
Abstract
A rotator cuff tear is an age-related common cause of pain and disability. Studies including our previously published ones have demonstrated that mesenchymal stem cells cultured under hypoxic conditions [hypoxic multipotent stromal cells (MSCs)] facilitate the retention of transplanted cells and promote wound healing. However, there are very few, if any, reports targeting the punctured supraspinatus tendons to create more or equally serous wounds as age-related tears of rotator cuff. It remains to be determined whether transplantation of bone-marrow-derived hypoxic MSCs into the punctured supraspinatus tendon improves tendon repair and, when combined with ultrasound-guided delivery, could be used for future clinical applications. In this study, we used a total of 33 Sprague-Dawley rats in different groups for normal no-punched control, hypoxic MSC treatment, nontreated vehicle control, and MSC preparation, and then evaluated treatment outcomes by biomechanical testing and histological analysis. We found that the ultimate failure load of the hypoxic MSC-treated group was close to that of the normal tendon and significantly greater than that of the nontreated vehicle control group. In vivo tracking of cells labeled with superparamagnetic iron oxide (SPIO) nanoparticles revealed an enhanced retention of transplanted cells at the tear site. Our study demonstrates that hypoxic MSCs improve rotator cuff tear repair in a rat model.
Introduction
The rotator cuff is a critical component of shoulder function, and is important for the completion of shoulder movements 1 , particularly in raising and rotating an arm. A rotator cuff tear is a common cause of pain and disability. Its age-related asymptomatic prevalence rates range from 13% to 80%2,3. Depending on the study, the prevalence of symptomatic rotator cuff tear accounts for 4% to 32% of people with rotator cuff tears. As shown in a study by Yamaguchi et al. 4 , which the bilateral shoulders of patients with unilateral shoulder pain were scanned by ultrasound, there was a positive correlation between cuff tear and aging. In general, the etiology of rotator cuff tear is multifactorial and has been attributed to both extrinsic and intrinsic mechanisms 5 . The extrinsic factor of chronic degeneration is impingement from the bone structure adjacent to the cuff to the cuff tissue, and intrinsic factor is when the tensile load within the tendon exceeds its recovery and adaptive responses. Although acute avulsion of the rotator cuff is common in trauma or contact sports, microtrauma, as the result of repetitive activities, often causes a certain degree of inflammation or swelling, usually seen in overhead-throwing athletes 6 .
The repetitive microtraumas and full-thickness rotator cuff tears do not heal over time and may progress into more severe shoulder syndromes4,7–9. There are no reliable conclusions about the best treatment for degenerative cuff tears. Due to limited evidence, no conclusions have been drawn about the relative advantages and disadvantages of surgical or conservative treatment either1,10–12. However, studies have shown that the recurrent tear rates after surgical repair for this type of injury vary greatly, ranging from 20% to 70%13,14.
Due to recent advances in stem cell technology, there has been considerable interest in biological and cell-based therapeutic approaches aimed at improving healing and function before and after surgical repair15–17. The benefits and advantages of hypoxic culture on ex vivo-expanded bone marrow multipotent stromal cells (MSCs) have already been demonstrated18–20. In long-term culture, hypoxia has been found to inhibit senescence, increase proliferation rates, and enhance the differentiation potential of different MSCs. Hypoxia can also modulate the paracrine effects of MSCs, leading to various secreted upregulatory factors, including vascular endothelial growth factor and interleukin 6 (IL-6), to promote wound healing. Finally, hypoxia plays an important role in the migration and homing effect of MSCs, mainly through its ability to induce stromal-cell-derived factor 1 to express it in association with its receptor CXCR4 18 . Huang et al. 21 used the hypoxic MSCs to repair injured Achilles tendon and proved its efficacy in helping the healing process. Chen et al. investigated the role of adipose multipotent stromal cells (AMSCs) and bone marrow multipotent stromal cells (BMSCs) in tendon differentiation in a model of patellar tendon injury under hypoxia, and performed histological and biomechanical analyses. The resulting data showed that hypoxia significantly enhanced the expression of Col-1a1, Col-3a1, Dcn, and Tnmd in BMSCs in vitro. Furthermore, hypoxic BMSCs exhibited improved histological appearance and biomechanical properties compared with normoxic BMSCs in vivo 20 . This study aimed to investigate whether the use of hypoxic MSCs could enhance the healing from a full-thickness tear of a supraspinatus tendon in a rat model.
