
Abstract
Bone marrow stem cell (BMSC) transplantation during coronary artery bypass graft (CABG) is an innovative treatment for ischemic heart disease (IHD). We conduct a meta-analysis to examine whether patients with IHD presenting heart failure with reduced ejection fraction (HFrEF) can be beneficent from CABG with additional BMSC transplantation. Electronic searches were performed on PubMed, EMBASE, Cochrane Library, and ClinicalTrials.gov from their inception to July 2021. The efficacy was based on left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVEDD), left ventricular end-diastolic volume (LVEDV), left ventricular end-diastolic volume index (LVEDVi), left ventricular end-systolic volume index (LVESVi), and 6-min walk test (6MWT) change after treatment. Eight randomized-controlled trials (RCTs) were included in this meta-analysis, with a total of 350 patients. Results showed BMSC transplantation significantly improved the LVEF [mean difference (MD) = 6.23%, 95% confidence interval (CI): 3.22%–9.24%, P < 0.0001], LVEDVi (MD = −20.15 ml/m2, 95% CI: −30.49 to −9.82 ml/m2, P < 0.00001), and LVESVi (MD = −17.69 ml/m2, 95% CI: −25.24 to −10.14 ml/m2, P < 0.00001). There was no statistically significant difference in the improvement of LVEDD, LVEDV, and 6MWT between the cell transplantation group and control groups. Subgroup analysis revealed that the intervention for control group could affect the efficacy of BMSC transplantation. Sensitivity analysis found the conclusion of LVEDD, LVEDV, and 6MWT changes was not stable. Therefore, among patients with IHD presenting HFrEF, BMSC transplantation during CABG is promising to be beneficial for postoperative left ventricular (LV) function improvement. However, according to the unstable results of the sensitivity analysis, it cannot be concluded whether the extra step has a positive effect on left ventricular remodeling and exercise capacity. RCTs with larger cohorts and more strict protocols are needed to validate these conclusions.
Introduction
Ischemic heart disease (IHD), also known as coronary heart disease or coronary artery disease, is one of the major causes of heart failure, especially in developed countries 1 . Many projects are dedicated to protecting the damaged myocardium and reducing heart remodeling. Previous studies have demonstrated that surgical revascularization is an optimal choice for IHD.
Based on the preoperative left ventricular ejection fraction (LVEF) and clinical symptoms, patients can be classified according to their grade of heart failure. Heart failure with reduced ejection fraction (HFrEF) is defined as LVEF lower than 40% combined with symptoms of heart failure 1 . Patients with HFrEF tend to develop a poorer prognosis2,3. Although patients with low LVEF are at high risk of surgery, they can obtain longer life expectancy and improved quality of life 4 . In most cases, for patients who underwent coronary artery bypass graft (CABG), LVEF improvement after surgery is associated with amelioration of heart failure symptoms as well as better prognosis4–6. However, not all patients with IHD have improved LVEF after revascularization, and the determining factors are varied, including preoperative LVEF status, heart remodeling, and incomplete revascularization 7 .
Stem cell therapy is a promising treatment for heart failure. It has been studied in small cohorts in ischemic, dilated, and restrictive cardiomyopathy, and the results are encouraging 8 . Stem cells can be derived from bone marrow, umbilical cord, and adipose tissue; among them, bone marrow stem cell (BMSC) is the most widely applied in basic researches and clinical practice. Bone marrow mixed with various types of cells, such as bone marrow mononuclear cells (BMMNCs), are a population of unpurified stem cells, mainly containing hematopoietic stem cells expressing CD31, CD34, CD45, and CD133; mesenchymal stem cells (MSCs) which express CD73, CD90, and CD105; endothelial progenitor cells (EPCs); and several other cell lines 8 . BMMNCs are widely used as they can easily be isolated by density gradient centrifugation, while harvesting subgroups with specific biomarkers require extra steps such as flow cytometric methods. CD34+, CD45+, and CD133+ hematopoietic stem cells are commonly used due to their angiogenic ability, which contribute to the improvement of blood supply for ischemic myocardium9,10. MSCs are not as effective as hematopoietic stem cells owing to the different expression of proangiogenic factors 11 . Researchers have attempted to combine the two therapies to investigate whether better outcomes can be achieved. However, the outcomes remain controversial.
Heart failure with recovered ejection fraction (HFrecEF) is a new definition recently proposed for HF with baseline LVEF ≤40%, a ≥10% increase from baseline LVEF, and a second measurement of LVEF >40% 12 . A retrospective and observational study showed that IHD patients with postoperative ejection fraction changes meeting the definition of HFrecEF had a significantly reduced risk of long-term mortality up to 39% compared with patients with persistent HFrEF 13 . Here, we performed a meta-analysis to evaluate the potential therapeutic effects of combining BMSC transplantation during CABG for heart failure patients with reduced ejection fraction.
Methods
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines 14 . The methodology used to conduct this study was as follows.
Search Strategy
Electronic searches were performed on PubMed, EMBASE, Cochrane Library, and clinictrials.gov (all from their inception to July 2021) with the following database-appropriate terms: coronary artery disease, chronic IHD, myocardial infarction, BMSCs, mesenchymal stromal cells, stem cells, coronary artery bypass, CABG, surgical revascularization, and trial. There were no restrictions on publication time or language. In addition, we did a citation search in relevant reviews. The references of the selected papers were read for potentially relevant information.
Inclusion Criteria
Studies were included based on the following criteria: (1) patients diagnosed with chronic IHD; (2) randomized-controlled trials comparing CABG in combination with BMSC therapy and standard CABG for chronic IHD, the stem cell can isolate either directly from bone marrow or from peripheral blood after mobilization of bone marrow; (3) preoperative LVEF ≤40%; and (4) follow-up for at least 3 months after cell transplantation therapy.
Exclusion Criteria
The exclusion criteria were as follows: (1) nonrandomized-controlled trials, (2) acute myocardial infarction or emergency surgery, (3) surgical procedures other than CABG (eg, percutaneous coronary intervention) or combining with valve replacement, (4) cells derived from sources other than the bone marrow (eg, umbilical cord blood), and (5) the study’s inclusion criteria for participants was LVEF ≥40% or not mentioned in the criteria.
Quality Assessment
Cochrane Collaboration’s tool was used to evaluate the risk of bias among the included studies. The aspects that were assessed include the potential bias in selection, performance, detection, attrition, and reporting processes of studies.
Data Collection and Analysis
Two researchers independently reviewed and assessed the included studies, and extracted data from the original studies. The primary outcome was the mean difference (MD) of LVEF change after treatment (
The calculation resulted in Corr = 0.55 for the experiment group and Corr = 0.25 for the control group. And then the SD of

