
Abstract
Objectives:
To test whether a newly developed person-, theory- and evidence-based website about acupuncture helps patients make informed decisions about whether or not to use acupuncture for back pain.
Methods:
A randomised online study compared a newly developed ‘enhanced website’ to a ‘standard website’. The enhanced website provided evidence-based information in a person-based manner and targeted psychological constructs. The standard website was based on a widely used patient information leaflet. In total, 350 adults with recent self-reported back pain were recruited from general practices in South West England. The two primary outcomes were knowledge change and making an informed choice about using acupuncture. Secondary outcomes were beliefs about and willingness to have acupuncture.
Results:
Participants who viewed the enhanced acupuncture website had a significantly greater increase in knowledge about acupuncture (M = 1.1, standard deviation (SD) = 1.7) than participants who viewed the standard website (M = 0.2, SD = 1.1; F(1, 315) = 37.93, p < 0.001, η2 = .107). Participants who viewed the enhanced acupuncture website were also 3.3 times more likely to make an informed choice about using acupuncture than those who viewed the standard website (χ2(1) = 23.46, p < 0.001). There were no significant effects on treatment beliefs or willingness to have acupuncture.
Conclusion:
The enhanced website improved patients’ knowledge and ability to make an informed choice about acupuncture, but did not optimise treatment beliefs or change willingness to have acupuncture. The enhanced website could be used to support informed decision-making among primary care patients and members of the general public considering using acupuncture for back pain.
Introduction
In the United Kingdom alone, approximately 4 million acupuncture treatments are provided annually by over 10,000 registered acupuncturists practicing a range of acupuncture styles. 1 Back pain is highly prevalent and burdensome for patients and societies,2,3 the beneficial effects of acupuncture for back pain have been established, 4 and patients commonly seek acupuncture for back pain.1,5 While the balance of evidence suggests acupuncture is more beneficial than usual care, it may not be superior to placebo or sham acupuncture. 6 This leads to differing interpretations of the evidence base by policy-makers and in clinical guidelines.6–9 For example, the UK National Institute for Health and Care Excellence recently switched from recommending to not recommending acupuncture for back pain,6,9 but their interpretation of the evidence has been criticised for prioritising problematic comparisons with sham acupuncture (which probably has active components) over more clinically meaningful comparisons with usual care. 10 This situation can be confusing for patients and suggests a need for educational resources to support patients making informed choices about acupuncture.
When considering trying acupuncture, consumers seek information from their social networks, print and online media.11,12 One study found that many (but not all) of 401 acupuncture patient information leaflets sourced from UK clinical settings successfully provided ethically sound information consistent with the scientific evidence base. 13 There is also scope to improve information provided to patients in acupuncture trials. 14 In contrast to leaflets, which provide limited information and can only provide text and static images, websites can incorporate additional interactive and other features (e.g. quizzes, audio and film) 15 that can: enhance engagement and effective education; 16 provide more extensive information to those who are interested without overwhelming others; and be easily and cheaply disseminated for widespread access. 15 Online health information is increasingly important to consumers,17,18 but websites about complementary therapies can be unreliable.19,20 Indeed, there is evidence of knowledge gaps, misconceptions and concerns about acupuncture among acupuncture patients, 11 trial participants, 21 healthcare providers 22 and the wider community.23–25 For example, approximately 50% of community-dwelling adults with a history of back pain surveyed did not know that acupuncture is not statutorily regulated in the United Kingdom. 23 Lack of knowledge might deter use 26 and is important to address. Therefore, people considering acupuncture might benefit from a reliable online source of accurate, evidence-based information to support their decision-making.
In addition to supporting decision-making, information about acupuncture might also change patients’ beliefs about acupuncture and, in doing so, could impact clinical outcomes. Evidence suggests that patients who have more positive expectations of benefitting from acupuncture may subsequently experience better clinical outcomes, including pain relief and functioning,27,28 while presenting information in a very neutral frame might be detrimental. 29 Encouraging patients to have positive expectations of acupuncture’s effectiveness might thus enhance clinical outcomes, but is challenging to implement because it would be unethical and potentially harmful to foster unrealistically positive expectations.
Two standardised patient information leaflets on acupuncture are in use 30,31 and educational programmes for medical students have been described. A few formal evaluations of these educational programmes have been published including, for example, some using digital resources. 32 However, we could not locate any published studies testing interventions to improve patients’ knowledge and/or informed choices about acupuncture.
We designed a new website to provide scientifically accurate evidence-based information about acupuncture, aiming to increase knowledge, support informed decision-making and encourage realistically positive outcome expectancies among people who might be considering using acupuncture. The objectives were to determine whether, compared to a control website, the new website could: (1) increase knowledge; (2) improve informed choice; and (3) change beliefs about acupuncture in adults with recent back pain.
