
Abstract
Moxibustion (艾灸) is a traditional Chinese medicine therapy performed using Artemisia argyii. Zusanli (足三里, ST36) is an acupoint in the stomach meridian, long associated in ancient Chinese medical practices with the extension of life span when moxibustion is applied to it. The aim of this study was to investigate changes in insulin-like growth factor 1 (IGF-1) levels after application of moxibustion to ST36. Four healthy men and women participated in this 28-day trial and were randomly divided into 2 groups. Group A received moxibustion treatment from days 1 to 14, while group B received moxibustion treatment from days 15 to 28. Blood samples were taken 5 times during this study to measure serum IGF-1 (s-IGF-1) levels. The s-IGF-1 levels increased in both groups after 7 and 14 d of moxibustion therapy (group A: 11.02% [7 d] and 29.65% [14 d]; group B: 169.12% [7 d] and 274.85% [14 d]). After moxibustion therapy had been completed (day 14), s-IGF-1 levels continued to increase in group A (increases on day 21 and day 28 were 53.19% and 61.45%, respectively). There were no adverse events in either group. The s-IGF-1 levels were significantly raised in both groups after 7 and 14 d of moxibustion therapy. Moreover, once therapy had been completed, s-IGF-1 levels continued to increase in group A up to 14 d after the treatment.
Introduction
Insulin-like growth factor 1 (IGF-1) and growth hormone (GH) are involved in the regulation of glucose metabolism, inflammation, and immunity 1,2 . IGF-1 is the predominant mediator of GH’s endocrine and metabolic effects 1 –4 . An individual lacking in IGF-1 will give rise to GH deficiency, which is primarily characterized by an increase in visceral fat leading to unfavorable lipid profiles, insulin resistance, and glucose intolerance 5 . Low serum IGF-1 (s-IGF-1) levels are associated with an increased risk of all-cause mortality in the elderly 6 and in patients with type 2 diabetes mellitus 7 and also linked to an increased risk of cardiac arrhythmias in the elderly 8 and somatotroph dysfunction in adults with pituitary diseases 9 .
IGF-1, as a neurotrophic and pleiotropic factor for neuronal cells, plays a significant role in the development and maturation of the central nervous system. It also promotes the growth, differentiation, maturation, survival, and proliferation of neural cells 2,10 –20 . Studies have investigated whether IGF-1 can have a beneficial impact on spinal formation, synaptogenesis, axon outgrowth, and myelination 13,21 . IGF-1 has also been studied in relation to the treatment of Alzheimer’s disease pathologies and spinal cords in amyotrophic lateral sclerotic models 21 . Moreover, the neuroprotective actions of IGF-1 are involved in blocking early apoptosis after hypoxic-ischemic brain injury both in vivo and in vitro 10,11,22 IGF-1 may also play an essential autocrine/paracrine role in the recovery of hypoxic-ischemic brain injury, reducing the loss of oligodendrocytes, and demyelination while also inhibiting programed cell death 23 .
In traditional Chinese medicinal theory, the stomach meridian has the primary responsibility of digestion as well as providing nourishment and energy to the body and its organs. Moxibustion (艾灸) is a traditional Chinese medicine therapy using Artemisia moxa. In ancient Chinese medical practices, moxibustion applied to ST36 has long been used not only for treating diseases, but also for improving health and extending life span.
IGF-1 is a significant contributor to hypoxic-ischemic brain injury, including decrease in postischemic white matter injury, short-term brain rescue, and delayed cell death in animal models 10,23 and can presumably inhibit postischemic programed cell death 23 . The aim of this pilot study was to investigate the association between the moxibustion therapy and the s-IGF-1 levels by moxibustion applied to acupoint ST36, in order to propose the potent impacts on hypoxic-ischemic brain injury and extending life span for further research.
Materials and Methods
Study Design and Subjects
The inclusion criteria for study subjects were healthy adults aged between 25 and 35 years without any chronic diseases and no history of serious diseases. Four subjects were enrolled in this trial and randomly assigned to either group A or group B, ensuring that 1 woman and 1 man were in each group. All subjects received a 14-d treatment course of moxibustion during the 28-d trial: either during the first 14 d (group A) or during the second 14 d (group B).
To protect personal information, approval was obtained from the institutional review board at the China Medical University Hospital (CMUH105-REC3-095). All participants gave their informed consent before this trial.