Secondary outcomes were based on other parameters associated with left ventricular remodeling and exercise capacity, such as left ventricular end-diastolic diameter (LVEDD), left ventricular end-diastolic volume (LVEDV), left ventricular end-diastolic volume index (LVEDVi), left ventricular end-systolic volume index (LVESVi), and 6-min walk test (6MWT). Statistical analyses use the same method as LVEF change.
Analyses were done with RevMan (Version 5.4. The Cochrane Collaboration, 2020). Statistical heterogeneity was assessed using the I 2 statistic. The value of I 2 is expressed as a percentage, with 25%, 50%, and 75% indicating low, medium, and high heterogeneity, respectively 20 . If the studies are of low heterogeneous, the fix-effects model was selected. If not, the random-effects model was selected. Funnel plots were used to detect the possible publication bias. In addition, subgroup analysis was conducted to evaluate whether the characteristics (sample size, type of cells, count of cells, delivery routes, intervention for control group and measurement method) of studies affect the primary outcome. Sensitivity analysis was used to detect the source of heterogeneity. P < 0.05 was considered as statistically significant.
Results
Search Results
Initial search identified 418 studies. After removing 68 duplicates, we screened 350 articles. Among this, 306 were screened out after reviewing the title and abstract, the remaining 44 studies were screened for further full-text assessment. As four articles were from the same cohort, we selected 1 trial 21 that contained most of the parameters and combined other secondary parameters in the rest of the articles. Citation search identified 65 studies. The final number of studies included in this meta-analysis was eight. A PRISMA flow diagram depicting the detailed process is presented in Fig. 1.

PRISMA 2020 flow diagram.
Study Characteristics
A total of eight studies met the inclusion criteria for the present meta-analysis, including 350 patients with chronic IHD. The “cell transplantation group” (n = 190) included participants who had received CABG combined with BMSCs transplantation, while the “control group” (n = 160) included patients who had CABG with or without placebo injection. Characteristics of included studies are summarized in Table 1.
Study Characteristics of Included Studies.

