
Abstract
This article draws upon recent scholarship on technoscientific imaginaries and the sociology of technology expectations to reveal the mediating roles played by a number of disease-focused research charities in the United Kingdom. We examine the expectations they deal with about regenerative medicine research, and how they develop strategies to support and ‘protect’ potential medical scenarios for new therapies for dread diseases. In so doing, we develop and detail a concept of scenario maintenance to denote the strategic discursive and practical work of preserving stakeholders’ faith in specific disease research pathways in the face of obstacles. Semi-structured in-depth interviews (N = 10) of research managers at nine research charities were qualitatively analysed, alongside a variety of charities’ documentary data. Our analysis yielded three themes: managing and moderating media expectations; specifying expectations about disease-specific appropriateness of regenerative medicine; and maintaining scenarios of possible pathways for future success taking challenges into account.
Keywords
1. Introduction
Regenerative medicine (RM) is an emerging interdisciplinary field that applies engineering and life science principles to technologies to promote regeneration that can potentially restore diseased and injured tissues and organs for patients. RM research has seen significant developments in recent years across a range of complex disease areas, including neurology, immunology and ophthalmology. Research aims to bring RM therapies and treatments closer to patients. Its techniques aim to accelerate the pace at which the body can heal itself (Mason and Dunnill, 2008) by repairing or replacing damaged or malfunctioning cells and tissues. Targeted disease areas include immune disorders, age-related defects, chronic liver disease, diabetes, neurological diseases such as Parkinson’s disease and Alzheimer’s, arthritis and skin and eye disorders (Mimeault et al., 2007).
There is substantial, growing interest in the field. This is characterised by expectations about the potential that RM holds to change the future of patient care for those with clinically unmet needs. For patients with degenerative diseases, RM has understandably become a source of hope and a symbol of change in the context of current treatment paradigms.
The field has seen some shift from widespread hype to realistic hope in some applications, especially within stem cell research (Nadig, 2009), and within areas showing technological advances potentially offering treatments for patients with particular recalcitrant diseases, such as type 1 diabetes (Chhabra and Brayman, 2013). However, the development of anticipated treatments across a range of disease areas remains a long way from routine clinical application, despite the promissory rhetoric of the media and commercial projections of the potential market. The reasons for this comprise a range of complex issues, including scaling up material for clinical trials, regulatory stringency, limited funding and difficulties in negotiating reimbursement (Rosemann, 2014). Despite these challenges, UK policymakers and funders remain active in funding and supporting RM research (House of Lords, 2013).
What are disease research charities?
Disease research charities are organisations whose primary aim is to fund medical research for the purpose of advancing understanding of a specific disease, and to find treatment, prevention or cure. In the United Kingdom, there are approximately 440 medical research charities (CharityChoice, 2017). While disease research charities are typically involved in a range of activities, including lobbying for their specific interests on behalf of patient groups, they are seen primarily as raising and providing funding to support research to generate new knowledge, translate research ideas into new products and services and create evidence that will influence policy or other stakeholders (Association of Medical Research Charities (AMRC), 2017).
In this article, we consider research charities as key players who are active in the support of innovative treatments across a range of complex disease areas. Whether seeking to find a cure for type 1 diabetes, or preventing the onset of Parkinson’s disease, such charities are both developing RM innovations and discursively and practically contributing to its ongoing emergence as a field. They work in a complex scientific and institutional environment where there exists a multitude of wild hopes and a range of more or less promising achievements and disappointing setbacks. They thus experience a central dilemma of both sustaining hope and expectations about possible therapies but simultaneously moderating hyped expectations in a reasonable, evidence-based way. We explore the discursive and practical roles played by such charities, in the context of scientific research, patients’ hopes, mass media messages and the funding and investment strategies of state and industry. Our study aims to present and conceptualise the positions and roles that these organisations adopt in pursuing such multiple aims in the contemporary politico-economic context of innovative scientific biomedicine, the ‘bio-economy’. We develop the analysis with information from a selection of such charities based in the United Kingdom (see ‘Methods’ section), which are directly involved in RM research. In the following section, we outline the conceptual approach that we have developed in order to do so.
2. Conceptualising disease research charities’ roles: Technoscientific imaginaries, expectations and scenarios
It is obvious that disease research charities’ roles negotiate, what in terms often deployed in the public domain are referred to as, hope, promise, hype, breakthroughs, setbacks and such like. Some Science and Technology Studies (STS) scholarship has been formulated in such language, as cited in this article. Here, we locate such notions in the over-arching concept of discursive ‘technoscientific imaginaries’, and within this frame, we apply the well-developed ideas of ‘technology expectations’, alongside a novel concept of ‘scenario management’ which we develop in the article. We outline the three concepts of this approach below.
