
Abstract
Bioartificial organ manufacturing technologies are a series of enabling techniques that can be used to produce human organs based on bionic principles. During the last ten years, significant progress has been achieved in the development of various organ manufacturing technologies. According to the degree of automation, organ manufacturing technologies can be divided into three main groups: (1) fully automated; (2) semi-automated; (3) handworked (or handmade); each has the advantages and disadvantages for bioartificial organ manufacturing. One of the most promising bioartificial organ manufacturing technologies is to use combined multi-nozzle three-dimensional printing techniques to automatically assemble personal cells along with other biomaterials to build exclusive organ substitutes for defective/failed human organs. This is the first time that advanced bioartificial organ manufacturing technologies have been reviewed. These technologies hold the promise to greatly improve the quality of health and average lifespan of human beings in the near future.
Keywords
Introduction
Organ failure is the leading cause of mortality all over the world despite advances in interventional, pharmacological, and surgical therapies 1 –3 . Bioartificial organ manufacture has been a long-term dream since then beyond the memory of man 4 –6 . Throughout history, people have tried many ways to prolong life through substitution or restoration of defective/failed organs. Currently, orthotopic organ transplantation is the only effective way to achieve this; however, it is seriously limited by issues such as donor shortage, high price, immune rejection and ethical conflict 7 –9 .
With rapid developments in science and technology, some advanced material processing technologies, such as multi-nozzle rapid prototyping (MNRP), additive combined molding (or additive combined molds), decellularized matrix regeneration, electrophoresis, and magnetic adsorption of cells have emerged, making the area of bioartificial organ manufacturing more and more attractive 10 –12 . A common feature of advanced organ manufacturing technologies is that they have the capacity to integrate heterogeneous cell types and multiple materials to recapitulate native organ geometries, constituents and functions 13 –15 . How to assemble heterogeneous living cells with predesigned architectures, including hierarchical vascular, neural and/or lymphatic networks, while ensuring that the corresponding functionality is realized, is one of the main concerns of bioartificial organ manufacturing technologies.
Generally, an artificial organ is an engineered device that can be implanted or integrated into a human body—interfacing with living tissue—to replace a natural organ, to duplicate or augment a specific function or functions so the patient may return to a normal life as soon as possible 16 . According to the materials used, artificial organs can be divided into three main classes: (1) mechanical, made of inanimate polymers (i.e., plastics) and/or metals; (2) biomechanical, made of partially living cells and inanimate polymers and/or metals; and (3) biological (i.e., bioartificial), made of living cells, biodegradable polymers and/or metal elements. Normally, the former two classes can only partially and temporarily replace and repair the failed organs in the human body, while the biological class can totally and permanently restore defective/failed organs. In this article, only biological (or bioartificial) organ manufacturing technologies are reviewed.
Definition of Organ Manufacturing
Through the whole of history, “manufacture” is a very old and prevalent concept that can reflect the rise and decline of a nation, a country, or even an era. The concept of manufacture is defined as “to make a good with tools and/or machines by effecting chemical, mechanical, or physical transformation of materials, substances, or components, or by simulating natural processes, usually repeatedly and on a large scale with a division of labor 17 .”
Thus, the concept of manufacturing is “the production of merchandise for use or sale using labour, machines, tools, and/or chemical and biological changes.” It is closely connected with engineering, industrial design, and changes in material properties 18 . Processes without any changes to the physical, chemical, or biological properties of the starting materials can only be called fabrication or machining. Manufacturing occurs under all types of economic systems, and manufactured items are presented as being different from other similar goods in one or more aspects under a particular brand name. Modern manufacturing, in particular, includes various intermediate processes required for the production and integration of a product’s components.
In a broad sense, organ manufacturing is any procedure that can produce organ substitutes (i.e., artificial organs) using any available materials, such as polymers, cells, metals, etc. In a narrow sense, organ manufacturing is any procedure that can produce bioartificial organs mimicking their counterparts' structures, components and functions. Thus, organ manufacturing can be defined as “to produce bioartificial organs using living cells (such as multiple adult cells and stem cells), along with other biomaterials (such as polymers, growth factors, bioactive agents or biochemical signals), and some advanced processing technologies.’ As with building a nuclear power plant, organ manufacturing is a dynamic transformation process that possesses the basic characteristics of life, with a series of physical, chemical and biological changes of the cell-based biomaterials 1 –6 . Correspondingly, organ manufacturing technologies are a series of enabling techniques that can produce bioartificial organs based on bionic principles 19 –27 . They cover the physical, chemical, biological, and/or/even physiological, pathological clinical transformations of multiple biomaterials, including cells, cell-laden polymeric hydrogels and bioactive agents. One of the main objectives of organ manufacturing technologies is to produce bioartificial organs to partly or totally repair/restore failed/defective native organs. One of the distinctive features of organ manufacturing is that its products are living entities that containing at least two heterogeneous cell/tissue types.
