteroids, which have generally been well-tolerated.2,3 However, long-term use of topical corticosteroids may lead to resistance, dependence, and a variety of other side effects, such as skin atrophy, atrophic striae, and rosacea-like eruptions.2,4
Acupuncture has been widely applied for the treatment of many chronic diseases, especially dermatological conditions.5,6 Some clinical trials have demonstrated that acupuncture can significantly reduce itch intensity and allergen-induced basophil activation in patients with AE.7,8 Three systematic reviews related to acupuncture for AE have been published since 2014, but the poor quality of the inclusion criteria in these reviews may have biased the overall conclusion.9–11 New randomized controlled trials (RCTs) investigating the effects of acupuncture for managing AE have been published in the past 4 years, but there has been no systematic review of the effects of acupuncture for AE including these newer clinical trials. Therefore, we integrated the latest research studies and systematically assessed the effectiveness and safety of acupuncture for the treatment of AE, with the aim of providing clinicians some direction with respect to their use of acupuncture to manage AE.
Methods
This systematic review and meta-analysis was registered in the PROSPERO database at http://www.crd.york.ac.uk/PROSPERO (ref. CRD 42018096261) and performed according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. 12
Study inclusion criteria
Study type
We included all RCTs that were published in English or Chinese. Non-randomized controlled trials, quasi-randomized controlled trials, retrospective studies, medical record reports, reviews, and summary of articles were excluded.
Participants
Participants in all studies were diagnosed with either AE or CE.1,2 There were no age, gender, or race restrictions.
Study interventions
Studies of the following penetrating forms of acupuncture were included: body acupuncture, scalp acupuncture, manual acupuncture, ear acupuncture, electroacupuncture, fire needling, dermal needling, plum blossom needling, and abdominal acupuncture. Combined interventions, defined as the use of two different forms of acupuncture, were also included. We excluded moxibustion, traditional acupuncture point injections, laser acupuncture, cupping, pricking, blood-letting, and any acupuncture therapy combined with Chinese herbs.
Comparisons of interest included the following:
Acupuncture versus no treatment (effectiveness);
Acupuncture versus sham/placebo acupuncture (efficacy);
Acupuncture versus conventional medicine (comparative effectiveness);
Acupuncture combined with conventional medicine versus the same conventional medicine (effectiveness as an adjunct).
Study outcome measures
Trials using one or more of the following outcome measures were included.
Primary outcomes
Eczema area and severity index (EASI)
Severity scale was based on AE symptom severity relative to body area, size of AE, and proportion of each body region. 13 The scale ranged from 0 to 72 (0 = none, 72 = most severe).
Itch intensity measured by visual analogue scale (VAS)
The VAS scale ranged between 0 (0) and 10 (100) to assess AE itch degree (0 = none, 10 (100) = most severe). 14
Severity scoring of atopic dermatitis (SCORAD)
The scale assessed AE severity according to the extent, severity, and subjective symptoms of AE ranging between 0 and 103 (0 = none, 103 = most severe). 15
Secondary outcomes
Global symptom improvement
Global symptom improvement was based on the EASI score. Effect index was calculated as (EASI baseline score − EASI score after treatment)/EASI baseline score × 100%.
Quality of life
We used the short form (SF)-12, SF-36, or other self-made questionnaires related to quality of life, recurrence rate, and adverse events.
Electronic search methods for study identification
Two reviewers searched the following databases from their inception to 31 July 2018: The Cochrane Library, PubMed, Embase, CiNi, Medical Online, Korea Science, Chinese Biomedical (CBM) database, China National Knowledge Infrastructure (CNKI), Chinese Medical Current Content (CMCC), Chinese Scientific Journal database (VIP), and WanFang database. Studies were searched using the inclusion and exclusion criteria with no language restrictions. We also searched academic dissertation databases and conference paper databases in CBM and CNKI, the New York Academy of Medicine Grey Literature Report (www.greylit.org), and the Electronic Theses Online Service through the British Library (http://ethos.bl.uk) for unpublished literature, conference papers, doctoral and masters theses, and other published literature. The search strategy was based on the Cochrane handbook guidelines 16 and is presented in Table 1.
Search strategy for PubMed database.
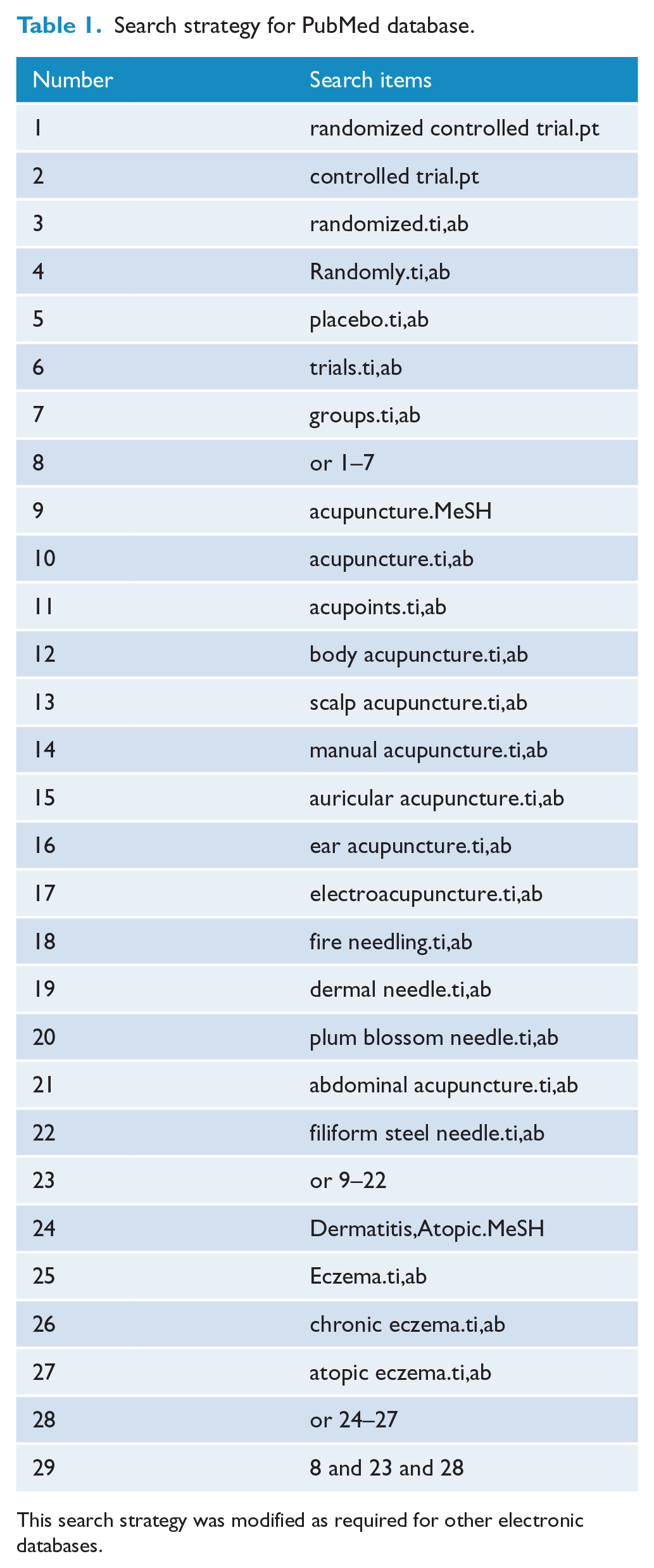
This search strategy was modified as required for other electronic databases.
