
Abstract
In Romania, as elsewhere, there is persistent controversy surrounding homeopathy wherein various parties try to draw the boundaries of legitimate medical practice. The literature on complementary and alternative medicine features little discussion on the temporal dimensions of controversies surrounding these therapies, focusing mainly on the temporalities of the lived experience of treatment. Yet time is a powerful resource for challenging and gaining legitimacy. In order to capture the use of time as a resource for legitimating or contesting homeopathy, we advance the theory of time work by examining the rhetorical role of different temporalities in this dispute. We find that proponents and users of homeopathy appeal to temporal properties of treatment, such as the longer duration of consultation, and of healing, namely, a specific sequence of symptoms and reactions, stories of failed biomedical treatments followed by successful homeopathic interventions, and stories of durable efficacy. Critics invoke the temporal properties of science, especially a cumulative record of failed attempts to prove homeopathic efficacy beyond placebo, or to causally account for its putative effects. Argumentative time work also involves manipulation of temporal modalities, in which homeopathy is legitimized both through continuity with the past and through breaking away from the past, with an eye to a promised future. At the same time, critics of homeopathy invoke temporal modalities to cast homeopathy as a relic of an unscientific past. This research illustrates the value of "argumentative time work" as a conceptual tool in examining public controversies.
Introduction
In this article, we examine how homeopathy, a form of “complementary/alternative” medicine (CAM), has been legitimized through temporal tactics in contemporary Romania where it enjoys some popularity among patients, following a worldwide trend. In contrast to other countries (e.g., UK and Germany), it can be practiced only by conventional physicians as an officially recognized “medical competence” and only in the private sector since it is not included in the public health insurance system.
Worldwide, there is persistent controversy surrounding homeopathy wherein various parties try to draw the boundaries of legitimate medical practice. This is a dispute that started in the beginning of the 19th century when Samuel Hahnemann, the German physician who invented homeopathy, proposed its therapeutic principles as an alternative to the conventional medicine of the time. From then on, irrespective of the degree of legitimacy and official recognition that homeopathy has reached in various countries, it has always been a controversial subject due to its infinitesimal dilutions and its scientific implausibility.
In our approach, we avoid taking sides on matters of medical efficacy. Instead, we offer a sociological perspective on how homeopathy gained legitimacy in Romania, by scrutinizing a specific resource of legitimation: manipulation of temporal characteristics, or time work, as conceptualized by Flaherty (2003). In the next section, we review scholarly attention to the legitimacy of CAM practices and argue for the relevance of time work in our efforts to understand such controversies. We then proceed to a brief description of our research methods, followed by a discussion of our findings and conclusions.
Time work as tactics of cultural legitimation
Legitimacy is the result of a process whereby cultural arrangements are “explained and justified” (Berger and Luckmann, 1966: 61). Therefore, we offer a central place to justifications as an analytical concept. In contrast to a psychological understanding of justifications as rationalizations, we take inspiration from Boltanski and Thévenot’s (2006) work and see justifications as ways of placing value on people and things. This is a fruitful analytical window for approaching the temporal dimensions of cultural legitimacy or how time is used as a justificatory resource for gaining popular support in controversies. We combine different but convergent theoretical strands inspired by French and North American pragmatists. In our analysis, we view controversies as arenas for enacting and transforming public issues, and we examine them as objects of study per se rather than as symptoms of deeper social structures.
The co-existence of competing medical therapies in a single country presents us with an opportunity for inquiry into processes of legitimation. These processes may take different paths depending on biomedicine’s institutional domination and its relationships with what in the West are considered “alternative therapies” (e.g., Ayurveda in India is recognized as a nationally standardized and accredited therapy). Historically, medical pluralism converges with European colonialism, and we are currently living in a globalized world in which different health ideologies are either bypassed or meshed through various translations. Hence, contemporary Asians may aspire to be “modern individualists” while Westerners may strive toward “holism” and being in touch with nature (Narainda et al., 2014: 6). As Cloatre (2019) points out, we are witnessing conflict between divergent visions of modernity in which 19th century notions of progress and unilinear time are contested by contemporary health movements. Nonetheless, regulatory systems still impose biomedicine’s temporalities on other forms of therapy.
Cobb (1977) proposes the notion of pluralistic legitimation based on a case study of chiropractic in the USA. She conceptualizes legitimation in terms of four components: (1) legal sanctions (including licensure laws, government funding, and academic sanctions); (2) professionalization (taking into consideration knowledge monopoly, service orientation, and work autonomy); (3) social movements (Cobb notes the importance of the ecological movement and the health food movement in fostering popular appeal for that which is “natural”); and (4) popular demand. This multifaceted model has also influenced Cant and Sharma’s (1999: 131) exploration of medical pluralism in the West, since “the boundaries of what is legitimate or dissident are always mediated by the relevant professional groups, the public, and the politicians."
In contrast to these pluralist models of legitimacy, previous studies of CAM are split as a rule between either an emphasis on practitioners’ perspectives and official regulations or patients’ motives and experiences of use, making salient the difference between professional legitimation and cultural legitimation. Studies of professional legitimation focus on how CAM practitioners appeal to the mainstream medical profession or official authorities for access to resources, statutory self-regulation, and integration in academic or biomedical settings. These efforts may entail adding medical knowledge to the training for CAM therapy, promoting peer-reviewed research or clinical trials, establishing professional standards and qualifications, and introducing CAM practices to academic institutions (Degele, 2005; Freidin, 2017; Givati and Hatton, 2015; Rughiniş et al., 2017; Wahlberg, 2007; Welsh et al., 2004), processes that point to the role of formalizations as performative devices (Matei and Preda, 2018).
