
Abstract
Brain death (BD) is associated with a systemic inflammation leading to worse graft outcomes. This study aimed to compare plasma cytokine values between brain-dead and critically ill patients, including septic and non-septic controls, and evaluate cytokine release kinetics in BD. Sixteen brain-dead and 32 control patients (16 with and 16 without sepsis) were included. Plasma cytokines were measured by magnetic bead assay after the first clinical exam consistent with BD and every 6 hours thereafter, and at the time of study entry in the control group. The values for IL-8 and IFN-γ were higher in brain-dead and septic patients than in non-septic patients [IL-8: 80.3 (18.7–169.6) vs. 68.2 (22.4–359.4) vs. 16.4 (9.2–42.7) pg/mL; P = 0.006; IFN-γ: 2.8 (1.6-6.1) vs. 3.4 (1.2–9.0) vs. 0.5 (0.5–1.8) pg/mL; P = 0.012]. TNF showed a clear tendency to increase in brain-dead patients [2.7 (1.0–4.8) vs. 1.0 (1.0–5.6) vs. 1.0 (1.0–1.0) pg/mL; P = 0.051], and IL-6 values were higher in brain-dead patients than in non-septic controls [174.5 (104.9–692.5) vs. 13.2 (7.3–38.6) pg/mL; P = 0.002]. These differences remained even after excluding brain-dead patients who also had sepsis (n = 3). IL-1β and IL-10 values increased from baseline to time point 2 (∼6 hours later) [IL-1β: 5.39 (1.93–16.89) vs. 7.11 (1.93–29.13) pg/mL; P = 0.012; IL-10: 8.78 (3.62–16.49) vs. 15.73 (5.49–23.98) pg/mL; P = 0.009]. BD-induced and sepsis-induced plasma cytokine values were similarly high, and both were higher than the observed in non-septic critically ill patients.
Background
Brain-dead donors are the main source of organs for transplantation 1,2 . Brain death (BD) causes acute and massive catecholamine release, leading to an inflammatory state characterized by cytokine upregulation 3 . Accumulating evidence suggests that BD-induced inflammatory activity adversely affects graft survival 4 –8 .
Experimentally, renal tubules and glomeruli from rat models of BD have demonstrated increased expression of tumor necrosis factor (TNF), interleukin-1β (IL-1β) and interleukin-6 (IL-6) compared with controls 9 . In line with this, renal biopsies from brain-dead donors have shown higher cytokine values than biopsies from living donors 10,11 . Moreover, kidney grafts from HLA-mismatched living donors have higher survival rates than kidneys from HLA-matched brain-dead donors 12 .
Primary lung graft dysfunction is a common complication of lung transplantation that results from ischemia-reperfusion injury, a process that might also be triggered by the systemic inflammatory state of the donor 13 . A significant increase in interleukin-8 (IL-8) values in bronchoalveolar lavage fluid from brain-dead lung donors has been demonstrated and correlates with early graft dysfunction after lung transplant 7 . In addition, patients who died within 30 days of lung transplant had elevated IL-6 gene expression in biopsies prior to implantation 14 . Interestingly, myocardial TNF mRNA expression during organ retrieval predicted right ventricular dysfunction in heart recipients 15,16 . Furthermore, liver biopsies from brain-dead donors have shown higher CD4 and CD8 infiltration than biopsies from living donors 17 . In a previous study by our group, we observed an increase in IL-6 and TNF plasma values and upregulation of TNF mRNA expression in pancreatic tissue from brain-dead donors compared with control patients undergoing pancreatectomy due to malignant tumors, but the kinetics of cytokine release during BD was not evaluated 18 .
Brain-dead patients suffer a variety of insults, ranging from the lesion that has led to BD to shock, mechanical ventilation, cardiac arrest, and sepsis. All these injuries are frequently observed in other critically ill patients and may also trigger the inflammatory cascade 19 –21 . To date, the contribution of critical illness to BD-associated inflammation has not been investigated. The present study was therefore designed to compare plasma cytokine values from brain-dead patients with those from critically ill patients, including septic and non-septic individuals, and evaluate the cytokine profile following BD in a time-dependent manner.