Data extraction and management
Two reviewers independently used a pre-designed data extraction table to extract data from the included trials. The data extraction table mainly included the following aspects: general information, study design and methods, participants, interventions, outcomes, and adverse events. Any disagreements were resolved by discussion between the two reviewers. If no agreement was made, arbitration by a third person resolved the issue. If the relevant content of the included trials was incomplete, we first filled out the data extraction form and then contacted the study author by phone or email to acquire information.
Risk of bias assessment
The included studies were independently assessed by two reviewers using the Cochrane Handbook for Systematic Reviews to determine risk of bias. 17 Study quality was evaluated according to seven aspects: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Each category was scored as low, unclear, or high risk of bias. Disagreements were resolved by discussion between the two reviewers. If no agreement was reached, arbitration by a third person resolved the issue. If 10 or more studies were included in the meta-analysis, we had intended to use funnel plots to analyze potential publication bias.
Data analysis
We used Revman V.5.1 software to analyze the data. Dichotomous data were analyzed using risk ratio (RR) and 95% confidence intervals (CIs). Continuous data were analyzed using mean differences (MDs) with 95% CI. We attempted to obtain missing data from the original studies and data were analyzed using the intention-to-treat (ITT) principle. When we could not obtain sufficient data, we based our analysis on the available data.
