
Abstract
Individuals with brachial plexus injury (BPI) require upper limb function restoration, but the treatment remains controversial. Vitamin B12 may aid in pain control and nerve regeneration. We present the technical aspects of ultrasound-guided perineural vitamin B12 injection for BPI. The demonstrative case is a 50-year-old man with BPI resulting from a traffic accident. Under ultrasound guidance, vitamin B12 was injected precisely into the brachial plexus compartment around the swollen neuroma of the C6 root. Motor and sensory functions of the left upper extremity improved over 6 months. Ultrasound-guided perineural vitamin B12 injection may be an efficient and personalized intervention in cases of post-ganglionic BPI that failed to improve in the first 3 months.
Introduction
Brachial plexus injury (BPI) is a serious condition that causes upper limb function impairment and may result in life-long disability 1 . BPI can result from various etiologies, including penetrating injuries, falls, and motor vehicle trauma 2 . The incidence of BPI has been increasing. The brachial plexus comprises 5 roots, 3 trunks, 6 divisions, 3 cords, and terminal branches. BPI can be preganglionic or postganglionic, and the level of injury determines the appropriate treatment method or prognosis 3 .
BPI is diagnosed through physical examination, electrophysiological examination, and imaging and based on clinical history 4 . Electromyography conducted 2 to 3 weeks after the insult is commonly used as an early confirmation method; it involves identifying muscle fibrillation 5 . The image modalities of choice are computed tomography (CT) myelogram and magnetic resonance imaging (MRI) 6 . CT is fast and accurate but involves radiation exposure and artificial shading of bones. MRI plays a crucial role in differentiating between preganglionic and postganglionic injuries 7 . It may help determine the location and severity of injuries 8 . Furthermore, bone artifacts are avoided, multiplanar images can be obtained, and both proximal and distal parts of the brachial plexus are involved. Recently, high-resolution ultrasound has also emerged as a diagnostic tool and it helps to diagnose the post-ganglionic lesions of the brachial plexus6,7.
Conservative treatments include medications (e.g., steroids, vitamin B12, non-steroidal anti-inflammatory drugs [NSAID], and gabapentin), splint, and physiotherapy 4 . Surgical intervention is considered when recovery remains poor after 3 months 9 . In particular, the possibility of nerve regeneration is low in case of preganglionic injury, thereby necessitating nerve graft or transfer depending on the location and severity of the injury. Postoperative outcomes are better when the operation is performed within 6 months after injury (Fig. 1) 10 . The prognosis is better in the younger population and for injury to C5 to C7 roots 11 . Early diagnosis and prompt treatment initiation lead to better functional recovery. Nevertheless, no treatment guidelines for BPI exist.

Flowchart of brachial plexus injury management. EMG: electromyography CT: computed tomography; MRI: magnetic resonance imaging.
Perineural injection of medications for BPI is an emerging technique, and its efficacy remains to be validated. A previous study 12 administered vitamin B12 perineural injection in patients with peroneal neuropathy; the treatment was efficacious and was a fast, feasible, and safe treatment alternative for patients. Here, we present the technical aspects of ultrasound-guided perineural B12 injection for BPI, in which muscle power showed significant improvement after the treatment.
Case Presentation
Inclusion Criteria
Patient has incomplete postganglionic BPI diagnosed by clinical neurologic examination, EMG and MRI.