Technoscientific imaginaries
The increasing importance of technoscientific (or sociotechnical) imaginations as a constitutive and performative force in the relations of science, politics and society over recent decades has been widely noted (Jasanoff and Sang-Hyun, 2015; Pellizzoni, 2017). Technoscientific imaginaries are conceived as visions of desirable futures formulated and articulated by participating stakeholders for a putatively emerging field of technoscience. Such imaginaries may have a pathway-shaping effect on the development of a field, and their formulations may conflict between different actor organisations (Pellizzoni, 2017; Rommetveit and Wynne, 2017). Such imaginaries can be seen to enter into the work of policymakers, research scientists and technology developers, companies, research funders, and others involved in technoscientific innovation projects. We propose that such imaginaries are useful for considering disease research charities as well. They can be conceptualised as comprising two key dynamics, first a promissory form of work focused around envisioned, expected desirable societal benefits, and second a ‘protective’ dynamic focused on the preservation of the possibilities of emerging technology in the face of challenges, risks or ‘obstacles’. Scholarship in these terms has noted that ‘deficit models of publics are becoming partially supplanted by an “obstacle model”, in which the issues are framed as barriers and obstacles’ (Rommetveit and Wynne, 2017: 142). Such dynamics invite examination of the specific roles of the different types of organisation involved in and co-producing potentially emergent technoscientific fields. Research charities can be viewed as ‘promissory organisations’ producing future-orientated knowledge claims, often from strong institutional positions (Pollock and Williams, 2010). In the field of biomedicine and the bioeconomy, the role of such organisations, compared to pharmaceutical companies and regulators, for example, has been relatively neglected.
Expectations and scenario management
One dynamic of technoscientific imaginaries is performative technology ‘expectations’. A well-established set of STS and sociological studies have explored the significance of expectations in the shaping of the social processes of scientific and technological innovation (Borup et al., 2006; Brown et al., 2000; Brown and Michael, 2003; Michael, 2000; Van Lente, 1993; Verganti, 1999). The ‘sociology of technology expectations’ considers stakeholders’ expectations as playing a constitutive role in the development of science and technology. Understanding the roles of expectation-shaping organisations is crucial to the analysis of potentially emerging technological innovation such as RM. We consider here that the expectations that research charities form and mobilise about their own respective technologies are more than speculative claims, having the capability to shape the trajectory of potential clinical applications for patient benefit (Borup et al., 2006). Promissory expectations can be described as predictions, envisioning the future but situated in the present, and having performative potential (Borup et al., 2006). Morrison (2012) states that within RM, expectations act as ‘promissory narratives’ which can mobilise groups through shared technological visions (Morrison, 2012). Recent scholarship has explored promissory narratives across a range of RM settings, including lab scientists (Lysaght et al., 2008), the media (Michael et al., 2005), biotechnology (Kitzinger and Williams, 2005; Tutton, 2011) and within politics and governance (Gardner et al., 2015; Geesink et al., 2008). Yet, the performativity of such expectations typically varies in an emerging field, being subject to different actors’ investments of emotion, resources and energies. Shared visions, if they are reached, are a negotiated accomplishment.
Expectations and promissory narratives typically co-exist alongside disappointment. Unfulfilled expectations have consequences in how they can create mistrust within a field, and may dampen visions of future progress and hope (Pollock and Williams, 2010). The rise and fall of expectations has been analysed as occurring within a cycle of early promise and hope, followed by disappointment, known as the ‘hype cycle’ (Borup et al., 2006; Brown and Michael, 2003). This is often seen in positive hype reporting of RM in the mass media that can amplify hype, fuelling reactions that further promise an envisaged future or feed a lack of trust (Brown and Michael, 2003).
Within an innovative field such as RM, ‘work’ on expectations can be understood as aligned with such cycles of potential and disappointment, as new and emerging technologies generate competing and sometimes contradictory discussion. RM has yet to see many major products reach clinical practice, though the field may no longer be in an initial phase of development (Morrison, 2012). In such a scenario, language and the dynamics of discourse play a key shaping role (Brown and Michael, 2003). In this article, we demonstrate with data and argue that research charities are directly involved in discursive expectations work, especially in relation to how they manage and moderate media expectations, and how they specify appropriate disease-specific expectations for RM in the face of various extreme claims.
Complementing the management of expectations, the second instantiation of technoscientific imaginaries that we identify is the future-oriented work of ‘scenario management’, a novel construct that we elaborate here. We note that a concept of ‘scenario management’ has a history as a tool for strategic, focused, practical business enterprise planning (Gaussemeier et al., 1998). We adopt the term to refer to the discursive and practical work that an organisation may undertake in order to characterise, support and protect the specific imaginaries constituting a technoscientific field, in which there are multiple forces at play, notably destabilising and disruptive forces. We thus provide a conceptualisation that details organisational attributes, discursive mediating strategies and practical actions that enact the more emotion-related concept of ‘hope’ that is prevalent in the field. We propose that scenario management can be seen to be mobilised to preserve the positive prospects of technoscientific fields in relation to various material and discursive obstacles. The downward turn of the hype cycle is likely to be met by expert and informed actors undertaking strategic discursive and practical work to manage and preserve scenarios of hope and possibility. We argue that research charities are involved in analysing evidence to protect the future of RM in this way.
3. Methods
This article draws upon data collected as part of the REGenableMED project, funded by the Economic and Social Research Council (ESRC; see Acknowledgement). As part of a much larger empirical study involving over 80 interviews, ten semi-structured interviews were conducted with research managers or senior researchers working at nine research charities in 2015 and 2016.
