
Abstract
Scientific uncertainty during pandemic outbreaks poses a challenge for health communicators. Debates continue over the extent to which health officials should be transparent about uncertainty and the extent to which they should suppress uncertainty and risk losing the public’s trust when information changes. The middle ground, the concept of “reasoned transparency,” proposes that communicators focus on interpreting uncertainty to the public in ways informed by risk research. However, little guidance exists for health officials on how to do so in this context. After conducting a series of one-to-one interviews about people’s coronavirus disease 2019 information habits, we identified significant trends in the heuristics that people depended on to process uncertainty. Based on those trends, we propose health communicators use narratives of science as evolving to set expectations for change, and that when changes do occur, health communicators note divergences from the past and avoid simply replacing old information with new information.
Keywords
1. Introduction
Interviewer: If later on, researchers came out and said that this information had changed or was no longer accurate, how would you feel about that? Anna: I don’t think there’s harm in it, but it does just make it seem less credible when every day has a new direction. So it’s a double-edged sword. I understand changing your narrative with new information, but that doesn't mean it doesn’t make it seem uncredible when it flip flops.
How do public health communicators remain transparent about scientific uncertainty during emergent infectious disease events without undermining their future credibility or confusing their audiences with changing messages? Negotiating scientific uncertainty is particularly difficult during pandemics and continues to challenge health communicators in the present climate (Davis, 2019; Driedger et al., 2018; Rajkhowa, 2020). For instance, complications arose in early 2021 as uncertainty about coronavirus disease 2019 (COVID-19) vaccine safety (e.g. concerns over blood clots related to the AstraZeneca vaccine) resulted in mixed messaging, leading to confusion and vaccination hesitancy (SteelFisher et al., 2021). Effective communication strategies aimed to help individuals navigate public responses to changing pandemic messaging are necessary to avoid such confusion and loss in credibility. This article aims to help address this need by presenting two strategies stemming from a qualitative study that examined how people respond to hypothetical changes in COVID-19 science.
Previous scholarship on navigating pandemic uncertainty has called for public health messaging to employ “reasoned transparency” rather than “fishbowl transparency,” that is, to follow a strategy guided by communication principles meant to ensure that audiences are not merely provided with information, but that information is interpreted and contextualized, so that the public can understand it (Driedger et al., 2018; Löfstedt and Bouder, 2014). This article builds upon such scholarship by isolating one variable in public responses to changing pandemic science: heuristic shortcuts.
We conducted one-on-one elicitation interviews to examine spontaneous reactions to hypothetical changes in two areas of science related to COVID-19: the efficacy of face-masks and the efficacy of vaccines. Results from the analysis revealed two dominant trends in heuristic responses. Trust and affect heuristics were somewhat called upon to formulate participant responses; however, expectancy heuristics—particularly the expectation that science will change—were the most powerful influence on participant strategies of coping with changing public health messaging. This pattern held true in responses to hypothetical changes in both face-mask and vaccine science. However, although the confirmation of expectations that science would change was influential enough to spark a positive response to changing face-mask science, that effect was counteracted by other factors in responses to vaccine information, notably tradition and previous knowledge, so that responses were decidedly more negative. Based on these findings, we offer two communication strategies guided by a reasoned transparency approach.
2. Review of relevant literature
The field of science communication has advanced far beyond an “information deficit model” that assumes that public misunderstanding of science is primarily attributable to a lack of scientific knowledge (Lévy-Leblond, 1992). For example, in the context of the pandemic, a deficit model presumes that if citizens do not understand how to best mitigate COVID-19 in their lives, it is because they do not have the right information (Seethaler et al., 2019). In contrast, research over the past several decades has demonstrated that individuals’ relationships with information is impacted by a wide array of cultural, social, political, moral, ideological, and economic factors (National Academies of Sciences, Engineering, and Medicine (NASEM) et al., 2017). For example, Rutjens et al. (2021) argue that attitudes toward science can be better understood from the perspective of individuals’ worldviews, ideologies, and cultural identities. Kahan et al. (2011) not only support that argument but also postulate that “cultural cognition shapes individuals’ beliefs about the existence of scientific consensus and the processes by which they form such beliefs” (p. 1). Better understanding of such effects are essential at times such as the ongoing pandemic as polarization in public opinion and group denial of scientific evidence may become both a threat and an obstacle to efforts being made to mitigate the impact of COVID-19 on public health systems.