Materials and Methods
Isolation of MSCs From the Bone Marrow of Sprague-Dawley (SD) Rats
The animal experiments were conducted in accordance with the Guide for the Care and Use of Laboratory Animals and were approved by the Animal Board Committee of China Medical University (Taichung, Taiwan). Both femurs of two skeletally mature SD rats were removed and collected, and the soft tissues were detached aseptically. The ends of the bones were cut and an 18-gauge needle that was inserted into shaft of the bone marrow was extruded by flushing it with basal medium consisting of α-minimal essential medium (α-MEM; Gibco-BRL, Gaithersburg, MD, USA). Before the mononuclear cells were seeded in plastic dishes, density gradient centrifugation was used to isolate them from bone marrow aspiration, and complete culture medium (CCM) consisting of α-MEM, 16.6% fetal bovine serum (FBS), 100 U/ml penicillin, 100 µg/ml streptomycin, and 2 mM
Animal Protocol
A total of 31 SD rats, 12 weeks of age and weighing 250 to 300 g, were used for supraspinatus tendon healing experiments (Fig. 1), which involved biomechanical testing (3 tendons) and histological (32 tendons) and superparamagnetic iron oxide (SPIO) cell tracking analyses (4 tendons). All rats were purchased from the National Laboratory Animal Center (Taipei, Taiwan). They were given sufficient food and allowed light in a laboratory room with controlled temperature at 22°C ± 2°C and suitable humidity between 50% and 70%. The calculated maximum dose of chloral hydrate (15307; Riedel-de Haen, Seelze, Saxony, Germany) was set at 0.01 ml/kg for adequate anesthesia and was injected intraperitoneally in SD rats. The moderate size full-thickness rotator cuff tears were done aseptically and were mechanically manufactured by a puncher. The procedure went like this: (1) Cut the shoulder skin open with a 2-cm wound; (2) cut into the muscle layer for about 1 cm along the acromion triangle; (3) use a pair of forceps to lift the supraspinatus tendon with muscle, then place it underneath the supraspinatus muscle and hold it; and (4) carefully and firmly punch a 1.8-mm diameter hole at the center of the tendon (Fig. 2). The same procedure was performed on both supraspinatus muscles of the rat. Each hole of the supraspinatus tendons was filled with an injection of hypoxic MSCs with glue gel in the right side (hypoxic MSC group) 22 and only glue gel in the left side (as control group). The rats were returned to the original cages after the procedures and with their wounds closed. Both supraspinatus tendons in each rat were used for either biomechanical analysis or histological evaluation. The entire supraspinatus muscle and tendon of the shoulder along with the humeral head of treated rats were isolated and collected at 2 and 4 weeks. The rats were fully anesthetized during the procedures and euthanized afterward with chloral hydrate.
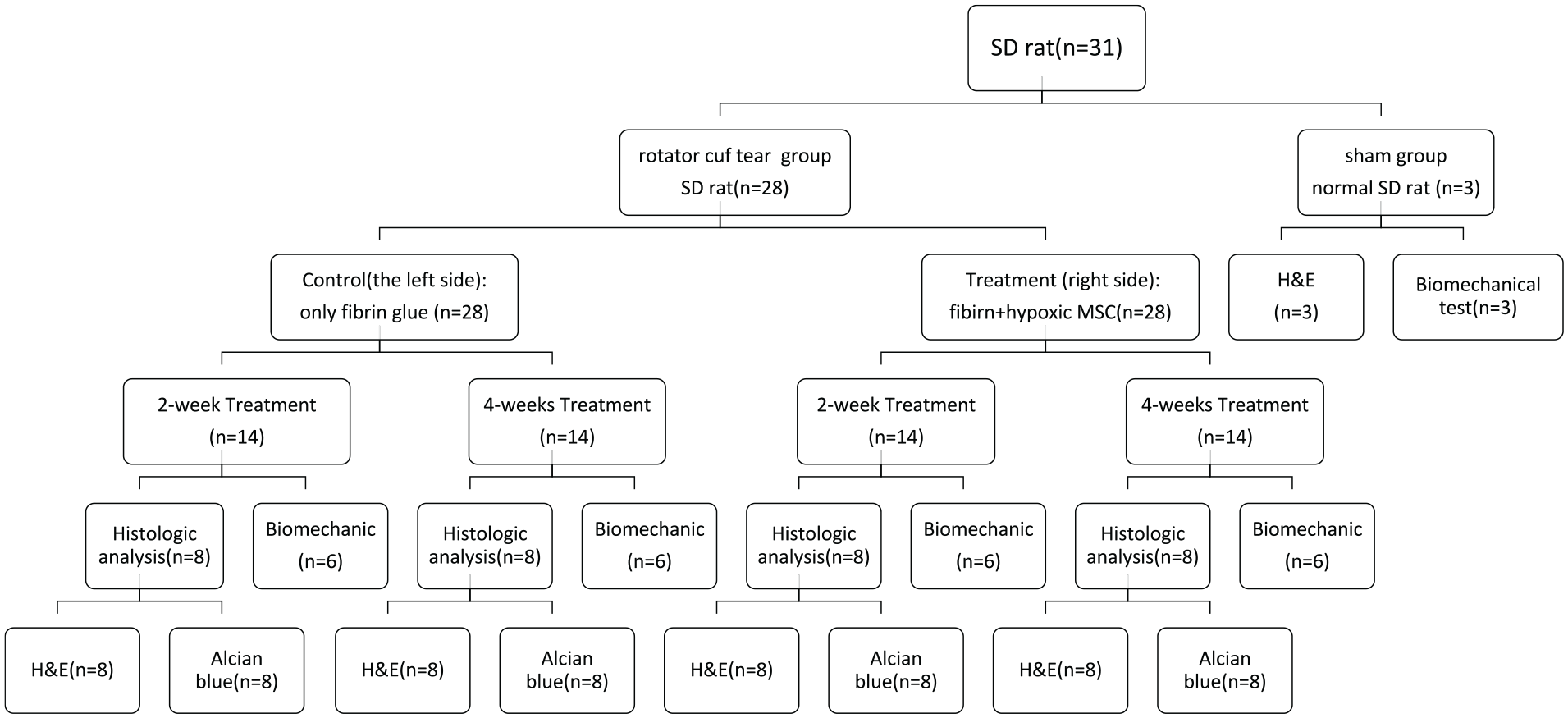
Schematic flowchart and use groups of the experimental design in the study of hypoxic cultured MSC healing improvement. MSC: multipotent stromal cells; SD: Sprague-Dawley.