Depending on the I2 statistic, we applied fixed-effect or random-effect models to estimate the pooled effect size. A p value <0.05 was considered statistically significant. When there was obvious heterogeneity (I2 > 50%) among the included studies, we performed sensitivity analyses to identify the source of heterogeneity. We were unable to perform a subgroup analysis due to an insufficient number of eligible trials.
Level of evidence
The primary outcomes and global symptom score improvement were also assessed using levels of evidence as determined by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE). These outcomes were assessed based on five domains: risk of bias, consistency, directness, precision, and publication bias. The level of evidence for these outcomes was categorized as high, moderate, low, or very low.18,19
Results
Study selection
We identified a total of 370 records through electronic searches, of which 140 duplicates were excluded. We excluded a total of 204 studies by screening the titles and abstracts, and 18 studies were excluded after screening the full-texts. A total of eight RCTs met the inclusion criteria.8,20–26 A flow diagram of the study selection is displayed in Figure 1.
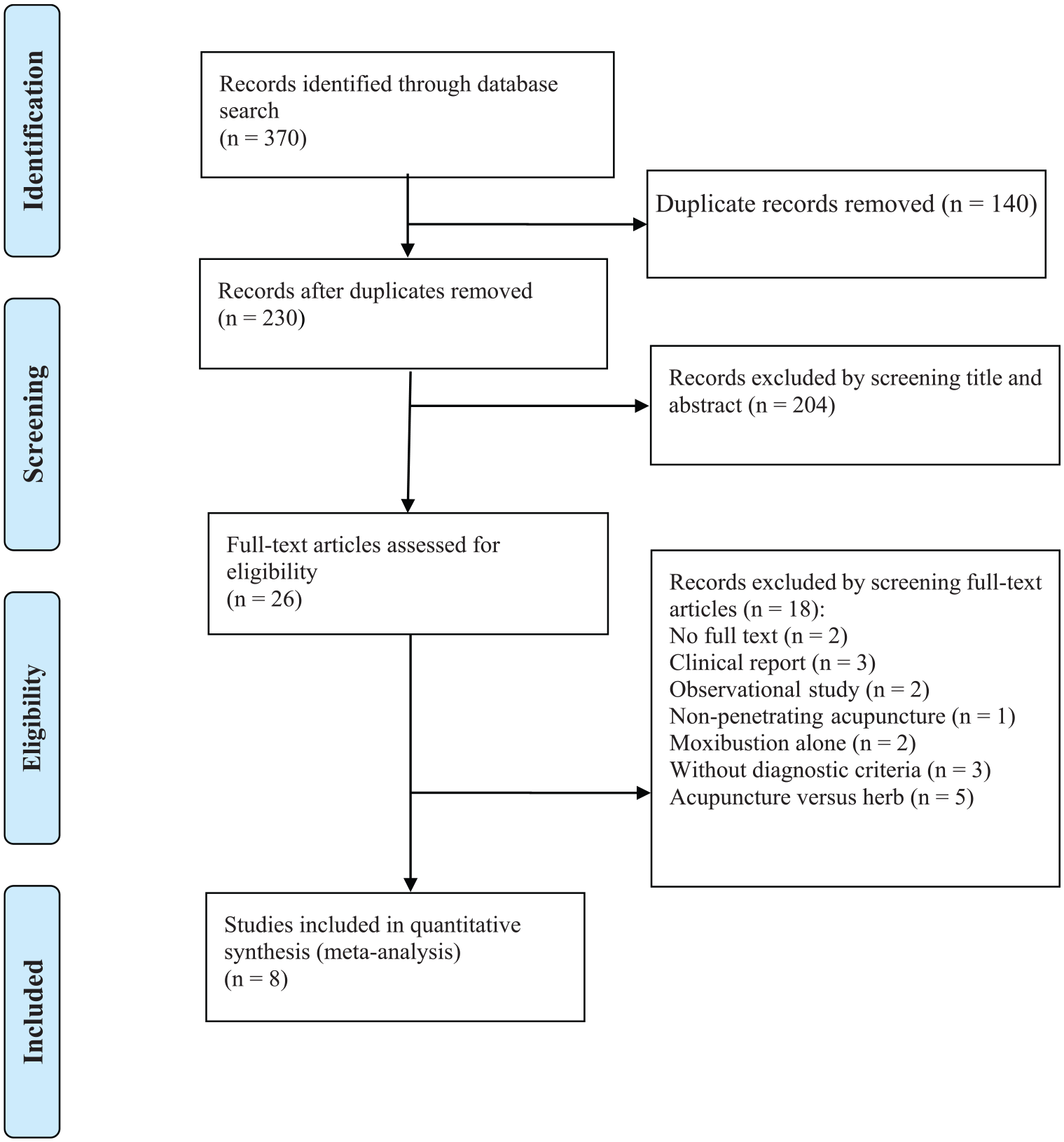
PRISMA flow diagram of study selection process.
Study descriptions
Of the eight included RCTs,8,20–26 seven trials20–26 were published in Chinese and performed in China from 2011 to 2018, and one 8 was published in English and performed in Germany in 2011. In total, four RCTs20–23 were masters theses and four RCTs8,24–26 were published in peer-reviewed journals. The characteristics of the included trials are shown in Table 2.
The characteristics of the included trials.
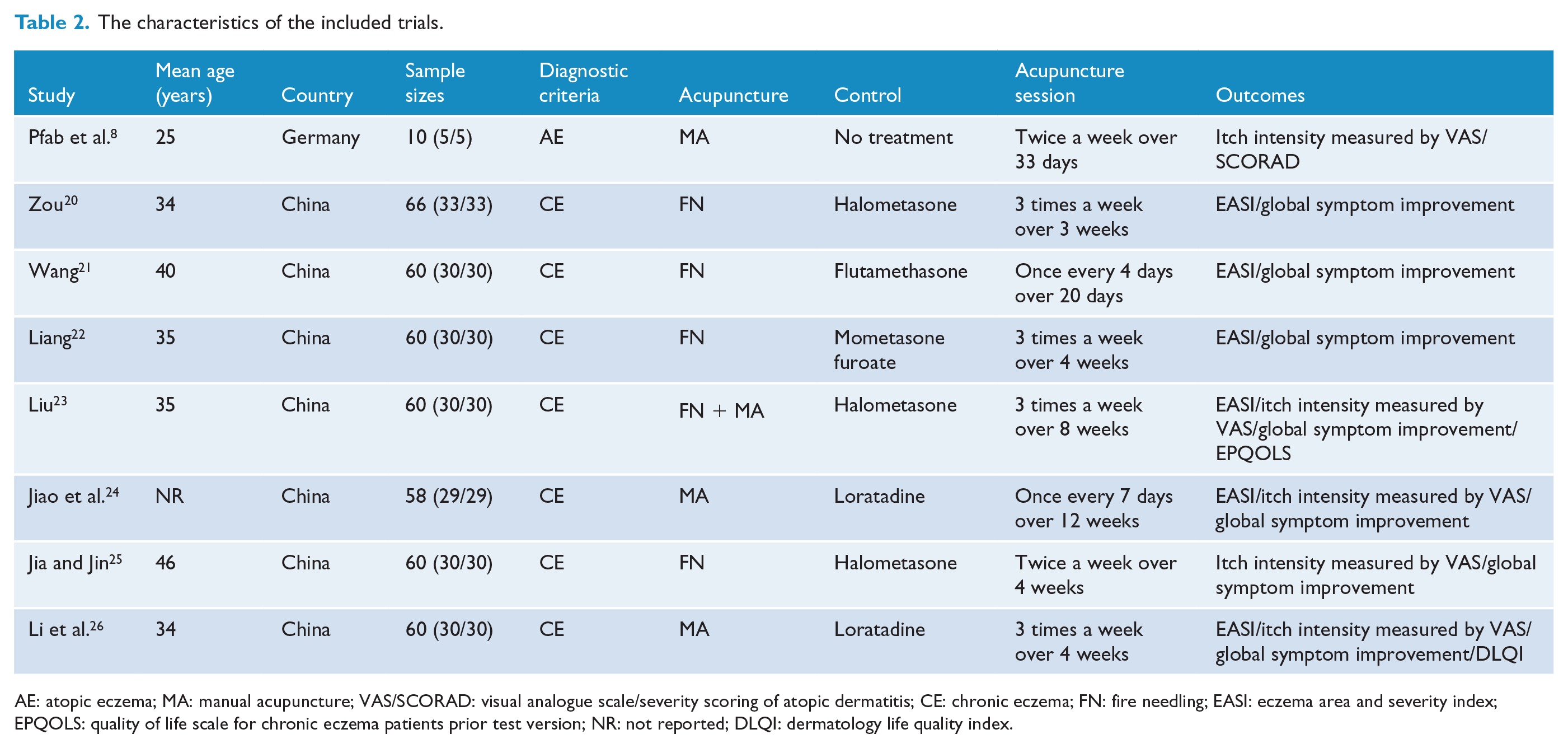
AE: atopic eczema; MA: manual acupuncture; VAS/SCORAD: visual analogue scale/severity scoring of atopic dermatitis; CE: chronic eczema; FN: fire needling; EASI: eczema area and severity index; EPQOLS: quality of life scale for chronic eczema patients prior test version; NR: not reported; DLQI: dermatology life quality index.