Beyond the concern with uncertainty in science, there is also the risk of science skepticism. Although science is mostly accepted by communities in many places around the world, research has also indicated a surge in the systematic rejection of scientific evidence and practice (Pew Research Center, 2009; Rutjens et al., 2022). The increase of science skepticism, although not generalized, still poses a significant threat to public health, especially when it comes to domain-specific skepticism around topics, such as vaccination, climate change, and, more recently, the COVID-19 pandemic (Dryhurst et al., 2020; Rutjens et al., 2018). In other words, understanding science skepticism, and the factors that influence how people engage with scientific information in a changing information environment is essential for improved science communication.
Another fundamental aspect of science communication that must be accounted for is tied to the operation of science itself, specifically the way in which science changes and can at times be uncertain, as is the case with emergent infectious disease events. Indeed, no science is ever absolute (NASEM et al., 2017), and this inherent uncertainty (of varying degrees) presents several challenges for science communication. When members of the public engage with science information, they typically seek “yes” or “no” answers, not uncertainties or ambiguities (Kruglanski and Webster, 1996). In addition, the reception of science communication can be influenced by various factors, such as an individual’s prior knowledge of science or numeracy. However, when dealing with uncertain or complex information, people often unconsciously rely on heuristics, or mental shortcuts (NASEM et al., 2017). Frequency of appearance, alignment with pre-existing beliefs, expectations, tradition, endorsement from friends and trusted sources, previous knowledge, association with good memories, and many other heuristic cues alleviate the mental load of evaluating uncertain information and enable people to cope both with complexity in general and with complex scientific information in particular (Fazio et al., 2015; Lindström et al., 2018; McCabe and Balota, 2007; Slovic et al., 2004). Heuristics are neither good nor bad; they are simply part of how humans process complex information; however, attention to how they operate is crucial for science communicators and educators because heuristics can bias audiences against science information that does not satisfy heuristic cues (Fazio et al., 2015; Tversky and Kahneman, 1974).
Given the complex influence of factors that impact science communication, it is perhaps unsurprising that there is no consensus on how public health communicators should express scientific uncertainty during pandemic situations. Some argue that health officials must emphasize the uncertainty of their messaging because trust in scientists cannot be built if scientists are not honest about the limitations of their information (Holmes, 2008). During the 2009 H1N1 pandemic, for example, Australian health officials at first established a core message that the virus was dangerous to everyone and that everyone should take precautions while giving few caveats about the certainty of that message. When their information changed, health officials pivoted to a new message that the virus was only dangerous to some people without really explaining how or why the message had changed; this lack of transparency led to a public backlash (Davis, 2019). In contrast, some suggest that public health communicators should suppress the uncertainty of their information because members of the public do not know how to deal with lack of certainty (Frewer et al., 2003). For example, during the same 2009 H1N1 pandemic, Toronto public health officials adopted the opposite strategy to those in Australia: officials openly emphasized the uncertainty of their information, but the inability of officials to give the public the certainty they demanded resulted in a loss of confidence in health officials (Driedger et al., 2018). Clearly, the solution to the uncertainty problem is likely not “either/or” expressing or suppressing uncertainty as both paths can seemingly lead to confusion and loss of confidence. Rather, the solution seems to suggest a more nuanced, “reasoned transparency” based on further research into how members of the public consume and cope with uncertainty (Coglianese, 2009; Driedger et al., 2018; Löfstedt and Bouder, 2014).
Reasoned transparency has been defined in medical communication as a collaborative relationship between patients and health care professionals built on sound explanations and strong relationships aimed “to foster patient understanding” (Mabillard et al., 2021) and in political communication as the disclosure of the reasons underlying government actions (Coglianese, 2009). While the disclosure of information about government decisions and the involvement of the public in decision-making are valuable discussions in those fields, reasoned transparency within the context of pandemic communication remains largely undefined. As a useful start, Löfstedt and Bouder’s (2014) definition of reasoned transparency is simply a version of transparency that is guided by risk research as opposed to “fishbowl transparency” which is not guided by research. Driedger et al. (2018) emphasize the need for communication science to inform the ways health authorities communicate about science, as transparency is complex and nuanced. As such, while scholars have called for the application of reasoned transparency to pandemic communication, that seems to remain little more than a principle of research-informed-communication, lacking explicit strategies or best practices for communicators to follow. Through an examination of hypothetical attitudes toward changing mask and vaccine science, this article seeks to provide practicable insights into how public health communicators can employ reasoned transparency as a strategy that foregrounds evidence-based understanding of science communication by identifying how changing pandemic information can trigger positive heuristic reactions and avoid triggering negative heuristic responses.