The supraspinatus tendon was lifted into view by a pair of forceps and a hole of 1.8 mm in diameter was carefully punched in the center to make sure its severity level.
Biomechanical Testing
Before the treated rats were put to euthanasia, the supraspinatus tendon between the musculotendinous junction and the great tubercle of humerus was transacted and harvested at 2 and 4 weeks after the treatment of cultured MSCs; 9 to 18 supraspinatus tendons in each group were used at each time point. A rate of 10 mm/min with a preload of 5 N23,24 was set on a material testing machine (JSVH1000; Japan Instrumentation System, Nara, Japan) to gauge the load to failure and its tear mode. The treated/untreated supraspinatus tendons harvested were placed on the horizontal rack of a thrust apparatus, a customized fixture clamping system, one by one with one end of the tendon muscle deep-freeze sprayed (−40°C) to make it adhere to one side of the machine to go through a tensile testing. Each treated/untreated supraspinatus tendon was fixed to the clamping system with its tendon to bone forming a right angle and along its anatomical orientation for maximum loading capacity purpose, and was gradually pulled and loaded to capacity then ruptured in the middle or separated from the bone. The maximum tensile strength of the tendons from nonpunched normal rats was also measured for comparison and analysis. All rats received injection of hypoxic MSCs in the right tendon (hypoxic MSC group) and the left tendons (control group) were used for both biomechanical analysis and histological evaluation.
Tissue Preparation, Histological Analysis
For histological analyses, the excised supraspinatus tendons were fixed in formalin (10% formaldehyde) for 1 week, then went through a paraffin infiltration process for dehydration and wax block building. Afterward, they were cut into 4-mm chunks and randomly stained using Alcian blue, hematoxylin and eosin (H&E), or Masson trichrome stain, and formed three different sample groups. The stain type of the sample groups was not revealed to evaluators for blind test purpose. The tenocyte, ground substance, collagen, and vascularity variables of the longitudinal sections of the supraspinatus tendons were evaluated for histopathological analysis according to the semiquantitative Bonar histopathological scale 25 . Each variable was evaluated and given a number between 0 and 3, with 0 meaning normal (best) and 3 indicating an abnormal appearance (worst). The final score for each microscopic slide varied between 0 (normal tendon) and 12 (severest abnormal appearance). The focal points of the evaluation for each variable are as follows: (1) the morphology and proliferation for tenocyte (spindle cell), (2) the presence or absence of ground substance, (3) the bundle characteristics of collagen, and (4) the degree of vascularity. Each microscopic slide of tendon tissues from nontreated or hypoxic MSC groups was examined by a pathologist.