Methods
Interventions
Two websites about acupuncture were developed: an enhanced website and a standard website. The enhanced website and its development, using a person-, evidence- and theory-based approach, have been described elsewhere. 33 In brief, the website comprises 11 main pages and addresses key topics of interest to potential acupuncture patients, including beneficial and adverse effects, mechanisms of action, safety, practicalities and patients’ experiences. Figure 1 shows an example page. The website conveys information through text, written evidence summaries, audio-clips of four patients’ stories and two acupuncturists’ descriptions of their practice, and three short films. The content was based on published scientific evidence, focused on support for acupuncture providing clinically meaningful pain relief for some patients with back pain. This is consistent with the balance of the evidence, including an individual patient data meta-analysis 4 and a pragmatic view that, as acupuncture is demonstrably superior to conventional treatments, 6 patients should be told about its potential benefits.
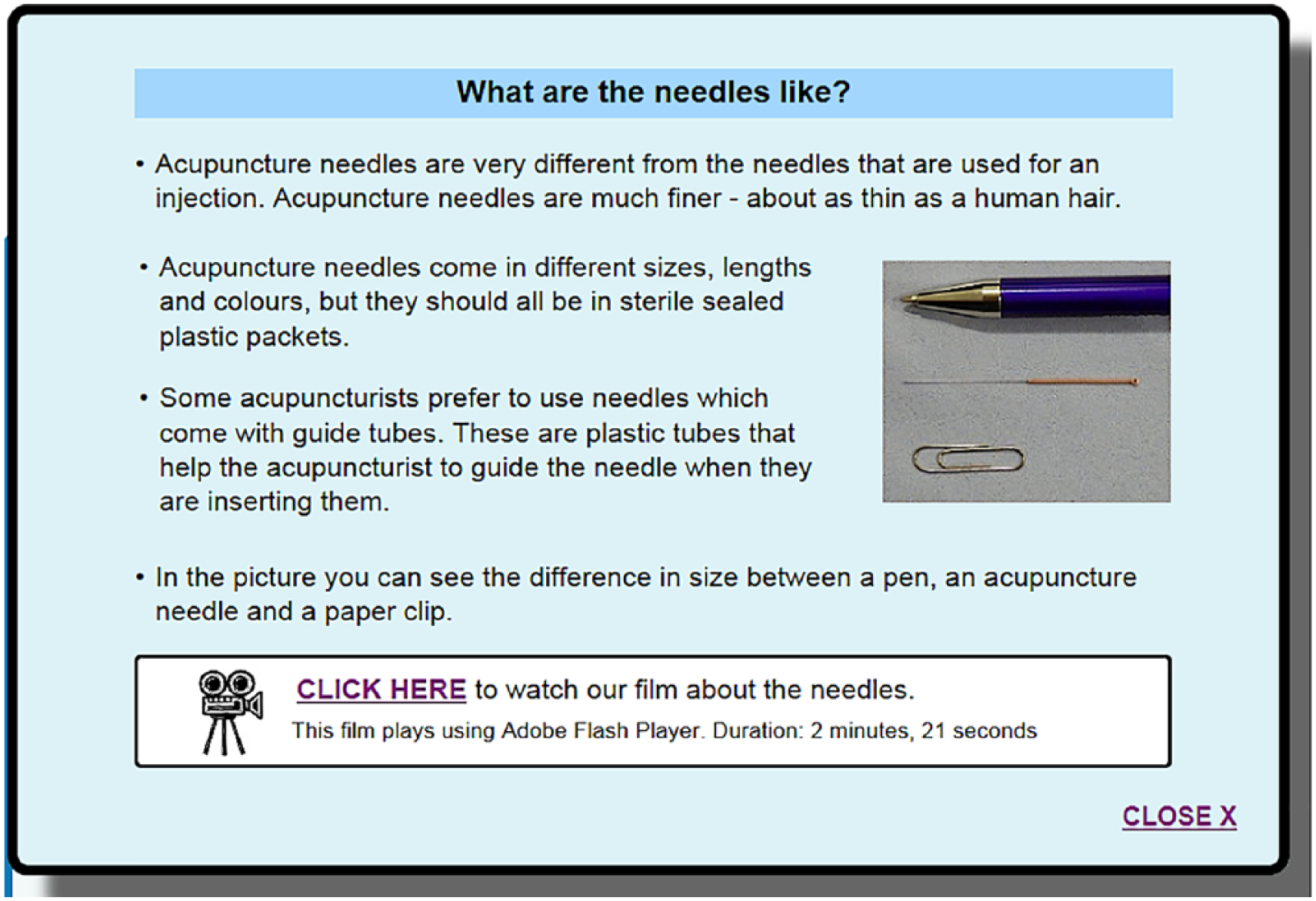
Example screenshot from enhanced website.
