
Abstract
Can homeopathy cure all diseases? Depending on whom you ask, answers to this question might be very different. This research investigates what homeopathy users believe about (a) whether and how homeopathy should be used to treat serious conditions like cancer, and (b) science and the relevance of scientific evidence regarding homeopathy. Using latent profile analysis (N = 225), we identify subgroups of homeopathy users that differ in their normative beliefs about the use of homeopathy in serious conditions: supporters of standalone use of homeopathy in serious conditions (~9%), those who are open toward standalone use (~43%), supporters of supplementary use (~35%), and supporters of both supplementary use and nonuse in serious conditions (~13%). Subgroups that supported or were open toward the standalone use of homeopathy in serious conditions held the most negative attitudes toward science. These findings are relevant for interventions aiming to prevent the risks associated with homeopathy use.
Keywords
Homeopathy is a pseudoscientific school of medicine that was developed by the German physician Samuel Hahnemann (1755 – 1843). Based on observations he made during self-experimentation, Hahnemann developed the idea that illnesses could be cured by substances which, if administered to healthy people, cause similar symptoms to that same illness (Loudon, 2006). This idea is known as the similarity principle (“like cures like”) and remains at the core of homeopathy to this day. For instance, to treat insomnia, a homeopathic product based on caffeine would be appropriate, since caffeine can cause sleep problems. A range of highly diverse substances, ranging from plants and minerals to remnants of the Berlin Wall, serve as the basis for homeopathic products (Mukerji and Ernst, 2022).
Another core principle of homeopathy is “potentiation”: To produce homeopathic products, the initial substances are diluted in a specific manner until a certain ratio of dilution is reached. This process is thought to make even poisonous substances useable for treatment. The higher this “potentiation,” the greater is the efficacy of the product thought to be. Often, the final products are so dilute that the initial substance becomes unmeasurable, so that homeopathic products typically consist of nothing more than water and sugar (Grimes, 2012). To test homeopathic products, these are administered to healthy persons in so-called “proving.” The participants subsequently observe changes of any kind on themselves, which is thought to reveal the kinds of symptoms that the remedy can treat.
Considering the implausibility of these principles, it is perhaps unsurprising that homeopathy is found to be no more effective than a placebo in randomized controlled trials (EASC, 2017; Mathie et al., 2017; National Health and Medical Research Council (NHMRC), 2015; Shang et al., 2005). It has also been argued that homeopathy qualifies as a pseudoscience, since its proponents often claim scientific standing yet make “bizarre ontological claims incompatible with natural science” (Mukerji and Ernst, 2022: 1). Despite this lack of evidence and plausibility, homeopathy remains popular around the world (Relton et al., 2017), particularly in German-speaking countries. According to a recent survey, more than 60% of German citizens have used homeopathy at least once, and around 20% are fully convinced of its effectiveness (IfD Allensbach, 2023).
Why might this be? A variety of processes are likely at play, such as disappointment with official medical system, fear of side effects of conventional treatments, or a desire for more “holistic” and “natural” remedies (Schmacke, 2020). Another crucial factor likely is that homeopaths are able to dedicate considerably more time to their patients than conventional health practitioners: The first consultation with a homeopathic doctor takes between one and three hours, during which the patient can freely talk about their problems and concerns (Grams, 2015). As such, homeopathic consultations may provide benefits similar to counseling or person-centered psychotherapy (Grams, 2015). In addition, the fact that homeopathic treatments are covered by many public health insurances lends them an unwarranted sense of legitimacy (Siggelkow, 2024).
1. Adverse consequences of homeopathy use
One might argue that it is unproblematic if people rely on homeopathy: Common homeopathic products consist of nothing but water and sugar. Thus, such products might help leverage placebo effects without any side effects. Placebo effects describe the phenomenon that sham treatments can produce symptom improvements (e.g. Tang et al., 2022). These improvements are thought to result from the expectation of improvement elicited by the treatment context (Tang et al., 2022). However, the placebo effect is not uncontroversial: It has been argued that it is not a reliable phenomenon and may be explained in large parts by statistical phenomena (regression to the mean) and spontaneous remission (Hengartner, 2020).
Detrimental effects of homeopathy use in the context of serious conditions have been documented in several places: Research has shown that a standalone treatment with alternative medicine in cancer patients is linked with a 2.5 to 6 times greater risk of death compared to conventional cancer treatment (Johnson et al., 2018b). In addition, patients who used alternative medicine delayed conventional cancer treatments (Akhtar et al., 2018). Further, patients who received complementary alternative medicine refused additional conventional treatments (e.g. surgery, chemotherapy, or radiotherapy) more frequently and showed poorer 5 year overall survival than patients choosing exclusively conventional treatments (Johnson et al., 2018a). The higher mortality rate associated with complementary alternative medicine was mediated by the refusal of additional conventional treatments.