Cell Labeling With SPIO Nanoparticles
The aqueous SPIO solutions in the form of 0.2 M iron (II) (Sigma-Aldrich, St.Louis, MO, USA) and 0.1 M iron (III) (Sigma) were made by dissolving FeCl2 and FeCl3, respectively
26
; 4 ml of iron (III) (Sigma) and 1 ml of the iron (II) (Sigma) solutions were mixed to make Fe3O4 nanoparticles at room temperature, and 5 M NaOH was added to make its pH value at 11. To achieve complete coating of the particle surface, 3 g of organic acid was added to the precipitates after their exposure to a magnet and washed with deionized water. The excess adherents were removed by centrifugation before the precipitates were redispersed in deionized water again. The aqueous SPIO solution was coated with poly-
Statistical Analysis
All quantitative variables are expressed as mean and standard deviation. Statistical comparisons of the biomechanical testing and the histopathological grading were performed for both groups. The null hypothesis that there is no difference between the means was rejected when P value was less than 0.05, and we concluded that there were significant differences. Statistical analyses were performed using SPSS software version 11.0 (SPSS, Inc., Chicago, IL, USA).
Results
Preparation and Expansion of MSCs Under Hypoxic Conditions
MSCs isolated from the same SD rats were expanded under hypoxic conditions before use. Hypoxic MSCs were used to treat the injured supraspinatus tendon and their effects on tendon healing were compared. The expansion of MSCs was carried out by the following steps. The first step was to culture the mononuclear cells of bone marrow under hypoxic (1% O2) conditions at a seeding density of 104 cells/cm2 for 24 h 21 . In the second step, an irrigation procedure was performed by changing the medium to remove nonadherent cells. In the third step, some adherent cells were observed at 72 h after the initial culture. In the fourth step, most cells in the hypoxic culture formed aggregates after 9 days, with its confluence at the center. In the fifth step, the cells would begin a series of subcultures every 9 days where cells always reached confluence. They were harvested and subcultured at a lower density of 100 cells/cm2 at each subculture. The series of subcultures could be repeated up to 7 times and the data indicate that a rat MSC culture in a hypoxic setting increases its expansion efficiency and proliferation capacity. The hypoxic MSCs met the minimal criteria for defining multipotent mesenchymal stromal cells 27 . For example, they were plastic-adherent when maintained in standard culture conditions. Second, they expressed CD105, CD73, and CD90, and lack expression of CD45, CD34, CD14 or CD11b, CD19, and HLA-DR surface molecules. Third, hypoxic MSCs maintained the ability to undergo differentiation into osteoblasts, adipocytes, and chondroblasts in vitro 28 .
Macroscopic Assessment
The effects of hypoxic MSCs on the tendon healing were examined on the incised supraspinatus tendons of the animals sacrificed at 2 and 4 weeks after the transplantation of the hypoxic MSCs from the same SD rat donor. The supraspinatus tendons in both the cell-treated and nontreated groups had a hole punched with a diameter greater than 1.8 mm. The appearances of the supraspinatus tendons were similar at 2 weeks after injury for both groups. However, the punched holes in supraspinatus tendons of the nontreated group were apparently observable at 2 weeks after injury while holes in the cell-treated group were almost undetectable. But no clear macroscopic differences between the two groups could be observed at 4 weeks after injury.
Biomechanical Testing
A total of 12 SD rats underwent the tendon tensile test: 6 received the biomechanical test 2 weeks after punching and the remaining 6 were tested 4 weeks after punching. The results after 2 weeks showed that the mean values of failure load were 48.4 and 37.49 N/mm2 for treated and untreated rats (different sides of the same rat), respectively (Fig. 3A; P = 0.0034, P < 0.05). The results after 4 weeks showed that the mean values of failure load were 49.94 and 36.31 N/mm2 for treated and untreated rats (also different sides of the same rat), respectively (Fig. 3B; P = 0.0055, P < 0.05). The mean failure loads of the tendons treated with hypoxic MSCs for 2 or 4 weeks were not significantly different from the mean failure load of normal tendons (54.98 N/mm2) as the unpaired t test with Welch’s correction (P = 0.13, P = 0.29; Fig. 3C).