The concept of organ manufacturing was first put forward in 2003 with the establishment of the Center of Organ Manufacturing, in the Department of Mechanical Engineering, Tsinghua University 28 –38 . Since then, more and more research articles have been published, accompanying with a series of invited reviews (Fig 1). It the meantime, plenty of unique advanced technologies, theories, and practical protocols for organ manufacturing have been developed 1 –6 . Various organ precursors, such as vascularized adipose tissues, innervated/vascularized liver tissues, and multifunctional osseous tissues, have been created successfully. Different from tissue engineering, organ manufacturing has its own connotations.

A schematic description of several pioneered 3D bioprinters made in Tsinghua University, Prof. Wang’s laboratory: (A) hepatocytes and/or adipose-derived stem cells (ADSCs) in the gelatin based hydrogels were first printed into large scale-up tissues in 2004 using the single-nozzle 3D bioprinter 23 ; (B) two cell types in the gelatin-based hydrogels were printed simultaneously into large scale-up organs in 2007 24 ; (C) both cells containing natural gelatin-based hydrogel and synthetic polymer systems were printed into large scaled-up vascularized organs with a branched vascular template, which can be sutured to the host vasculatures, using the home-made double-nozzle low-temperature deposition manufacturing (DLDM) system (i.e., DLDM 3D bioprinter). An elliptical hybrid hierarchical polyurethane and cell/hydrogel construct was produced using the DLDM 3D bioprinter 26 ; (D) a schematic description of the modeling and manufacturing processes of four liver constructs with a four-nozzle low-temperature 3D bioprinter 5 .
It is commonly accepted that organ manufacturing is a branch of traditional manufacturing that is associated directly with human organs. It is an interdisciplinary field consisting of an array of scientific technologies, such as biology (especially stem cells), materials, chemistry, physics, informatics, mechanics, computing, surgery, and medicine. Advanced processing technologies for heterogeneous cell/extracellular matrix (ECM)/growth factor assembling are pivotal to successful organ manufacturing. The advanced organ manufacturing technologies for heterogeneous cell/ECM/growth factor assembly have close inter-relationships with many modern sciences and technologies, such as stem cell science and controlling, materials science and processing, tissue science and engineering, nano science and manipulating, drug science and screening, metabolism science and remolding, organ science and building (e.g. individualized or customized organ constructing).
It is realized that the simplest and most direct approach to organ manufacturing is to mimic the natural counterpart with respect to structure (including architecture), component and function. Nevertheless, building valid bioartificial organs requires not only precise control over multiple heterogeneous cell types and material components, but a detailed understanding of the human body’s fundamental intricate response to all environmental factors. Sometimes, physiological functions can be realized through different available materials.