Practitioners may be engaged in what Givati (2015) calls performing pragmatic holism, which involves moving strategically between narrowed or expanded versions of holistic therapy in relation to different audiences and settings, incorporating references to scientific evidence, or just emphasizing the integrative and individualizing aspects of holism. These tactics lead to the general conclusion that, in order to gain institutional legitimacy, CAM therapies must align themselves with biomedical standards. Consequently, original concepts and practices may have to be abandoned or compromised. These revisions may be rejected by some proponents leading to internal factions (Degele, 2005; Welsh et al., 2004), or they may generate epistemic and moral stress (Brosnan and Cribb, 2019). Other studies investigate processes of delegitimisation, which entail the use of rhetorical strategies in public discourse for denigrating CAM practices and defending the boundaries of science by means of contrasts such as academic integrity versus profit, rationality versus faith, or logic versus magic (Caldwell, 2017; Lewis, 2019).
Studies of popular support for CAM therapies show that this is usually the result of dissatisfaction with biomedicine’s therapeutic outcomes, frustration with the physician–patient relationship (Barry, 2006; Danell, 2015; Gale, 2014), or cultural congruence with the popularity of “natural” and “lifestyle” medicine (Douglas, 1994; Freidin and Ballesteros, 2015; Raffaetà, 2013; Sointu, 2012; Whitaker, 2003). In contrast to biomedicine, CAM therapies usually have weak institutional legitimation in terms of scientific evidence and statutory recognition (Sointu, 2012). Nevertheless, they can gain various degrees of legitimacy due to cultural congruence, namely, an overlap between the ideas embedded in a medical practice and widespread cultural values concerning the body, health, and subjectivity. Other studies look at the attractiveness of CAM temporalities, positioned in contrast to the short-term quick fix of biomedicine by addressing the deep-seated, long-term causes of disease (Ecks, 2014; Lindquist, 2005).
We build on these insights by defining temporality as a resource for cultural legitimation and examine the role of time work in the controversy surrounding homeopathy. In his initial formulation of this concept, Flaherty (2003) describes how people modify various dimensions of time in order to bring about desired forms of temporal experience, thereby accommodating or resisting the external and constraining circumstances. He calls these efforts time work, drawing inspiration from the ethnomethodological perspective on social interaction as “reality work” (Mehan and Wood, 1975: 113). He demonstrates that people seek or avoid certain temporal experiences along six dimensions: duration, frequency, sequence, timing, allocation, and taking time. For example, someone placed in a situation in which time is perceived as passing slowly may try to accelerate temporal experience through various strategies, such as avoiding attention to a clock or calendar, controlling in this way the lived duration of an interval. Although this temporal creativity may take various forms in everyday life, Flaherty notes that it is constrained by cultural prescriptions, organizational logics, and relational obligations.
Our approach to time work departs from a narrow focus on temporal experience and examines how time, in its various dimensions, may be manipulated in situations of dispute. This treatment enables us to elaborate on the concept of temporal agency since, in our analysis, it assumes the form of rhetoric from various actors who argue for or against homeopathy. The time work that we examine is of an argumentative type: we investigate how individuals and groups invoke time or temporal experience when they try to make a case for or against homeopathy. Rhetorical efforts at justification or critique often involve time work, because various dimensions of temporality are made relevant when one attempts to attack, defend, persuade, and gain allies. The temporal creativity in our study concerns discursive attempts to justify or explain one’s position or view of something. We find that, through argumentative time work, the advocates for homeopathy assert cultural congruence between their practices and general values concerning temporality in healthcare.
Research methods
For this article, we draw on fieldwork undertaken by the first author for her doctoral thesis and supervised by the second author from March 2016 to July 2018 in two Romanian cities, Bucharest and Piatra Neamţ, and in online environments. The research design has been approved by the ethics committee of the Faculty of Sociology and Social Work, University of Bucharest. We chose to do research in Bucharest because, according to previous studies, it is the city that has the largest number of consumers of homeopathy and, more generally, of “green consumption.” Bucharest is the capital and the most economically developed Romanian city, offering a wide range of medical services in the private and public sectors. Given the huge socioeconomic differences between Bucharest and other urban areas, we chose also to do research in the first author’s native city, Piatra Neamţ, a medium-sized locality in the northeast, one of the most economically depressed regions of Romania.
The fieldwork involved interviews with patients and homeopathic practitioners, observation of homeopathic consultations, and attendance at homeopathic conferences. Patients (N = 20) were recruited by means of snowball sampling procedures through which researchers’ acquaintances and interviewees made referrals to other persons that undergo homeopathic treatment. The first author recorded observations at two national conferences (the 2016 National Congress of Homeopathy held in Braşov and the 2016 National Congress of Integrative Medicine held in Bucharest), both with public access, and she also attended six workshops organized monthly by the Romanian Society for Homeopathy (SRH), to which she was granted access by the Society’s secretary. During these events, she met homeopaths who were willing to participate in her research, either by agreeing to be interviewed (N = 6), or agreeing to have their consultations witnessed (N = 3). Of the latter, one was a lecturer at homeopathic postgraduate courses, so he was used to having students in his office observing the consultations. Another homeopath invited the first author to participate in a proving (a testing for a homeopathic remedy) and accepted the first author’s presence at some of her consultations, with patients’ approval. The first author also observed three of her own consultations and one of an acquaintance that agreed to her presence. In addition, some audio recordings of consultations were made available as pedagogic material during the workshops (with patients’ approval). A second way we recruited homeopaths for interviews was to send invitations via email, but only four of our 20 invitations were accepted. When we discussed this reluctance with one of them, he commented that due to public denunciations of homeopathy, many practitioners are unwilling to cooperate with any form of interviewing.