Face masks and vaccines have both been the subject of changing public health messaging at different moments of the pandemic, and thus made ideal themes for investigation. In the first half of 2020, the World Health Organization (WHO), along with other health organizations and national governments, were criticized for confusing messages about the use of face-masks to prevent the spread of COVID-19. On 6 April 2020, the WHO (2020a) released guidance on the use of masks which asserted that masks should only be worn by healthcare workers. On 5 June, the WHO (2020b) updated its guidance and asserted that the general public should wear masks. During this period (roughly March to August) a series of news and opinion articles critiqued the negative impact that this changing messaging had on efforts to control the pandemic (e.g. Cheung, 2020; Kottasová, 2020). Later in the early months of 2021, AstraZeneca, state governments, and international health agencies all came under fire for sowing confusion and vaccine hesitancy through contradictory messaging around the safety and efficacy of the Oxford-AstraZeneca vaccine (Wise, 2021). Throughout March 2021, 25 nations suspended or restricted the use of the Oxford-AstraZeneca vaccine over concerns that the vaccine was connected to a rare blood clotting disorder (Al Jazeera 2021). At the same time, the WHO and the European Medicines Agency (EMA) released statements insisting that despite uncertainty, the vaccine was safe and nations should not restrict its rollout (EMA, 2021; WHO, 2021). These mixed messages led to another series of news and opinion articles charging public health communicators with undermining confidence in vaccines at a critical moment in COVID vaccination campaigns (Rosenbaum, 2021; Sorkin, 2021). At the time that our interviews took place, COVID vaccines had not yet been developed and only changes to face-mask messaging had taken place; however, we sought to be future-oriented and anticipated that changes to vaccine messaging may become an issue later in the pandemic, and so that, we designed our research to address hypothetical changes to both face-mask and vaccine messaging. We thus posed the following research questions: what heuristic cues do people lean on to cope with hypothetical changes in pandemic-related health messaging, and how can these heuristic cues inform messaging strategies?
Methodology
We conducted 27 semi-structured elicitation interviews to explore heuristic responses to changes in public health science during a pandemic. Potential participants were Canadians who were at least 18 years of age at the time of data collection and who had recently engaged with COVID-19 information online. To incentivize participation, we offered the choice of either donating US$25 to Food Banks Canada or receiving a gift certificate of the same value if they completed an interview. Participants were recruited using a Facebook advertisement. Potential participants completed a short demographic questionnaire, which we used to sample participants purposefully such that the final sample would be sufficiently diverse (e.g. different age groups, educational level, province of residence, etc.). We conducted interviews in an iterative manner until data saturation was reached. Such an approach to saturation is typical in qualitative research (Baker and Edwards, 2012). The final list of pseudonymous participants is provided in Table 1 in alphabetical order. Participants resided in Ontario (n = 15), British Columbia (n = 7), Alberta (n = 3), and Manitoba (n = 2), and their age ranges were 18–29 (n = 10), 30–45 (n = 7), 46–59 (n = 6), and 60+ (n = 4). Seventeen participants self-identified as women, nine as men, and one chose not to self-identify. Most participants had earned a bachelor’s degree.
Participants.