In sum, relying on homeopathy can cause people to delay or completely replace effective conventional treatments with ineffective homeopathic remedies (Posadzki et al., 2012). This is particularly worrisome in the context of serious medical conditions. Nonetheless, it is easy to find reports of clinics that rely on homeopathy alone in the treatment of serious conditions (e.g. Hehli, 2017), organizations that promote homeopathic treatments for victims of natural disasters, epidemics, or poverty (e.g. Homeopaths without Borders, 2024), or official treatment guidelines that take homeopathy to improve patients’ quality of life into consideration (AWMF Leitlinien Register, 2024).
2. The present research
Given the risks associated with homeopathy use in serious conditions, it is important to identify what homeopathy users believe about whether and how homeopathy should be used in the treatment of serious conditions. Individuals who believe that homeopathy is suitable as a standalone treatment are at risk of harming their own and others health: When faced with a serious disease, they might trust a practitioner recommending a standalone homeopathic treatment and lose valuable time for an effective treatment.
Not much psychological research has examined beliefs about homeopathy, let alone normative beliefs about the conditions in which it should (and should not) be used. A notable exception concerns Stoneman et al.’s (2013) Latent Class Analysis of attitudes toward homeopathy and evidence-based medical treatments. They found that the majority of people in a general population sample from the UK held positive views toward both homeopathy and conventional medicine: Most participants preferred the use of homeopathy alongside conventional medicine rather than relying on just one. Here, we take a similar approach but focus on homeopathy users specifically (rather than the general population) and their beliefs regarding homeopathy in the context of serious conditions.
We aim to identify distinct subgroups of homeopathy users that differ in their normative beliefs about whether and how homeopathy should be used in the treatment of serious conditions. Toward that end, we apply latent profile analysis, a person-centered technique that identifies underlying subgroups in a population (Van Lissa et al., 2024). Should the findings of Stoneman et al. (2013) generalize to a German context and serious conditions, a large subgroup that supports the use of homeopathy alongside conventional medicine (i.e. as a supplement) can be expected. We were particularly interested in whether a subgroup supportive of the standalone use of homeopathy in serious conditions could be identified.
In a follow-up analysis, we further investigated the subgroups’ attitudes toward science. Homeopathy users often leverage claims about the alleged corruption of scientists and the alleged limitations of the scientific method to justify their beliefs and dismiss the scientific evidence regarding homeopathy (Information Network Homeopathy, 2024; Munro, 2010). Comparing the subgroups’ attitudes toward science will provide us with a better understanding of their characteristics.
In summary, we address the following research questions: (1) Are there distinct subgroups of homeopathy users that differ in their normative beliefs about the use of homeopathy in serious conditions? (2) Does a subgroup that supports the standalone use of homeopathy in serious conditions exist? (3) How do the identified subgroups differ in their attitudes toward science and scientific evidence regarding homeopathy? Answering these questions will lay the groundwork for future psychological research on the use of alternative and evidence-based medicine and provide important insights for efforts aimed at mitigating the health risks associated with reliance on treatments not backed by empirical evidence, such as homeopathy, at the cost of evidence-based alternatives.
3. Method
Participants
The sample consists of n = 225 people that indicated to have used homeopathic remedies in the last year. Participants were recruited via social media (e.g. Facebook groups related to alternative medicine), student mailing lists at the University of Osnabrück, Germany, mailing lists of alternative-medicine related organizations, and flyers in doctor’s offices. Participants had the opportunity to win one of two vouchers worth 100€ each. On average, participants were 40.68 years old (min = 29, max = 79, SD = 15.15). The sample consisted of 185 women, 25 men, and 4 diverse participants (1 person did not indicate their gender). These gender proportions are likely driven by the fact that women are more likely to use homeopathy than men (IfD Allensbach, 2023; Kristoffersen et al., 2014; Statista, 2024). Almost all participants (n = 219) were German nationals, other nationalities included Swiss, Belgian, Mexican, and Finnish.
Measures
All items were answered on a 7-point Likert-type scale from 1 (do not agree at all) to 7 (agree completely). The measures used in this research were part of a larger survey that additionally included items about participants’ reasons for using homeopathy and visiting homeopathic practitioners.
Use of homeopathy in serious conditions
We used three self-developed items to measure beliefs about the use of homeopathy in the context of serious conditions. In conjunction, these items allow to differentiate the subgroups of interest: (1) “Homeopathy can cure any kind of disease,” (2) “Homeopathy should only be used supplementary to conventional medicine in the treatment of serious conditions (e.g. cancer),” (3) “Homeopathy should not be used at all when treating serious conditions (e.g. cancer).” These items were used as indicators in the latent profile analysis.