Materials and Methods
Brain-Dead Patients and Controls
The study protocol was approved by the ethics committee at Hospital de Clínicas de Porto Alegre. Informed consent was obtained from patients or their legal representatives. BD was assessed independently by two physicians and was based on the following criteria: coma with complete unresponsiveness, absence of brainstem reflexes, apnea test, and confirmatory test with absence of cerebral blood flow, according to Brazilian law 22 . From June 2013 to June 2015, brain-dead patients older than 18 years admitted to the intensive care unit (ICU) were prospectively included in the study after the first clinical examination consistent with BD. Controls were defined as critically ill patients without suspected BD admitted to the same ICU. For each brain-dead patient, two control patients were included: the first septic patient to the right and the first non-septic patient to the left of the case’s bed. Sepsis was defined as the presence of infection and organ dysfunction 23 . Blood samples were collected at study entry for all groups. For the BD group, additional blood samples were collected at 6 and 12 hours (h), for a total of three samples per patient. Control patients had blood samples collected only once, at study entry, as we considered that controls would have a steady inflammatory profile. Clinical and laboratory data were recorded for brain-dead and control patients.
Plasma Cytokine Quantification
Blood samples were immediately centrifuged at 1260 units of gravity (g) for 10 min at 4 degrees Celsius (°C) and plasma was stored at −80°C until analysis. All samples were analyzed at the same time after being thawed at room temperature and centrifuged at 1000 g for 10 min. Plasma values of TNF, IL-1β, IL-6, IL-8, interleukin-10 (IL-10), and interferon-γ (IFN-γ) were assessed by magnetic bead assay using the Human Magnetic Custom Luminex® Kit (Invitrogen Life Technologies, Carlsbad, USA) and the Luminex® 200™ magnetic bead plate reader (Luminex, Austin, USA) following the manufacturers’ instructions. A standard curve was generated by serial dilutions of the reconstituted standard. Samples and standards were incubated with mixed beads overnight at room temperature on an orbital shaker. Beads were washed and then incubated with a detection antibody at room temperature for 1 h and with streptavidin for 30 min. Beads were washed and resuspended, and the plate was subsequently analyzed on the Luminex® 200™ reader. The results were plotted as a function of fluorescence intensity. Mean fluorescence intensity (MFI) takes into account the number of fluorescent pixels within the scanned area. MFI values below the detection limit were assumed to be equal to the lowest value detected (0.91 pg/mL for TNF, 1.93 pg/mL for IL-1β, 0.36 pg/mL for IL-6, 2.87 pg/mL for IL-8, 1.17 pg/mL for IL-10, and 0.48 pg/mL for IFN-γ). MFI was then converted to picograms (pg)/mL based on the standard curve. All samples were analyzed in duplicate.
Statistical Analysis
Categorical variables were expressed as percentages. Data were expressed as mean and standard deviation (SD) if normally distributed. Variables with skewed distribution were expressed as median and interquartile range. Groups were compared using one-way analysis of variance with Tukey’s post-hoc test, Kruskal–Wallis test, or chi-square test as appropriate. Plasma cytokine levels from brain-dead patients were compared at different time points using generalized linear models. Sample size for this study was calculated considering a power of 80% and an α-error of 5% to detect a difference of at least one SD in TNF log 18 . Values were considered statistically significant if P<0.05. Statistical analyses were performed using SPSS, version 18.0 (Chicago, IL).
Results
Sixteen brain-dead patients and 32 controls (16 septic and 16 non-septic patients) were included in the study. The baseline characteristics of all patients are shown in Table 1. Stroke was the leading cause of BD (62.5%), followed by anoxic encephalopathy (12.5%). The most common sites of infection in septic patients were the lung (40.0%) and the abdomen (26.6%). Non-septic patients were admitted to the ICU due to pulmonary embolism (20.0%), hemorrhagic stroke (20.0%), cardiac arrest survivors (13.3%), elective cardiac surgery (13.3%), or other causes (33.4%). Age, sex, body mass index and illness severity, assessed by APACHE II score, did not differ significantly between groups. Length of ICU stay and duration of mechanical ventilation were similar between groups. As expected, brain-dead and septic patients required more vasopressor support than non-septic patients, and hypernatremia and hypothermia were more common in brain-dead patients than in both control groups.