Material Basis of Organ Manufacturing
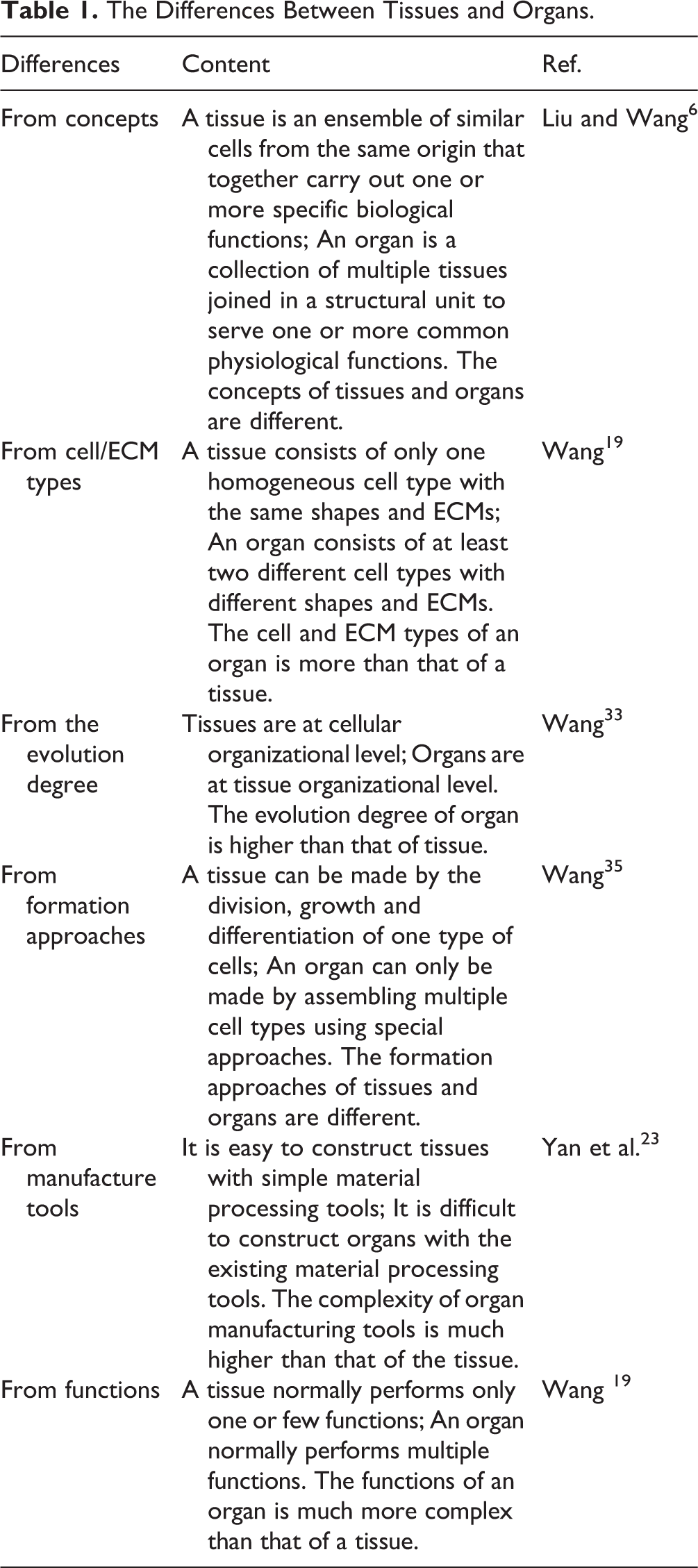
All complicated living phenomena in the world, including organs, are the outcome of physical, chemical or biophysical, biochemical changes. Small organic and inorganic molecules polymerize or combine to form large polymers or compounds. Large polymers and compounds then aggregate to form cells with organelles inside the cell membrane. The cell is the basic unit of life. It is also the basic structural and functional unit of the human body. Tissues are made of homogeneous cells/ECMs, while organs are made of heterogeneous cell/ECM types. Cells, tissues, and organs are different forms (degrees or levels) of materials existing in human body.
For example, an artery can be regarded as a special organ since it is generally comprised of three layers in its tubular wall with three major cell/tissue types (Fig 2): (1) the innermost thin tunica intimal layer made of endothelial cells (i.e., endothelium) and basal lamina, consisting of mainly type IV collagen and laminin, with the main functions of anticoagulant of the blood, and anti-infection/anti-inflammation of the surrounding tissues; (2) the middle thick tunica medial layer made of smooth muscle cells (i.e., muscular layer) arranged circumferentially around the vessel (i.e., vascular wall), type I, III collagen, elastin and proteoglycan, with the main function of mechanical support, such as anti-pulse or anti-stress; (3) the outermost loose tunica adventitial (or external) layer made of fibroblasts, longitudinal collagens, and elastic fibers, with the main function of anchoring the blood vessel to the surrounding tissues and provision of additional mechanical support 39 . Each of these layers plays an important role in transporting nutrients, oxygen, and metabolic wastes, and in maintenance of homeostasis

Diagram of an artery 39 .
The anatomical structures and compositions of artery tissues correspond closely to their biochemical and physiological functions. Unlike tunica adventitia, all the ECMs of the tunica intima and media, such as collagen, laminin, elastin, and proteoglycan, are synthesized by smooth muscle cells. The topological arrangement of the thick type I and III collagen in the tunica media make the middle layer strong enough to withstand blood flow and pressure. In a healthy artery, once the old terminal differentiated cells, such as the endothelial cells, smooth muscle cells, and fibroblasts, in the three tubular layers die, new cells coming from blood stem cells or mesenchymal stem cells (MSCs) will replenish them and fill in each of the three layers. The complexity of the cell/tissue types, ECM components, and topological arrangements of the constituents in the organ determine the difficulty level of organ manufacturing technologies.