Study participants
A total of 434 participants were included in the eight RCTs. All participants were diagnosed with CE20–26 or AE. 8 The age of the participants ranged from 18 to 70 years and the course of AE ranged from 6 months to 35 years.
Study interventions
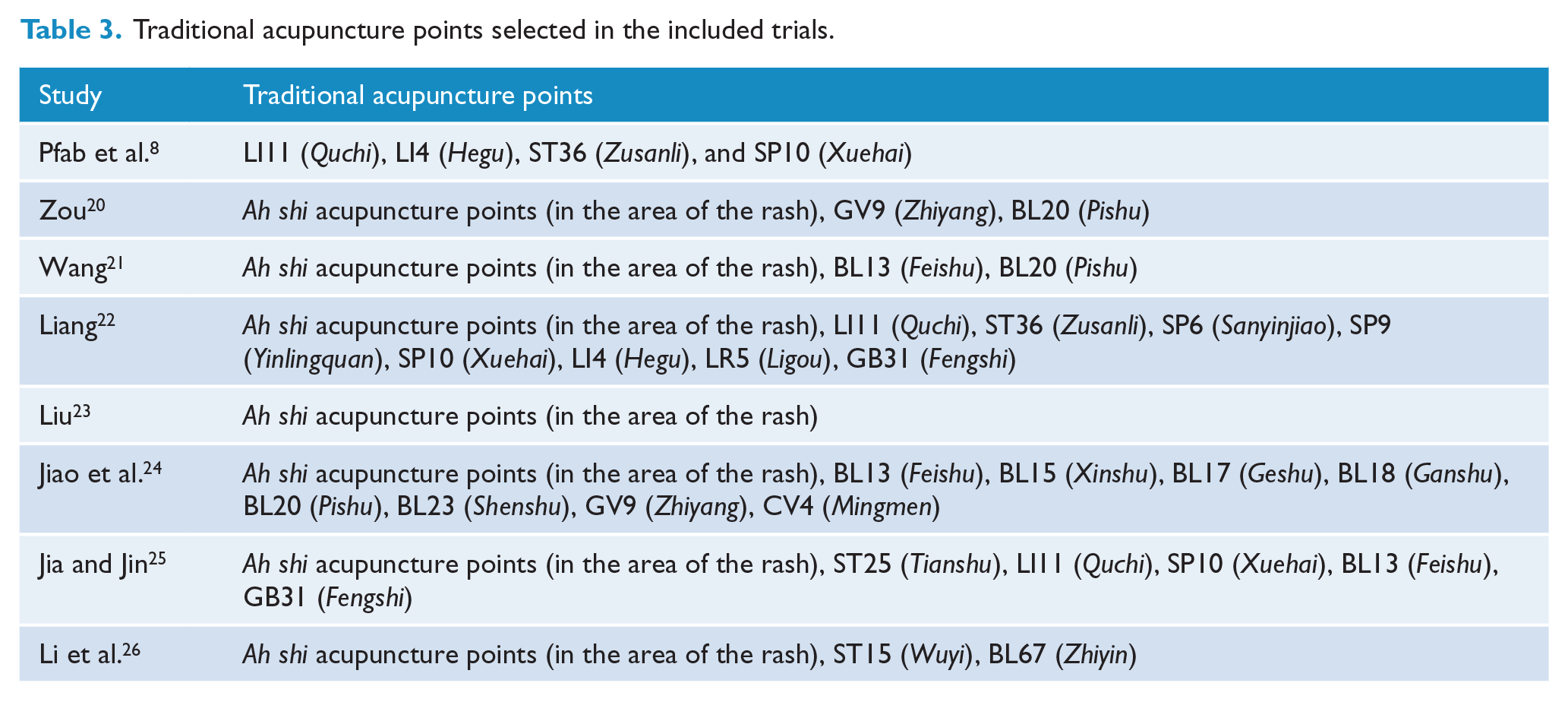
Fire needling was applied in seven RCTs20–26 and manual acupuncture was used in one RCT. 8 Acupuncture at ah shi points was most frequently used in the included RCTs (7/8 in the area of the rash, 87.5%). The second most frequently utilized traditional acupuncture points were BL13 (Feishu, 3/8, 37.5%) and BL20 (Pishu, 3/8, 37.5%). The traditional acupuncture points at which acupuncture was administered in the included trials are shown in Table 3. Seven trials20–26 used conventional medicine as the intervention in the control group and one trial 8 used no treatment in the control group. Conventional medical treatments included halometasone, flutamethasone, momestasone, and loratadine.
Traditional acupuncture points selected in the included trials.
Outcome measures
For the primary outcomes, three RCTs23,24,26 reported EASI and itch intensity measured by VAS, three RCTs20–22 only reported EASI, one RCT 8 reported SCORAD and itch intensity measured by VAS, and one RCT 25 only reported itch intensity measured by VAS. For secondary outcomes, seven RCTs20–26 reported global symptom improvement based on the EASI. Three trials defined recovery as at least 70% improvement, and four trials defined recovery as at least 60% improvement. We used 60% improvement to define recovery as a positive category and the remaining data were used as a negative category; hence, the global symptom improvement data were dichotomous. One RCT 23 reported quality of life using a Chinese self-made questionnaire (the quality of life scale for chronic eczema patients—prior test version, EPQOLS), and one RCT 26 reported quality of life by measuring the dermatology life quality index (DLQI).