Values are mean ± SD. BMMNC: bone marrow mononuclear cell; BMSC: bone marrow stem cell; CMR: cardiovascular magnetic resonance; Echo: echocardiography; IC: intracoronary; IM: intramyocardial; ONCABG: on-pump coronary artery bypass graft; OPCABG: off-pump coronary artery bypass graft.
Risk of Bias Assessment
Of the eight included studies, five (62.5%) adequately generated their randomization sequence, three (37.5%) concealed allocation, six (62.5%) blinded participants and personnel, and five (62.5%) blinded outcome assessment. Trifunović et al. 26 had a high risk of performance bias and detection bias due to an open-label study. Soetisna et al. 19 was a single-blind trial with a high risk of detection bias. All studies had a low risk of bias regarding selective reporting and a low risk of bias regarding missing outcome data. The detailed information on risk of bias is provided in Figs 2 and 3.

Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.

Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.
Primary Outcome
All eight studies, including a total of 324 participants, reported the change in LVEF after surgical revascularization. The LVEF change in patients who underwent BMSC transplantation during CABG is statistically significant compared with standard CABG procedure (MD = 6.23%, 95% CI: 3.22%–9.24%, P < 0.0001; Fig. 4).

Forest plot of comparison: left ventricular ejection fraction changes after treatment.
Secondary Outcomes
Secondary outcomes among both examined groups for all trials are detailed in Fig. 5. The additional bone marrow transplantation and conventional treatment are both beneficial for left ventricular parameters. There is no significant difference on the change of LVEDD (MD = −3.16 mm, 95% CI: −10.27 to 3.95 mm, P = 0.38; Fig. 5A) and LVEDV (MD = −16.33 ml, 95% CI: −42.49 to 9.83 ml, P = 0.22; Fig. 5B) after treatment between the cell transplantation groups and control groups. While the reduction of LVEDVi and LVESVi after treatment are significantly different in comparison with the control: −20.15 ml/m2 (95% CI: −30.49 to −9.82, P < 0.00001; Fig. 5C) for LVEDVi and −17.69 ml/m2 (95% CI: −25.24 to −10.14, P < 0.00001) for LVESVi (Fig. 5D). Although the exercise capacity reflected by the 6MWT is improved after surgery, the improvement is not significant (MD = 34.96 m, 95% CI: 9.63 to 60.30 m, P = 0.54; Fig. 5E).
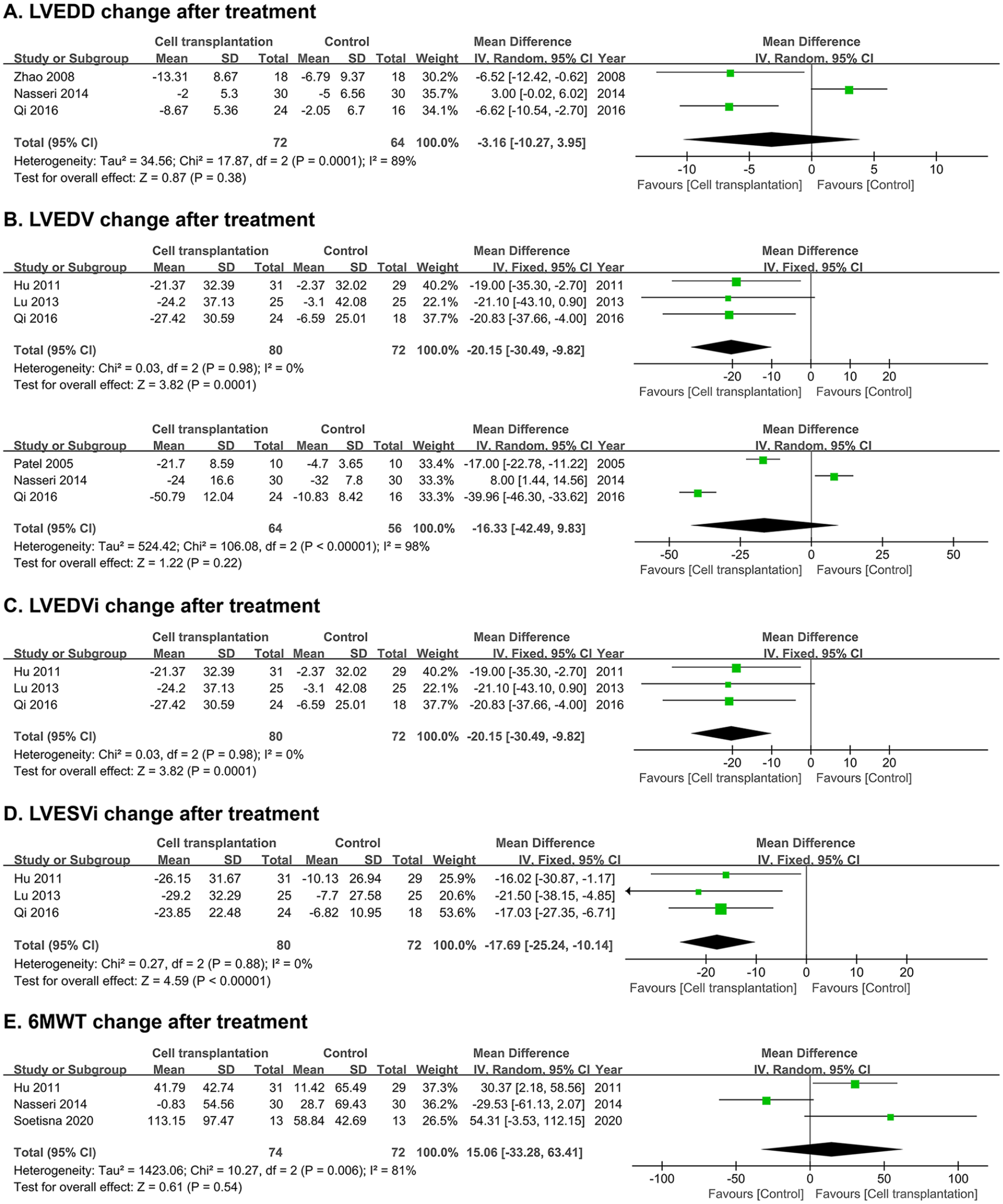
Forest plot of secondary parameters comparison: (A) left ventricular end-diastolic diameter change after treatment; (B) left ventricular end-diastolic volume change after treatment; (C) left ventricular end-diastolic volume index change after treatment; (D) left ventricular end-systolic volume index change after treatment; and (E) 6-min walk test results change after treatment.
Publication Bias
Funnel plot (Fig. 6) was used to assess the potential publication bias. As shown in the figure, there was publication bias in the included eight studies. The asymmetry can be explained by the heterogeneity of the studies and differences in methodological quality.