Our research methods include the content analysis of various documents. Given that patients and homeopathic practitioners made frequent references to the mass media (as sources for medical information, therapeutic recommendations, and health-related shopping), we began to examine how homeopathy is depicted in diverse offline and online formats: practitioner webpages, CAM blogs, conventional medicine sites, homeopathic association webpages, social media postings, articles in the popular press (newspapers and news magazines), and television interviews.
These heterogeneous materials (interview transcripts, field notes, and documents) were converted into texts and examined through iterative processes of thematic analysis (Joffe, 2011). We inspected the entire corpus of data by looking for instances of time work as conceptualized by Flaherty (2003), but with a focus on discourse and justification—that is, rhetorical efforts at the manipulation of temporal dimensions in order to account for homeopathy’s efficacy. Our analysis benefitted from in-depth discussions among the co-authors, deriving value from our distinctive personal assessments of, and experiences with, homeopathy. Typically, the second author was more skeptical concerning its therapeutic effectiveness and conceptual soundness, while the other two authors were more likely to consider the shortcomings of institutionalized biomedicine and the virtues of therapeutic diversity. In light of these balanced orientations, we abjure any particular standpoint and study legitimation as a process driven by its own social logic. We examined time work symmetrically for the legitimation and denunciation of homeopathy, but the limited scope of this article does not permit the presentation of both sides of this debate.
Dimensions, tactics, and vocabularies of worth in justificatory time work.
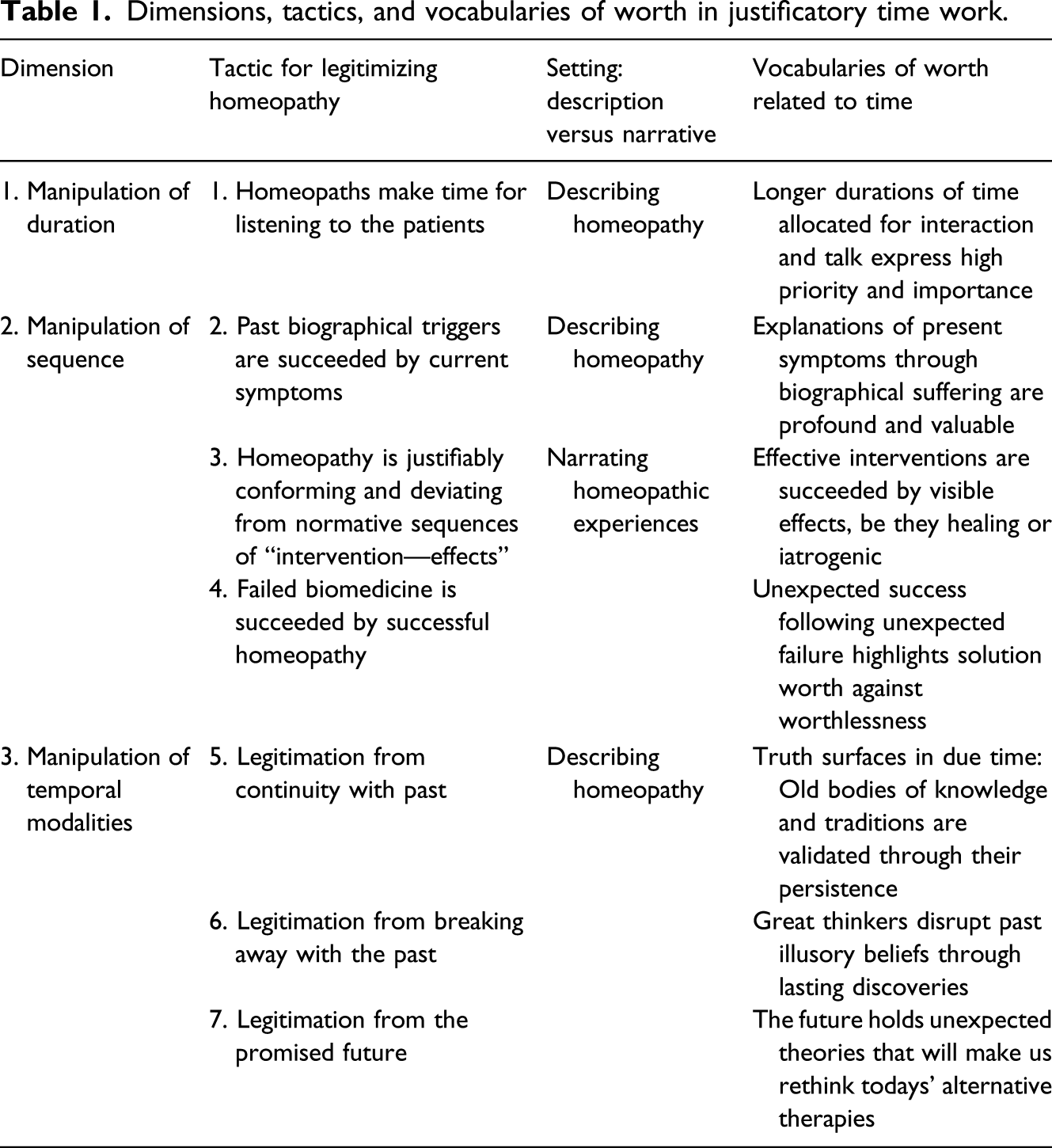
First, proponents of homeopathy may justify their practice in public disputes as a medical encounter that is more patient oriented due to the longer duration of medical interaction. They appeal to a generally shared vocabulary of longer durations as a code for expressing high priority and importance (Zerubavel, 1987), a shared expectation of truth emerging in due time, and trust placed in long used and thus proven remedies. Second, proponents of homeopathy may manipulate sequence in three different ways that resonate with an understanding of health as something that must be reached after sickness, through a meaningful narrative of healing. We have also identified a third dimension of time work that is not included in Flaherty’s original conceptualization: the manipulation of temporal modalities. In the public presentation of homeopathy, its proponents resort to the temporal modalities of past and future, simultaneously arguing that homeopathy is a century-old medical practice and appealing to tradition as a source of legitimacy, while also highlighting its rupture of contemporary medical conventions, thereby arguing for a charismatic source of novel legitimacy. Thus, argumentative time work is also orientated to the future, invoking uncertainties to be resolved through scientific progress.