Biomechanical test revealed that better failure loads correlated with hypoxic MSC-treated tendons. (A) The average ultimate failure load of the harvested tendons from the hypoxic MSC-treated group was significantly greater than those in nontreated group at 2 weeks after punch (48.4 vs 37.49 N/mm2, P = 0.0034). (B) The average ultimate failure load of the harvested tendons from the hypoxic MSC-treated group was significantly greater than those in nontreated group at 4 weeks after punch (49.94 vs 36.31 N/mm2, P = 0.0055). (C) There was no significant difference between the average ultimate failure load of the normal tendons, which was 54.98 N/mm2, and the average failure loads of the tendons treated by hypoxic MSCs for 2 and 4 weeks, respectively. MSC: multipotent stromal cell.
Histological Findings
Microstructural and biochemical changes in tendon punch wounds were assessed using the Bonar score.
Under the microscope, tendon sections from the hypoxic MSC-treated group showed more tenocytes (spindle cells) than slides from untreated cells (Fig. 4). At 4 weeks after punching, the scores of the tenocyte (spindle cell) variable were similar in the untreated and hypoxic MSC-treated groups, indicating that there was no significant difference in the maturity of supraspinatus tenocytes between the cell-treated and untreated groups at that time.
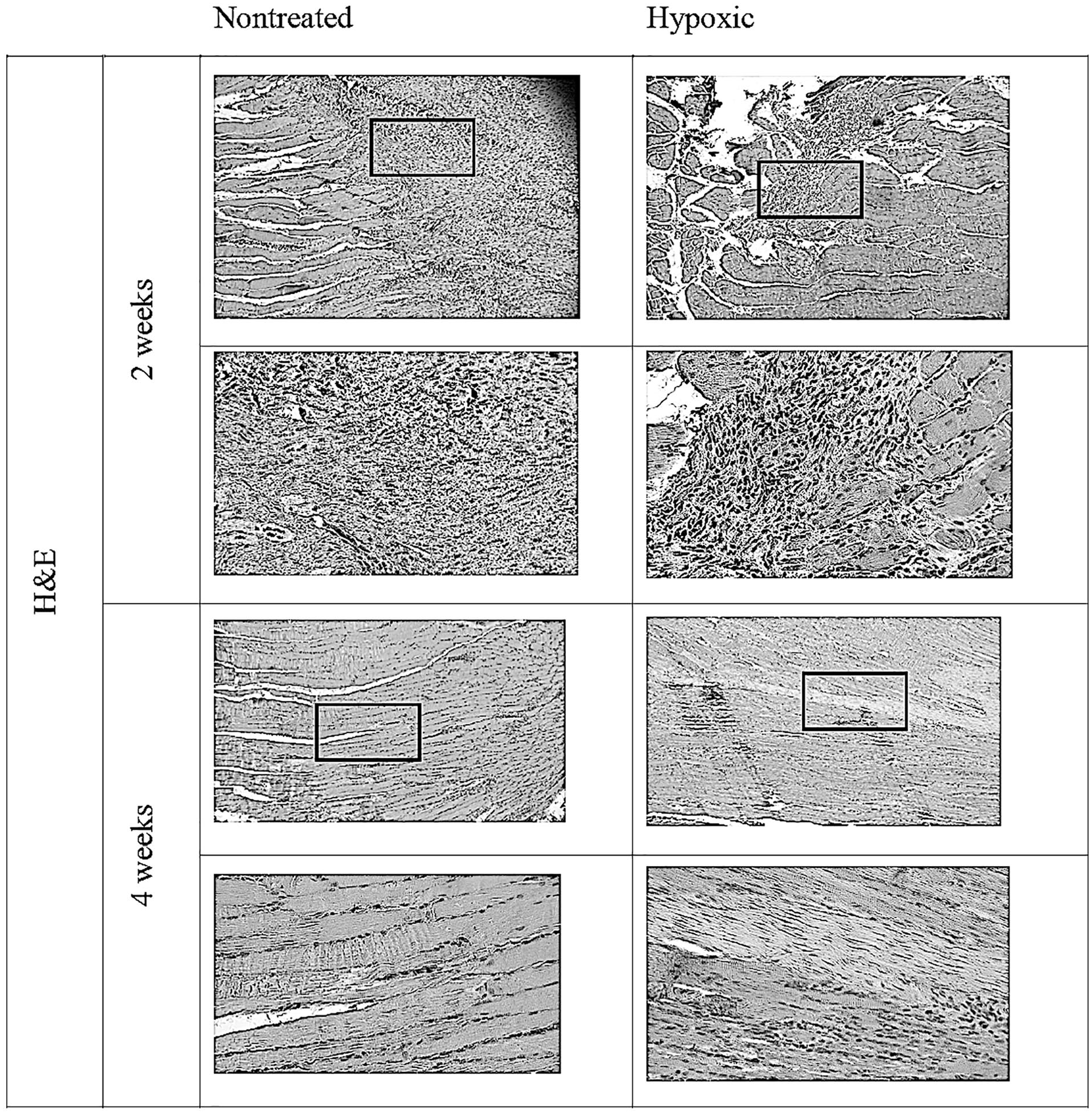
The scores for the tenocyte (spindle cell) variable (for histopathological analysis) at 4 weeks after punch in the control group and hypoxic MSC group. The tendon slides from the cell-treated group showed more spindle cells than the slides from the nontreated group under microscopic examination. MSC: multipotent stromal cell.