Baseline Characteristics of Brain-Dead Patients and Controls.

†BMI: body mass index. §Non-septic control patients are different from brain-dead and septic control patients. ¶Brain-dead and septic control patients and brain-dead and non-septic control patients are different. * Brain-dead and non-septic control patients are different.
BD Induces Inflammation Similar to that Observed in Sepsis
First, we examined the plasma cytokine profile of brain-dead and control patients at study entry (1.4 ± 1.3 h after the first clinical examination consistent with BD) and data are shown in Fig 1. The values of IL-8 were significantly higher in brain-dead and septic patients than in non-septic patients [80.3 (18.7–169.6) vs. 68.2 (22.4–359.4) vs. 16.4 (9.2–42.7) pg/mL; P = 0.006]. Similar findings were obtained for IFN-γ values, which were also higher in brain-dead and septic patients than in non-septic controls [2.8 (1.6–6.1) vs. 3.4 (1.2–9.0) vs. 0.5 (0.5–1.8) pg/mL; P = 0.012]. Regarding IL-6, plasma values were upregulated in brain-dead patients compared with non-septic control patients [174.5 (104.9–692.5) vs. 13.2 (7.3–38.6) pg/mL; P = 0.002], but not compared with septic patients [174.5 (104.9–692.5) vs. 134.7 (7.2–413.6) pg/mL; P = 0.524]. Conversely, there were no differences in IL-1β [5.4 (1.9–16.9) vs. 3.1 (1.9–15.0) vs. 1.9 (1.9–4.0) pg/mL; P = 0.271] and IL-10 values [8.8 (3.6–16.5) vs. 8.5 (4.3–22.9) vs. 3.0 (1.2–16.1) pg/mL; P = 0.185] between brain-dead, septic, and non-septic patients. TNF showed a clear tendency to increase in brain-dead patients compared with the other two groups [2.7 (1.0–4.8) vs. 1.0 (1.0–5.6) vs. 1.0 (1.0–1.0) pg/mL; P = 0.051].

Plasma cytokine values determined by magnetic bead assay in brain-dead patients and controls. A. Tumor necrosis factor (pg/mL). B. Interleukin-1β (pg/mL). C. Interleukin-6 (pg/mL). D. Interleukin-8 (pg/mL). E. Interleukin-10 (pg/mL). F. Interferon-γ (pg/mL). Kruskal–Wallis with pairwise comparison. Statistically significant differences as indicated by the bars (IL-6: P = 0.01 for BD vs. non-septic controls; IL-8: P = 0.029 for BD vs. non-septic controls and P = 0.01 for septic vs. non-septic controls; IFN-γ: P = 0.028 for BD vs. non-septic controls and P = 0.031 for septic vs. non-septic controls). Graphs are plotted on a logarithmic scale, representing median and interquartile range. Dots and asterisks represent outliers.
Influence of Superimposed Sepsis on Cytokine Levels in Brain-Dead Patients
Three brain-dead patients (18.7%) had sepsis, all of pulmonary origin. In order to eliminate this potential confounder, septic brain-dead patients were excluded from the analysis. IL-6 values remained significantly higher in brain-dead patients than in non-septic control patients (P = 0.003), while IFN-γ levels remained higher in brain-dead and septic patients than in non-septic patients (P = 0.011). There were no differences in IL-1β (P = 0.281) and IL-10 (P = 0.213) values between groups. IL-8 values differed only between brain-dead and non-septic patients (P = 0.008). Remarkably, TNF values became significantly higher in brain-dead patients than in non-septic patients (P = 0.025).