During the development stages of a human body, the great variety of human cell types develops from a single fertilized egg, a process that is governed by regulatory networks controlling the required genetic programs. Different tissues combine to form organs. For a typical tissue, the cell and ECM types are the same. In an typical organ, the cell and ECM types are very different. An organ consists of at least two or three different cell/ECM types with certain morphological characteristics and physiological functions. The differences of tissues and organs are summarized into Table 1. With the help of enzymes biochemical reactions in the human body are so quick and mild that we cannot sense them in most cases. Though cells, tissues, organs, and systems in the human body are at different complexity degrees (or levels), they are all based on the combinations of organic and inorganic materials. In particular, organs can be manufactured through assembling different cell types or stem cells/growth factors along with other biomaterials 1 –6 . Stem cells need to be controlled as they differentiate into different cell types before the formation of heterogeneous tissues. Two stem cell engagement strategies have been developed in our former studies. One of them is to mix growth factors in the cell-laden polymeric hydrogels before three-dimensional (3D) printing. The other is to add growth factors in the culture medium after 3D printing. The later is termed as “cocktail stem cell engagement”, in which different growth factor combinations are added into the culture medium in chronological order 28 –38 . Homogeneous tissue forms with the same growth factor incorporation, while heterogeneous tissue forms with different growth factor combinations. Temporal and spatial effects are necessary for multiple tissue formation in a specific 3D construct. Both natural and synthetic polymers are essential for producing branched vascular, neural and/or lymphatic networks with anti-suture capabilities.
The Differences Between Tissues and Organs.
Organ Manufacturing Process
Ordinarily, there are four basic steps for an organ manufacturing process (Fig 3): (1) architectural predesign; (2) preparation of materials and construction tools; (3) homogeneous/heterogeneous cell assembling (or integration); (4) post multi-tissue maturation. For the fully automated MNRP and partially automated additive combined molding technologies, computer-aided design (CAD) modeling can be used for the architectural predesign to create a blueprint, while for manual cell seeding and perfusable decellularized organ regeneration technologies, the architectural predesign stages can be omitted when the organ’s original architecture is used. During the construction or building stages, the construction tools play a key role in recapitulating the micro, meso, and macro (i.e., multi-scale) cell survival environments, the integration of homogeneous and heterogeneous cell types, and the realization of multi-tissue functionalities 1 –6 .

Typical processes for organ manufacturing technologies: multi-nozzle rapid prototyping (MNRP), additive combined molding, and decellularization matrix regeneration.
As with building a nuclear power plant, a blueprint is necessary during the architectural predesign stage. Materials, such as different types of cells or stem cells with different growth factors, and construction tools are essential for the material/tool preparation stage. Cells from the individual patient, including adult cells and stem cells, are preferred to overcome immune rejection issues. Stem cell/ECM/growth factor assembling is a promising approach during the third homogeneous/heterogeneous cell assembling stage. Some MSCs, such as the adipose-derived stem cells (ADSCs), bone marrow mesenchymal stem cells (BMSCs), and umbilical cord blood stem cells (UBSCs), have become more and more popular in the organ manufacturing fields. Growth factors, such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor (b-FGF), are essential for vascular endothelium formation, while hepatocyte growth factor (HGF), human platelet-derived growth factor (PDGF-BB), and transforming growth factor β1 (TGF-β1) are essential for tunica media generation. These growth factors are therefore very important for any complex organ manufacturing involving incorporation of a branched vascular/neural/lymphatic network incorporation. Among all the effective enabling organ manufacturing technologies, MNRP and additive combined molding have offered great benefit in the following homogeneous/heterogeneous cell arrangement and hierarchical vascular/neural/lymphatic network integration stage.
Emphasis should be given to the post multi-tissue maturation stage. During the post multi-tissue maturation stage, the assembled 3D constructs containing homogeneous/heterogeneous living cells need to be stable for in vitro culture or in vivo implantation. Physical, chemical and/or biochemical crosslinking of the supportive polymers are usually necessary to immobilize the living cells and to improve the structural stability 28 –38 . Within the 3D construct, homogeneous and heterogeneous cell aggregation takes place to form homocellular and heterocellular tissues with the spatially and temporarily mechanical support of the crosslinked polymers. Thus, post multi-tissue maturation is a self-finishing process in which homogeneous or heterogeneous cell populations contact and coalesce to form coherent functional tissues. It is a continuous, materially changing, process that can provide living cells with multi-directional environmental signal, including biophysical (e.g., mechanical)/biochemical (e.g., enzymic) even physiological (e.g., potential of hydrogen, PH)/pathological (e.g., viral), stimulation. Only through multiple tissue formation, maturation and coordination, can a bioartificial organ with a whole spectrum of physiological functions be realized. For a solid organ with more than three cell types, such as the liver, heart or kidney, multiple gradient time and space factors need to be considered sufficiently.
During the multi-tissue maturation stage, stem cells can also be engaged into different cell/tissue types using a cocktail induction procedure. For example, ADSCs in a 3D printed construct have been induced effectively into various cell/tissue types, such as endothelial cells/tissues, adipose cells/tissues, smooth muscle cells/tissues and fibrocytes/tissues, under the guidance of sequential growth factor signals applied to the culture medium 28 –38 .