Attitudes toward homeopathy-related science
We used three self-developed items that capture different beliefs that homeopathy users might hold toward homeopathy-related science: (1) “The efficacy of homeopathy is scientifically proven,” (2) “I believe in the efficacy of homeopathy even if it is not yet scientifically proven,” and (3) “I do not care if the efficacy of homeopathy can be scientifically proven or not.”
Attitudes toward science in general
To measure general attitudes toward science, we used items from the Negative Perceptions of Science Scale (Morgan et al., 2018). Since we used subsets of these subscales, their factorial structure cannot be taken for granted. We subjected all items to an exploratory factor analysis (oblimin rotation) and maintained those items that (a) loaded onto their primary factor above 0.40, (b) loaded onto secondary factors below 0.30, and (c) demonstrated a difference of 0.20 between primary and secondary factors (Howard, 2016). This resulted in four factors corresponding to the expected subscales: science as corrupt (e.g. “Scientists are often dishonest about their research findings”), onerous (e.g. “Science is too complicated to understand”), heretical (e.g. “Religious scriptures [e.g. The Bible] are the ultimate explanation for how the world works”), and limited (e.g. “The scientific method is limited”). Two items from the “science as limited” subscale were excluded due to cross-loadings with the “science as corrupt” factor (i.e. “Science produces many contradictory findings,” and “Science has significant limitations”). Cronbach’s alpha for all resulting subscales ranged from .74 to .88. Full scales and details on the factor analysis are presented in Supplemental Material.
4. Results
All data, materials, and analysis code be found on the Open Science Framework: https://osf.io/hbrz4/
Latent profile analysis: Model selection
We followed best-practice recommendations for latent profile analysis (Van Lissa et al., 2024) and estimated a variety of latent profile models with different variance-covariance specifications and increasing numbers of profiles. We compared all models that could be successfully estimated on several fit indices that are recommended to consider jointly in the process of class enumeration: the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), and the sample-size adjusted BIC (Van Lissa et al., 2024). The lower the value of these fit indices, the better the model fit. As recommended, we additionally considered classification diagnostics (Van Lissa et al., 2024): classification probabilities for the most-likely latent profile (ideally, individuals should have a high classification probability for one class and low probabilities for all others) and entropy values, which summarize class separability into a single statistics (for details on model fit, see Supplemental Material).
We estimated models with up to 5 latent profiles. The BIC, which is often considered a suitable default for model selection (Van Lissa et al., 2024), favored the five-profile model with equal variances and no covariances. The AIC and sample-size adjusted BIC favored the five-profile model with equal variances and equal covariances. This model, however, yielded one class that was very small and potentially unreliable (3% of the sample). For that reason, we compared the five- and four-profile models with equal variances and no covariances. The additional profile in the five-profile model appeared to be a variation of profile 4 and did not provide substantively new insights (see Figure S1 in Supplemental Material). For that reason, we selected the four-profile model. According to the classification diagnostics, this model provides accurate classification and well-separated profiles (see Supplemental Material for details). We ensured that our main conclusions were robust against this decision (Figures S1 and S2 in Supplemental Material).
Latent profile analysis: Description of final model
Figure 1 demonstrates the item profile plots of the final model. On the x-axis, the indicator variables are depicted; on the y-axis, the average agreement of each profile on these indicator variables is depicted. The plot shows raw data, whose transparency is weighed by the posterior class probability, such that each observation is most clearly visible for the class the model has assigned it to (Van Lissa et al., 2024). Table 1 summarizes the final model.