Plasma Cytokine Release Kinetics over Time in Brain-Dead Patients
The time course of plasma cytokine levels during BD was then characterized, showing variation over time (Table 2). The levels of IL-1β and IL-10 increased from baseline (1.4 ± 1.3 h; first clinical examination consistent with BD; n = 16) to time point 2 (7 ± 1.2 h; second clinical examination consistent with BD; n = 15), but no significant differences were observed at time point 3 (14.7 ± 2.1 h; at the time of organ retrieval; n = 6). IFN-γ showed a non-significant increase in post-hoc analysis from time point 2 to time point 3 (P = 1.0), probably due to the reduced sample size.
Plasma Cytokines Kinetics in Brain-Dead Patients.
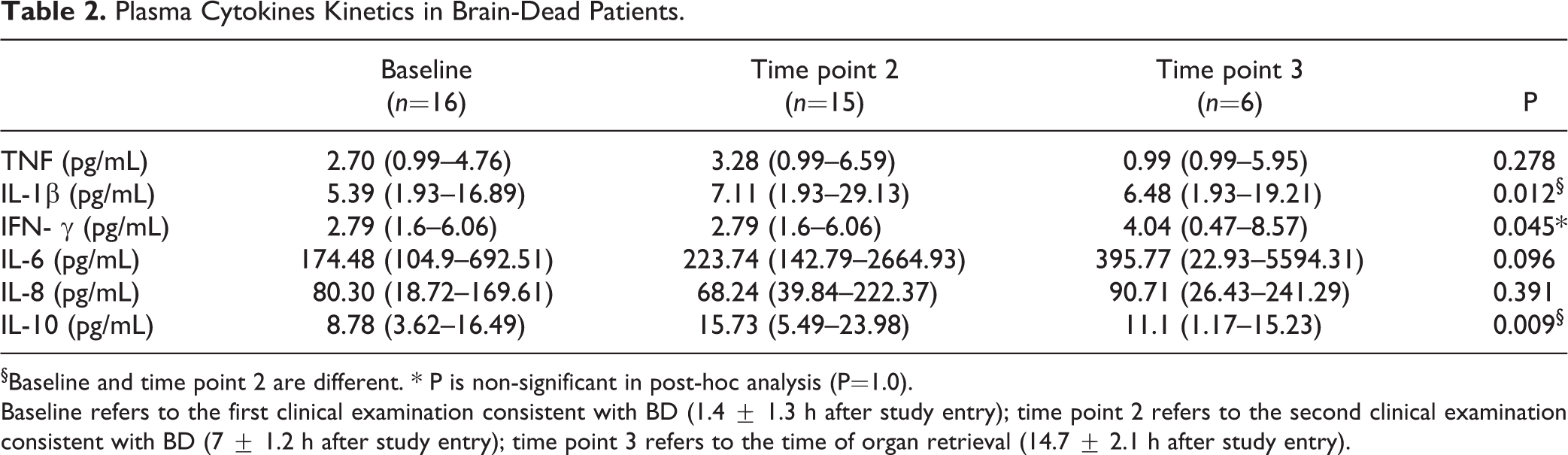
§Baseline and time point 2 are different. * P is non-significant in post-hoc analysis (P = 1.0).
Baseline refers to the first clinical examination consistent with BD (1.4 ± 1.3 h after study entry); time point 2 refers to the second clinical examination consistent with BD (7 ± 1.2 h after study entry); time point 3 refers to the time of organ retrieval (14.7 ± 2.1 h after study entry).
Because cytokines varied during the observation period, we therefore compared plasma cytokine levels between brain-dead patients at time point 2 and the control patients sample at baseline. The results showed that IL-8 and IFN-γ plasma values were significantly higher in brain-dead and septic patients than in non-septic control patients [IL-8: 68.2 (39.8–222.4) vs. 68.2 (22.4–359.4) vs. 16.4 (9.2–42.7) pg/mL; P = 0.003 and IFN-γ: 4.0 (1.8–14.3) vs. 3.4 (1.2–9.0) vs. 0.5 (0.5 -1.8) pg/mL; P = 0.001], similar to the results obtained at the baseline analysis, reported above. IL-6 also showed the same pattern observed at the baseline analysis, with higher values in brain-dead patients at time point 2 than in non-septic control patients [223.7 (142.8–2664.9) vs. 13.2 (7.3–38.6) pg/mL; P = 0.001], but both groups did not differ from the septic group. Notably, IL-10 and TNF values, which were not significantly different at baseline, became higher in brain-dead patients than in non-septic control patients at time point 2 [IL-10: 15.7 (5.5–24.0) vs. 3.0 (1.2–16.1) pg/mL; P = 0.047 and TNF: 3.3 (1.0–6.6) vs. 1.0 (1.0–1.0) pg/mL; P = 0.01]. Plasma IL-1β values were similar in all groups regardless of the time point of measurement.