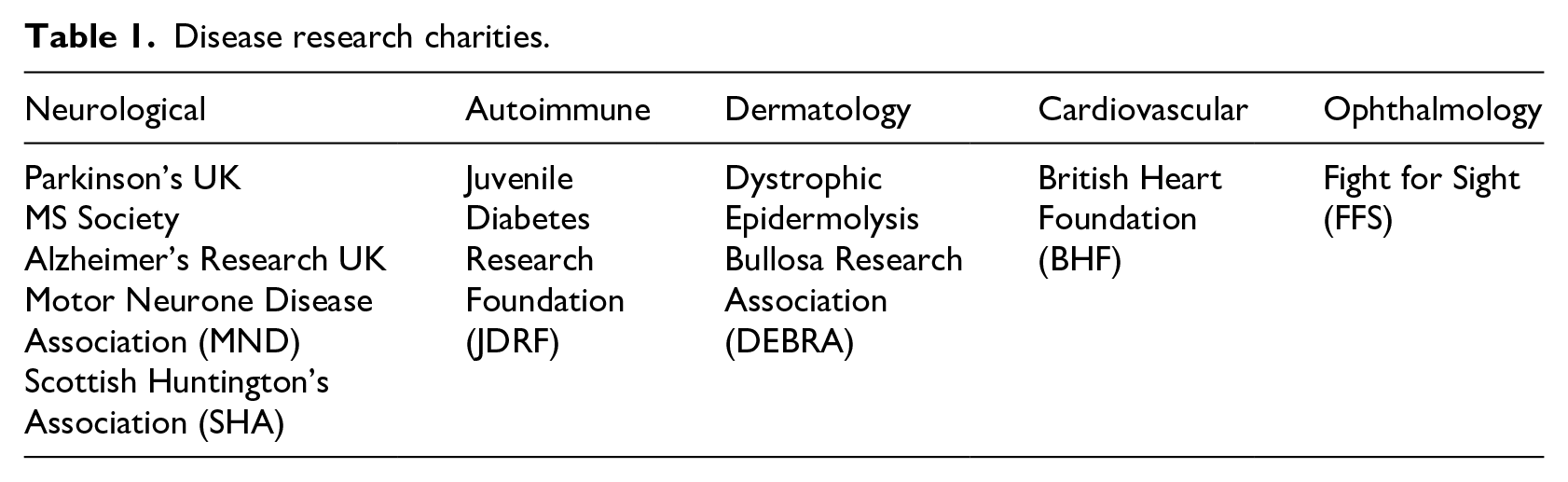
The selection of relevant disease research charities began with desk research to identify those charities based in the United Kingdom that were active in funding RM research. This search produced a list of 32 charities. From this list, nine charities were selected. This selection was primarily informed by the aim of gaining representation across various disease areas (Table 1). The majority of interviews fell under the field of neurology. The neurological field was especially important to explore given that there are a range of research charities therein which have RM programmes, given that it is a well-developed research area. It must be acknowledged that the interview data come from specific and well-known disease areas, and there are other under-developed areas that have not been explored. While we were able to gain perspectives from other disease areas, failures in recruitment and limited resources prevented further interviews from taking place.
Disease research charities.
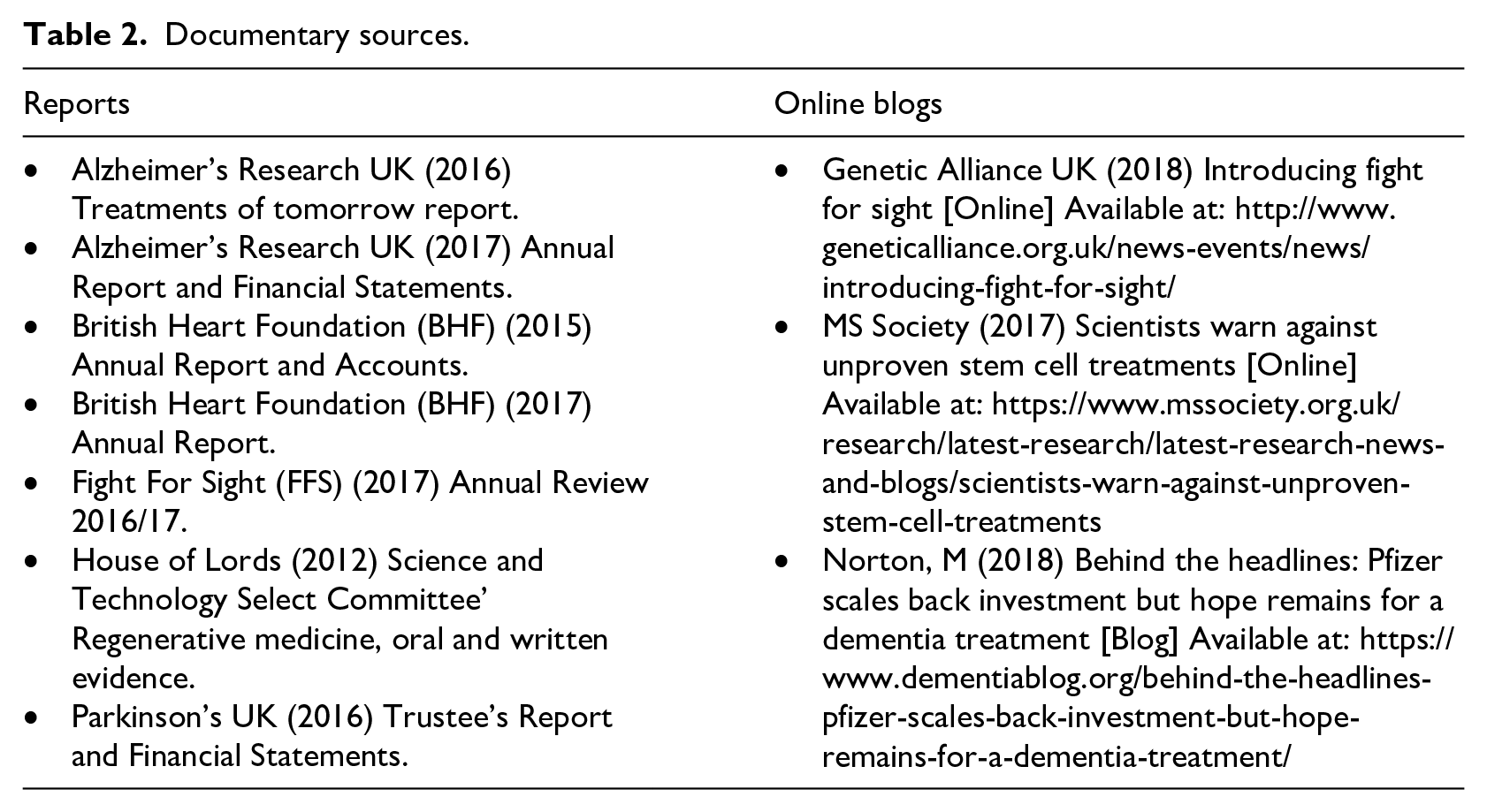
Initial contact was made via email, which detailed the outline of the overall project and a participant information sheet which explained their participation. On acceptance of the interview, formal consent was gained to audio record the interviews. The interviews were semi-structured and a list of specific questions guided each interview. The interviews explored the participant’s perspectives of RM, focusing on the challenges and areas of promise within their field. The participants all had extensive scientific and clinical knowledge of their respective fields. In order to protect the anonymity of participants in this study, each participant has been ascribed a pseudonym (e.g. Participant 1). Transcripts of the interviews were coded using Nvivo10 software to identify themes (see Supplemental material). Ethics approval for data collection was obtained from the appropriate institutional ethics review board, and written informed consent was obtained from all participants. The interview data are augmented by a variety of documentary sources of charities, including annual reports and online blogs, to triangulate and strengthen our analysis. These documentary sources have been referenced in the findings section by author name and year of publication (e.g. Parkinson’s UK, 2016), and are listed in Table 2.
Documentary sources.
We now proceed to present our interview-based and documentary findings, under three primary themes, before offering a concluding summary and discussion of the substantive and conceptual significance of the study.
4. Analysis
In the following section, we present the three main themes which we derived from the data, framed by the notion of technoscientific imaginaries.
Expectations work
Managing and moderating media expectations
In this section, we explore the ways in which research charities are engaged in a form of expectation management in how they respond to the media’s typical rhetoric of promise.
The way in which the mainstream media report RM presents a challenge for research charities. Participants agreed that more often than not, media reporting takes a positive stance when describing technological advances for patients, which was generally characterised by our interviewees as ‘hype’. For them, promissory hype narratives were defined by a time span, more specifically imminent futures and therapies closely approaching the clinic. Time concepts are used by the media as a device to create buzz and hype: There are people who always ask the question ‘how long?’. The question people always ask is, as I say when there’s this great, big news article and lots of fanfare, they say, ‘What does this mean for me? How long until I get it?’ . . . And it is always frustrating when you have to say to people; ‘This looks great now, but we’re still a long way off. It’s still ten, fifteen years’, and I think that we’ve learned not to put a time scale on things. (Participant 6)
Participants described the ways in which success stories about potential advancements often mislead the public by overemphasising the benefits, underplaying the risks and causing confusion around actual current progress. As a result, research charities respond to public enquires, clarifying facts and information. This ‘expectation work’ is essentially the tempering of hype for patients, and instead relaying ‘corrected’ information. This expectation work appears to be more pertinent for patients with life-threatening diseases who are desperate for a cure, such as those with neurological diseases: So we’ve got a helpline. They would receive lots of calls if there was something in, say, The Daily Mail . . . and then we’d talk to a lot of people who would have misunderstood or been misled . . . We would make sure we put something on our website explaining our view of what was discussed to help people understand it properly. (Participant 1) It’s important that people understand that we’re making progress in research . . . but it’s just the way it sometimes gets presented, I think, means that it’s good if organisations such as ours can help try and, you know, temper some of that. (Participant 3)