Treatment
Moxibustion therapy uses mini moxa sticks (Fig. 1) made from dried mugwort. Subjects used a mini moxa stick attached to the Zusanli acupoint (ST36) at the same time everyday during their course of moxibustion. After the complete combustion of the first stick, a second stick was placed on ST36 of the same leg. Therapy was performed on the left and right legs on alternate days. ST36 is located four finger widths’ down from the bottom of patella and a thumb widths’ lateral from the anterior border of the tibia. No treatment was performed during the nonmoxibustion therapy course.

Mini moxa sticks applied to the ST36 (Zusanli) acupoint.
Group A received the moxibustion therapy for the first 14 d, followed by a nonmoxibustion therapy for the second 14 d, while group B first received the nonmoxibustion therapy followed by the moxibustion therapy. Both groups A and B underwent blood specimen collections (BSCs) five times over the course of the study period. All subjects had their first BSC the day before this study commenced (day 0). The second, third, fourth, and fifth BSCs were taken after therapy on days 7, 14, 21, and 28, respectively (Fig. 2).

Intervention of the study. Abbreviation. BSC—blood specimen collection. First BSC: the day before this trial; second, third, fourth, and fifth BSCs are taken after 7, 14, 21, and 28 days of finishing treatment, respectively.
Outcome
The s-IGF-1 values were measured as the outcome of this study, and s-IGF-1 levels were detected by ELISA. The first blood sample was obtained in the morning on day 1, and the others were obtained in the morning after days 7, 14, 21, and 28. None of the participants was fasting when blood samples were taken.
Statistical Analysis
Descriptive statistics, average and relative changes in s-IGF-1 levels, were calculated in Microsoft Excel 2010.
Results
Both groups A and B consisted of one participant of either sex. The age of the female and male participants was 29 and 32 years in group A and 28 and 25 years in group B, respectively. The groups received 2 different treatment models (Table 1). Because the s-IGF-1 level of subject given the code B2 was rather different from other participants at baseline (Table 1), the relative change in s-IGF-1 (RC s-IGF-1) was analyzed instead of absolute values in this study.
Baseline Characteristics and Treatment Models.

Abbreviation: IGF-1, insulin-like growth factor 1.
The s-IGF-1 levels were increased after moxibustion for 7 d and 14 d for all the participants. The average RC s-IGF-1 after moxibustion for 7 d and 14 d were as follows: group A: 11.02% and 29.65% respectively; group B: 169.12% and 274.85%, respectively. The RC s-IGF-1 levels after 14 d of moxibustion were higher than after 7 d in both groups (Table 2).
Relative Change in Serum IGF-1 between Baseline and after Treatment.
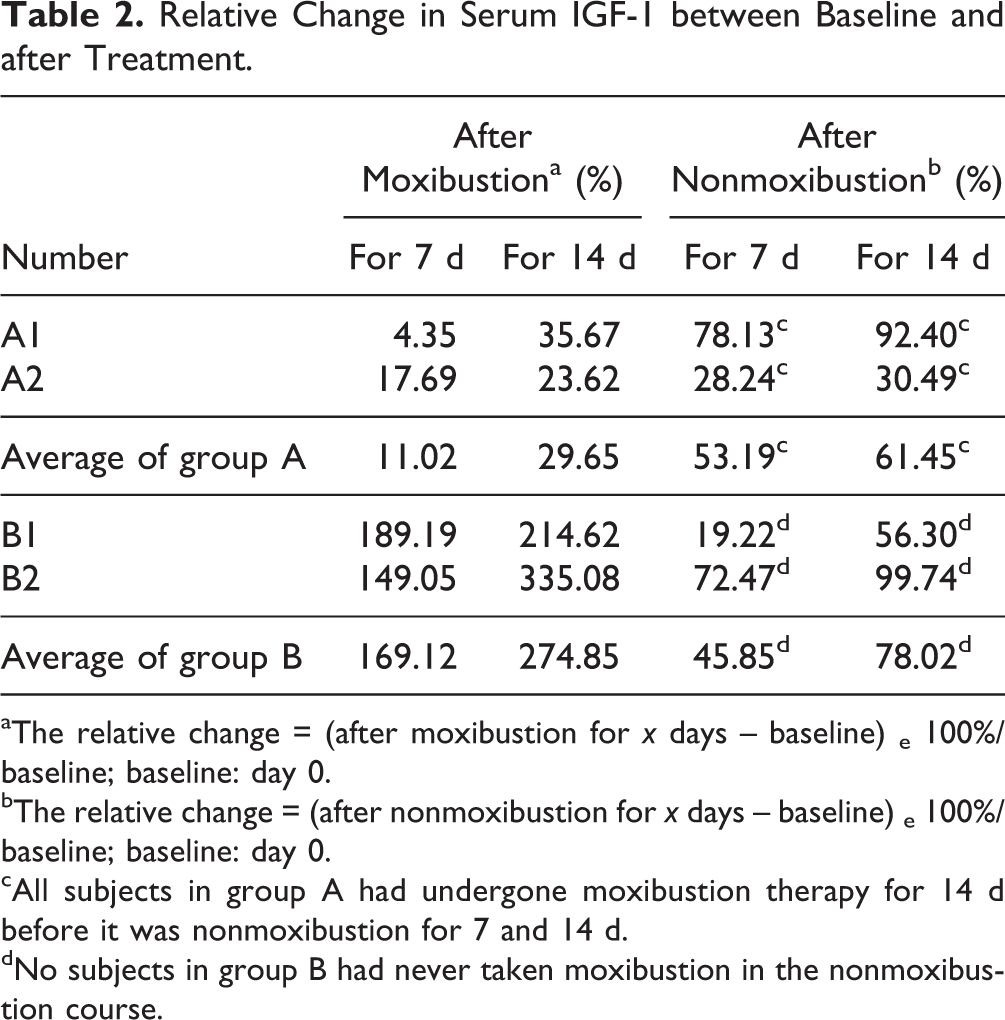
aThe relative change = (after moxibustion for x days − baseline) e 100%/baseline; baseline: day 0.
bThe relative change = (after nonmoxibustion for x days − baseline) e 100%/baseline; baseline: day 0.