The ‘standard’ website was based on an information sheet and consent form designed by consensus among leading UK acupuncturists 30 and commonly used in UK clinical practice. 13 The standard website gives brief information (two pages) about acupuncture, its safety, possible side-effects and contraindications. Supplementary Material 1 compares the two websites.
Design
An online study was conducted with a mixed factorial two-by-two design, intended to test two new websites, one about acupuncture (the focus of this paper) and one about placebo. 34 The two factors were topic (acupuncture website vs placebo website) and website (‘enhanced’ vs ‘standard’ website). Each ‘enhanced’ website was compared to a ‘standard’ website on the same topic. Participants were randomised automatically by study website to one of the four groups, representing every combination of the two factors; each participant thus viewed one website (enhanced or standard) about acupuncture and one website (enhanced or standard) about placebo; the order of which was counterbalanced within groups. There were no interaction effects between the acupuncture and placebo websites and no effects of placebo website on acupuncture-related outcomes, that is, whether the participants viewed the standard or enhanced version of the placebo website had no effect on the acupuncture outcome measures. Therefore, here, we report the enhanced versus standard comparison for the acupuncture website only, collapsing across the placebo website conditions.
Measures
Participant characteristics
Clinical characteristics were assessed using items from the recommended minimum data set for back pain. 35 Single items assessed pain duration, frequency, intensity, catastrophising, spread to legs and pain-related legal claims, disability benefits or compensation. Four-item scales assessed pain functioning and interference with excellent internal consistency (Cronbach’s alphas in this sample are 0.96 and 0.92, respectively). Single items measured ethnicity, age, gender and education.
Primary outcomes
Primary outcomes were knowledge and informed choice about acupuncture. Knowledge was assessed using a 10-item quiz, comprising true–false questions selected from a larger pool of 15 items pilot-tested in a community-based sample of 202 adults with recent back pain. 23 The 10 items most commonly answered incorrectly by the community-based sample were selected (e.g. ‘Acupuncture is never available on the NHS’ – false). The knowledge score is the total number of items answered correctly. The quiz was completed before and after viewing the websites, and a difference-score was calculated.
Making an informed choice has been defined as choosing based on knowledge and consistent with one’s values.36,37 To make an informed choice, one needs an accurate understanding of the options, to consider one’s values and to make a decision consistent with one’s knowledge and values. An informed choice to try acupuncture requires knowledge about its possible beneficial and adverse effects, a positive attitude and a decision to try acupuncture. An informed choice not to try acupuncture requires knowledge about its possible beneficial and adverse effects, a negative attitude and a decision not to try acupuncture.
The knowledge component of informed choice was measured using the knowledge quiz described above. Attitudes were measured using four items derived from theory-based guidelines for assessing attitudes, 38 for example, ‘having acupuncture treatment would be good’. Behavioural intentions were used as a proxy for behaviour and were measured using three items similarly derived, 38 for example, ‘if given the opportunity, I intend to have acupuncture treatment’. Attitudes and intentions were measured on 7-point Likert-type scales labelled strongly agree to strongly disagree; scores across constituent items were summed. The attitude and intention scales had good internal consistency (Cronbach’s alphas are .97 and .84, respectively). Participants were categorised as making an informed choice or not based on their knowledge score (high/low, based on median split), attitude (positive/negative, split by scale midpoint) and intention (high/low, split by scale midpoint). Participants were categorised as making an informed choice if they scored above the median on knowledge and either (1) above the scale midpoint on both attitudes and intentions or (2) below the scale midpoint on both attitudes and intentions. All other score combinations were categorised as not making an informed choice.
Secondary outcomes
Secondary outcomes were beliefs about and willingness to have acupuncture. Four dimensions of belief were measured using the four, four-item, subscales of the low back pain treatment beliefs questionnaire: 39 concerns (e.g. ‘I worry that acupuncture could make my back worse’), individual fit (e.g. ‘I think acupuncture could suit me as a treatment for my back pain’), expectancy (e.g. ‘Acupuncture can work well for people with back pain’) and credibility (e.g. ‘Using acupuncture for back pain makes a lot of sense’). All items had 5-point Likert-type response scales labelled strongly disagree to strongly agree. All subscales had good internal consistency (Cronbach’s alphas for concerns = 0.83, individual fit = 0.91, expectancy = 0.84 and credibility = 0.84).
One item asked whether participants would be ‘willing to have acupuncture treatment’ (yes/no). Supplementary Material 2 presents the outcome measures.