This type of ‘correcting’ work also extends to how charities respond to public enquiries about clinics offering unproven treatments. On their website, MS Society reveals how their expert scientists are warning the public against unproven stem cell treatments: We’ve had a number of people call us about clinics offering false hope with ‘scam treatments’. It can be hard to tell what’s backed up by proper science and what are just empty promises. We’re really concerned about unproven stem cell treatments being marketed to people with MS. They raise unrealistic hopes . . . and that just isn’t right. (MS Society, 2017)
Alongside the impact hyped media claims have on the public, there is also recognition of the impact for the research community, and more specifically on the development of new treatments. Recent news of a new clinical cell transplantation trial for Parkinson’s disease raised hopes in the patient community (Barker et al., 2016). However, comment from a scientific expert from Parkinson’s UK warns of the implications of not being cautious: As with many such exciting news items, one should react with caution. Especially since the outcome of this trial can affect the development of other stem cell programmes moving towards clinical trials. (Barker et al., 2016)
The perception of the media as a risk to realistic expectations is further exemplified by how charities perceive themselves to be under public scrutiny and attack. In a message from the British Heart Foundation’s (BHF) chairman in 2017, he addresses this challenging context, highlighting the ‘unprecedented media attacks on the charity sector’ (BHF, 2017). Parkinson’s UK also addresses this issue: Charities are rightly now under increased public scrutiny to show how we channel generous donations into positive change. While we forge new paths, we must also apply renewed energy to key areas such as close compliance with fundraising regulations, vigilant protection of people’s information and prudent management of our finances. (Parkinson’s UK, 2016)
One way such risk is mitigated is how charities choose to interact with the media. Some are actively engaged in maintaining a relationship with the media for a number of purposes, one of which is to maintain their own position as a trusted source of information. Also, this is a mechanism to share with the public experiences of the disease and raise awareness of fundraising efforts: We continue to provide expert comment for the media, maintaining our position as a go-to trusted resource on new developments in dementia research and policy. By talking to journalists about their experiences, our media volunteers share the devastating impact of the condition on people’s lives, while our fundraisers captured imaginations by sharing their stories of the astonishing lengths they reached in support of our cause. (Alzheimer’s Research UK, 2017)
The importance of informing the public of perceived important advances via the media was identified within both the interviews and reports (BHF, 2015, 2017; FFS, 2017). However, managing public expectations was perceived to be a delicate task. For one participant, careful consideration is placed on how new discoveries or therapies are communicated in a balanced way: Yes, we proactively talk about things in the media but we have to do it in a very balanced way. We have to be careful because there’s a certain control that we lose when we start talking to the media about things because they will listen to us but they can go away and write whatever headline they want and we need to not talk about things too much before we really know the answer. (Participant 10)