Discussion
We presently show that BD is associated with higher systemic inflammation than that induced by critical illness without associated sepsis. Interestingly, cytokine values in BD were similar to those observed in sepsis. This is evidenced by upregulation of IL-6, IL-8, IL-10, IFN-γ, and TNF in brain-dead patients. In addition, we demonstrated an elevation in IL-1β and IL-10 values during the course of BD diagnosis.
Sepsis is a clinical syndrome classically associated with increased inflammation, with both pro- and anti-inflammatory cytokine upregulation 24,25 . Increased cytokine release is partially responsible for the clinical manifestations of sepsis and for organ dysfunction 26 . In addition, TNF, IL-6, and IL-10 are associated with organ failure and mortality 27 –30 . Notably, in our study, the systemic inflammation in brain-dead patients was similar to that observed in septic patients. Moreover, even after excluding brain-dead patients with sepsis from the analysis, the two groups remained similar.
Other acute critical illnesses, such as trauma 21 , hemorrhagic shock 31 , and cardiac arrest 32 may manifest as a systemic inflammatory response that contributes to multiple organ dysfunction syndrome. Adrie et al. investigated the inflammatory response of 61 successfully resuscitated out-of-hospital cardiac arrest patients compared with septic patients and healthy controls. Plasma values of IL-6, IL-8, and IL-10 were elevated on admission, with values as high as in patients with severe sepsis, and vasopressor use was associated with increased cytokine release in non-survivors 33 . Mechanical ventilation has also been shown to trigger pulmonary and systemic inflammation with enhanced values of TNF, IL-1β, and IL-6 in plasma and bronchoalveolar lavage even in normal lungs 34 –38 . In our study, cytokines, except for IL-1β, were higher in brain-dead patients than in non-septic control patients, although these two groups of patients did not differ in terms of occurrence of cardiac arrest, disease severity (as assessed by APACHE II score), or duration of mechanical ventilation; however, as expected, brain-dead patients more frequently required vasopressor support. Taken together, these findings suggest that systemic inflammatory response in BD is triggered mainly by BD itself rather than by other injuries that develop during critical illness.
Inflammation secondary to BD is partially responsible for primary graft dysfunction and induced by the innate and adaptive immune systems 39 . Cytokines participate in both responses and are released in reaction to injury and infection, orchestrating the inflammatory response by acting on immune cell differentiation, proliferation, and activity. Increased values of IL-6 have been consistently found in brain-dead patients 6,8,18,40 –42 . Our findings are consistent with the presence of systemic inflammation in BD and shed light on the cytokine profile and kinetics during BD. Interestingly, we identified increased plasma values not only of IL-6 but also of IL-8, IFN-γ, IL-10, and TNF in brain-dead patients compared with critically ill patients without sepsis. IL-10 and TNF values were elevated at time point 2 (around the time of confirmation of BD), which is consistent with the period in which TNF was upregulated in our previous study 18 . However, these results should be interpreted with caution, since these cytokines were similar among groups when baseline results were considered and were statistically elevated in BD patients only at time point 2. The importance of inflammation in transplant outcomes has been demonstrated in a recent study by our group 43 . In an experimental model of BD, rats treated with exendin-4, a glucagon-like peptide-1 (GLP-1) analog that has anti-inflammatory properties, showed reduced inflammation and increased pancreatic islet viability compared with brain-dead control animals 43 . In that study, pancreatic gene expression of IL-1β was elevated in brain-dead rats, but decreased with exendin-4 treatment. Thus, therapies to reduce inflammation in organ donors, such as pro-inflammatory cytokine blockade, appear to be a promising intervention in donors in order to improve recipient outcomes.