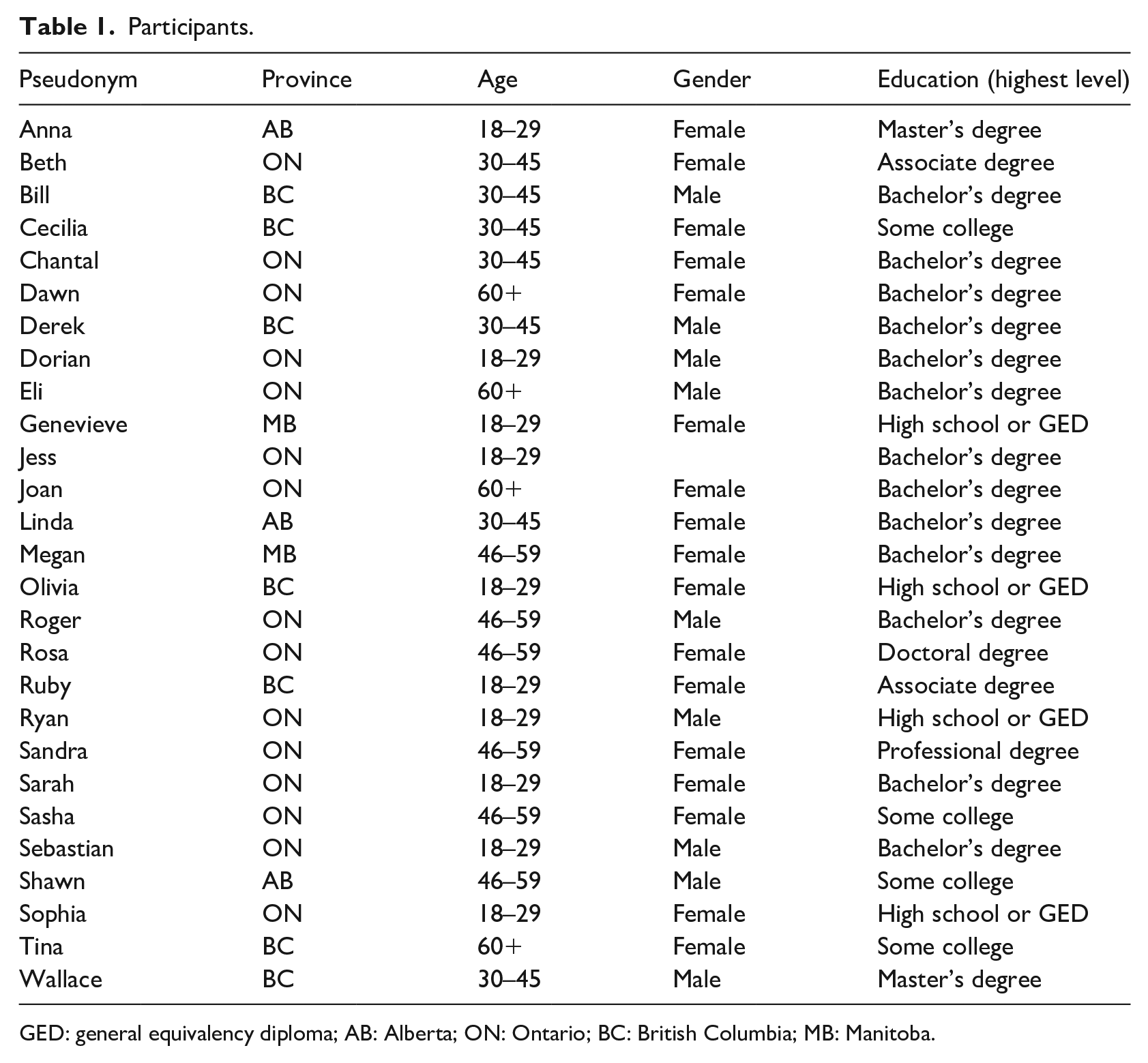
GED: general equivalency diploma; AB: Alberta; ON: Ontario; BC: British Columbia; MB: Manitoba.
Data were collected via one-on-one online interviews held between 22 June and 6 July 2020. The semi-structured interview protocol covered various aspects of participants’ engagement with COVID-19 information, including their views on two artifacts (see Supplemental Material) which were designed by the WHO and retrieved from Facebook. In this article, however, we focus specifically on questions about participants’ thoughts on how they would react if the science behind the efficacy of face-masks and vaccines was to change in the future. Participants were asked two separate questions in two different parts of the interview: “If in the future, researchers find out that this information [about face-masks, or about vaccines] is actually untrue or inaccurate, how would you respond?” We utilized these hypothetical prompts to limit preconceived responses to real-world events and thereby assess heuristic responses to new, fictional events.