The lexicon surrounding emotive words such as ‘cure’ was highlighted by one participant, and the challenges this word evokes in the research setting dealing with many practical challenges. Discrepancies between perceived timescales of potential therapies and of research and clinical trials become obvious: Quite often, what happens is that an article might be published in the mainstream press which will say something like there are going to be trials for stem cell therapy and how exciting it all is. Unfortunately, they also tend to say things like, ‘This is going to cure Huntington’s disease’. Of course, usually by that stage, the studies are up and running and the participants have been selected and what people don’t get very easily is information about where studies are taking place and whether or not they can participate in them. (Participant 5)
While it is not the primary purpose of these organisations, it is apparent that expectation management work has become a major part of their role. They are mediators who take on a ‘correcting role’ reframing public expectations. Hence, research charities can be considered as being in a dual relationship with the media, trying to maintain a delicate balance between two contrasting effects. On the one hand, research charities require a certain amount of publicity in order to maintain public interest in and gather funding for the illness they represent, but as exemplified here, some forms of publicity can have a detrimental effect if not moderated or ‘corrected’.
Specifying appropriate disease-specific expectations for RM
RM has been framed in public media and in government policy as a panacea for many illnesses, for example, being deemed one of the ‘Eight great technologies’ by the UK government in 2014 (Gov.uk, 2014). In this light, imaginaries of the realistic applicability of RM to particular diseases have become a further dimension of charities’ mediation of public and policy expectations. This theme refers to the way in which RM is deemed appropriate within different disease areas. Scientific evidence demonstrates that the applicability of RM techniques will differ widely depending on the specific disease area. For four interviewees, the more complex disease areas posed specific challenges which were deemed to be fundamentally incompatible with RM techniques. One disease area which was considered appropriate was type 1 diabetes, because of the science and biology of the disease: I think with type 1 there is absolutely no doubt that by replacing these beta cells you are going to cure the disease, as long as you handle the autoimmune bit. In that respect, it’s a perfect disease for regenerative medicine because you absolutely know your cells and you know that if you put them in they’re going to have an effect. It’s a bit like with, let’s say with Parkinson’s, the dopamine producing cells, it’s known that if you were able to replace those cells you would actually be able to have an effect on the disease. (Participant 6)
In contrast was the perspective that RM is inappropriate for dementia, due to the complexity surrounding the condition. There is an acknowledgement of other and ‘easier’ disease areas such as Parkinson’s: What I don’t see, and I don’t think anybody sees, for some little while, is that technology translating to therapies based on regenerative medicine but rather therapies that have been developed using those cellular models. I think Parkinson’s is the easiest, possibly a little bit different and I think we’re some way off that in Alzheimer’s and other dementias. (Participant 3)
Clinical trials were also identified as another barrier for one participant, especially in relation to how they can be difficult to construct for some conditions: There’s a barrier at the moment to these kinds of trials that are testing regenerative medicine. How do you actually know the brain is regenerating? How do you know if you are slowing down Parkinson’s? How do you really design a study that can prove that? That’s a big barrier, so there is a horse and cart problem; we’ve got the potential drugs but we don’t have a really good way to test them and know if they work or not. (Participant 1)
The failure of clinical trials was also characterised by disappointment and a reminder of the difficult process of drug development: Millions worldwide were hit by disappointment in late 2016 when a phase III clinical trial of the drug Solanezumab, developed by Eli Lilly, failed to show benefits for people with Alzheimer’s disease. Many had high hopes for the treatment, and the trial results were a reminder of the many challenges of developing a drug for this complex disease. (Alzheimer’s Research UK, 2017)
In these examples, the form and strength of expectation is related to the nature of the disease. One relevant biological aspect is the simplicity or complexity of the disease (focal or systemic), defining its suitability for RM approaches. Here, complex disease areas are considered to be mismatched with the techniques of current RM.