Risk of bias
The risk of bias assessment by domain is presented in Figure 2. Seven included RCTs reported adequate methods of random sequence generation, randomization tables were used in six RCTs20–26 and computer-generated randomization was used in one trial. 8 Four RCTs8,21–23 used opaque envelopes to conceal the allocation schedule while the other included trials were considered to have an unclear risk of bias due to the lack of any described method of allocation concealment. Seven RCTs20–26 were deemed to be at high risk of performance bias. Only the RCT by Pfab et al. 8 mentioned that the acupuncturist and the outcome assessor were two different individuals, while seven trials neither described blinding of the participants nor the outcome assessors. Thus, we rated the RCT by Pfab et al. 8 as having a low risk of detection bias. Meanwhile, three RCTs20,21,24 reported patient drop-outs in a reasonable range, and we therefore considered these trials to be at low risk of attrition bias. All included RCTs8,20–26 reported all expected outcomes, but four RCTs20–23 were master theses and hence at high risk of bias for other sources of bias.
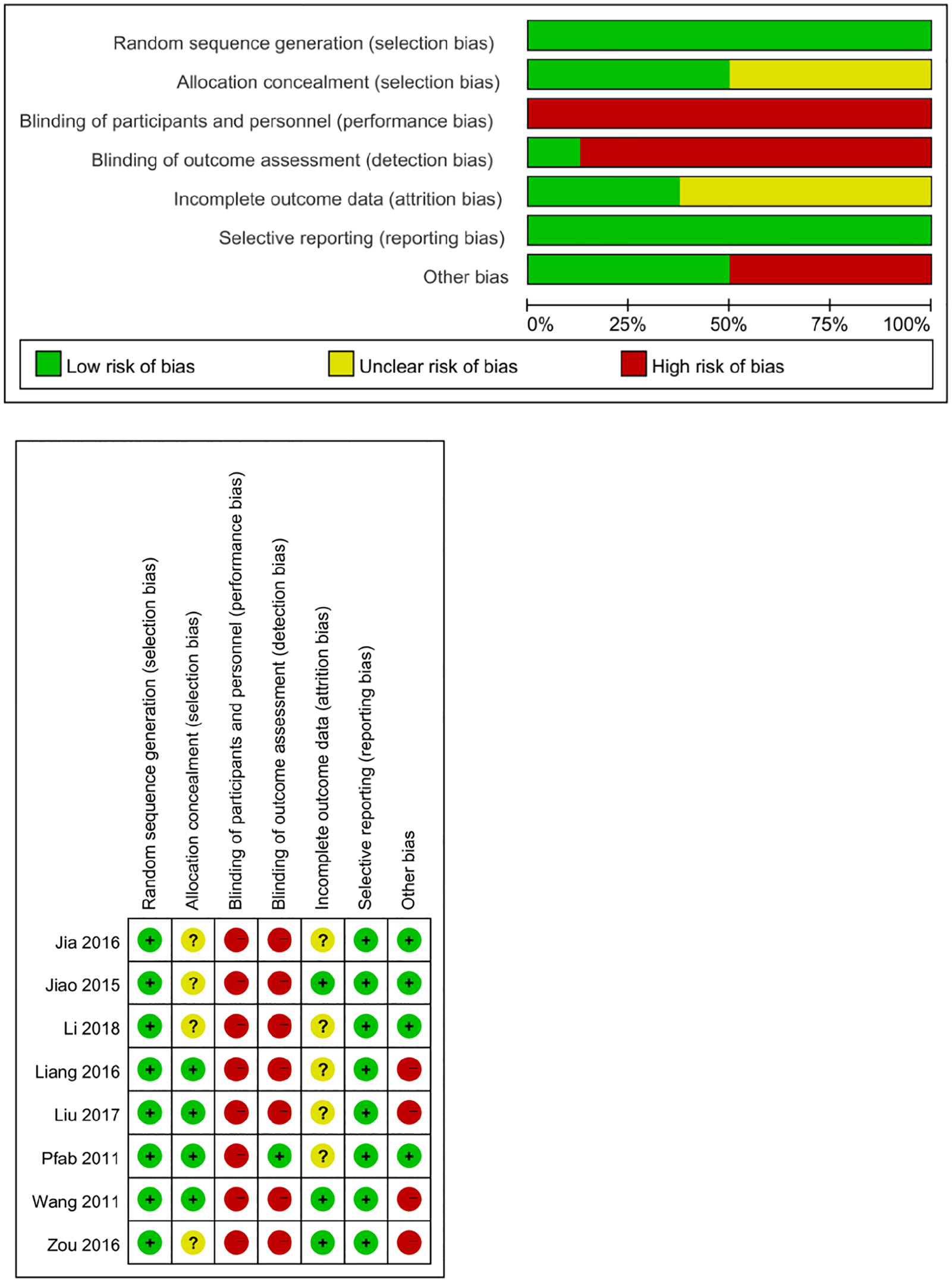
Risk of bias assessed using the Cochrane risk of bias tool.
Effects of acupuncture
Trials were classified into one of four types based on different comparison groups: (1) acupuncture versus sham/placebo acupuncture, (2) acupuncture versus no treatment, (3) acupuncture versus conventional medicine (positive control), and (4) acupuncture combined with conventional medicine versus conventional medicine alone.
Acupuncture versus sham/placebo acupuncture
None of the included trials reported acupuncture versus sham/placebo acupuncture.
Acupuncture versus no treatment
Only one trial 8 involving 10 participants reported on acupuncture versus no treatment for AE.
SCORAD
This trial demonstrated that there was no significant difference between the acupuncture and untreated groups in the reduction of SCORAD score (−5.6 ± 17.6 vs 3.5 ± 3.4, p > 0.05). GRADE analysis reported that the level of this evidence was low because of a high risk of bias and imprecision due to the small sample size (Table 4).