In real-world, media-rich environments, heuristic responses are often only the initial reaction to new information. We may initially decide to believe a piece of information because we trust the source, because the font is appropriate, or because it aligns with our previous beliefs. But that initial response is not fixed, and upon re-evaluation, we may change our minds. If a participant is asked about how they reacted to real-world changes in science, answers will reflect the participant’s cumulative evaluation since first encountering the change, and not their immediate heuristic responses. By asking about hypothetical changes in science, we sought to restrict participants’ opportunity for re-evaluation to assess their initial, heuristically informed responses. This is supported by psychological research into the experience of being asked a hypothetical question, which suggests that such questions allow access to less conscious or rational judgments through their metaphorical nature (Branthwaite and Lunn, 1985; Krueger, 1998). Moreover, as stated above, there had been no changes in vaccine science at the time of interviewing, but we anticipated that this would become an issue later on in the pandemic, and so that asking about hypothetical changes in science enabled us to orient our research toward future problems.
Two researchers iteratively analyzed the data arising from the interviews. The first part of the analysis consisted of an independent review of all interviews by each researcher to facilitate broad understanding. Next, three interviews were randomly selected to be read and coded by both researchers. The open coding process was guided by the constant comparative approach to data analysis (Glaser and Strauss, 1967). This process consisted of the comparison of codes created for each new interview with codes that had been generated previously: if codes that were created previously captured the nature of the new information they were used in the coding of new data; if not, new codes were created, thus ensuring that new relevant information would be captured. After the initial round of independent coding, the researchers met to discuss the emerging categories seen in the data. As the codes were found to be similar, the remaining interviews were iteratively coded by the researchers. Once coding was concluded, three researchers reviewed the findings and identified themes.
3. Results
Heuristics and changing science
A wide variety of cognitive heuristics were employed by participants and appeared to play a role in their responses to changing science. Multiple heuristics are often employed concurrently and, as research by Gigerenzer and Todd (1999) suggests, work together to determine how our participants responded to science change. Alongside affect, three other heuristic cues were employed by the participants: trust, tradition, and expectancy. Interestingly, the influence of these four heuristics was evenly split between positivity and negativity. Affect and tradition cues were associated with negative responses to changing information. None of those who expressed emotional responses expressed positive emotional responses. Sebastian, for example, said that “I would be a little bit fearful” if vaccine science changed, while Cecilia told us that changing face-mask science would be “shocking.” For these participants, affect heuristics tended toward rejection or resistance to changes in science. Tradition cues also tended toward rejection or resistance. Joan said she would be skeptical of changing face-mask science because “masks have been worn for a long time in health care,” while Anna said she would be skeptical of changing vaccine science because “people have thought vaccines worked for a number of years . . . it’s been the held opinion for so long.” Trust and expectancy cues, on the other hand, tended toward positive responses to changing information. Ryan said that he would accept changing face-mask science if it came from the WHO because “they use academic journals to check their, to get their research. And I know that academic journals are generally peer-reviewed and there’s large processes for them to go out into the world.” Expectancy cues also tended to positive responses when participants expected science to change. In response to the idea of vaccine science changing, Dorian said that “I wouldn’t be personally too bothered by it because I can respect and understand that science as a field of knowledge is ever changing.” In response to face-mask science changing, Chantal talks about how more research can lead to changes in science and how we need to adapt to it: I think we all don’t like when the rules change or when the information changes, but the fact of the matter is as we do more research, things can happen like that in science. So we adjust and we take the new information and do our best with it. (Chantal)
Sasha provides a similar account when it comes to possible changes to science. She argues that those changes are something to be expected rather than surprised by: Oh, now coffee is good for you, just as a small example, so health information changes all the time, and sometimes it changes. It’s a 360 degrees shift. What is good is now bad, and what is bad is now good. So yeah, it could well be that at some point, they’ll say, hey, actually, we were wrong all along and vaccines are really the most terrible thing for you. Yeah. I wouldn't be surprised at that. (Sasha)