cAll subjects in group A had undergone moxibustion therapy for 14 d before it was nonmoxibustion for 7 and 14 d.
dNo subjects in group B had never taken moxibustion in the nonmoxibustion course.
In group A, the RC s-IGF-1 were still increasing during the nonmoxibustion therapy despite the moxibustion therapy being discontinued 7 and 14 d earlier; the average RC s-IGF-1 were 53.19% and 61.45%, respectively. The RC s-IGF-1 were raised from 11.02% (moxibustion for 7 d) to 61.45% (14 d after moxibustion treatment; Table 2).
In group B, participants who still had not received their moxibustion therapy displayed increased RC s-IGF-1 from baseline. The average RC s-IGF-1 for 7 d and 14 d were 45.85% and 78.02%, respectively. The RC s-IGF-1 increased from 45.85% (7 d before moxibustion therapy) to 274.85% (after moxibustion for 14 d; Table 2).
The RC s-IGF-1 of participants who had undergone moxibustion therapy for 7 d and 14 d were raised 4.35% to 189.19% and 23.62% to 335.08%, respectively. The RC s-IGF-1 were still raised 7 and 14 d after the cessation of the moxibustion therapy 28.24% to 78.13% and 30.49% to 92.40%, respectively (Fig. 3).

Relative change (%) in serum IGF-1 between baseline and after treatment 1. Group A: moxibustion therapy during day 1 to day 14 and nonmoxibustion during day 15 to day 28. 2. Group B: nonmoxibustion therapy during day 1 ∼ day 14 and moxibustion during day 15 to day 28.
Adverse Effects
No adverse effects occurred in this study.
Discussion
In group A, the s-IGF-1 levels continued to rise up to 14 d after the completion of the therapy; therefore, moxibustion therapy might have residual effects. It may be worthwhile to investigate the duration of moxibustion therapy’s effects, considering the washout period of a crossover trial in future research.
There might have been a placebo effect in group B during the nonmoxibustion treatment 24 –26 because the RC s-IGF-1 levels were increased even though participants had not yet received the moxibustion therapy (Table 2). It is not possible to say which group benefited more from the moxibustion therapy, although, the RC s-IGF-1 levels at day 28 were higher in group B than group A (Table 2, Fig. 3). First, the baseline levels of s-IGF-1 in group B were lower than those in group A (Table 1). Second, the size of this study is too small to support the result.
IGF-1 is not only a pleiotropic factor in neuronal cells but also involved in development, differentiation, and maturation of a variety of cell types. The anti-apoptotic function of IGF-1 is capable of increasing survival and promoting embryonic implantation and growth in mouse models 2,11,13 . Mice with an IGF-1 gene defect have reduced body, brain, and spinal cord size as well as growth retardation, muscle hypoplasia, delayed ossification, infertility, abnormal lung development, and deafness 13,14,16,18,27 –32 . Moreover, the IGF-1/IGF-1 receptor system is involved in organ growth in humans, including the regulation of generation, differentiation, and maturation of neurons, as well as the proliferation and survival of neural progenitors during central nervous system development and adult neurogenesis 2,10,12 –20 .