Thus, a typical organ manufacturing process can be described as follows: (1) like building a nuclear power plant, the manufacturing process is a dynamic transformation process, but in this case, containing the basic characteristics of life, with a series of changes in the physical/chemical/physiological properties of the starting materials; (2) advance processing technologies play a key role in the architectural predesign, homogeneous/heterogeneous cell integration, and multi-tissue formation, maturation and coordination stages; (3) stem cell engagement is benefitial for multi-tissue formation, maturation and coordination with respect to the limited cell resource, amount, and type; (4) both natural and synthetic polymers are useful in producing a branched vascular/neural/lymphatic network with anti-suture capabilities; (5) the generation of a hierarchical multi-scale vascular/neural/lymphatic network is critical to successful vascularized bioartificial organ manufacture with a whole spectrum of physiological functions.
Remarkable Events of Organ Manufacturing Technology
In 2000, solid freeform manufacturing (SFM), also known as rapid prototyping (RP) technologies began to be employed in tissue engineering areas for porous scaffold manufacturing. Later in 2010 and 2014, the related technologies were named as additive manufacturing (AM) and 3D printing, respectively. AM (i.e. SFM or RP) is a process in which material is added and joined typically on a layer-by-layer basis to make products using digital data from a 3D model, contrary to subtractive manufacturing and formative manufacturing methodologies 40 –48 . Meanwhile CAD models have since been introduced. Nevertheless, most 3D printed structures are porous tissue repair scaffolds with no living cells inside. Though the porous scaffolds can be seeded with cells before being implanted, they are not the ideal products for organ repair/restoration/regeneration. It is essentially a traditional tissue engineering protocol, which cannot satisfy the basic requirements for many different tissues co-exist in an elaborate 3D structure for one or more common physiological functions.
As stated above, the first “Organ Manufacturing” center was set up in Tsinghua University in 2003, accompanied by the creation of several series of automatic and half-automatic bioartificial organ manufacturing technologies. Its range and content are much broader than those of traditional tissue engineering strategies.
In 2008, Macchiarini and coworkers made a recellularized tracheal substitute through recolonization of a decellularized matrix with epithelial cells and mesenchymal stem-cell-derived chondrocytes 49,50 . The tracheal substitute was then used to replace the recipient’s left main bronchus with a functional airway. The findings prove that autologous cells combined with appropriate biomaterials can provide successful treatment for patients with serious organ disorders.
In 2009, a large scaled-up vascularized adipose tissue was made in Tsinghua University using our home-made 3D bioprinter 30,31 . After the ADSC-laden gelatin/alginate/fibrinogen was printed into large scaled-up lattice structures, cocktail growth factor combinations (i.e., 1 mmol/L insulin, 10 ng/mL VEGF, and 50 μg/mL aprotinin for endothelization of the ADSCs; 1 mmol/L insulin, 1 mmol/L dexamethasone, 0.5 mmol/L isobutylmethylxanthine, and 50 μg/mL aprotinin to induce ADSCs to form adipose cells) were sequentially added to the culture medium to induce the ADSCs into vascular endothelial cells and adipose cells, respectively. Aided by spatial effects, ADSCs in the gelatin-based hydrogel can fully differentiate into different tissues (e.g., endothelial tissues and adipose tissues) in the 3D constructs. This was the first time that a large-scale vascularized solid organ was manufactured automatically. With this technology, various large-scale vascularized solid organs have now been produced.
Despite these successes, little to no advanced technology is currently available to totally duplicate a natural organ both in architectural structures and physiological functions with high fidelity. Each of the existing technologies, no matter whether fully automated, semi-automated or handmade, has some technical bottlenecks that are hard to overcome. For example, it is hard to make all the disparate networks, such as vascular, neural, lymphatic and biliary, with one single organ manufacturing technology. Several combined technologies including MNRP, additive combined molding, and decellularized matrix regeneration, are attracting more and more attention. A main characteristic of these technologies is that they are capable of creating gradual structures with multiple cell types, heterogeneous polymeric hydrogels, as well as bioactive agents. These gradual structures can be integrated into an organic entity under the guidance of a prescribed CAD model.
Classification of Organ Manufacturing Technologies
Traditionally, there are several different types of artificial organs. According to the materials used, these artificial organs can be divided into three classes: mechanical, biomechanical, and biological. To date, the former two classes can only partially and temporarily replace and repair failed organs in the body, while biological artificial (i.e., bioartificial) organs can totally and permanently replace and cure failed organs.
According to the traditional manufacturing processes, bioartificial organ manufacturing technologies can be sorted into three basic classes: (1) fully automated, such as AM, RP, or 3D bioprinting 51 –55 ; (2) semi-automated, such as rotational combined mold system, involving mechanical handling (i.e., mechanized operation) steps 26,36 ; (3) hand-manipulated, such as the layered biomaterial casting, cell sheet overlapping, and decellularized organ regeneration 29,30 .