Participants and recruitment
Adults (aged 18 years and over) who had general practitioner (GP)-documented back pain within 3 years were recruited via 26 general practices in South West England. GP staff conducted database searches and mailed study invitation packs (comprising cover letter, information sheet and study website address) to eligible patients. Those with needle phobia or unable to complete questionnaires in English were excluded. Figure 2 shows participant flow.
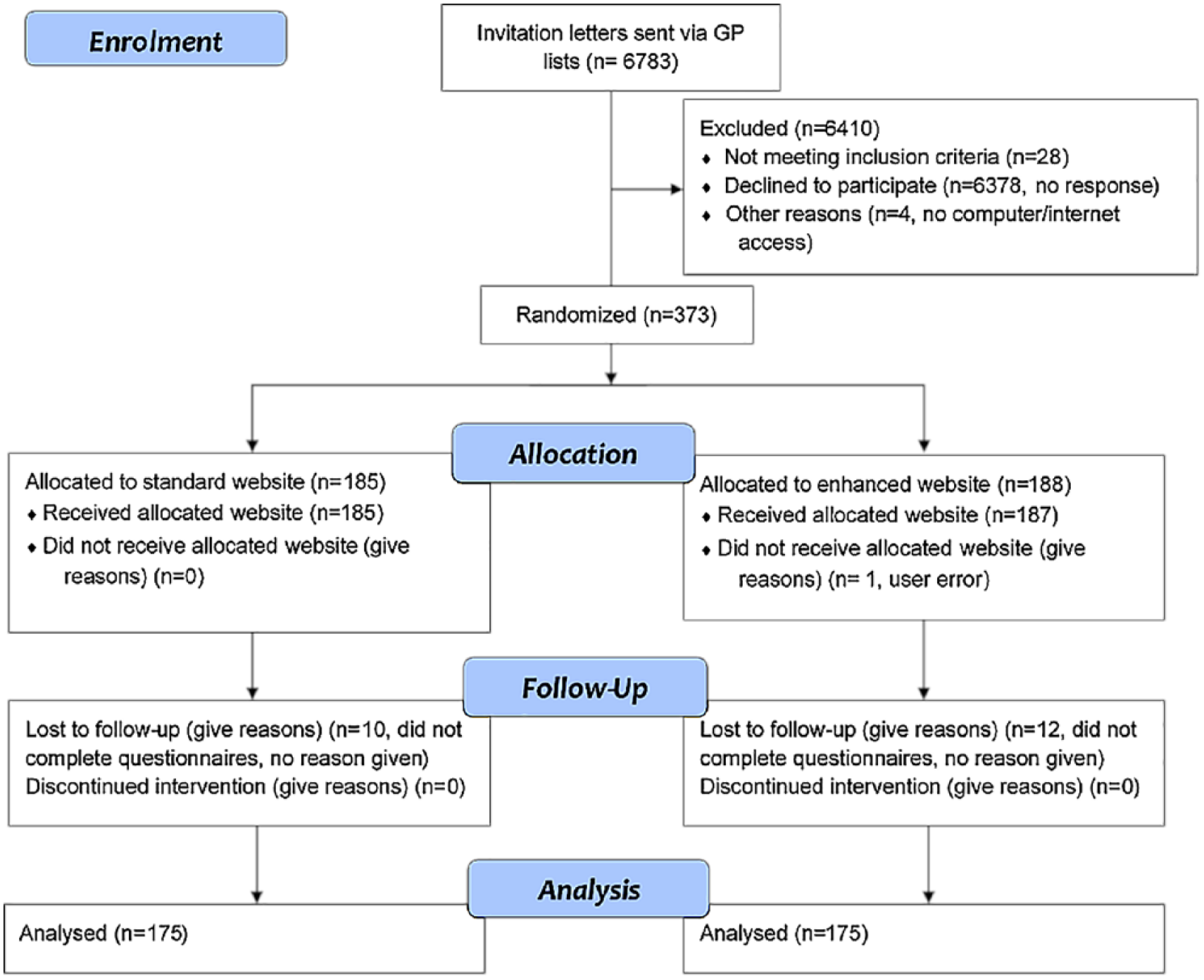
Participant flow diagram.
An a priori power calculation was conducted using G*Power. Assuming an effect size f = 0.15 (based on unpublished pilot data), power 0.8 and alpha 0.05 for a factorial analysis of variance (ANOVA), it was estimated that n = 351 participants would be required; assuming 5% drop-out, we required 369 patients to be randomised.
Procedure
Ethical approval was obtained from the University of Southampton (reference: 12323) and NHS NRES Committee East of England – Hatfield (reference: 14/EE/1176).