Studies have suggested that children with homozygous defects of the IGF-1 gene have smaller head circumferences and shorter stature 33,34 . The IGF-1 defect would lead to abnormal development of the central nerve system during both prenatal and postnatal periods 34 . A low level of IGF-1 has beneficial impacts on protective, anti-inflammatory, and antioxidant activities. It can also prohibit pathogenic mechanisms such as carcinogenesis and early stage cancer development 4 . It is disputable whether IGF-1 is involved in increasing bone mineral density and growth or not 27 .
However, a low s-IGF-1 level, even within the normal range, is associated with an increased risk of all-cause mortality in the elderly, 6 whereas a study has suggested that both low (10th percentile) and high (90th percentile) IGF-1 levels had higher risk of all-cause mortality than moderate IGF-1 levels in men, but not women 3 . Another study has implicated higher s-IGF-1 levels (160-239 ng/mL) in those aged 50 years and older as being associated with an elevated risk of cancer death 35 .
Another study supports that high IGF-1 and IGF-2 levels were associated with an increased risk of squamous intraepithelial lesions of the cervix 36 . Additionally, high IGF-1 levels and elevated IGF-1: IGFBP-3 (insulin-like growth factor binding protein-3) ratios among premenopausal and postmenopausal women have been associated with higher terminal duct lobular unit counts, which are related to increased risk of breast cancer 37 . The possible drawback of moxibustion at the ST36 is whether the elevated s-IGF-1 level is helpful or harmful for an individual, although the increased s-IGF-1 level by moxibustion therapy is the benefit of this study. To determine the range of elevated s-IGF-1 level by moxibustion being favorable to human health will be the urgent issue in further studies.
IGF-1 levels might be altered by specific medication. A cohort study of people suffering from mental disorders found that IGF-1 levels can be reduced in patients taking antidepressants, who are depressed or suffering from anxiety disorders, whereas these levels were raised in individuals not taking antidepressants 38 .
A study that addressed electroacupuncture at acupoint ST36 found that it could improve myocardial pathological morphology in rats with chronic myocardial ischemia 39 , and another study investigated whether acupuncture and electroacupuncture at ST36 could reduce hypertension in a rat model of renal failure–induced hypertension 40 . Acupuncture and electroacupuncture at acupoint ST36 will make good progress in rat models of chronic diseases and conditions, but there have been very few studies conducted on the effect of moxibustion applied to ST36. The potential impact of moxibustion at ST36 and other acupoints on s-IGF-1 levels will be considered for further studies.
Conclusions
The s-IGF-1 levels were obviously increased in both groups after 7 and 14 d of moxibustion therapy. Moreover, after moxibustion therapy had been completed, s-IGF-1 levels continued increasing in group A; this effect lasted for the remaining 14 d of the trial. The s-IGF-1 will be raised by moxibustion therapy in this study.
Furthermore, this study suggests that moxibustion therapy is quite effective for elevating s-IGF-1 levels, and it can be an alternative therapy to apply on hypoxic-ischemic brain injury in order to conquer programmed cell death and increase survival.
Limitations of the Study
There are several limitations in this pilot study. First, baseline s-IGF-1 levels were rather different between groups A and B. Therefore, the RC s-IGF-1 was analyzed instead in this study. Second, this is the first study performed to explore the association between moxibustion and IGF-1, and it was rather difficult to determine the washout period. That was why no washout period existed in this study design. Third, the sample size was 2 in each group, which therefore might not provide strong enough evidence to support our results.
Footnotes
Acknowledgments
This study was supported by China Medical University Beigang Hospital, Taiwan, influence of moxibustion on stem cells progenitor in young adults project (CMUBH R103-007).
Authors’ Contributions
Jaung-Geng Lin, Shinn-Zong Lin, and Lih-Hwa Lin provided equal contribution to this work. J.-G. Lin, S.-Z. Lin, and L.-H. Lin contributed equally to work as cofirst authors.
Ethical Approval
Approval was obtained from the institutional review board at the China Medical University Hospital (CMUH105-REC3-095).
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from participants before this trial.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paul R. Sanberg (PRS) is the coeditor in chief of Cell Transplantation. Neither PRS nor any of his colleagues were involved in the peer-review process or decision for this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.