Taken together, we argue that these manipulations of different temporal dimensions constitute time work tactics through which proponents of homeopathy gain cultural legitimacy by appealing to a generally shared understanding of healing in time and history.
Manipulation of duration: Making time for listening
In homeopathy, there are two kinds of consultations: case taking and follow-up. A case taking is the first encounter between a homeopath and a patient, and it follows a format in which homeopaths ask a variety of detailed questions about a patient’s current complaints, medical history, and mental and emotional characteristics. The follow-up consultations are usually shorter, and homeopaths ask questions related to changes in symptomatology that patients have felt during treatment. The case takings that we observed lasted from 66 to 120 minutes, while the follow-ups lasted from 16 to 30 minutes.
Homeopathy accounts that circulate in the online space and face-to-face conversations refer to this normative temporality. Thus, the expertise of a homeopath who dedicates a restricted time for the consultation is questioned. For example, recounting their first visit with a homeopath, Ioana and Mara described it as an “unhappy experience” given the much more restricted duration than the one expected: What we knew about homeopathy, what we read previously was that there was this interview… well, that during the first consultation the homeopath asks a lot of things, that it lasts one or two hours. But we went there, she asked me two questions, she gave a scheme of treatment with 10–15 remedies and we left. (Ioana, patient, research interview, April 17, 2016) We realized that it is not okay, we did not like his attitude, the consultation lasted 5 minutes – 3 minutes, something like that… he was looking, we were looking, and then he said take this and that … he treated you like... really, like you were a nobody. (Mara, patient, research interview March 17, 2017)
These atypical cases diverge from normally much longer visits with homeopathic practitioners, but by the same token, they reveal something important about the expected duration of such consultations. Indeed, the ordinarily open-ended duration of homeopathic consultations often serves as a rhetorical resource for justifying homeopathy’s legitimacy in public debates. For example, a homeopath (Firuti, 2018) posted an article on her site entitled Why people feel good at the homeopath contrasting the typical homeopathic consultation, in which the practitioner listens to the patient for a long time (operationalized as an average of 1 hour), with the biomedical consultation, in which the physician has no interest in what a patient has to say (which is evident in the short amount of time allotted for the consultation). Appealing rhetorically to personal experience, she describes her orthopedic (biomedical) consultation as one in which the physician talked for 25 of the 30 min, nearly the total length of the consultation, and in which she could not say or ask something. She wondered “what the physician has understood about my suffering and in what measure can we follow his recommendations if he barely listened to me,” assessing the entire experience as one of “frustration” and as typical for biomedical consultations which may be even shorter.
As in other countries, the duration of a biomedical consultation in Romania, both in public and private clinics, is regulated due to the dominant cost-effective model of healthcare. This requires physicians to take control of the conversation and gives shape to a consultation more focused on medically relevant symptoms and data, to the expense of broader social or psychological conditions. The logic of efficiency in the cost-effective model of healthcare drastically limits the amount of time that a physician can spend with a patient. For a general practitioner’s consultation, the average optimal duration established by the Health Ministry and the National Health Insurance is 15 minutes. As such, sociotemporal structures become more important than specific tasks in constructing time, a constraint that may be felt as a burden even by physicians. As one general practitioner describes the regulation of time allotted for consultations, which is imposed from “above”: “we do it… how to say… like on a conveyer belt, like in a factory” (in Rusu, 2015: 9).