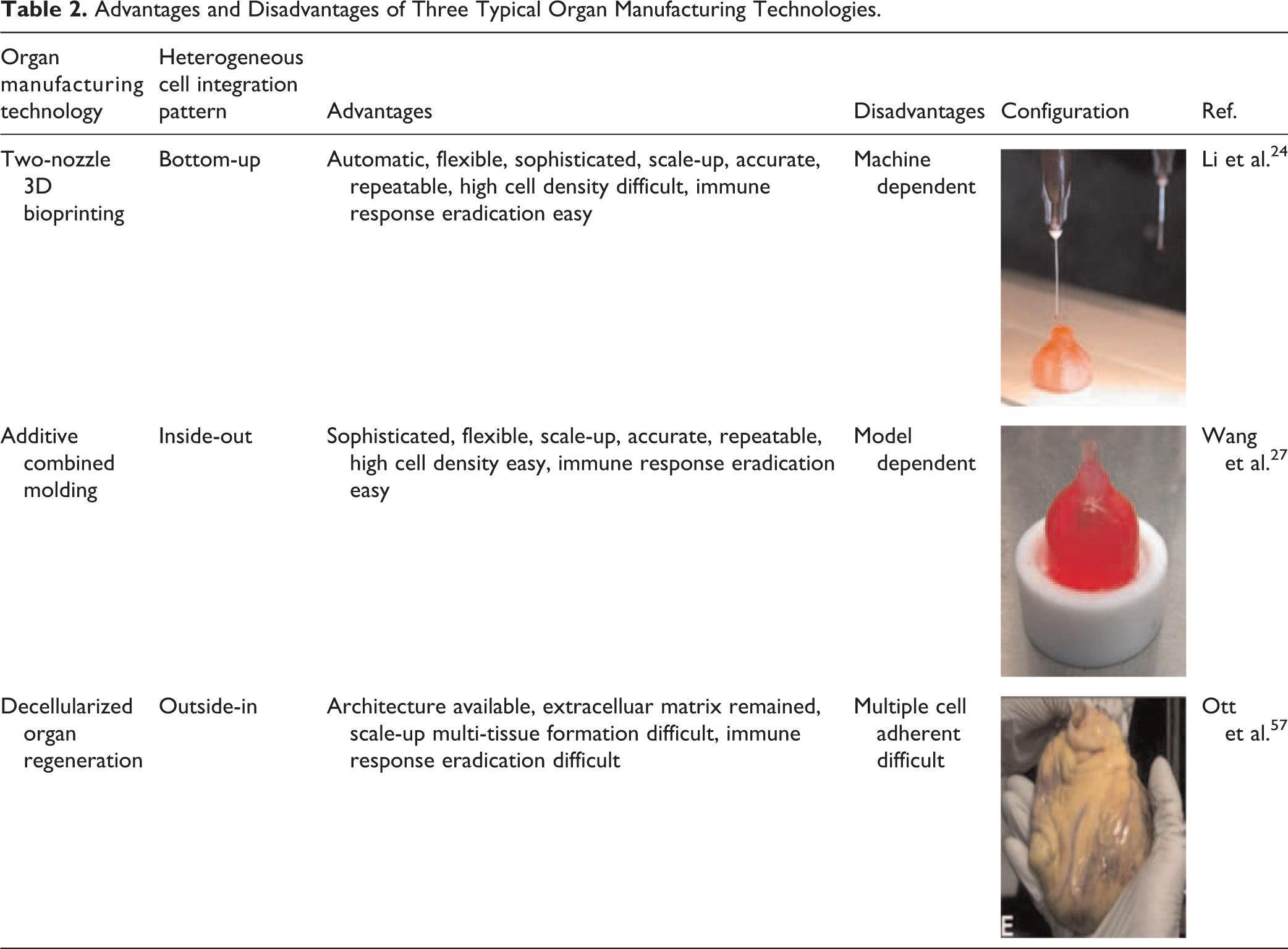
Depending on the processing mechanism, bioartificial organ manufacturing technologies can also be classified into several patterns: (1) bottom-up engineering technologies capable of integrating multiple homogeneous/heterogeneous cells in a bottom-up layer-by-layer deposition manner 56 –59 , e.g., MNRP is a typical fully automated bottom-up engineering approach employing sophisticated 3D printing. (2) Inside-out engineering technologies capable of integrating multiple homogeneous/heterogeneous cells in an inside-out, layer-by-layer increasing manner. Additive combined molding is a typical semi-automated inside-out engineering technique regarding to the predefined scale-up molds 26,36 . (3) Outside-in engineering technologies capable of integrating homogeneous/heterogeneous cells in an outside-in layer-by-layer attachment manner; decellularized organ regeneration is a typical hand-manipulated outside-in engineering protocol involving heterocellular adhesion on the preserved vascular networks 60 –63 .