After reading the online information sheet, participants gave consent by clicking a button. They were then asked screening questions assessing age, current or recent back pain (within 3 years), and needle phobia. Those not meeting the associated inclusion criteria were directed to an exit page. Eligible individuals entered their email address and created a website password. The acupuncture knowledge quiz then assessed baseline knowledge, after which participants were presented with two websites sequentially according to the randomisation. Participants could take breaks, log out and return to the study later, and stop viewing each website whenever they wanted (‘click here when you have finished looking at the information’ button was on every page). After viewing the websites, participants completed the participant characteristics, primary outcome measures and secondary outcome measures. Finally, participants were directed to a debriefing page with further information and links to other resources; those who completed the study were emailed a £10 online shopping voucher.
Statistical analysis
The proportion of missing data was small (<5% for any one variable), but was not missing completely at random, suggesting imputation might be inappropriate, but unlikely to alter the results. 40 All analyses were repeated excluding missing data and imputing missing values with the expectation–maximization (EM) algorithm. The results were the same; the reported analyses included all available data with no imputation.
Pearson’s χ2 compared the number of people making an informed choice between the two website groups. ANOVAs tested the effects of website on knowledge change, treatment perceptions and willingness to have acupuncture. Models were adjusted for possible confounders (previous acupuncture use and looking up additional information about acupuncture during study breaks). Unadjusted models are reported for the primary outcomes as the covariates were not significant.
Results
Participant characteristics
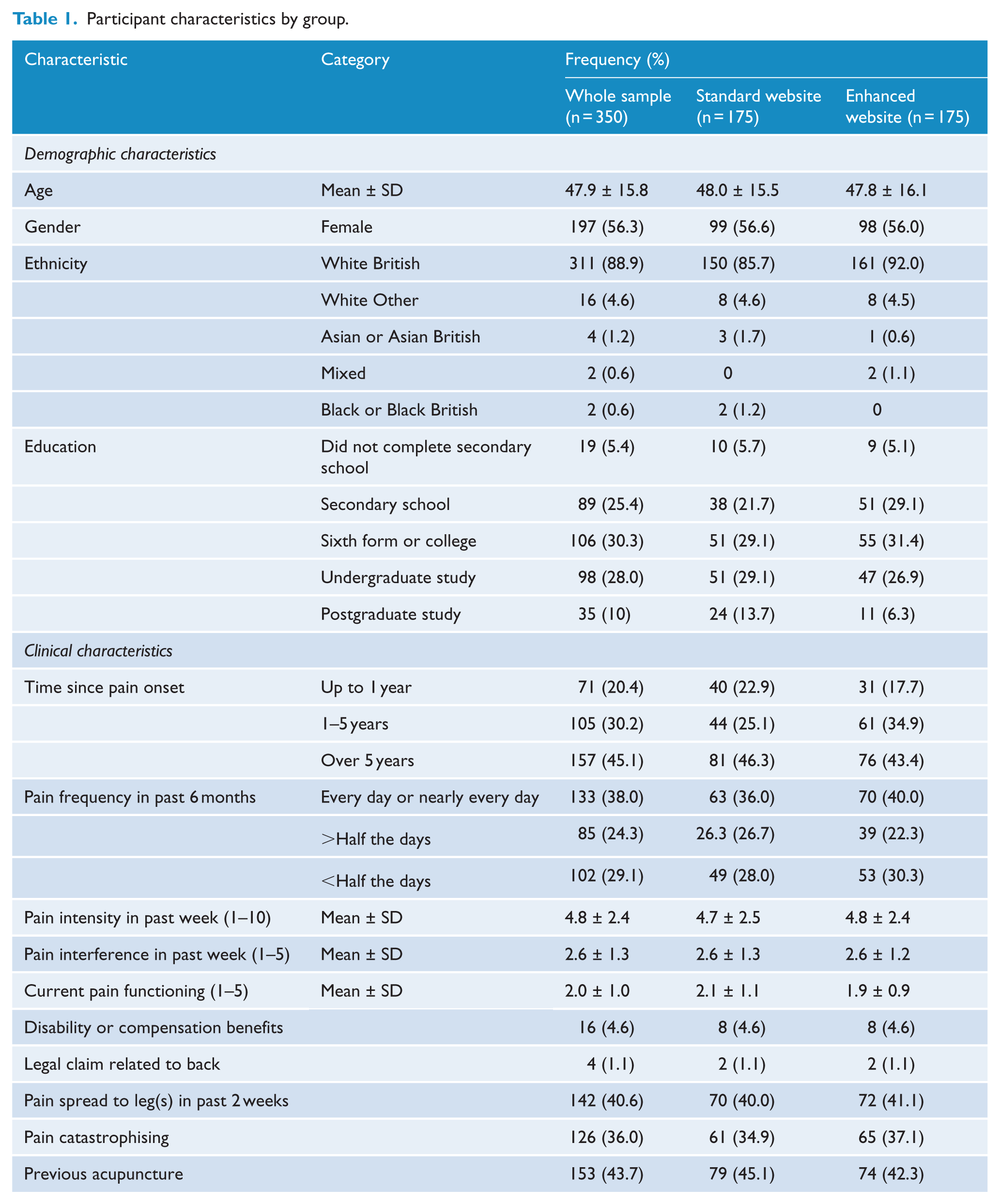
In total, 350 adults took part; a slight majority were female, most were White British and over half had completed college education or higher (see Table 1). Participants typically had long-standing back pain (45% had onset over 5 years ago) that affected them on a daily or near-daily basis (38%) and was of moderate intensity (mean = 4.8 on a 1–10 scale). There were no significant between-group differences in demographic or clinical measures (all ps > 0.05).