Two models of time, what Davies (1990) calls process time and clock time, operate in medical practice, sometimes in a conflicting manner, affecting the lived duration of a consultation. Davies describes process time as a temporal framework in which there is no time limit on a particular task, the task in itself determining the amount of time needed. In contrast, clock time is an expression of a highly rationalized measurement of time in which tasks are controlled by the amount of time allotted for their completion. The pressures to attend to a clock-time treatment of patients, a model of time that has become dominant in healthcare, has often been critiqued as a depersonalizing treatment that ignores a patient’s lifeworld. Given that they practice outside of the bureaucratic management of health, homeopaths more easily engage in process time, a time for listening and recognizing, letting the task of questioning the patient follow a trajectory that is more sympathetic to a patient’s overall condition. As we have seen, this may not be embraced by all homeopaths in their practice, but the negative reactions to those homeopaths perceived as hurrying the consultation reflect the value of time in medical encounters. There is a shared understanding that one should be granted sufficient time to express one’s problems during a diagnosis. This value is evident in the way Diana emphasizes process time and subordinates clock time when answering our question about how long a homeopathic consultation lasts: [Consultations last] for how long it takes and what I have to say, what is necessary for me to say…. I have to say what troubles me and what changed or what is new. In general, consultations are about half an hour, but if more time is needed, it’s up to me. (Diana, patient, research interview, September 15, 2016)
Manipulation of sequence
The biographical sequence “triggers—symptoms”
Homeopathy shares with biomedicine an understanding of illness as having a temporal trajectory. In contrast to biomedicine, homeopaths claim to go beyond a restricted materialist understanding to determine how psychosocial elements might have contributed to its development. Thus, during the homeopathic consultation, practitioners ask questions not only about medical history, such as parents’ diseases, but also about a patient’s childhood or about past events that marked him or her in one way or another. Although a patient may come to a consultation complaining about a stomachache, the discussion may lead to past traumatic experiences, previous relationships, or other forms of the past that haunt patients in the present. Due to the importance of mental and emotional symptoms, a patient’s current condition may be seen as an effect of a more distant event, which has been suppressed psychologically and has erupted in a physical way. The rhetoric of suppression is also used when describing biomedical treatments as strictly temporary remediations that do not bring about “real healing.” In contrast, homeopathic treatments are described as solutions for regaining a “long-term balance.”
Exploring the past in search of an explanatory narrative for a current condition can be accepted as a legitimate practice. Moreover, as one patient recounted during an interview, in some cases, this process may lead to a new understanding of a disease or a patient’s overall concerns: At our first consultation, we told her a lot. She asked me about my childhood, what trauma did I have, what… you know? And when I was little… they cut a very big aspen from my street. And we were many children. And they said they will cut it, that it will fall in one side, but it fell in the side where the children were, and I got hurt. I had the right hand broken, with my bones out… well, and she [the homeopath] told me that it might be from then, since I have all the pains. I am always more sensitive on the right side… Well, and she said that it might be from then, you know? And my nervous moods she associated them with my parents’ death, because they were like this, one after another. Therefore, in a sense, she made me understand some things that were obvious… And this is it, from discussing she made me understand a lot of my problems. (Andreea, patient, research interview, August 17, 2018)
Conventional medicine may also give support to psychosomatic models of illness and to narrative-based interpretations (Kalitzkus and Matthiessen, 2009). Still, its dominant perspective is that of the objective biomedical report in which biographical time is reduced to a materialist etiology. In contrast, homeopaths try to answer the “Why me?” question: Why did I get sick in this way, at this moment? For this individualizing question, a materialist causal explanation, even if accepted, seems to offer only a partial response. A different way to address the “Why me?” question is by reviewing the sequence of events in a patient’s life in order to find a psychosomatic reason for the patient’s current condition, such as a past traumatic event that made the body more susceptible to various afflictions. As such, homeopathy’s etiological framework resembles the widespread cultural logic of understanding disease as caused by emotional trauma and “stress” in one’s past. In the words of one homeopathic physician, [When she was only a recovery physician] Patients used to tell me very frequently that [for instance] “when my husband died, I got sick of that or another,” “when I got very upset because of my child I felt sick,” and so on. They were very frequently connecting these organic decompensations or even disease debut with a previous problem. Having a more mechanistic education, I used to get bored, and I was telling myself, “Auch, here comes again another life story.” But, in time, I became more curious because I noticed that some types of problems related to some types of diseases.… For example, very rigid persons in their everyday life have problems with a very rigid backbone, spondylitis. Or the persons that were very sad lapsed into lung diseases. (Elena, homeopath, psychotherapist, and physical recovery physician, research interview, April 19, 2017)
The “intervention—effect” sequence
Homeopathy conforms to the sequence “intervention—healing effects”
The most important justification for homeopathy invokes its conformity with the normative sequence of medical intervention followed by healing effects. In brief, this account states that homeopathy works. This legitimation is frequently found in discussions with patients and practitioners, as well as in the public debate surrounding homeopathy. However, the same temporal logic is turned against homeopathy when practitioners, patients, or scientists conclude that homeopathy does not work—that is, treatment is not followed by expected effects (other than placebo). Due to the observed sequence of intervention followed by healing effects, Diana, a mother, tells us about her successful experience with homeopathy for her son’s otitis and her daughter’s general healthcare: Regarding these issues, I don’t know, many are very reticent, yes, but I really believe in it because I have seen results. (…) I was taking my son to the doctors and they gave me this allopathic medication, but I did not give them to him. I just went there for the diagnosis. And then I gave him the homeopathic ones. (…) What can I tell you, yes, one can see results. Also with my little daughter, I also have a 7-year-old girl with whom I started [homeopathic treatments] when she was very young…. When she was one month old I took her to Ms Doctor. And I want to tell you that she is now seven years old and she did not take any antibiotics. (Diana, patient, research interview, 28 August 2016)
This tactic of argumentative time work also concerns an aspect of duration, as we can see in the extract quoted above: not only does homeopathy produce expected consequences in a proper cause—effect sequence, but it does so for long periods of time. For some of our respondents, the value of homeopathy can be considered self-evident, given that they have used it for long periods of time and are satisfied with its results. Experiential success is taken to indicate that truth has surfaced in due time: I read an article on one of those sites, in which a dull… a two pence writer, anyway, was saying that Oscillococcinum [a homeopathic remedy] has a 1 to one million concentration, as if you took just water and so on, so forth, well, that homeopathy is quackery. Hey, how come you talk without having a clue? Have you talked with people who were cured? Have you talked with any doctor? Do you have any medical specialty of which I am not aware? What’s your point with these concentrations, if they lead to effects? (…) I said, come on brother, for 10 years my entire family takes these pills and we feel very fine, and you start commenting, you, who are clueless. (Mara, patient, research interview 14 August 2016)
Homeopathy deviates from the sequence “intervention—iatrogenic effects”
One of the frequent justifications for homeopathy invokes its deviance, rather than conformity, from an expected sequence: homeopathy is said to have no adverse effects. Asking “What homeopathy is and what homeopathy is not,” a practitioner answers on her website (Trifa, 2018):
What homeopathy is It is a medical science and therapy It is practiced by specialist doctors with competence in this qualification It is accredited and recognized by the Ministry of Health and WHO It is a profound, causal, and efficient therapy It is a holistic medicine It is a medicine based on scientific evidence and confirmed to be efficient both clinically and in the laboratory It is a noninvasive therapy and without side effects It is the therapy of the future!