The time horizon of possible advancements was also significant. Especially in the complex disease areas, the potential of RM was framed in terms of the future, earmarked as being a ‘long way off’: There’s plenty to more to be learned about the pathologies themselves, and I think there’s certainly not that much known about adult neurogenesis in humans, so those are, sort of, two, I think, reasonably big knowledge gaps. So you either want to simulate neurogenesis, which could possibly help, and if that would come under regenerative medicine then that is possible. I mean it’s a very tricky area, and I personally think it’s far too premature to be thinking too far ahead. (Participant 3) I think the model for treating Huntington’s disease going forward is comparable to HIV in the sense that we aren’t going to cure this disease any time soon and that would require the ability to massively manipulate the genetics of an individual and remove the faulty element of the gene and I think some day that will happen, but it’s certainly not in the near future. (Participant 5)
For one participant, the excitement that surrounds the potential of RM for Parkinson’s disease exists directly alongside cynicism about its appropriateness due to the lack of results to show efficacy: The level of excitement and cynicism is different for each individual. So our trial is a good example, like some neurologists and clinicians who see people with Parkinson’s might have advised their patients to think about taking part but some of them might say, ‘I wouldn’t bother, because I don’t think it’s going to work’, but they have quite diametrically opposed views because a lot of trials have been done and failed. (Participant 1)
This notion of prematurity was also extended to the complexities surrounding future translation and adoption into the health service. Within the current context of accelerated access (Wainwright et al., 2016), RM techniques/approaches were mostly perceived as being at an early stage. Potential future modelling of practical scenarios of adoption is considered too early. Interviewees linked disease appropriateness to clinical adoption issues, suggesting that for some disease areas National Health Service (NHS) adoption is simply too far away; I think it’s good to be thinking about NHS uptake of some of this innovation. I just don’t know if it’s too premature . . . I think there is great potential in this area, and I think there’s probably a government push to make the UK a leader in this, which is probably good because we have some excellent science here. Is it too soon to be mapping pathways for adoption by the NHS if we are still trying to work out some of the basic science? (Participant 3)
Overall, we see in this section the importance of disease applicability as a key dimension of expectations for RM. Disease charity representatives show reasoning that revolves around considerations first of biological science, and also of issues of trialling, imagined timescales, and clinical adoption. They consider their own particular disease focus in the context of understanding the broader aspirational imaginaries of RM that circulate in policy communities and society at large. Their mediating expectations management work is informed by detailed technical understandings formulated within technoscientific imaginaries that balance their view of public and patient concerns with their own scientific insight.
Scenario management
Scenario management to maintain possibilities for future success in the face of obstacles
This theme concerns some of the practical and theoretical developments which the participants envisioned if RM were to succeed in the future. Here, we see evidence of a discourse of challenges, problems, barriers, and ‘issues’ that point towards the ‘obstacle model’ referred to in our conceptual introduction (Rommetveit and Wynne, 2017), and the research charities’ efforts to preserve and protect scenarios for RM in the face of perceived threats. We found that these threats included the identification of more clinicians at research level, the improvement of the current healthcare infrastructure to support increasingly expensive treatments, and increased capacity for research within the NHS: We have had some real leaders in the field, and of course they’re going to retire at some point. There’s a slight worry about succession. We need more clinicians thinking about dementia research because I think without the guidance of people who are experienced with a complex set of illnesses, the basic research could also go down blind alleys. (Participant 3) The challenge then is providing the infrastructure within the current health service. At the moment we’re struggling as it is and if they think that £3,000, £5,000 per treatment 12 times a year for a cancer therapy is a lot, it’s nothing like what’s coming and not only for our disease but for lots of others. (Participant 7)
Practical issues are also raised by the BHF in their written evidence to the Science and Technology Select Committee (House of Lords, 2012). They highlight the importance of addressing specific challenges within the NHS related to bureaucracy, incentivisation of clinical research and the effective adoption of innovative therapies (House of Lords, 2012). The BHF also identify the barriers to ‘translation’ in the way in which the NHS is conventionally seen as slow to adopt new technologies: Without a ring fenced budget aimed at adopting new technologies into NHS practice, we believe that it will be difficult within the current financial climate for any new technology to be introduced . . . New technologies often begin by costing extra, but as clinical experience helps to refine these technologies, they can save money for the NHS over the long term. (House of Lords, 2012)
Alzheimer’s Research UK also identify a number of high-level policy challenges in ensuring proven disease-modifying treatments reach patients, which include system challenges (limited data on health outcomes and cost), affordability challenges (increased investment into infrastructure, equipment, staff and training) and cultural challenges (low uptake of innovation, need for collaboration across clinical disciplines (Alzheimer’s Research UK, 2016).