For the collagen variable (fibrosis), tendon sections from the hypoxic MSC-treated group showed a more pronounced fibrous separation and chaotic structure under the microscope than the untreated group 2 weeks after punching. Four weeks after punching, more fibrotic tissue was arranged in tightly bound, well-defined bundles in the supraspinatus tendons treated with hypoxic MSCs compared with the untreated group.
At 2 weeks after punching, there were different amounts of ground substances between the untreated and hypoxic MSC-treated groups. Mucin staining was found between bundles, but bundles remained discrete for untreated group 2 weeks after punching. At 4 weeks after punching, lower Bonar scores were observed in the supraspinatus tendons untreated or treated with hypoxic MSCs, approaching healthy Bonar scores, with no significant difference between the two groups (Fig. 5). The scores for the vascular distribution variable were lower in the hypoxic MSC-treated group than in the untreated group 2 weeks after punching, but the scores were at the same level in untreated and hypoxic MSC-treated groups 4 weeks after punching (Fig. 6). The comparison of Bonar scores in the vascular category was statistically significant at 2 weeks after punching (P = 0.0068), while it was not statistically significant at 4 weeks after punching (P = 0.88). At 2 weeks after punching, the total score was statistically significant in both the treatment and control groups (P = 0.007). At 4 weeks after punching, the total score was not statistically significant (P = 0.886; Table 1).

The picture showed the collagen variable (fibrosis, for histopathological analysis) at 2 and 4 weeks after punch in the control group and hypoxic MSC group. The tendon slides from the cell-treated group showed less marked separation of fibers and less chaotic architecture than the slides from the nontreated group under microscopic examination. MSC: multipotent stromal cell.
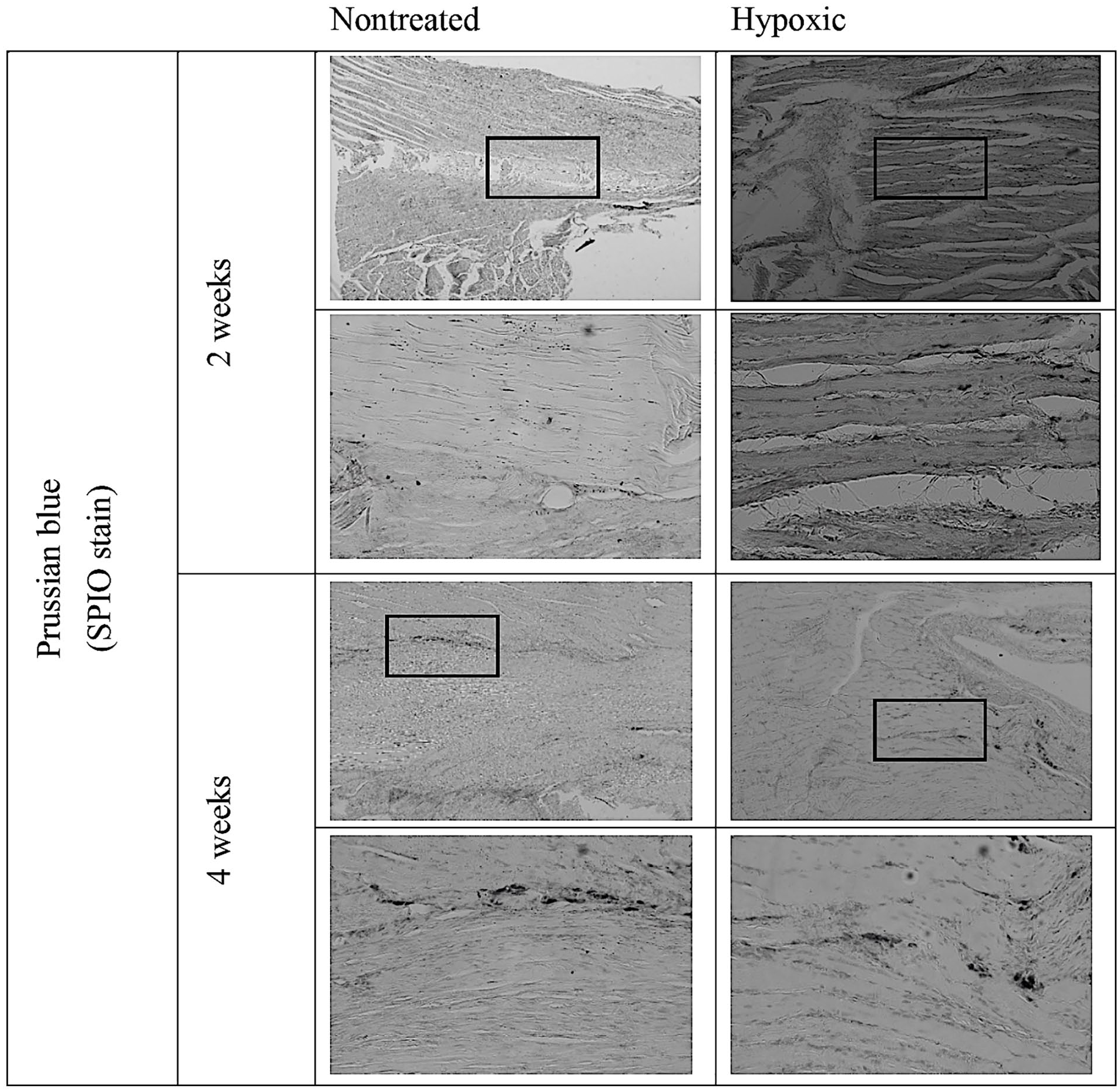