In this quote, Sasha did not express negative feelings about the prospect of science changing, because she expected health information to change “all the time.” The expectation of a change, was enough to express that she was not bothered by the idea that it could change. Finally, Dorian, when discussing possible changes to vaccine science, describes how science discoveries that lead to changes are adopted and play a role in advancing society: Very similarly, again, like science, just as a field of knowledge is is something that changes over time and if we later find that there is more robust and better clinical practices that are should be adopted, because they’ve been tested and and found to be much more effective in, in preventing or protecting ourselves against something like this, then I think that that evidence, that new evidence, assuming that it’s been tested very adequately, ought to be accepted into clinical practice. I think that’s how science tends to advance our society. (Dorian)
Several participants used appeals to authority especially with respect to the WHO and researchers. Genevieve, for example, said that she would feel fine about changes in mask science if it came from the WHO, which both Eli and Wallace echoed with respect to vaccine science. Appeals to tradition were also quite common. For example, Joan’s skepticism was grounded in the fact that masks have been worn in health care for a long time, and Cecilia was resistant because, as she indicated, she had been told all her life that vaccines are good. While all four heuristic cues were invoked in response to changes in both vaccine and face-mask science, they were not invoked in the same proportions. Across both topics, expectancy was the dominant heuristic cue. Expectancy heuristics are in operation when an individual encounters uncertain information. The extent to which the information conforms to or violates their expectations (e.g. of who provides the information, of how it is formatted, or of its content) impacts whether they trust or mistrust the information (Ault et al., 2017; Bogomoletc and Lee, 2020; Johnston et al., 2015; Metzger et al., 2010). There were 24 references to expectancy, compared to 14 references to tradition, seven to trust, and five to affect. Expectancy was also the dominant heuristic cue for each individual topic, with 12 references in the context of vaccines and 12 in the context of masks. However, while the expectancy cue was the dominant heuristic response across both topics, its valence was different depending on the topic: responses to changing face-mask science were overall positive, while responses to changing vaccine science were overall negative.
If invocation of the expectancy heuristic tended toward positive responses, and the expectancy heuristic was the most invoked heuristic in response to both vaccines and face-masks, then why did participants respond positively to face-masks and not to vaccines? The answer is observed in the relative balance of positive and negative heuristic cues invoked in response to both topics. In the context of face-masks, the next most common heuristic cue after expectancy was trust (n = 4), followed by tradition (n = 2) and then affect (n = 1). Thus, positive cues (n = 16) far out-weighed negative cues (n = 3). The dominance of positive heuristics (expectancy and trust) successfully indicated that most participants had a positive response to changing mask science. Responses to changing vaccine science were quite different. The prominence of expectancy cues (n = 12) was tied with that of tradition cues (n = 11), followed by affect (n = 4) and trust (n = 3). Thus, positive cues (n = 15) were balanced with negative cues (n = 15). While the positive expectancy heuristic was equally matched by the negative tradition heuristic, negativity won out: most participants (n = 20) had a negative response to changing vaccine science.
Many participants expressed their rejection of hypothetical changes to vaccine science in direct opposition to their understanding of science as inherently changing. While aware that science necessarily evolved, their perception of the long-standing nature of vaccine science overrode participant openness to change. Consider how Bill reconciled his perception of science as unsettled with his perception of vaccine science as settled.
Again, with the general understanding that things, cause it, cause I feel like, you know, I think of vaccines as a whole, that’s been around for much longer than, let’s say like just the whole mask thing. Like I said, I think vaccines. I was like, well, that’s not, I mean I guess it could change. Theoretically science will always change. But I feel like that’s something that, if someone said that to me, I would kind of like pass over it until I kind of followed it a little bit more on the news and it would become, I feel like something like this, it would have to be like pretty much major.
Bill compares his perceived novelty of face-masks with his perceived traditionality of vaccines, and determines that tradition trumps novelty even though he expected science to change. Such sentiments were also expressed by Megan, who said that “I don’t know that this particular information [vaccines science] can change. But I do think that, yeah, in general information changes.” Chantal further demonstrates this trend, stating that “I think that as science evolves, you know, our views on things change and we adjust” while simultaneously emphasizing that she would be unwilling to acknowledge changes to vaccine science “because it’s been working for a long time.”