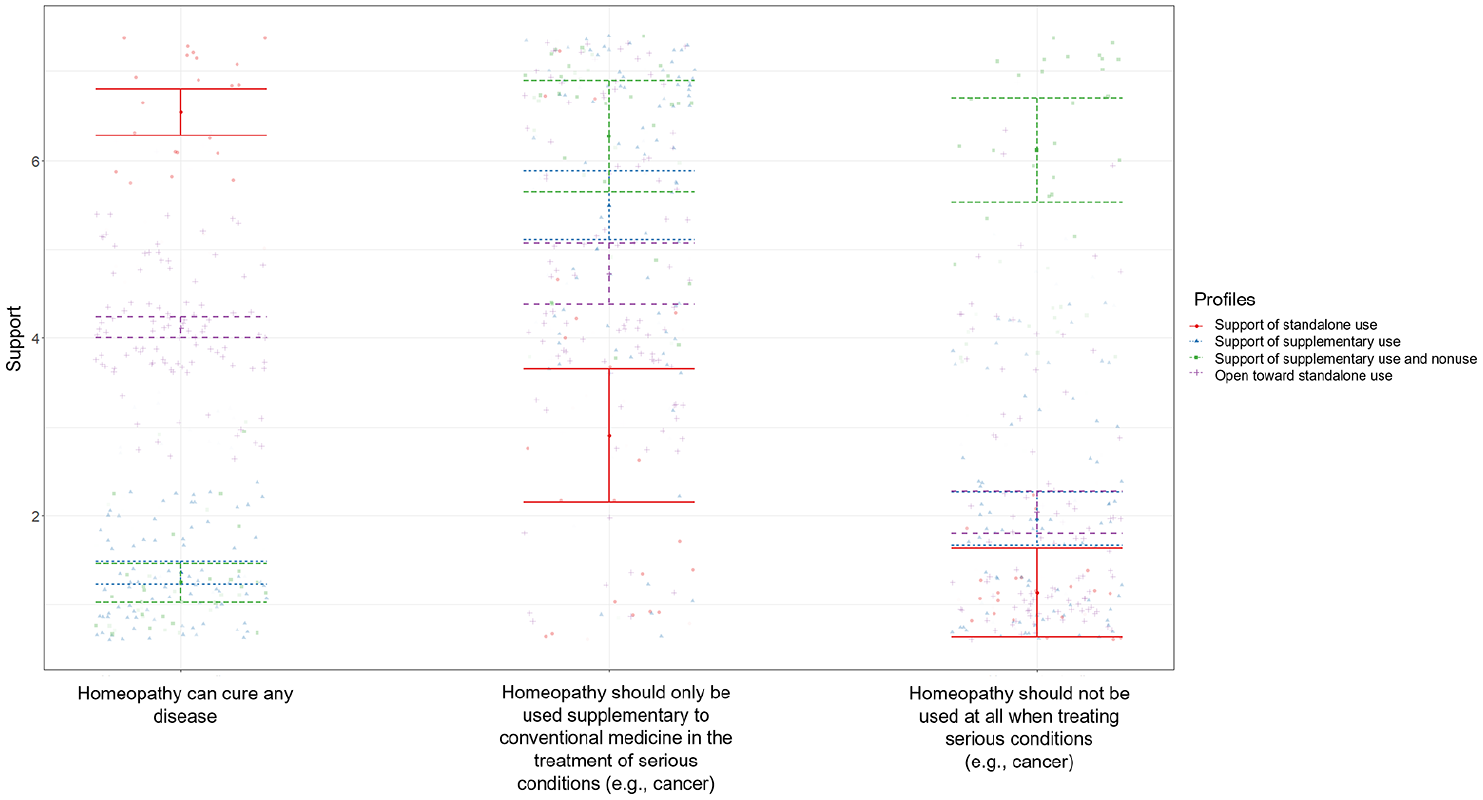
Item profile plot.
Summary of model results.
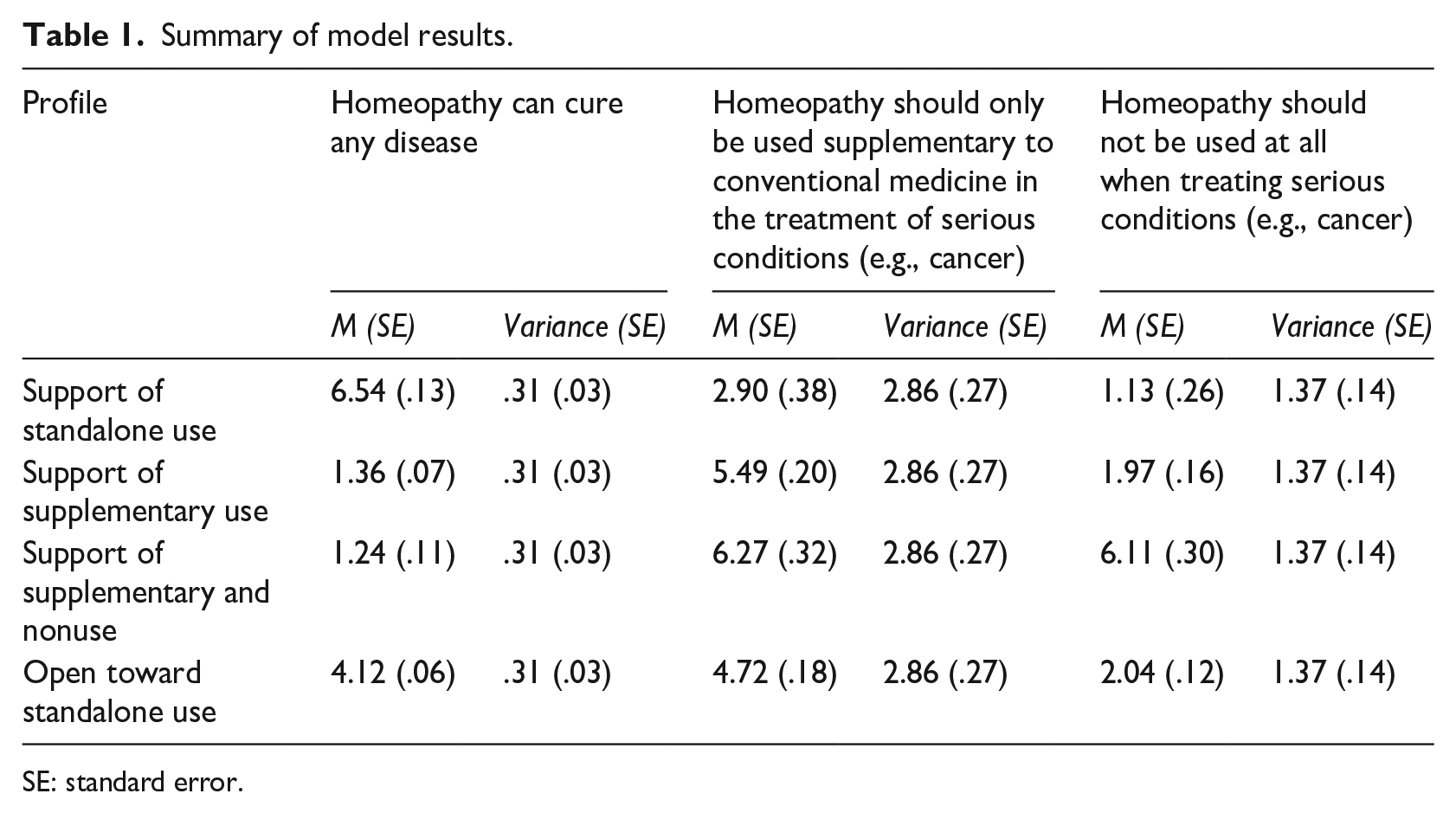
SE: standard error.
The four profiles represent well-interpretable subgroups reflecting different stances toward the use of homeopathy in serious conditions. Members of class 1 (n = 21, 9.42%) agree with the statement that homeopathy can cure any disease and support its standalone use to treat serious conditions, as indicated by a rejection of both statements that homeopathy should be used only supplementarily in serious conditions, and that it should not be used at all. Hereafter we label that class “Support of standalone use.” Members of class 4 (n = 96, 42.50%) are undecided whether homeopathy can cure any disease (they score, on average, around the scale mean). Notably, they are also undecided whether homeopathy should be used only supplementarily in serious conditions and reject the statement that it should not be used at all in these cases. Thus, this class demonstrates an openness toward the standalone use of homeopathy in serious conditions, although it is not as convinced as class 1 (hereafter, we label this class “Open to standalone use”).
Members of classes 2 (n = 78, 34.67%) and 3 (n = 30, 13.42%) disagree with the idea that homeopathy can cure any disease and tend to agree with its use as a supplement. Class 2 rejects the idea that homeopathy should not be used at all in serious conditions (and thus explicitly supports the use of homeopathy as a supplement), while class 3 also supports this statement. Apparently, class 3 accepts both supplementary and nonuse of homeopathy in serious conditions (hereafter “Support of supplementary use and nonuse”), while class 2 explicitly wants homeopathy to be used as a supplement (hereafter “Support of supplementary use”).
Follow-up analyses
Attitudes toward homeopathy-related science
In order to test whether the subgroups significantly differ in their attitudes toward homeopathy-related science, we conducted likelihood ratio tests that take the classification uncertainty associated with latent profile membership into account (using the recommended BCH-method (Van Lissa et al., 2024)). Results revealed that the subgroups differed significantly in the belief that the effectiveness of homeopathy was scientifically proven (ΔLL (6) = 50.45, p < .001), in their agreement that they believed in homeopathy although it is not yet scientifically proven (ΔLL (6) = 42.48, p < .001), and in their agreement that they do not care whether homeopathy can be scientifically proven or not (ΔLL (6) = 19.31, p = .004). Overall, the profile “Support of standalone use” scored highest on all three items, followed by the profile “Open to standalone use” (see Figure 2). Pairwise comparisons are reported in Supplemental Material.