Prussian blue staining revealed the endocytosis activities of the MSCs as SPIO-labeled cells migrated into the punch area of the supraspinatus tendon at 4 weeks after MSC injection. MSCs: multipotent stromal cells; SPIO: superparamagnetic iron oxide.
The Bonar Score System Was Used to Determine the Degree of Tendon Tissue Damage by Measuring Tendon Tissue Condition Under Four Categories: “Tenocyte Morphology/Proliferation,” “Ground Substance,” “Collagen Bundle Characteristics,” and “Vascularity.”

The best condition for each item was 0 and the worst condition was 3; therefore, the total score was 0 for the best condition and 12 for the worst condition. The results showed that there was a significant reduction (improvement) in the Bonar scores of the ruptured tendons after 2 or 4 weeks of hypoxic MSC treatment. MSCs: multipotent stromal cells; ANOVA: analysis of variance.
Values are expressed as mean ± standard deviation. 0 = best score and 3 = worst score.
P < 0.05; **P < 0.01 (two-way ANOVA).
In Vivo Tracking of Hypoxic MSCs Labeled With SPIO
We used the Prussian blue staining to confirm the endocytosis of SPIO nanoparticles by the MSCs. SPIO-labeled MSCs were identified throughout the punch side in vivo (Fig. 6). These findings suggest that SPIO-labeled hypoxic MSCs migrated into the punch area of the supraspinatus tendon and engrafted into the injured tendon at 4 weeks after transplantation.
Discussion
Often isolated from a variety of connective tissues, mesenchymal stem cells have the ability to self-renewal and differentiate into osteoblasts, chondrocytes, and adipocytes. They possess multilineage potential and can be expanded in vitro. Studies have indicated that in vitro-induced differentiation of bone marrow MSCs into tendon cells can be achieved by a combination of biophysical, soluble, and extracellular matrix factor modulation29–32. A number of in vivo studies have also indicated that treatment with transplanted MSCs can improve tendon healing for various parts in animal models, including Achilles tendon defects33–37, rotator cuff defects35,38, and patellar tendinitis 39 .