During the last decade, all three classes (i.e. automated, semi-automated, and hand manipulated) of organ manufacturing technologies have developed very quickly. Some specific MNRP, additive combined molding and decellularized organ regeneration techniques have been extended rapidly, with substantial progress in the field of manufacturing certain complicated organs, such as the liver, heart, lung, and bone. Theoretically, these technologies hold extraordinary versatility in creating any organ in the human body, especially for those complex organs containing more than three cell types and multi-scale hierarchical vascular/neural/lymphatic and nerve networks. Currently, each of the fully automated, semi-automated, and hand-manipulated organ manufacturing technologies has its own limitations in creating bioartificial organs mimicking native counterparts in both physical structures and physiological functions. The advantages and disadvantages of MNRP, additive combined molding and decellularized matrix in producing organ substitutes are summarized in Table 2. Despite the great benefits and flexibility of these technologies in creating complex organs, these technologies currently still face some obvious limitations in producing organ substitutes with a whole spectrum of native organ functions.
Advantages and Disadvantages of Three Typical Organ Manufacturing Technologies.
For example, in 2013, a hybrid hierarchical polyurethane (PU)-cell/hydrogel construct (i.e., an elliptical bioartificial liver precursor), with a branched vascular network made of ADSC/hydrogel and PU overcoat, was first created in my laboratory using a double-nozzle low-temperature 3D bioprinter 25 . It is necessary to connect the two half-ellipses and let the blood capillaries form by the sandwiched cells/hydrogels themselves. This is a typical fully automated organ manufacturing technology (e.g., MNRP) technology, and the practice protocol has proven very popular in some pertinent research areas, such as high-throughput drug screening, energy metabolism model establishment, and 3D stem cell engagement. Despite its great flexibility in 3D printing of heterogeneous materials, this technology currently faces limitations in printing anatomical multi-scale vascular networks, especially capillary blood vessels 64 –69 . The major advantage of the hand-manipulated decellularized matrix regeneration approach over other organ construction technologies is that the acellular organs preserve the 3D architectures and the natural ECM components of native organs, which are critical for the later cell perfusion and adhesion. However, it is extremely difficult for this technology to regain the multicellular contents of the natural counterpart, as well as full endothelialization of branched vascular networks.
One of the roles of bioartificial organ manufacturing is to create a fully functional, multicellular organ substitute that can thrive within a human body to restore, repair or regenerate the failed organs. The first edition of our book “Organ Manufacturing” was published by the Nova Science Publishers Inc, NY, USA in August, 2015 1 , symbolizing that human beings have entered a brand new era in which every failed organ can be restored by a similar substitute. The average life span will be drastically elongated and quality of health will improve dramatically in the near future.
Advanced Organ Manufacturing Technologies
During the last several years, a wide variety of organ manufacturing technologies have been exploited. These technologies include fully automated MNRP, partially automated additive combined molding, manual coculture cells on porous scaffolds (i.e., traditional tissue engineering), and decellularized matrix regeneration 70 –73 . Some other technologies, such as electrophoresis and magnetic adsorption of cells or nanocomposite cell-laden hydrogels have been used for spatially and temporally controlling heterogeneous cell arrangement 74 – 78 .
Nevertheless, all the technical bottleneck problems encountered in biomaterials, cell therapy, tissue engineering, drug screening and other regenerative medicine areas for more than several decades, have been gradually surmounted in my own laboratory with the profound scientific and technological backgrounds, pioneering works, and landmark breakthroughs 1 –6,28 –38 . For example, the first real 3D cell-laden latticed structure was created by our home-made one-nozzle 3D bioprinter1-6. Heterogeneous cell types were assembled into an organic entity with a branch vascular network using our home-made double-nozzle 3D bioprinter 28 –38 . Hybrid cell-laden natural and synthetic polymeric hydrogels were fabricated into intricate architectures with controlled go-through channels and branched vascular networks using our home-made double-nozzle low-temperature 3D bioprinter, in which cells could be long-term preserved under minus 80°C when cryoprotectant, such as dimethyl sulfoxide (DMSO), glycerol, or dextran-40, was added in the natural polymeric hydrogels 28 –38 . A fully perfusable vascular network, including arteries, arterioles, veins, venules, and capillaries, with a tight, confluent endothelium lining, was established 31 –35 . Most outstandingly, the creation of the scale-up hierarchical vascular network is a long-awaited dream either in the fields of both tissue engineering and regenerative medicine.