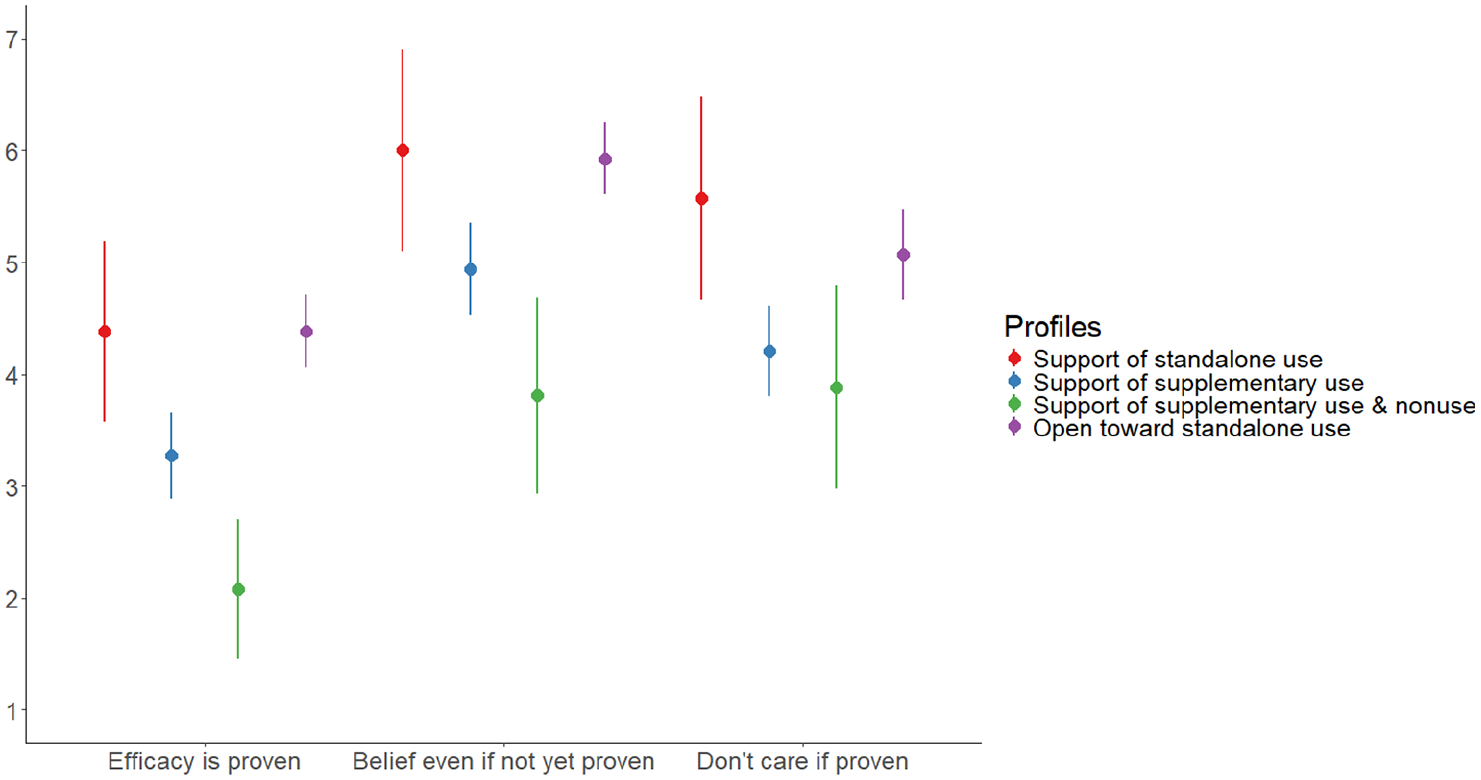
Means and 95% confidence intervals for homeopathy-related science attitudes per profile.
Attitudes toward science in general
Likelihood ratio tests revealed significant differences between the profiles regarding science as corrupt (ΔLL (6) = 86.97, p < .001), science as limited (ΔLL (6) = 40.22, p < .001), science as onerous (ΔLL (6) = 23.54, p < .001), and science as heretical (ΔLL (6) = 173.58, p < .001). Overall, the profile “Support of standalone use” holds the most negative views of science: They score highest on science as corrupt, limited, onerous, and heretical, followed by the profile “Open to standalone use” (see Figure 3). The profile “Support of supplementary and nonuse” consistently scores lowest on all four subscales. Pairwise comparisons are again reported in Supplemental Material.