In addition to engagement with high-level biomedical policy, ‘de-risking’ was also identified as an issue in maintaining practical scenarios for future therapies, to encourage potential investment by the commercial sector, acknowledging the importance of perceived threat and the consequences of this for clinical translation. Perceived risks generate uncertain expectations, and our interviews suggest another type of scenario management work in how research charities may try to pre-empt cautious attitudes of the commercial sector and reframe their research accordingly: Well I think it’s been a barrier for a long time and we think it’s led to pharmaceutical companies being less likely to invest in Parkinson’s research because it’s so hard to prove a new therapy works and is better than the things we have at the moment. So if we can change that balance, make it less risky then, hopefully, that would bring new investment and new trials and more drive to find regenerative therapies for Parkinson’s. (Participant 10)
There is also evidence to suggest that charities are attempting to resolve this issue of confidence by being active in bridging the (funding) gap between drug development research and clinical trials. Comments from the BHF reveal such ‘de-risking’, highlighting a scenario that maintains new drugs and treatments as palatable for the fragile environment of pharmaceutical investment, and playing a mediating role by actually funding early-stage research: Traditionally the BHF has funded laboratory scientists in universities to look at molecular mechanisms. If scientists then came up with what looked like a promising new target for a drug or even a molecule that could be a drug itself then by and large we’ve expected the drug industry to then move in and pay for the research that develops that through to a drug. The problem with that is industry won’t pay for that research until it’s pretty certain that it’s going to produce an effective and safe drug. So, it’s clear to us that we have to bridge that gap. (Participant 8)
Similarly, FFS and Alzheimer’s Research UK also refer to such de-risking enactments within the context of their charities: Being patient-focused, Fight for Sight is able to fund early stage research, de-risking it for others by providing support at proof-of-concept stage. Consequently, significant funding that is necessary to take new drugs through the pipeline to the clinic can be leveraged once there are successes to build on. (Genetic Alliance UK, 2018) At Alzheimer’s Research UK, we work to bridge the gap between government, academia and pharmaceutical companies in the drug discovery process. (Norton, 2018)
Scenarios of the future success of RM were thus also framed around funding and underfunding. For one participant, underfunding was an obstacle within Alzheimer’s, concerning a shortage of experts, in turn related to a perception that the disease area has become an unappealing field to work in: Not many people work in the field, so it’s been seen as an unattractive area to work in, therefore not many applications for funding are made, and therefore not much funding goes into it. You know, a lot of the discussions that we’ve been having with other funders, including government is, can you just turn a tap on if you want to fund more in an area? . . . So there are precedents for saying, ‘Look, not many people are working on this, but we’ve got to make sure they do and we’ll get results if we throw money at it’. (Participant 3)
Underfunding was also a prominent issue at clinical trial level. One participant identified the impact of lack of funding for clinical trials for Huntington’s disease while another identified trial underfunding largely due to past failure of clinical trials: I think people gradually realised that there were issues with funding, there was not enough money to spend on the trials that were needed and it was not effectively coordinated on an international basis either. (Participant 5) If you look at why the trials may have failed, there are a number of reasons which I think one can rationally argue without saying, ‘Well we don’t know anything and we’ll never make any progress’, which I think is the view of some people. So overcoming that perception . . . You know, if we get some success and say, ‘there is a pipeline, there are drugs in phase three’, and as we learn more I think we have to have some optimism that we will get some success. (Participant 3)
An ‘obstacle model’ of technoscientific imaginaries and the charities’ mediating position in attempting to preserve positive scenarios are evident in the above statements and the evidence of their practical interventions, as the charities seek to maintain potential scenarios for effective therapies in the face of funding, staffing and investment challenges.
5. Discussion
In this article, we have drawn on sociological and STS concepts of technoscientific imaginaries, and specifically those that examine biomedical expectations and the roles of ‘promissory organisations’. We have developed the notion of scenario management, elaborating ‘hope’ as being mobilised through discursive and material strategies, to further explore the intermediary roles and expectations work that disease research charities enact. We showed how these compare and sometimes come into conflict with expectations produced by the media and commercial actors, how they work to preserve positive potential innovation pathways, and so play a performative role in shaping the future of the field. Much STS scholarship on expectations has had a tendency to focus on particular technologies in a way that highlights processes of expectation and hope-building and disappointment across the different participating stakeholder actors, according relatively less attention to the specific roles and contributions of individual types of actors (TASM, 2006). Here, we contribute to the field by highlighting empirically the various strategic mediating interventions of disease research charities as one particular, neglected, type of technoscientific and biomedical actor.