Funnel plot for comparison of changes in left ventricular ejection fraction.
Subgroup Analysis
Significant heterogeneity was observed in the primary outcome. We performed a subgroup analysis based on the characteristics of studies (Table 2). In subgroup analyses, there were no differences in the LVEF change after treatment based on sample size, type of cells, count of cells, delivery routes, and measurement method. However, comparison of intervention for control group (placebo injection vs no placebo in the control group) detected a statistically significant difference (P = 0.007).
Subgroup Analysis for LVEF Change of Cell Therapy.

BMMNC: bone marrow mononuclear cell; BMSC: bone marrow stem cell; CABG: coronary artery bypass graft; CI: confidence interval; CMR: cardiovascular magnetic resonance; Echo: echocardiography; IC: intracoronary; IM: intramyocardial; LVEF: left ventricular ejection fraction; MD: mean difference.
Sensitivity Analysis
We discovered a significant heterogeneity in a few metrics. Sensitivity analysis revealed that the Nasseri et al. 25 study is the source of heterogeneity. When this specific study was removed, the remaining four studies showed dramatic reduction of heterogeneity in the comparison of LVEF change after treatment (P = 0.09, I 2 = 46%, MD = 7.68%, 95% CI: 5.64%–9.71%), but it does not markedly affect the result. However, the results of LVEDD, LVEDV, and 6MWT change after treatment are not consistent if the Nasseri et al. 25 study was removed (Table 3), indicating that the conclusions were not reliable.
The Influence of Secondary Outcomes When Excluding Nasseri et al. 25 Study.