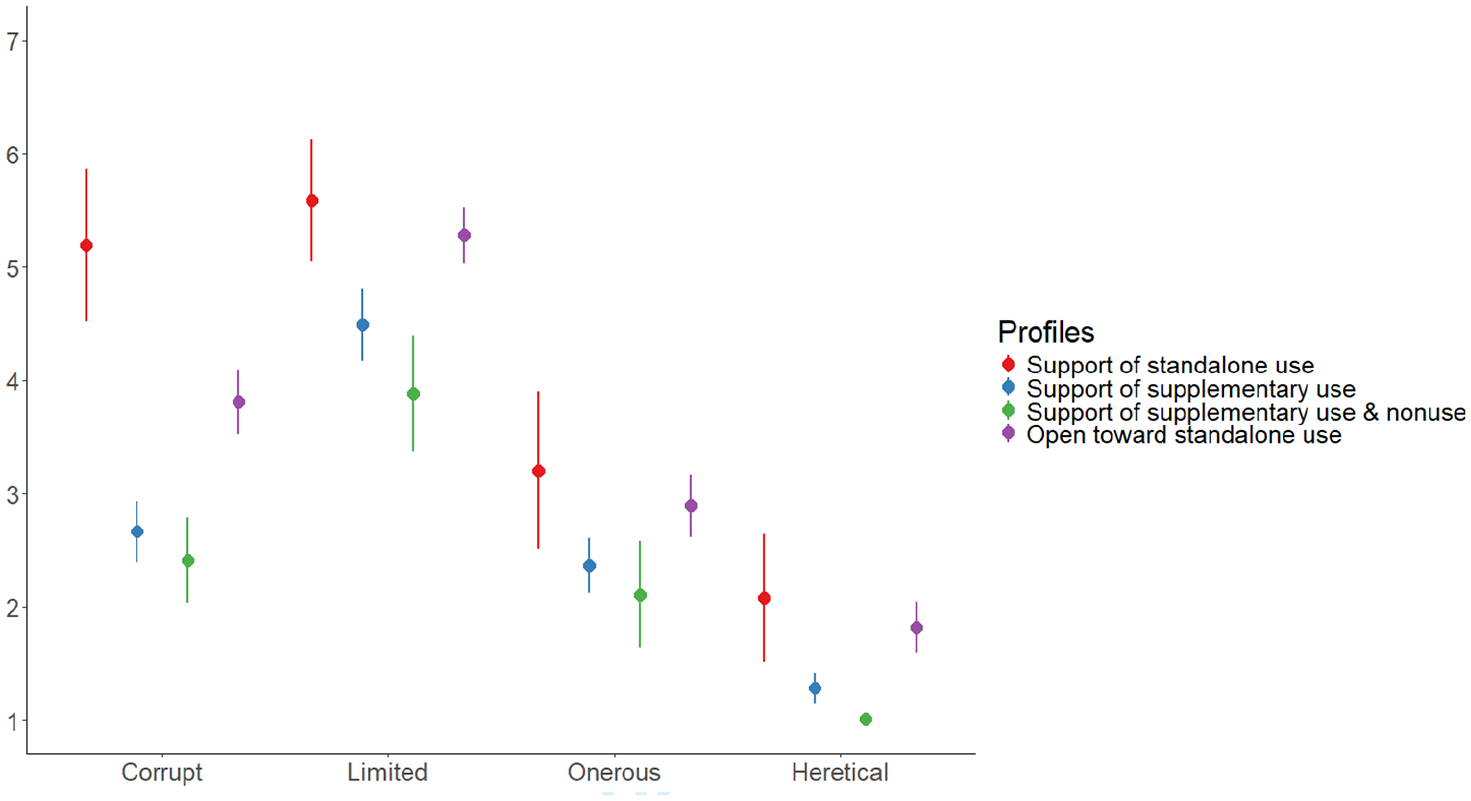
Means and 95% confidence intervals for attitudes toward science in general per profile.
5. Discussion
This research investigated what homeopathy users believe about the use of homeopathy to treat serious medical conditions like cancer. Using latent profile analysis, we identified four subgroups with different stances toward the use of homeopathy in serious conditions: supporters of standalone use of homeopathy in serious conditions (~9%), those being open toward/undecided about the standalone use of homeopathy in serious conditions (~43%), supporters of supplementary use (~35%), and supporters of both supplementary use and nonuse in serious conditions (~13%). These subgroups further differed in their attitudes toward science: The subgroups that supported or were open toward the standalone use of homeopathy in serious conditions perceived science to be the most limited, corrupt, onerous, and heretical. They also cared the least about scientific evidence regarding homeopathy and indicated to believe in its effectiveness even if it is not yet scientifically proven.
In this sample, the subgroup that clearly supported the standalone use of homeopathy in serious conditions constituted a minority. In terms of mitigating public health risks, this is good news. Nonetheless, such people clearly exist and could be identified without further ado in a convenience sample of homeopathy users recruited on social media, student mailing lists, and alternative-medicine-related organizations. These people are clearly at risk of trusting clinics that offer, for example, homeopathic cancer treatments or relying on organizations providing homeopathic “emergency services.” In addition, a large subgroup of undecided users emerged (~43%), which moderately agreed that “homeopathy can cure any disease,” indicating that they at least consider this a possibility. We do not know how members of this subgroup would actually behave when faced with a serious medical condition. However, on the basis of these results, the possibility that they might choose a standalone homeopathic treatment (or at least try it out first) cannot be excluded.