Level of evidence (GRADE).
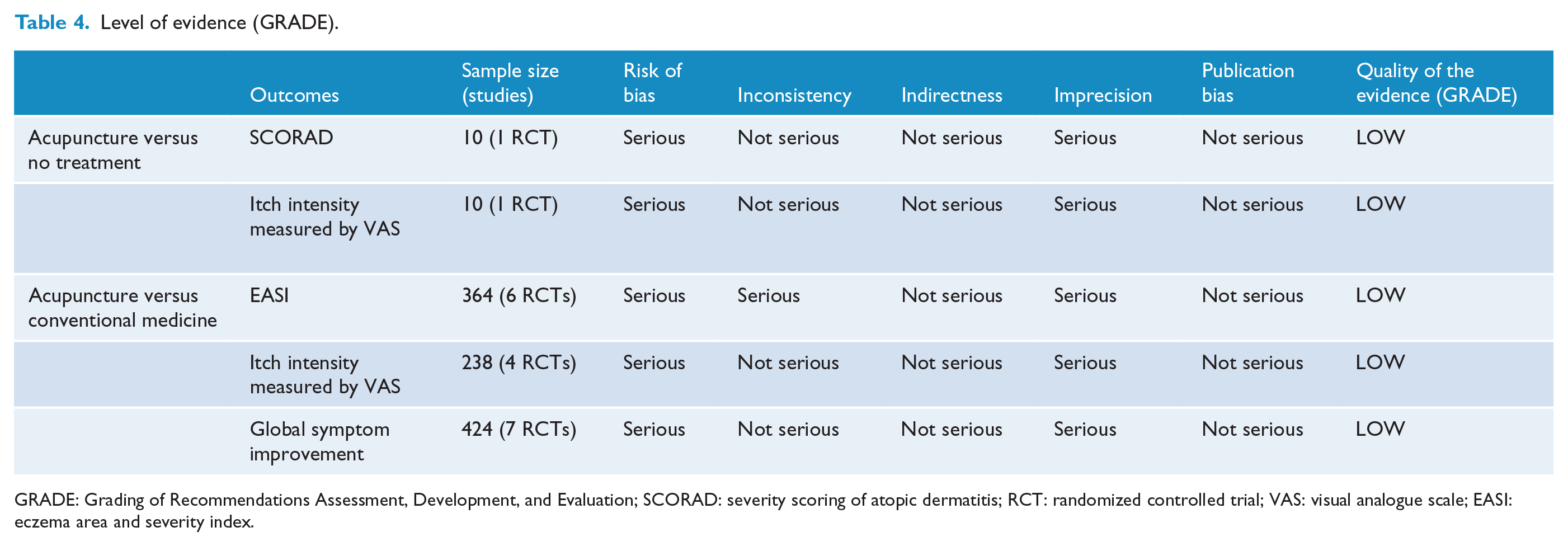
GRADE: Grading of Recommendations Assessment, Development, and Evaluation; SCORAD: severity scoring of atopic dermatitis; RCT: randomized controlled trial; VAS: visual analogue scale; EASI: eczema area and severity index.
Itch intensity measured by VAS
Acupuncture was effective compared with no treatment at reducing itch intensity measured by VAS (−2.4 ± 3.1 vs 2.9 ± 0.9, p < 0.05). GRADE analysis reported that the level of this evidence was low because of a high risk of bias and imprecision due to the small sample size (Table 4).
Acupuncture versus conventional medicine
EASI
The meta-analysis of six RCTs,20–24,26 involving 364 participants, demonstrated a significant difference between medication and acupuncture in the reduction of EASI with high heterogeneity (MD: −1.89, 95% CI −3.04 to −0.75, I2: 78%, Figure 3(a)). The trials performed by Liu, 23 Jiao et al., 24 and Li et al. 26 were considered to be the source of heterogeneity as determined by sensitivity analysis. The heterogeneity disappeared (I2: 0%) after eliminating these three trials from the data combination. Meta-analysis of the three remaining RCTs20–22 (involving 186 participants) demonstrated a significant difference between acupuncture and conventional medicine in the reduction of EASI with no heterogeneity (MD −2.82, 95% CI −3.92 to −1.72, I2 0%, Figure 3(b)). The trial by Liu adopted a special form of acupuncture manipulation called “Ban Ci,” while the other trials did not adopt any form of acupuncture manipulation. The trials by Jiao et al. and Li et al. adopted antihistamine medication (loratadine) in the control group, while the other trials adopted topical corticosteroids such as halometasone, flutamethasone, or momestasone. Use of the antihistamine and the special acupuncture manipulation contributed to the heterogeneity in this analysis. GRADE analysis reported that the level of evidence was low because of a high risk of bias, imprecision of data analysis, small sample size, and inconsistency of unclear heterogeneity (Table 4).