CI: confidence interval; LVEDD: left ventricular end-diastolic diameter; LVEDV: left ventricular end-diastolic volume; MD: mean difference; 6MWT: 6-min walk test.
Discussion
Although there have been several meta-analyses for the effectiveness and safety of BMSCs, due to the different inclusion criteria of each trial and the updated definition of heart failure, no available meta-analysis has focused on this specific type of patients. IHD presenting HFrEF is a tough scenario in clinical practice and needs to be further studied. This study pooled eight randomized clinical trials that compared BMSC transplantation during CABG with standard CABG in patients who have HFrEF caused by IHD. Compared with standard CABG surgery, additional BMSC transplantation may have better improvement on LVEF, LVEDVi, and LVESVi after treatment. We found surgical revascularization beneficial for left ventricular remodeling and exercise capacity, though the statistical difference was not significant in our analysis. Sensitivity analysis revealed that the results of LVEDD, LVEDV, and 6MWT were not stable.
The included studies showed a high heterogeneity (I 2 = 89%). Thus, a subgroup analysis was conducted based on the study characteristics. Results of subgroup analysis revealed that the intervention for the control group affect the primary outcome. Among the three studies in the CABG only group, two trails19,26 did not use blinding, and one 22 may not strictly follow the requirements of blinding because the cardiologists may involve in both surgery and outcome measurement. The lacking of blinding may influence the patients’ and doctors’ behavior in the postoperative treatment, which will be the source of bias 18 . Sensitivity analysis suggests that Nasseri et al. 25 was a source of heterogeneity in the meta-analysis of LVEF, LVEDV, and 6MWT. It also affects the stability of LVEDD, LVEDV, and 6MWT. The result of Cardio133 trial reported by Nasseri et al. 25 claimed that CD133+ BMSCs did not improve global left ventricular (LV) function and clinical symptoms. The heterogeneity of Cardio 133 trial may owe to the longer storage time (48 h before surgery) in vitro and insufficient number of cells (Medium 5.1 × 106), which involves the questions often asked in cell therapy, such as when to prepare and inject cells, how to inject cells, which type of cells to use, and the dose of cells25,27,28. Also, the outcome can be affected by the medication after surgery. These issues have to be further studied before a common consensus or standard protocol can be achieved.
LVEF is not the only metric of left heart function, yet it is simple and intuitive. Only a few articles reported the relationship between postoperative LVEF improvement and prognosis, especially long-term follow-up results. The follow-up time in trails of cell therapy in patients with IHD is mostly between 6 and 12 months. In our analysis, the majority of follow-up time in the included studies was 6 months. Only one study conducted a long-term follow-up, with a median follow-up period of 5 years. Schiffer et al. 29 reviewed the data of surgical treatment for ischemic heart failure (STICH) trial and discovered that in patients with HFrEF, the normalization of LVEF after 2 years instead of early normalization tend to have a noticeable reduction of mortality in long-term follow-up. The mechanism behind this situation is the hibernating myocardium suffering from chronic myocardial ischemia takes months to recover after complete revascularization, which correlates with the severity of ischemia30,31. In our included studies, when the outcomes were evaluated with either magnetic resonance imaging (MRI) or single photon emission computed tomography (SPECT), they all discovered a better perfusion improvement and reduction of scar size at the injection site15,19,23,25. BMSC transplantation may contribute to the revascularization to restore the function of hibernating myocardium. However, whether LVEF normalization accelerated by BMSC therapy is beneficial for long-term outcomes needs more trials conducted with a longer follow-up period. The doctors’ interpretation of the outcome after cell transplantation needs to be based on the individual patient and evaluated on multiple dimensions rather than just LVEF.
Whether the stem cells are injected using intracoronary (IC) or intramyocardial (IM), the localization of stem cells is a problem to be solved. Weber et al. 32 described a hydrojet-based technique to transplant cardiomyocytes which derived from footprint-free induced pluripotent stem cells (iPSCs) into myocardium. As a more precise and less invasive way to transplant stem cells, hydrojet-based technique has the potential to be a superior approach to traditional needle-based injections (eg, IC or IM) in future CABG procedures or other cell-based therapies. Due to the current advances in biomaterials, some researchers use engineered epicardial patches made of hydrogel, fibrin, and other materials embedded with stem cells to enhance the function of damaged heart33–35. Most of these new strategies have not been tested in humans, but they provide new approaches and perspectives to improve the efficacy of cell transplantation in the future.
Although the results of our analysis are promising, there are some limitations. First, there was a publication bias in the included studies. The source of bias may be the flaw of study design or that positive results are more likely to be published. Second, significant heterogeneity was detected, which may relate to the design and performing of the trials, different parameters reported in each trial. The heterogeneity significantly affected the stability of secondary outcomes, as a result, we cannot draw a conclusion. Meanwhile, the sample size of included studies was relevantly small, and the follow-up time was short. Therefore, more caution is needed when generalizing the findings of the study to a larger group.
In conclusion, among patients with IHD presenting HFrEF, BMSC transplantation during CABG is promising to be beneficial for postoperative LV function improvement. Whether the extra cell transplantation process can reverse LV remodeling more effectively cannot be interpreted. Randomized-controlled trials with larger cohorts and more strict protocols are needed to validate this conclusion.
Footnotes
Availability of data,code,and other materials
All data collected and analyzed during this study are included in this published article and its supplementary information files.
Ethical Statement
Ethical approval is not applicable to this study.
Statement of Human and Animal Rights
This article does not directly involve any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The National Natural Science Foundation of China (No. 92168203, 82241201), Suzhou Municipal Science and Technology Bureau (SYS2020113, KJXW2021001), Natural Science Foundation of the First Affiliated Hospital of Soochow University (BXQN202131), and Postdoctoral Science Starting Foundation of Soochow University (No. 3231706319).