What homeopathy is not It is not placebo effect It is not a simple naturistic medicine It is neither magic nor psychotherapy
We see here a complicated landscape of justifications, including appeals to scientific authority and state power as well as argumentative time work tactics: conformity with the cause—effect sequence, deviance from cause—side effect sequence, and reliance on the modality of the future that we discuss below.
This temporal deviance may also be invoked to delegitimize homeopathy. In 2011, the Romanian Secular-Humanist Association and Sceptici.ro staged a local happening as part of a global series of events meant to prove the absurdity of homeopathy. The so-called “Campaign 10:23” performed an “overdosage event” in which participants ingested large amounts of homeopathic remedies, only to find that nothing happened to them. The president of the SRH reacted to this event in the press: We invite the activists to make an honest step and see what the results of homeopathic medicines would be if they will be taken for 20–30 consecutive days; after sufficient iterations in repetitive administration, the [aggravation] symptoms begin to appear.
Other proponents of homeopathy framed it as an event that proved only that homeopathic remedies have no side effects, rather than not having any effects whatsoever. Through the debates that it generated, the overdosage event makes salient the role of the expectation that effects (but not side effects) will follow interventions. On both sides of this debate, we see arguments about how sequence determines the assessment of a therapy’s efficacy.
Uncertainty in the sequence “intervention—healing effects”
In biomedicine, the current body of knowledge regarding most of the conventional drugs is of a technical nature that standardizes various temporal markers (e.g., how many pills, at what interval, how long it will be until various positive and negative effects may be noticed, with what probabilities). This standardization may not overlap with the subjective experience of taking a drug, but it is available as health information for patients and practitioners alike.
This is not the case with homeopathic remedies, which, except for the over-the-counter ones, do not enclose prescription directions, and information about them is extremely varied. One patient commented on this: I consider them as pills, but I have the feeling that they are more than pills, that they have effects beyond… I mean, it is not like when I take an ibuprofen medicine and know that it has an effect. You take it, and several hours after that there is no pain. This, you take it. In the long run, its effect is undetermined. I do not know how much it lasts. There are no instructions, I mean there is no prospect. When you have a prospect, you know what you must do, what you should not do, how much the effect lasts, what happens in case of overdose. There is a lot of uncertainty surrounding them, and it seems tougher to administer them (Ana, patient, research interview, August 4, 2016).
Thus, for some patients, there can be a lot of uncertainty regarding homeopathic remedies. Homeopaths usually respond by modifying the sequential expectations of effects, thereby creating a temporal space in which failure can be accommodated. Although practitioners and patients may speak of observed efficacy patterns similar to those of conventional drugs (faster in the case of acute diseases, longer in the case of chronic diseases), there are no formal protocols to explain the variable sequence of effects for the homeopathic remedy since they are not described by the materialistic logic of conventional drugs. Hence, homeopaths have developed an alternative sequential expectation to account for the less predictable effects of their repetitive remedies. First, homeopathic remedies may act through “aggravation,” that is, a patient’s symptoms get worse initially, a sign decoded as a body that starts to fight the disease. Only then can one expect to see healing effects. Also, homeopathic remedies may act first on the emotional and mental level and only after on the physical level. Consequently, one’s general condition may improve by feeling more energetic, optimistic, and so forth, even if one’s physical symptoms remain the same. Overall, these alternative sequential expectations are accounted for through a temporal ideology: homeopathic remedies address a unique person and not a disease shared by many, making the prescription more tentative than those for conventional drugs. One homeopath put it this way: Reactions to the homeopathic remedy, even if well chosen and correct, are individualized: there are patients who react very fast, and patients who react very slow. For some of them, the reactions are strong, dramatic, even spectacular (pains that disappear immediately, short but intense aggravations); for others, the reactions are slower, and for a while, it seems that nothing happens, but at a detailed consultation, the physician can observe signs of improvement. (Jurj, 2014)
Claims of temporal individualization and customization of medical treatment are not specific to homeopathy. This points to the fact that using individualization as a justification for medical practice has a more general import, while the recognition of an individuality that suffers and cures in idiosyncratic ways has strong cultural overtones. The resulting uncertainty is congruent with patients’ emphasis on personal experience and subjective feelings of disease and treatment (Broom and Tovey, 2008). As such, they tend to be comfortable with homeopathy’s tentative sequencing of treatment and effects. This foregrounding of their uniqueness contrasts with the temporal standardization of biomedical treatment, with its emphasis on the generality of statistical knowledge based on aggregates.