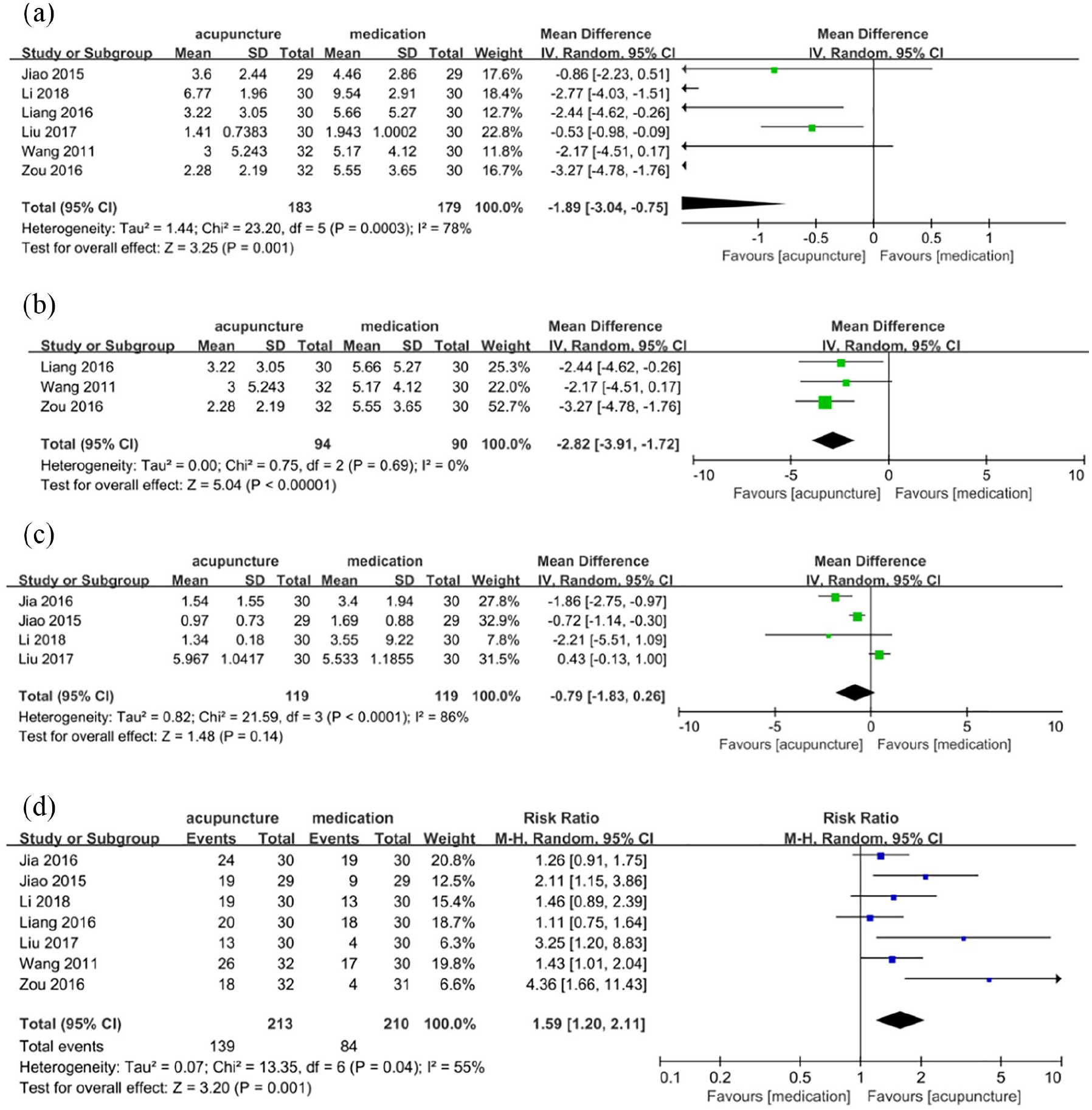
Forest plots of comparison of acupuncture versus medication for: (a and b) eczema area and severity index (EASI), (c) itch intensity measured by visual analogue scale (VAS), and (d) global symptom improvement.
Itch intensity measured by VAS
Meta-analysis of four RCTs23–26 involving 238 participants demonstrated that there was no significant difference between the acupuncture and conventional medicine groups in the reduction of itch intensity measured by VAS (MD −0.79, 95% CI −1.83 to 0.26, I2 86%, Figure 3(c)). GRADE analysis reported that the level of evidence was low because of a high risk of bias, imprecision of data analysis, and small sample size (Table 4).
Global symptom improvement
Meta-analysis of seven RCTs20–26 involving 424 participants demonstrated that there was a significant difference between the acupuncture and conventional medicine groups in global symptom improvement (RR: 1.59, 95% CI: 1.20–2.11, I2: 55%, Figure 3(d)). GRADE analysis reported that the level of evidence was low because of a high risk of bias, imprecision of data analysis, and small sample size (Table 4).
Quality of life
Two RCTs23,26 reported on quality of life measured by EPQOLS or DLQI. One trial 23 involving 60 participants reported that there was a statistically significant difference in EPQOLS scores between the acupuncture and conventional medicine groups (19.5 ± 4.81 vs 18.7 ± 6.22, p < 0.05). The remaining trial 26 involving 60 participants also reported a statistically significant difference in DLQI score between the acupuncture and conventional medicine groups (2.0 ± 0.15 vs 4.6 ± 0.29, p < 0.05).
Acupuncture combined with conventional medicine versus conventional medicine alone
None of included trials reported on acupuncture combined with conventional medicine versus the same conventional medicine (as an adjunct).
Safety (adverse events)
After screening all RCTs utilizing acupuncture for AE among 325 articles, 18 RCTs (1196 participants) were included in the safety assessment. Ten RCTs reported no adverse events and eight23,28–34 reported minor adverse events in the acupuncture treatment group or the acupuncture combined with other treatment group. There were no severe adverse effects in the 18 included RCTs. One RCT 23 reported four cases of worsened itching after acupuncture. One RCT 28 reported two cases of local hemorrhage in the skin after acupuncture. One RCT 29 reported two cases of local skin erythema and swelling after acupuncture. One RCT 30 reported three cases of localized spiloplaxia of the skin after acupuncture. One RCT 31 reported that two patients felt faint during acupuncture. One RCT 32 reported three cases of slightly red and swollen skin following treatment, and two RCTs33,34 reported eight cases of local chromatosis of the skin after treatment. None of the remaining trials reported any adverse events related to acupuncture.
Discussion
The aim of this systematic review and meta-analysis was to evaluate the effectiveness and safety of acupuncture treatment for AE. Our meta-analysis included eight RCTs that allowed us to compare acupuncture with no treatment or conventional medicine.