The half-automated additive combined molding technologies have paved the way to developing a multi-scale vascular network comprising an anti-suture overcoat with anastomosis capability, large blood vessels with a hierarchical arrangement of multiple cell types, small vasculature structures with circular cross-sections, and fully contiguous endothelium lining capillaries. It is also the first man-made perfusable vascular network, including arteries, arterioles, veins, venules, and capillaries 79 –88 . The inner surface of the vasculature was covered by tight, confluent endothelium alignment, clearly representing a long-awaited breakthrough in vascularized solid organ manufacturing over the last several decades.
In 2014, an implantable elliptic liver tissue with both vascular and neural networks in a synthetic polymer poly(lactic-co-glycolic acid) (PLGA) encapsulated ADSC/fibrinogen and hepatocyte construct was manufactured using a combined four-nozzle 3D bioprinter (Fig 4) 35 . This is another fully automated organ manufacturing technology. With this technology, the concentration of cell-containing hydrogels can be greatly decreased, or even omitted. ADSCs in the construct were engaged into endothelial cells and hepatocytes through two approaches: one by incorporating growth factors inside the cell-laden hydrogels, the other applying a cocktail of growth factor as described above. A complete perfusable hierarchical vascular network, including arteries, arterioles, veins, venules, and capillaries, was created with the company of a branched neural network. The synthetic PLGA was used as an overcoat to protect the cells/hydrogels from being washed out or swallowed up by bodily fluids and phagocytic cells. The PLGA-coated cell/hydrogel construct can be connected with the body blood vessels with anti-suture and anti-pressure capabilities. This is another hugely important milestone in complex bioartificial organ manufacturing.

A combined four-nozzle organ 3D bioprinting technology: (A) equipment of the combined four-nozzle organ 3D bioprinter; (B) working state of the combined four-nozzle organ 3D printer; (C) a computer aided design (CAD) model; (D) a 3D construct containing a poly (lactic acid-co-glycolic acid) (PLGA) overcoat, a hepatic tissue (i.e. hepatocytes in the gelatin/chitosan hydrogel), vascular (i.e. endothelialized ADSCs on the gelatin/alginate/fibrin hydrogel) and neural (i.e. fibrous Shwann cells in the gelatin/hyaluronate hydrogel) networks; (E) a cross section of (D), showing endothelialized ADSCs and Schwann cells around a branched channel; (F) a picture showing a thick nerve fiber formed in (D); (G) a picture showing the hepatocytes underneath the PLGA overcoat; (H) an interface between the endothelialized ADSCs and Schwann cells in (D); (I) a picture showing the thin nervous fibers.
Among the advanced technologies, MNRP and additive combined molding hold the greatest potential for integrating multiple materials with special structures, such as hierarchical vascular, neural, lymphatic and biliary networks 83 –88 . Generating a perfusable multi-scale hierarchical vascular network is no more one of the most critical challenges in most of the vascularized solid organ manufacturing. CAD techniques can be used in both architecture predesign and scale-up manufacturing stages to accelerate the automated or semi-automated processing procedures and improve processing accuracy. Although at an early stage, the successful implantation of a functional vascular network into mouse has marked the beginning of the automated and semi-automated organ manufacturing era.
Conclusions and Perspectives
Organ manufacturing is an interdisciplinary field that has close inter-relationships with many modern sciences and technologies, such as biology (especially stem cells), material science, chemistry, physics, mechanics, bioinformatics, computing, surgery, and medicine. Advanced technologies for heterogeneous cell/ECM/growth factor assembly are pivotal to successful complex organ manufacturing. The establishment of a scaled-up hierarchical vascular network is vitally important to consistently supply living cells with nutrients and oxygen to maintain their survival and metabolic function. Post multi-tissue maturation is another key factor for homogeneous/heterogeneous tissue formation, maturation, and coordination in a physiological functional organ substitute.
Organ manufacturing technologies can be classified into three major groups: fully automated, semi-automated, and hand manipulated. Advanced organ manufacturing technologies are normally interdependent, allowing mutual improvement during the material processing procedures. For example, combined MNRP technologies make multiple biomaterial integration automated and accurate; additive combined molding makes the perfusable multi-scale vascular network available; stem cells, make the amplification of huge number (i.e., large quantity) of patient-derived cells supply possible; growth factor combinations make sequential stem cell engagement practical; decellularized matrices facilitate the full simulation of native organ architecture facile; and CAD modeling makes the custom-design and reverse organ manufacturing feasible. The combination of these advanced technologies has paved the way to constructing (or developing) physiologically functional bioartificial organs. These organ manufacturing technologies, therefore, hold the promise to greatly improve the quality of health and average lifespan of human beings. The production of physiologically functional bioartificial organs thus heralds an exciting new era.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China (NSFC) (grant numbers 81571832 and 81271665) and the 2017 Discipline Promotion Project of China Medical University (CMU) (grant number 3110117049).