The “failed biomedicine—successful homeopathy” sequence
A frequent justification for homeopathy consists in examples of last instance healing. This tactic builds on the “intervention—effect” sequence by amplifying contrast between previous defeat against illness and current triumph. Homeopathy is depicted as offering a cure after a prolonged series of failed attempts in biomedicine. These accounts take two forms: narratives of “spectacular cases” or of common experiences. A spectacular case is a patient with a critical condition (e.g., cancer or nephrotic syndrome) who has received conventional biomedical treatments but without any favorable results, a failure succeeded by a “spectacular” homeopathic cure. This sequence takes mundane forms in patients’ accounts of homeopathic care-seeking generated by the fact that they did not manage to find a biomedical cure for a specific condition or for the recurrence of some symptoms.
In the extracts below, note the progression of events depicted through these narratives of a “spectacular case” and a mundane case of homeopathic success following biomedical failure. The first was told to us by a homeopathic physician, and it recounts the story of a case treated by a world famous homeopath. It has circulated widely from being presented during the summer classes for training in classic homeopathy organized by George Vitoulkas and attended by many Romanian homeopaths. The second represents a typical account of a patient’s alternative care-seeking when conventional means fail. There was this remarkable case of a patient with nephrotic syndrome who was bloated 30 kilos and who could not eliminate liquids. He was in Sweden, he had the best physicians, urologists, professors who gave him all the diuretics, even chemotherapy for eliminating that water, the substances that he could not discharge. And they said that he has no cure, and if someone succeeds, he deserves the Nobel award. And he got to Vitoulkas who treated him and 90% of his symptoms ameliorated. Therefore, Vitoulkas received the Nobel award, well, not the Nobel but its alternative for medicine. (Dora, homeopath, research interview, May 15, 2017) A year ago, we started to have problems with T. [her son] who had some health problems, a very awful dermatitis. After we tried all the possible creams and classical methods, we began looking after alternative treatment.… And we have been, we believe, to ten dermatologists, pediatricians, all of them, and all said that they do not know the cause for dermatitis and there is no treatment for it. One treatment works for some, for some, it doesn’t. And it is frustrating to be told that we do not know the cause of your condition, and so you should try this, and this, and this. (Ioana, patient, research interview, April 17, 2016)
These accounts reiterate the temporal contrast between biomedicine’s failure and homeopathy’s subsequent efficacy. The first depicts biomedicine as unable to fulfill its mission of curing despite all its specialization, authorities, and modes of treatment. Homeopathy takes a remedial role to this narrative. Confronted by “the practical question par excellence: ‘What to do next?’” (Garfinkel, 1967: 12), biomedicine fails to offer a solution, thus creating feelings of frustration and undermining its claim to be a totalizing system for reaching health, irrespective of the disease. This failure pushes patients to look for a solution outside the conventional medical landscape and legitimizes recourse to therapies that lack scientific explanations but participate in a “community of promise” (Brown, 2003) in regard to health. This narrative depicts the restoration of health, and this temporal sequence lends credence to the homeopathic claim to efficacy. In the popular arena, the cure is proof in itself, even if modern medicine, as Stengers (2013) argues, has defined itself in contrast with this kind of anecdotal claim, through the elaboration of observation protocols that try to identify the “real” versus placebo reasons for effects (e.g., through random control trials). Through the circulation of accounts of spectacular treatments, homeopathy is for its audience not a “supernatural practice” but rather a legitimate remedial one, a value generated by means of its sequential position after failed biomedical attempts at curing.
Manipulation of temporal modalities
While temporal modality is not included in the original formulation of time work by Flaherty, we found this dimension useful in examining legitimation tactics through argumentative time work.
Legitimation from continuity with the past
In May 2018, the Union “Save Romania” (USR) advanced a legislative proposal to print on all homeopathic remedies the warning “This product has no effects on health.” The proposal was not enacted, but it kindled significant public debate on the merits and demerits of homeopathy. In an open letter addressed to USR on this occasion, the president of the (SRH) started with the following assertion: Homeopathy is old. Homeopathy is a holistic treatment modality, based on the principle of analogy stated by Pythagoras in the 6th century B.C.… Hippocrates, orientated toward a holistic understanding of the sick human being, applied this principle in medicine in the 5th century B.C.… Samuel Hahnemann (1755–1843) took up the principle of similitude at the end of the 19th century and formulated the theory of homeopathy, its fundamentals, and the technique for preparing the homeopathic remedy in dynamised infinitesimal doses.
The USR authors of the legislative proposal justified their action based mainly on the fact that, according to contemporary scientific studies, homeopathic remedies have no effect beyond placebo. They do not qualify homeopathy as simply “nonscientific,” but also as “prescientific, even mystical,” and relegate it to a past characterized by a “philosophic–mystical atmosphere,” when it existed alongside phrenology, vitalism, humoralism, and mesmerism. From this standpoint, homeopathy’s survival is due to a “damaging cultural inertia,” (Wiener 2018) as if that past should not be part of a present in which science should be the arbiter of what is considered legitimately medical.