For primary outcomes, eight trials were included in this review. Only one trial 8 compared acupuncture with no treatment. This trial reported a significant difference in the reduction of itch intensity measured by VAS but not in the reduction of the SCORAD score. Since this trial was a pilot, with only 10 participants, the results were not considered to be reliable.
Seven RCTs20–26 compared acupuncture versus conventional medicine. Three RCTs20,23,25 used halometasone, one trial 22 used mometasone furoate, one trial 21 used flumethasone, and two trials24,26 used loratadine. Halometasone, mometasone furoate, and flumethasone are topical corticosteroids, while loratadine is an antihistamine. Our meta-analysis found that acupuncture was more effective than these conventional medical treatments at reducing the EASI when taking into account six RCTs,20–24,26 but only three of these RCTs20–22 were finally included in our meta-analysis. However, the results still suggested that acupuncture is more effective than conventional medicine at reducing the EASI given that there was no heterogeneity among these three RCTs (I2: 0%). We note that the lack of blinding of participants, acupuncturists, and statisticians may have biased the results; thus, the level of evidence may be limited in our study. In addition, four RCTs20–23 were masters theses, which are not peer-reviewed studies. Therefore, we need to confirm our results in further trials.
Among the trials comparing acupuncture with conventional medicine, our meta-analysis indicated that there was no significant difference in the reduction of itch intensity as measured by VAS in four RCTs.23–26 However, since these four RCTs were designed to detect the difference between acupuncture and conventional medicine, we could not conclude that acupuncture is superior to conventional medicine. Further trials and high-quality evidence are required to explore the effect of acupuncture on AE.
For secondary outcomes, global symptom improvement was evaluated in seven RCTs.20–26 The results of these seven RCTs showed that acupuncture is more effective than conventional medicine at improving global symptom scores in AE. However, we reclassified at least 60% improvement into a positive category regarding recovery and the other data into a negative category, which might have accounted for the difference between our results and those of the original six included RCTs. Thus, it is difficult to evaluate the effect of acupuncture because the cut-off points for global symptom improvement in the seven RCTs were different and self-defined. Two included trials23,26 demonstrated that acupuncture is better than conventional medicine at improving quality of life. However, one of these trials 23 utilized a Chinese self-made questionnaire without testing its validity and reliability to efficiently evaluate the quality of life of patients with AE. Thus, more robust trials with an authoritative scale of quality of life are needed to further support our conclusion. The included trials did not report the recurrence rate of AE, so there is insufficient evidence to show the effectiveness of acupuncture at reducing the recurrence rate of AE. However, since AE recurrence rates are high, it is necessary to perform a follow-up analysis of the recurrence rate in future trials.
Given the low level of evidence evaluated using the GRADE approach in this meta-analysis, there was common bias among the eight included trials. First, these included RCTs did not include blinded acupuncturists or participants, therefore poor methodological quality of these included trials (with a high risk of performance bias) resulted in relatively low levels of evidence. Furthermore, these trials did not appear to be have been registered in a clinical trial registry, nor did they report the details of their sample size calculation. Third, the expected effects of acupuncture are critical when comparing acupuncture with no treatment or conventional medicine. None of the included RCTs reported these preferences, or expectations regarding acupuncture compared to conventional treatments. Thus, we cannot confirm the specific efficacy of acupuncture for AE, and the effects of acupuncture may have been exaggerated in these trials. These common biases can hinder the ability to determine the real effect of acupuncture.
We conducted a descriptive analysis based on the adverse events observed in eight RCTs related to acupuncture treatment of AE. Eighteen RCTs were included in the safety assessment after screening all 325 RCTs. Ten studies reported no adverse events and eight studies23,28–34 reported minor adverse events after treatment. Thus, we would tentatively conclude that acupuncture is a safe treatment for patients with AE.
There were three similar systematic reviews published in English or Chinese from 2014 to 2016.9–11 Two reviews9,11 published in 2014 and 2015 included trials that compared acupuncture with acupuncture combined with Chinese herbal medicine or the inclusion of other forms of acupuncture (such as acupressure or warm needle acupuncture), so the actual effectiveness of penetrating acupuncture alone was not explored in these reviews. Moreover, Tan et al. 10 published a review in 2016 but did not provide any evidence-based conclusion after finding no eligible RCTs to include. In our systematic review, first, most included RCTs were published from 2016 to 2018. Then, we included the EASI, itch intensity measured by VAS, and quality of life of AE patients as outcome measures. Third, we paid attention to traditional penetrating acupuncture and generated more rigorous inclusion criteria to evaluate the effects and safety of acupuncture on AE.
There are several limitations to this meta-analysis. First, the low quality of the included trials may have biased the analysis, and so more high-quality trials should be conducted and reported according to the Consolidated Standards of Reporting Trials (CONSORT) statement 35 and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines. 36 Meanwhile, since only eight trials were included in this study, subgroup analysis was not performed. Second, most included trials were published in Chinese, so the results might not be generally applicable. Third, this analysis only included two comparison groups and the specific effects of acupuncture could not be evaluated. Future studies should include sham/placebo acupuncture groups.
Conclusion
In conclusion, acupuncture might be an effective treatment capable of reducing itch intensity, and may be more effective than conventional medicine at reducing EASI and improving global symptoms for patients with AE. Acupuncture is a safe treatment for patients with AE, but the available data are too few to suggest that acupuncture alone is effective at improving quality of life and recurrence rate. More high-quality trials with larger sample sizes are needed to confirm the effects of acupuncture on AE.
Footnotes
Contributions
R.J., Z.L., and Y.W. contributed to the conception and design of this study and revision of the article. R.J. drafted the article. R.J. and Y.Z. contributed to the literature search. J.Z. and Z.Y. contributed to screening of the studies, extraction of the data, and the risk of bias assessment. Z.Y. and R.J. contributed to statistical analysis. All authors read and approved the final version of the article accepted for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Not required.
Provenance and peer review
Not commissioned, externally peer reviewed.