About half of our sample favored practices that appear, at first glance, harmless: They either supported homeopathy use strictly as a supplement or accepted both supplementary use and nonuse in serious conditions. However, the supplementary use of alternative medicine in cancer patients is not without harm: It has been associated with the refusal of additional conventional treatments that were needed later in the treatment process, resulting in higher mortality rates (Johnson et al., 2018a). More broadly, using homeopathy as a supplement results in a situation of attributional ambiguity where any improvements may be wrongly attributed to the homeopathic treatment, increasing the likelihood that the patient will rely primarily on homeopathy in the future.
In conjunction, these results highlight the need for interventions aimed at preventing the use of homeopathy in the treatment of serious conditions. Such interventions could take place at both a structural (e.g. legal restrictions or stricter sanctions for practitioners that conduct or allow such treatments, better financing of evidence-based medicine so that doctors have more time for their patients) and individual level (e.g. educational efforts targeting homeopathy users). Regarding the latter, it needs to be kept in mind that both subgroups most in need of interventions (i.e. the subgroups supporting or being open toward the standalone use of homeopathy in serious conditions) indicated the most negative attitudes toward science: They cared the least about scientific evidence regarding homeopathy and perceived science to be the most corrupt and limited. Given these characteristics, simply informing members of these subgroups about the scientific consensus regarding homeopathy—as is typically recommended in the psychological literature to address beliefs in conflict with scientific evidence (e.g. van der Linden, 2021; Većkalov et al., 2024)—might not be an effective strategy. Instead, interventions might first have to create a shared understanding of the importance and value of scientific evidence and evidence-based treatments. This might entail, for example, a more foundational education about how the scientific method works, and why it is superior to, for example, relying on personal experiences and observations in making causal judgments.
Limitations and future research
More research is needed to understand why some homeopathy users dismiss the relevance of scientific evidence and why they perceive science to be corrupt and limited. For example, it should be studied how homeopathy users explain and justify their dismissal of science and scientific evidence (e.g. Gershman, 2019). Future research could then investigate whether specifically targeting these convictions can improve evaluations of homeopathy-related scientific evidence and evidence-based treatments. Ultimately, this may entail not only educational efforts but also structural changes that improve the transparency of scientific procedures and prevent undue influences of third-party funding (Fernández Pinto, 2020).
Participation in this study was voluntary and may be influenced by self-selection biases. Participants were partly recruited on social media groups related to alternative medicine. Members of such groups may hold more extreme beliefs than other homeopathy users, resulting in a potential overestimation of the risks associated with homeopathy use. Conversely, homeopathy users with highly negative attitudes toward science may have refused to participate, since the survey was administered by a scientific institution. Either way, the present sample may not be representative of the population of homeopathy users.
Relatedly, our sample size was rather small for a latent profile analysis. In general, about 300 cases are desirable, yet smaller samples may be adequate with simpler models (fewer indicators and classes) and well-separated classes (Nylund-Gibson and Choi, 2018). Since our model was simple and classes were well-separated, we are optimistic that sample size was adequate. Nevertheless, our results should ideally be replicated in a larger sample.
Further, the latent profile model selection process entails some subjectivity. Other models than the one chosen here could have been justified based on the fit indices. One cannot conclude that the chosen solution represents the literally true number of latent profiles that exist in the population, but rather an interpretable and (hopefully) useful approximation (Curran and Bauer, 2021). The fact that competing models yielded similar conclusions increases our confidence in this claim.
6. Conclusion
Despite being a minority in our sample, homeopathy users that support the standalone use of homeopathy to treat serious conditions like cancer clearly exist. These individuals are at risk of harming their own (and others’) health. In combination with the large subgroup of undecided users that emerged in our sample, these findings highlight the need for interventions aimed at preventing harmful homeopathy use. Most likely, before factual communication of scientific evidence can have a persuasive effect, negative attitudes toward science among homeopathy users need to be targeted.
Supplemental Material
sj-docx-1-pus-10.1177_09636625251332524 – Supplemental material for Can homeopathy cure all diseases? Subgroups of homeopathy users based on beliefs about whether and how homeopathy should be used to treat serious conditions
Supplemental material, sj-docx-1-pus-10.1177_09636625251332524 for Can homeopathy cure all diseases? Subgroups of homeopathy users based on beliefs about whether and how homeopathy should be used to treat serious conditions by Luisa Liekefett and Julia C. Becker in Public Understanding of Science
Footnotes
Acknowledgements
We thank Simone Sebben and several anonymous reviewers for very helpful comments and critiques that greatly contributed to this article.
Data Availability Statement
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.