Studies performing a time-course analysis of cytokine expression have shown increased cytokine levels at the time of BD diagnosis 13,39,40,44 . In humans, serial assessment of plasma IL-6 levels in patients with severe head injury showed values above the normal range on admission, but patients who developed BD had a marked increase in IL-6 at the time of BD confirmation compared with those who did not 40 . Supporting the hypothesis that inflammatory mediators peak before organ retrieval, Lopau et al. showed increased soluble interleukin-2 (IL-2) and TNF receptor values and IL-6 serum values at the time of BD diagnosis compared with controls undergoing neurosurgical intervention, followed by a drop after 6 h 44 . In the present study, cytokines increased from baseline to 6 h, which was approximately the time of BD confirmation.
This is the first study to compare plasma cytokine levels between brain-dead patients and critically ill patients, aiming to evaluate the role of sepsis and other intensive care situations in the inflammation promoted by BD. The main strengths of our study are the exclusion of septic brain-dead patients from analysis, eliminating a major confounder, and the collection of samples at the first clinical examination for BD, and then before BD confirmation. This approach allowed us to describe the kinetics of cytokine release from an early period, when we believed that the inflammatory response would be pronounced, until organ retrieval or circulatory arrest, when cytokine values may be decreasing.
This study has some limitations. First, the sample size was based on TNF values from a previous study 18 and may be underpowered to detect smaller differences. Second, we did not collect samples for time-course analysis in controls, so the results for IL-10 and TNF should be interpreted with caution, warranting further studies to clarify this issue. Third, we had a significant loss to follow-up at time point 3 (due to the fact that only a few patients became effective organ donors), limiting a better evaluation of the kinetics of cytokine release later after BD diagnosis. In line with this, a time course with more time points of measurement, such as at 1 and 2 h in addition to 6 and 12 h, might have more consistently demonstrated plasma cytokine behavior.
Conclusions
In conclusion, our data suggest that BD-induced systemic inflammation is as high as that induced by sepsis, and both BD and sepsis are associated with higher inflammation than the observed in critical illness without associated sepsis. These findings support the hypothesis that BD itself triggers the inflammatory cascade and prompt clinical evaluation of therapeutic approaches to attenuate this response and improve graft outcomes.
Footnotes
Acknowledgments
We thank Patricia Koehler Dos Santos for her expert assistance in the cytokine analysis and Vania Naomi Hirakata for her expert statistical counseling. We would like to thank the FIPE (Fundo de Incentivo à Pesquisa) of Hospital de Clínicas de Porto Alegre for their support in manuscript publication.
Authors’ Contribution
PS participated in the study conception and design, data acquisition, analysis and interpretation of data, statistical analysis, drafting and revision of the manuscript. GC participated in data acquisition and analysis. JR participated in data acquisition and analysis. DC participated in the study conception and revision of the manuscript. CBL participated in the study conception and design, interpretation of data, statistical analysis and revision of the manuscript. THR participated in the study conception and design, data acquisition, interpretation of data and revision of the manuscript.
THR is the guarantor of this work and, as such, had full access to all data and takes responsibility for the integrity of the data and the accuracy of data analysis.
Ethical Approval
The study protocol was approved by the ethics committee at Hospital de Clínicas de Porto Alegre. Informed consent was obtained from patients or their legal representatives.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the ethics committee at Hospital de Clínicas de Porto Alegre (130142) approved protocols and according to the Declaration of Helsinki of 1975.
Statement of Informed Consent
Written informed consent was obtained from the patients or their legal representatives for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fundo de Incentivo à Pesquisa e Ensino (FIPE) of Hospital de Clínicas de Porto Alegre and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS). CBL and DC receives a scholarship from Conselho Nacional de Desenvolvimento Cinetífico e Tecnológico (CNPq-PQ).