Participant characteristics by group.
Primary outcomes: knowledge and informed choice
There was a significant main effect of website on change in acupuncture knowledge, F(1, 315) = 37.93, p < 0.001, η2 = 0.107, explaining 10.7% of the variance in knowledge change. Participants who viewed the enhanced acupuncture website had a significantly greater increase in their knowledge about acupuncture (M = 1.1, standard deviation (SD) = 1.7) than participants who viewed the standard acupuncture website (M = 0.2, SD = 1.1).
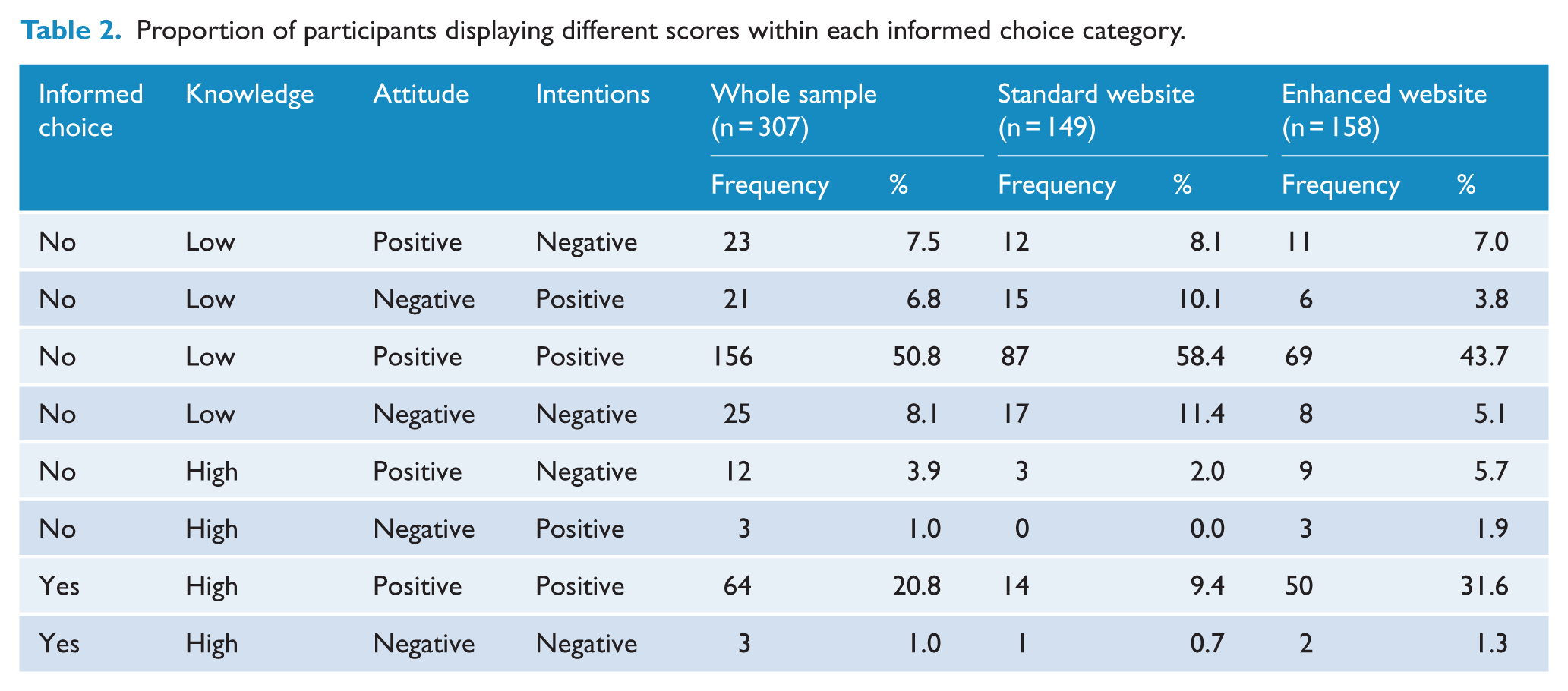
Table 2 shows how participants were classified as making or not making an informed choice according to their knowledge, attitudes and intentions. The most common pattern of scores (50.8% of participants) was to have positive intentions of using acupuncture and positive attitudes towards acupuncture, despite low knowledge. There was a significant association between website and informed choice about acupuncture (χ2(1) = 23.46, p < 0.001), with 32.9% (52/158) of people who viewed the enhanced website making an informed choice about acupuncture compared to 10.1% (15/149) of people who viewed the standard website. Thus, participants who viewed the enhanced website were 3.3 times more likely than those who viewed the standard website to make an informed choice about acupuncture.