Patient evaluated in outpatient department from 2012 to 2018
Patient who age from 18 to 65 years old
Exclusion Criteria
Patient who had perinatal complications, shoulder surgery, or other nerve repair procedures of the brachial plexus
Allergy or intolerance to constraint intervention materials
Clinical cases
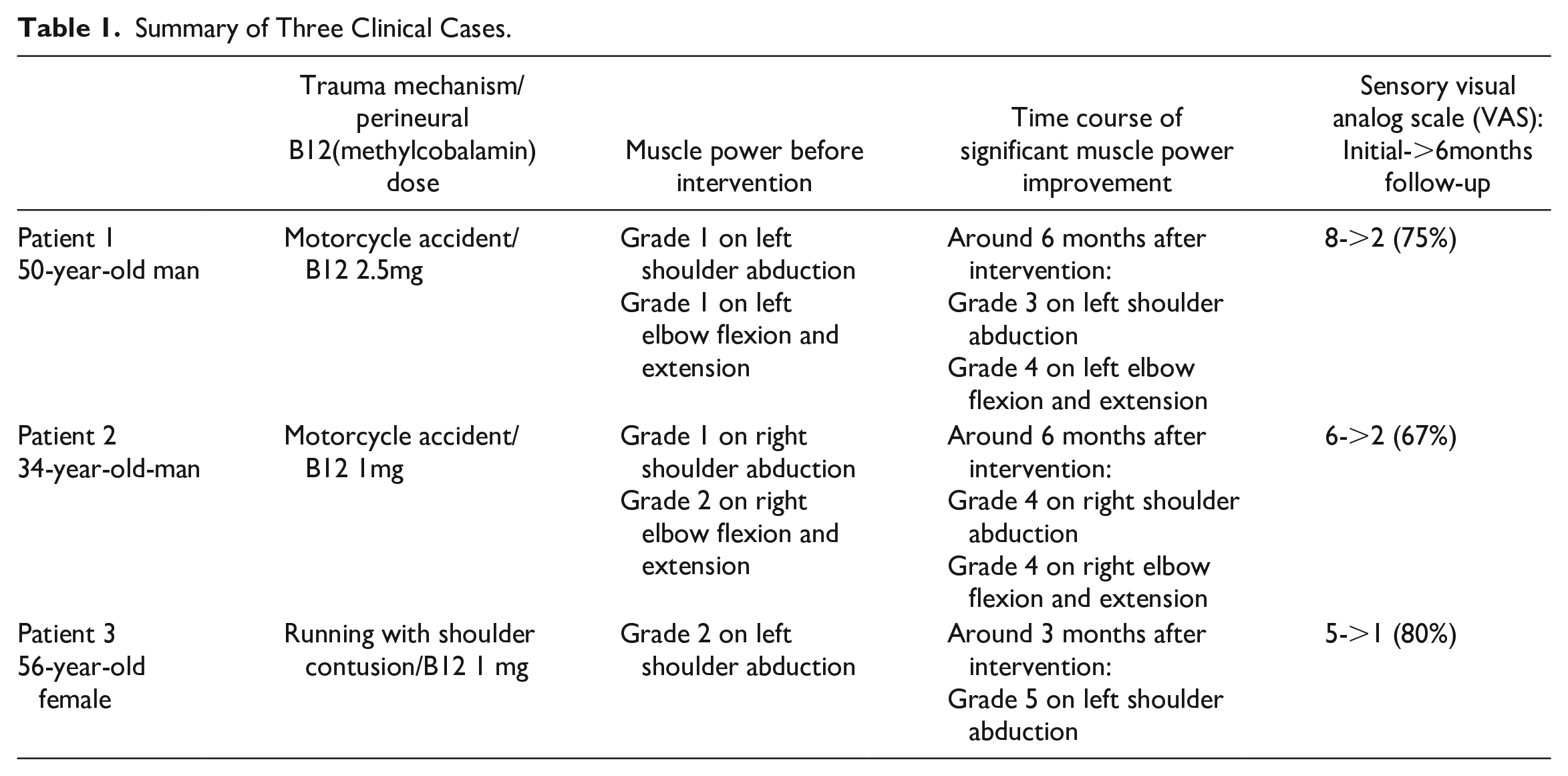
Demonstrative case: A 50-year-old man (Patient 1 of Table 1) presented to a community-based outpatient clinic with left arm weakness and numbness following a traffic accident 2 months before presentation, which involved traumatic subdural hemorrhage, facial bone fracture, left second rib fracture, and pneumothorax. He had no history of systemic illnesses, including diabetes mellitus, cancer, or immunological disorders.
Summary of Three Clinical Cases.
Electromyography and nerve conduction studies conducted 2 weeks after the accident confirmed a severe multiple trunk brachial plexopathy characterized by motor axon loss. MRI revealed increased signal intensity on a T2-turbo inversion recovery magnitude image over the left brachial plexus (Fig. 2). Traumatic BPI was suspected. The diagnosis of BPI was made by a neurologist.