We have suggested that the technoscientific imaginaries of disease research charities in their mediating roles can take both corrective and protective forms, managing hyped expectations and maintaining pathways of hope in the face of obstacles. We have shown that hype expectations produced by the media, set in the present, are modulated by research charities engaging in ‘expectations management work’, reframing messages for patient groups, and that this is embodied within their organisational practices and public media presence. The charities reconstruct hype narratives and thus shape the landscape of patient perceptions of RM progress. Performative organisations can mobilise the future of the field (van Merkerk and Robinson, 2006), but in this instance they have a more subtle role in tempering patient expectations because hype claims are seen to be misleading and damaging. The literature shows disappointment can occur following raised expectations which can lead to withdrawal from the field (Brown and Michael, 2003). Yet, at the same time, we show that research charities are also involved in strategies aimed at maintaining some optimism in the field by reframing stakeholders’ imaginaries in terms of what they regard as being more realistic scientific scenarios about its promise, aiming to sustain a positive prospect in the long term and so protect its reputation. Their involvement in research funding further reinforces their perspective and commitment that this is an area worth pursuing and protecting against potential collapse of trust.
Much of the charities’ discursive work takes place in the social spaces of the news media. Media and publicity departments maintain a constant supply of news and press releases which they publish on their websites. In the case of RM and what we have called scenario management, we note that the charities are sometimes able to collaborate positively with both companies and public research agencies to advance research priorities. Such developments are typically diffused to news media and, in particular, biomedical research policy communities. For example, Parkinson’s UK recently announced a £6 million grant to investigate brain cell death as precursor to new drug development with a large European public-private consortium, publicised via a press release (Parkinson’s UK, 2019). Such press releases will often be re-presented and augmented with the researchers’ voice in medical media, as in this case (Pharmaceutical-technology.com, 2019). The extent to which charities’ news media departments might seek to shape the media presentation of researchers that they support is an interesting question which would require further exploration.
Future hope-fuelled expectations such as those diffused through specialised news media are promissory in conveying potential materialisations of RM as a clinical field delivering novel therapies for specific disease areas. This type of expectation acts to define more limited but perceived realistic boundaries for specific disease areas. Precisely because of this specification process, a kind of hierarchical ‘triaging’ of expectations, the mediating work of such promissory expectations can be considered to be more effective at mobilising certain fields of clinical application, rather than others, as being the most appropriate and likely to succeed on scientific grounds, thus maintaining the research endeavour.
Stakeholders’ recognition of the limits and pitfalls facing the RM field is evident. It is here that we see the detail of the work of the charities in discursively and substantively preserving and protecting potential RM pathways. The charities’ reasoning and funding interventions include concerns about pharmaceutical investment and the scientific workforce, seen to be responsive to failures and obstacles in basic research. Research charities are aware that disappointed expectations can lead to subsequent withdrawal of others’ funding and support. Hence, some articulate a mediating role in which their own initiatives of bridging the gap between basic academic research and developments of sufficient promise are designed to bolster confidence and attract pharmaceutical company investment.
Our findings show that the charities assume a broadly defined, multidimensional intermediary position, negotiating pathways between public media, patients, policymakers, academia, pharmaceutical industry and investors. From this position, they aim to influence public and patient expectations, are aware of pharmaceutical industry attitudes, and can feed their knowledge into their own research agendas and priorities. This intermediary role is comparable to the industry consultants analysed by Pollock and Williams (2010), and like them, their expectations work and scenario maintenance work have a variety of ‘uneven’ influences, not simply promising positive advancements, but supporting pathways between scientific innovation and the clinic, taking specific challenges into account. Their roles thus support RM’s precarious ‘ongoing emergence’ (Morrison, 2012). Their interventions acknowledge that the field is susceptible to technological changes, funding and expectations of stakeholders, that there is no endpoint in sight and that ‘a range of stages are possible such as failure, fragmentation and setbacks’ (Morrison, 2012: 7) as well as positive developments. The findings from this study show the extent to which intermediary organisations such as research charities are engaged in complex negotiation of the field in their journey in securing and protecting realistic progress of RM.
In conclusion, we know from the literature that we have drawn on that future imaginaries of success can be instrumental to the development of RM among actor groups, including clinicians, researchers, patients and other stakeholders. We have shown how disease research charities adopt a multidimensional, intermediary position mobilising different dynamics, exhibited in moderating ‘expectations work’ coupled with positive scenario maintenance work. As with other technological fields that negotiate an innovative potential, RM will continuously be characterised by narratives of promise and expectation, and by challenges and setbacks. How these develop over time across different stakeholders and institutions has a material impact on how research agendas are shaped, how investment decisions are made and how clinical prospects for effective therapies are evaluated and enacted.
Supplemental Material
Supplementary_material_Duggal_and_Faulkner_in_Public_Understanding_of_Science – Supplemental material for Promissory and protective imaginaries of regenerative medicine: Expectations work and scenario maintenance of disease research charities in the United Kingdom
Supplemental material, Supplementary_material_Duggal_and_Faulkner_in_Public_Understanding_of_Science for Promissory and protective imaginaries of regenerative medicine: Expectations work and scenario maintenance of disease research charities in the United Kingdom by Sandhya Duggal and Alex Faulkner in Public Understanding of Science
Footnotes
Acknowledgements
The authors thank Professor Andrew Webster for comments on an early draft of the paper, as well as two anonymous peer reviewers, and the journal editors for valuable comments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research formed part of the REGenableMED project ‘Regenerative medicine and its development and implementation: an analysis of emergent value systems and health service readiness’, supported by the UK Economic and Social Research Council (ESRC) (Grant No. ES/L002779/1).
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.