Proportion of participants displaying different scores within each informed choice category.
Secondary outcomes: treatment beliefs
Table 3 shows mean scores on treatment beliefs by website. There was a small non-significant trend for people who viewed the enhanced website to have more positive expectations of benefit from acupuncture and to rate it as more credible compared to people who viewed the standard website. There were no effects of website on concerns about acupuncture or perceptions that acupuncture offered a good fit for the individual.
Treatment beliefs by group.
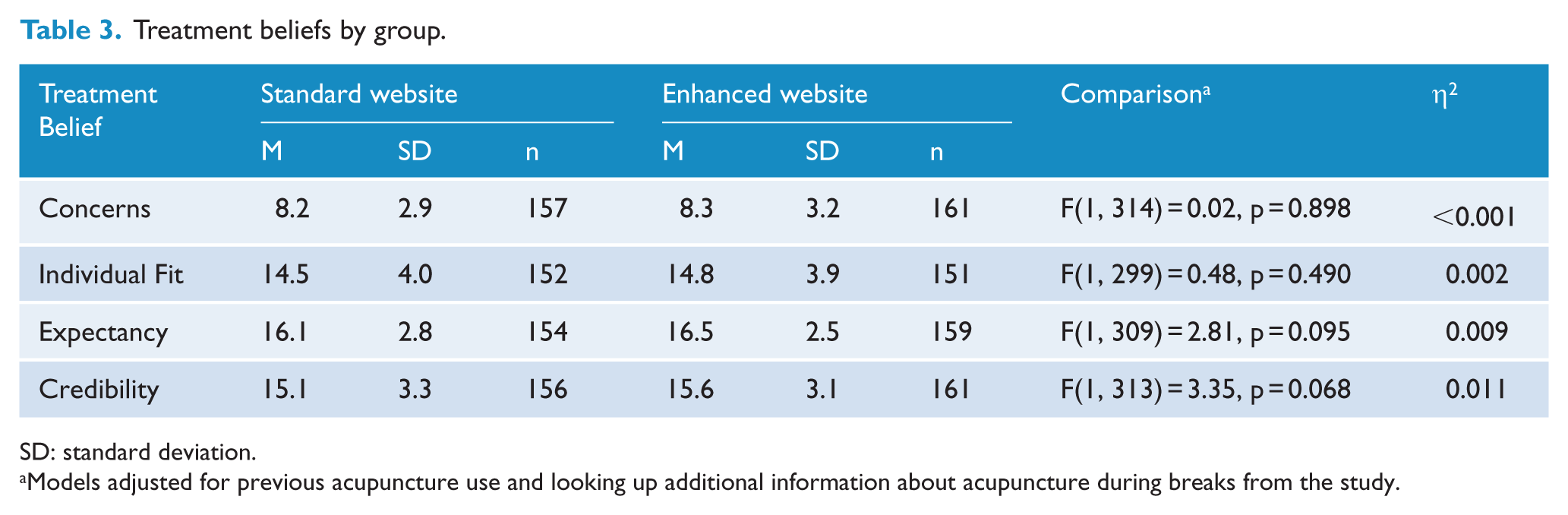
SD: standard deviation.
Models adjusted for previous acupuncture use and looking up additional information about acupuncture during breaks from the study.
Willingness to try acupuncture was very high and not affected by website: 85.1% of participants who had viewed the enhanced website and 82.8% of those who had viewed the standard website were willing to try acupuncture (χ2(1) = .34, p = 0.560).