Our initial examination of the interview data suggested that emotions, such as fear, anger, or frustration (and thus affective heuristic reasoning) would figure prominently into how people responded to hypothetical changes in face-mask and vaccine science. In-depth analysis of the interviews, however, revealed that emotions appeared to play a less important role than anticipated. It would be inaccurate to suggest that an absence of strong emotions means emotions were lacking in the interviews, only that emotions did not present strongly for interview participants. For example, the majority of respondents (n = 22) expressed no emotional response to the question about the possibility of face-mask science changing, and those with responses that could possibly be characterized as including an emotional reaction (n = 5) were ones, such as shock, as when Dawn said she would be surprised to find out that mask science had changed, or disappointment as in the case of Sasha who thought it indicated a lack of due diligence. Responses in relation to changing vaccine science were somewhat more emotional for participants than changes to face-mask science which, given the controversial nature of the question (given the growing trend of anti-vaccine rhetoric among popular influencers), is perhaps unsurprising. For example, two respondents said that they would be upset and four indicated they would be uncertain either about how they would feel or about the actual information itself. Others, however, expressed no emotions, with Derek going so far as to say he “wouldn’t have a feeling” if vaccine science changed. Although the interview data related to the affect heuristic were not as rich as initially anticipated, they did yield the insight that if people were not responding with as much emotion as we had expected, they were relying on some other means to assess potential future science changes. Our analysis led to the understanding that other heuristics, particularly expectancy heuristics, played a more important role in people making sense of changes in science.
4. Discussion
Our results provide insight into how public health communicators can tailor their pandemic-related messaging to help audiences cope with scientific uncertainty and changes in science. Our main findings indicate that when faced with the prospect of changes to pandemic science, people tend to develop either a positive or a negative response informed by four key heuristic cues: trust, expectancy, tradition, and affect. We found that participants predictably developed positive or negative responses depending on the relative balance of these four heuristic cues: positive if guided predominantly by trust and expectancy, negative if guided predominantly by tradition and affect. An extensive scholarship already exists around the importance of trust and emotion in pandemic communication (Bennett, 2020; Freimuth et al., 2014; Siegrist and Zingg, 2014), and our findings support this body of work. However, it is striking that trust and affect were the two least influential heuristic cues utilized by participants in this study. On the contrary, expectancy and tradition were far more influential factors on whether a participant responded positively or negatively to changing science. As such, we offer two communication strategies that incorporate how public health communicators can work with expectancy and tradition heuristic cues to encourage positive responses to changing pandemic messaging.
Communication strategy 1: Use narratives of science as changing to set expectations and normalize change
Building upon the work of Driedger et al. (2018) and Davis (2019), we suggest that communicators must be reasonably transparent about the uncertainty of the scientific information they provide, that is, as Dreidger et al. (2018) contend, “communicators need to be critically aware of how messaging can be perceived, and that transparency is not simply communicating the science without restraint, but about understanding communication science” (p. 591). Thus, contexts, such as an audience’s heuristic traditions, levels of skepticism, and cultural influence, need to inform communication efforts. As part of this reasoned transparency, our data suggest that audiences may benefit from being primed to expect change, so that when change does occur, it satisfies expectancy heuristics and supports a positive response, which may help avoid some of the concerns around credibility that full transparency has resulted in previous pandemics. In other words, reasoned transparency includes anticipating potential responses from the public to new messaging, and tailoring communication accordingly. In the context of changing science and consequent changing public health recommendations, we suggest that this anticipatory strategy can be pushed further to better prime positive responses to change by emphasizing that uncertainty is not a limitation, but a strength of the scientific process. Our study found that perceptions of science as inherently changing over time was the most powerful factor in influencing positive responses to changing science. We suggest that public health communicators can utilize the power of this narrative by reassuring audiences that change is good, and an indication that the process is working as meant to. Change is not divergence from the plan, change is the plan.