While the biomechanical and histological outcomes for injured tendons treated with MSCs are better than nontreated ones, fewer studies have compared their effects from different culture conditions. Previous studies have shown enhanced tendon healing in Achilles tendons that treated with MSCs cultured under hypoxic compared with those cultured under normoxic conditions 21 . However, no studies used MSCs from hypoxic culture to compare treatment effect with nontreated group on supraspinatus tendon defects. A similar study by Tsai et al. 18 has performed a treatment on bone defect and found increased bone healing capacity with hypoxic MSCs. We aimed at supraspinatus tendon wound in our study, and the results have indicated that MSCs cultured under hypoxic conditions enhanced supraspinatus tendon healing in terms of biomechanical strength and histological findings at 2 weeks. Previous studies have indicated that MSCs increase their multilineage differentiation potential and proliferation capacity both in vivo and in vitro under hypoxic conditions, and explained the characteristics of their expansion 28 .
The underlying mechanism why hypoxic MSC transplantation had better effect in tendon defect healing than nontreated group was not the focus of our investigation, but we have several hypotheses. First, the capacity of MSCs for multidifferentiation is seen improved under hypoxic condition both in vivo and in vitro. We assume the hypoxic condition will also improve the capacity of MSCs to differentiate into tendon tissues 28 . Second, the self-renewal capacity of MSCs is also improved under hypoxic condition. The regeneration of endogenous stem/progenitor cells is enhanced, so the inflammatory response to injury will be suppressed 40 . SPIO labeling was used to trace the MSCs after their transplantation 41 . The SPIO-labeled MSCs were still detectable 4 weeks after their transplantation. The “collagen” and “ground substance” scores of the Bonar-scale-based assessment suggested that the transplanted hypoxic MSCs engrafted and synthesized type I and type III collagens. As collagen is the main structural protein in connective tissue, it can enhance tendon healing. The increased “vascularity” score also suggested the angiogenic capacity of transplanted hypoxic MSCs.
The potential of allogeneic MSCs for disease treatment has been shown in recent years in articular cartilage defects 42 , myocardial infarction 43 , and graft versus host disease 44 . These studies have indicated that allogeneic MSCs, like autologous MSCs, can be a source for regenerative medicine. The current study also implicates the effectiveness of hypoxic MSCs for the healing of supraspinatus tendon in allogeneic recipients, as the outbred animal, SD rat, used in this study has also been used for the investigation of allogeneic transplantation of mesenchymal stem/progenitor cells 45 . A previous study showed that compared with MSCs cultured under normoxic conditions, hypoxic MSCs have the ability in proliferation and differentiation into more tendon tissues in allogeneic recipients with Achilles tendon defects, which indicated the benefits of hypoxic culture when used for allogeneic transplantation 21 .
There are several limitations to this study. First, the method used to induce a rotator cuff tear is a one-step procedure that does not recapitulate what occurs in humans with a combination of intrinsic and extrinsic etiologies 5 . Second, the glue gels used to deliver MSCs in injured sites may have a repairing effect on their own, so an auxiliary role cannot be ruled out, but at least glue gel alone does not improve repair. Finally, a comparison with normoxic MSCs can be added even though the superior repair capacity of hypoxic MSCs against normoxic MSCs was demonstrated in the Achilles tendon repair study 21 . However, the SD rats at 8 to 10 weeks of age, roughly equivalent to human teenagers, we used for our experiments might not be able to interpret all clinical situations as sports injuries represent only a portion of supraspinatus tendon ruptures while causes related to aging accounted for major reasons as well3,4. Further investigations should be made to study the results and effectiveness for cases of supraspinatus tendon ruptures caused by degeneration. Dosing effects should be further studied as we only applied single dose for MSC transplantation.
In conclusion, this study found that under hypoxic conditions, the repair effect of MSC-treated supraspinatus tendon tears was better than that of the untreated group. This study can lay a foundation for future cell therapy in the repair of the supraspinatus tendon and has clinical implications for the use of hypoxic mesenchymal stem cells for the treatment of supraspinatus tendon defects.
Footnotes
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Human and Animal Rights
All animal experiments were approved by the China Medical University Committee for the Use and Care of Animals (No. 104-131-N).
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Ministry of Science and Technology (MOST 109-2321-B-039-003), China Medical University (CMU110-Z-05), and China Medical University Hospital (DMR-108-BC-5). The funding sources had no involvement in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.