Discussion
We tested the effects of a new educational website about acupuncture on adults with recent back pain, comparing it to a standard website based on existing written patient information. Participants who viewed the enhanced website had greater increases in knowledge about acupuncture and were three times more likely to make an informed choice about acupuncture, compared to participants who viewed the standard website. On average, viewing the enhanced website led participants to answer one more knowledge quiz item correctly (out of 10), while the standard website led to no additional quiz items being answered correctly. These effects are likely to be due, at least in part, to the additional information presented in the enhanced website, but might also be due partly to the additional formats (e.g. video and audio) that were used in the enhanced website, but not the standard website. There were no effects on treatment beliefs or willingness to try acupuncture. This might be due to ceiling effects (on expectancy, credibility and individual fit) and floor effects (on concerns). It would be interesting to test the effects of the enhanced website in a sample of participants less inclined to try acupuncture, although the natural audience for the website in practice will be participants who are at least willing to consider acupuncture. Perhaps, attempts to optimise patients’ beliefs about acupuncture would be more successful if integrated into the first acupuncture consultation and delivered by acupuncturists.
Strengths of this study include the enhanced website, developed using an approach based on person-based, evidence-based and theory-based intervention design, 33 and the use of a control website based on existing standard patient information. 30 Compared to traditional paper-based patient information leaflets, creating a website-enabled provision of more detailed information in an accessible and engaging manner, for example, using text, audio and film. In 2015, 86% of UK households had internet access and 78% of adults accessed the Internet daily or almost daily, 41 making online health information accessible to a large majority – but not all – of the population.
The generalisability of this study is limited by the largely pro-acupuncture participants drawn primarily from primary care. We do not know whether our website might improve acupuncture knowledge among people who hold strong negative attitudes towards it. Our participants were also slightly younger and more educated than a previous primary care sample of adults with back pain from the same region. 39 However, we are reasonably confident that the website is accessible to adults with less formal education as we attended to accessibility issues during its development. 33 Information about regulation and practicalities of accessing acupuncture is UK-specific and will need revising to reflect ongoing changes in regulation and provision. The design process for the enhanced website was driven by the person-based approach, in conjunction with the evidence- and theory-based approaches to intervention design. 33 Our website might have had larger effects if it had also been designed as a traditional patient decision aid, as such aids have been shown to increase knowledge and improve other decision-making outcomes although to date have shown limited effects on clinical outcomes; 42 future research should explore whether the person-, evidence- and theory-based approach that guided our website design could beneficially be applied to traditional patient decision aids. The outcome measures were previously validated and included assessments of objective knowledge and informed choice, which are particularly relevant when considering the potential for using the website to inform clinical trial volunteers. However, the conceptual strength of measuring informed choice is balanced by the statistical limitations of loss of data associated with deriving this outcome measure (following published guidelines) by dichotomising three continuous variables. Future studies should also test the website’s effects on behaviour (e.g. acupuncture utilisation).
The enhanced website could be used to support informed decision-making about acupuncture for back pain among primary care patients and the general public. Although not tested in this context, it might also be helpful for patients considering entering clinical trials of acupuncture. Future studies could use the website as the basis for more complex online resources, to support decision-making about acupuncture across multiple clinical conditions and/or to support informed choice among the multiple potential therapies for back pain.
Supplemental Material
AIM827228_Supplemental_material_1 – Supplemental material for Supporting informed choice in acupuncture: effects of a new person-, evidence- and theory-based website for patients with back pain
Supplemental material, AIM827228_Supplemental_material_1 for Supporting informed choice in acupuncture: effects of a new person-, evidence- and theory-based website for patients with back pain by Felicity L Bishop, Maddy Greville-Harris, Jennifer Bostock, Amy Din, Cynthia A Graham, George Lewith, Christina Liossi, Tim O’Riordan, Peter White and Lucy Yardley in Acupuncture in Medicine
Supplemental Material
AIM827228_Supplemental_material_2 – Supplemental material for Supporting informed choice in acupuncture: effects of a new person-, evidence- and theory-based website for patients with back pain
Supplemental material, AIM827228_Supplemental_material_2 for Supporting informed choice in acupuncture: effects of a new person-, evidence- and theory-based website for patients with back pain by Felicity L Bishop, Maddy Greville-Harris, Jennifer Bostock, Amy Din, Cynthia A Graham, George Lewith, Christina Liossi, Tim O’Riordan, Peter White and Lucy Yardley in Acupuncture in Medicine
Footnotes
Acknowledgements
The authors thank all who participated in the study, the primary care research network and general practitioners (GPs) who facilitated recruitment. Christine Bagg (patient representative) contributed to study design and helped review the website. Dr Jin Zhang and the core LifeGuide team provided technical support.
Contributors
F.L.B., G.L. and L.Y. conceptualised the research; F.L.B. led the design with input from all authors. M.G.-H. collected the data, which was analysed by M.G.-H. and F.L.B. All authors contributed to the interpretation of data. F.L.B. drafted the work and all authors revised it critically for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Arthritis Research UK, Chesterfield, UK, grant number 20113.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.