Communication strategy 2: When changes do occur, attend to divergence from the past
While expectancy heuristics exhibited a powerful influence on producing positive responses to changing science, it could not compete with the power of tradition heuristics to produce negative responses. In contexts where participants had minimal traditions to pull from, such as wearing face-masks, expectations of scientific change were free to exert their influence, and produce a positive response. However, in contexts participants did have traditions to pull from, expectations of scientific change failed to produce positive responses. This means that the above strategy of emphasizing science as inherently changing will only work in some contexts. Thus, we suggest that when pandemic messaging needs to change, public health communicators should not seek to simply replace the old message with the new message, but should keep the two messages in conversation with one another. Audiences will not forget old messages, and our findings indicate that audiences tend to respond positively to new messages only to the extent that they could be reconciled with old messages. Strategies of “reasoned transparency” proposed by Löfstedt and Bouder (2014) and others have stressed the importance of interpreting data, so that, public audiences can better understand it. Our contribution is to emphasize that it is not just new data that need to be interpreted, but old data as well: why the old data were held as true at one time and not at another, how the old data were rendered invalid, and how the new data impact past decisions made using the old data. By doing so, public health communicators can undermine the power of tradition heuristic to produce negative responses to changing pandemic messaging.
5. Limitations and delimitations
This study’s methodology faces a number of limitations. First, it is important to acknowledge the possible limitations of self-selection as participants chose to respond to our Facebook ad. In addition, most of the interview participants (Table 1) had some level of university education, meaning their understanding of the scientific process may not accurately represent a population with a more varied education background. As COVID-19 has disproportionately affected minority groups (Garcia et al., 2020; Tai et al., 2021)—with some older individuals and those from low socioeconomic status and/or who have in the past experienced barriers accessing health care—it is possible that a sample with individuals from various age groups, and ethnic and socioeconomic backgrounds might have translated into different views toward science and science change. We also did not inquire about cultural or religious attitudes that can shape understandings of science, and groups less inclined to favor science may respond differently to not just changing science, but science more generally (Agley and Xiao, 2021). Second, the interviews focused on Canadian participants, which likely impacted the findings given an established high level of trust in government and health authorities. Readers should therefore be cautious in extending these findings to other populations.
Finally, although the qualitative analysis conducted in this study allows for the transferability of findings, the nature of the study and the number of participants means that these results cannot be generalized. We have, as a result, taken a number of steps to address the possible limitations posed by a qualitative analysis, including providing a thick description of the analysis, and acknowledge that these findings are not generalizable. Nonetheless, these results offer a rich starting point for future investigations that aim to examine whether our findings can be generalizable to the broader population. Researchers would benefit from engaging with a larger number of participants to examine the statistical significance of the varied responses to changing science in the context of the COVID-19 pandemic and how those results can be generalized. While the limitations described may limit the scope of the study, we do not believe that they pose significant challenges to its validity, credibility, and trustworthiness.
6. Conclusion
For researchers studying COVID-19-related health communication, it is important to continue interrogating the role that trust, tradition, expectancy, and affect heuristics play in helping and/or hindering people’s engagement with public health-related information. With respect to health communication on a topic that may spark resistance, this could mean that people need to be prompted to be reflective about their own heuristic shortcuts, biases, and emotional arousal to foster the skills and literacies necessary to spend more time deliberating the merits of the information itself, and future research could examine the role such prompts can play in how health communication is received and understood.
Our exploratory analysis provides an initial investigation of these themes, but there is much more that can be done to understand how these systems are working and the role played by the embodied experience of arousal. The medium of communication (e.g. should the message be delivered on YouTube, Twitter, Television, or Press release) is an important consideration for health messaging, and the way the message is structured is also important (e.g. how the rhetorical strategies used influence the reception), but what should also be better understood is what are the physical, emotional, and psychological influences that either support or mitigate COVID-19 and other pandemic-related communication. Finally, addressing racial and socio-economic demographics as a part of communication relying on reasoned transparency is also a key area for future research. Reasoning through crisis and risk communication is a complex task for both communicators and the public, and thus attention to any single factor, such as demographics or affect, will be incomplete without addressing further factors simultaneously.
Supplemental Material
sj-docx-1-pus-10.1177_09636625221135425 – Supplemental material for Heuristic responses to pandemic uncertainty: Practicable communication strategies of “reasoned transparency” to aid public reception of changing science
Supplemental material, sj-docx-1-pus-10.1177_09636625221135425 for Heuristic responses to pandemic uncertainty: Practicable communication strategies of “reasoned transparency” to aid public reception of changing science by Jaigris Hodson, Darren Reid, George Veletsianos, Shandell Houlden and Christiani Thompson in Public Understanding of Science
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Canadian Institutes of Health Research [Award number: 440296].
Supplemental material
Supplemental material for this article is available online.
Author biographies
![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.