T2-weighted image MRI of case 1. Increased signal intensity on a T2-WI image over the left brachial plexus. axi: axial view; cor: coronal view; MRI: magnetic resonance imaging; sag: sagittal view.
Physical examination confirmed marked ipsilateral sensory and motor loss of the upper extremity. Ultrasound indicated C6 root swelling with a hyperechoic scar along the injured nerves. Ultrasound-guided perineural injection with dexamethasone 1 ml (5 mg/ml) and methylcobalamin 5 ml (0.5 mg/ml) over the C6 root was performed. No procedure-related complications were reported. At the 3-month follow-up, the visual analog scale score improved from 8 to 3. The patient experienced marked motor improvement after 6 months.
Technical note
Ultrasonography examination was performed with a 10~18 MHz lineal ultrasound transducer (MyLab™25 Gold; Esaote S.p.A., Genova, Italy). The patient was positioned supine, with his head turned 30° to 45° contralateral to the side of the scan. A jelly pad was placed over the ipsilateral side of the injection site (Fig. 3A).

(A) Patient’s position and transducer was placed horizontally. (B) Identifying vertebral transverse process morphology. (C) Nerve tracking from neuroforamen revealed C6 neuroma formation over the interscalene groove. AT: anterior tubercle; PT: posterior tubercle; SCM: sternocleidomastoid muscle.
The steps of the ultrasound scan were as follows:
Step 1: The transducer was placed horizontally; the nerve roots were identified by analyzing the transverse processes of the corresponding vertebrae—C7 has only posterior tubercle and C6 has a prominent anterior tubercle (Fig. 3B).
Step 2: A transverse scan was performed between the anterior and middle scalene muscles. The transducer was placed transversely. Maintaining the transducer position, it was slightly tilted cephalad to adjust the ultrasound beam toward the cervical roots, and C5–C7 roots were visualized.
Step 3: The transducer was manipulated caudally to the supraclavicular area, with the same orientation until the vertebral artery appeared under color Doppler ultrasound. In our patient, the C6 root was swollen with a mass-like neuroma formation over the interscalene groove (Fig. 3C). After aseptic procedures, a 70-mm 23-gauge needle was inserted in the same plane in the lateromedial direction (Fig. 4A, B). Next, 1 ml (5 mg/ml) of dexamethasone and 5 ml of vitamin B12 (methylcobalamin, 0.5 mg/ml) (Fig. 4C *star) were injected around the neuroma and areas proximal and distal to it.

Ultrasound-guided perineural vitamin B12 injection of C6 neuroma. (A) Demonstrated illustration of neuroma injection. (B) In-plane injection from posterior to anterior, lateral to medial direction. (C) Drug was injected around the neuroma. ***: 5 mg of dexamethasone and 2.5 mg of vitamin B12; Arrow:23G needle.
Discussion
In the three clinical cases, precise ultrasound-guided perineural vitamin B12 injection appeared to be effective and beneficial for recovery from BPI, with sufficient neurological improvement observed and no apparent adverse effects.
High-resolution ultrasound has become a widely used diagnostic tool for peripheral nerve disorders. It offers many advantages, including portability, lack of radiation, real-time continuous imaging, and affordable guided interventions to detect neurovascular structures 7 . In patients with BPI, ultrasound allows direct visualization of the neurovascular structure of the brachial plexus, with an overall sensitivity of 87% to identify lesions from C5 to T1 6 , including swollen nerve fascicles or even neuroma 7 . In addition, this technical note demonstrated the feasibility and efficacy of ultrasound-guided perineural injection. The results of the ultrasound scan may also provide useful information for further surgical planning. Although medication for peri-neural regenerative injection is miscellaneous, such as 5% dextrose (D5W) and platelet-rich plasma (PRP), not limiting at vitamin B12 13 , vitamin B12 is crucial for numerous biological processes. It has affinity for neuronal tissues and serves as a cofactor for enzymes involved in folate metabolism and nucleotide biosynthesis 14 . Thus, it is required for the metabolism of fatty acids, amino acids, myelin, phospholipids, proteins, and neurotransmitters.
There are several literature regarding use of vitamin B12 to facilitate nerve regeneration (Table 2). Gan et al observed thickened myelin sheath and increased cross-sectional area of target muscle cells after daily mecobalamin administration intraperitoneally in rats with sciatic nerve injury 15 . In another study, vitamin B12 at concentrations above 100 nM is shown to increased Erk1/2 and Akt activities during the methylation cycle and subsequently facilitated neuronal growth 16 . Increased expression of βIII tubulin, the protein related to axonal maturation, was observed in a rat corneal injury model 17 . Experiments in a rat tibial nerve injury model indicated that vitamin B12 promoted myelin formation and reduced Wallerian degeneration 18 .
Literature Regarding Use of Vitamin B12 to Facilitate Nerve Regeneration.

When combined dexamethasone and vitamin B12 was administered, upregulation of brain-derived neurotrophic factor (BDNF), glial cell–derived neurotrophic factor, NT-3, and IL-6 were found in a rat sciatic nerve injury model 19 . Li et al demonstrated that vitamin B12 may up-regulated insulin like growth factor-1 (IGF-1) gene expression, and showed a better neuroprotective effect in the presence of good control of hyperglycemia in rats with diabetic peripheral neuropathy 20 .
Vitamin B12 supplementation relieves symptoms of peripheral neuropathy3,21,22. It may provide significant analgesic effects for postherpetic neuralgia, alcohol-related neuropathy, diabetic neuropathy, and aphthous ulcers 22 , with minimal adverse effects. By injecting vitamin B12 directly into the nerve compartment, a nerve regeneration effect is expected. In this technical note, the needle was introduced into the proximal and distal portions of the neuroma. To the best of our knowledge, few studies have analyzed the effect of local injection of vitamin B12.
Ide et al reported that high-dose intrathecal methylcobalamin injection can relieve symptoms of paresthesia, burning pain, and heaviness in patients with diabetic neuropathy 23 . In 2 randomized controlled trials conducted by Xu et al,24,25 the administration of vitamin B12 in varying forms in patients with postherpetic neuralgia and acute ophthalmic herpetic neuralgia sustainably and significantly decreased their pain severity for up to 1 year compared with controls receiving intramuscular injection of vitamin B12 and lidocaine. The results support the phenomenon observed in this report, in which vitamin B12 was injected at the swollen nerve roots.
Because a delay in providing therapy can lead to irreversible neurological dysfunction, advanced conservative therapy is strongly recommended in patients with BPI. Ultrasound-guided perineural injections can be administered before or after surgery to maximize the therapeutic effect.
In the demonstrative case, the cross-sectional area of C6 root swelling part has decreased from 15 mm2 to 12 mm2 three months after the procedure. The measuring of the nerve cross-sectional area has been used to determine the existence of nerve lesions.26,27 A quantitative ultrasonographic analysis of changes of the BPI may be desired in the future. Our results can guide future research on ultrasound-guided perineural injection of vitamin B12 in patients with BPI or other peripheral neuropathies.
Conclusion
High-resolution ultrasound has improved the diagnosis of brachial plexopathies, and ultrasound-guided perineural injection of vitamin B12 can serve as a treatment approach specific to injured nerves for preoperative or postoperative treatment in cases of post-ganglionic BPI.
Footnotes
Acknowledgements
I would like to express my deepest gratitude to the following individuals who have contributed to the completion of this article.
Authors’ Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used: “Conceptualization, C.H. Chen; methodology, S.P. Wang; software, H.Y. Huang; validation, S.P. Wang; formal analysis, S.P. Wang; investigation, S.P. Wang; resources, C.H. Chen; data curation, C.H. Chen; writing—original draft preparation, S.P. Wang; writing—review and editing, C.H. Chen.; supervision, C.H. Chen; project administration, C.H. Chen. All authors have read and agreed to the published version of the manuscript.”
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with “The Medical Ethics Committee of Kaohsiung Veterans General Hospital” approved protocols.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.