The legislative proposal disparages the past, whereas the open letter celebrates the past. As Verdery (1999: 117) argues, the shape of history may be different according to the notions of genealogy and ancestry that people construct, instilling in this way different individual or group self-understandings. Both accounts privilege a linear and upward temporality. Nonetheless, the legislative proposal draws on a scientific regime of justification that is based on perceived discontinuity between a prescientific and a scientific past, while the open letter constructs its justification based on a perceived continuity between a valorous past and the present. This continuity is also one that emphasizes a shared genealogy with conventional medicine through the figure of Hippocrates and the medical training of Hahnemann. Detractors of homeopathy usually frame the dispute as one between science and pseudoscience or as a struggle between reason and obscurantism, a representation that rests on a conception of the past as a place of backwardness. Freidson (1970:16) notes that the late 19th century establishment of a scientific foundation for official medicine has meant a “qualitative break with the past… making possible for the first time the predictable and reliable control of a wide spectrum of human ills by virtually any well-trained practitioner of the occupation, not solely by a great clinician.” Hence, the Hippocratic Oath still guides a present-day physician’s practice but Hippocrates’s humoral theories do not.
In contrast, homeopaths are not so eager to abandon the past, and they still find older medical theories valid. Most often, homeopathy is presented as a therapy that “stimulates a body’s natural healing capacity.” This conception of health originates from Hippocratic medical practice in which the treatment was highly reduced due to the assumption that nature has its own capacity for healing and the practitioner can only assist it (Freidson, 1970). Translated into a minimal medical intervention, it gained popularity during the first part of the 19th century in Western countries, where patients were looking for an alternative to the “heroic medicine” of that era (Bivins, 2008), as well as today in the case of patients who search for alternatives to the side effects of synthetic drugs. Currently, 19th century ideas, such as miasma theory, may still guide homeopathic practice. Although they may be practiced in an orthodox fashion or translated into a more biomedical idiom (e.g., talking about miasmas as a genetic predisposition), their current use reflects the fact that proponents of homeopathy are more reluctant to abandon the past than are advocates for biomedicine.
Legitimation from breaking away with the past
Time work that attempts to establish continuity with a glorious past implicates Weber’s (1958) insight that authority can be based on tradition. Insisting on the oldness of homeopathy, its proponents call on the authority of an “eternal yesterday,” mobilizing tradition as a source of legitimacy through an emphasis on the continuity of homeopathic knowledge and practices. However, there are also situations where discontinuity is stressed, such as when the “origin myth” regarding Hahnemann’s discovery of homeopathy depicts his critique and dissatisfaction with conventional medicine, even though he was a certified physician. This justification highlights an appeal to a different form of Weberian authority: charismatic legitimation. It implies that his work was innovative, breaking from the establishment and its “traditional” medicine, leading to the creation of new (and presumably superior) types of therapy. This alternation between valorizing and denigrating the past points to the versatility of such justifications and their consequential appeal to a broader public.
Legitimation from the promised future
Some advocates account for homeopathy’s incompatibility with mainstream pharmacology by claiming that there is a scientific explanation for homeopathic remedies that has not yet been discovered, trusting in a future that will remedy the situation. This trust is based on the reasoning that a “paradigmatic shift model” (Yoshida, 2002) is required, a belief that contemporary biomedical knowledge includes radically new theories for explaining currently incongruent data. This is the preoccupation of a narrow group of practitioners and researchers, with the more common attitude being one of a “technical adoption” based on perceived efficacy and utility from experience, sidelining, for now, any need for an explanatory theory. Still, this imagining of a future scenario of scientific legitimacy should not be underestimated. Its more general significance is suggested by how one practitioner presents homeopathy on her online site under the section “Beyond flat medical thinking [Dincolo de gândirea medicală plată]” (Firuti, 2018). She makes an analogy between the controversy in the medical world generated by the appearance of homeopathy and the controversy generated by the Copernican revolution, pointing to a history of knowledge in which disruptive innovations were later accepted as valid, after being rejected at first by the established institutions and common sense. This reasoning reflects a past-oriented image of the future since it imagines that the future will be based on the repetition of a past pattern, bringing the past’s factuality into the future’s possibility.
Another way of imagining an uncontroversial future for homeopathy is through the concept of “integrative medicine.” The term was coined in the 1990s by Andrew Weil, a Harvard-trained physician and proponent of holistic health, for denoting the combination of various CAM therapies in treatment. It has evolved into designating a growing adoption of or collaboration with CAM therapies within biomedicine (e.g., referral of a patient to a CAM practitioner and interdisciplinary group practice) (Baer and Coulter, 2008). The term seems to enjoy some popularity in Romania since the National Institute for Complementary and Alternative Medicines organizes annual conferences on “integrative medicine.” Its main assumption is that “man is a unitary being composed of body, mind, and soul.” Participants advocate the combination of different therapies, often including conventional medicine. As one homeopath explained during an interview, In general, worldwide, this is the aim [integrative medicine]: To integrate a lot of therapies, conventional and unconventional, for the patient’s benefit. Because it is obvious that the diseases are more and more complex, so the therapies should be so too.… [the clinic where she works] integrates because this is the future of medicine.… When a patient comes with a health problem, one tries to integrate homeopathy, acupuncture, massage, or other useful therapies, so one can help from various angles with natural therapies. (Anca, homeopath and school physician, research interview, December 14, 2016, italics added)
This future reasoning assumes that the emergence of more complicated diseases will necessitate the development of more sophisticated medical interventions. Some proponents go so far as to proclaim homeopathy as the “future of medicine” based on a need to change the status quo due to the shortcomings of biomedicine. Interviewed in a popular Romanian magazine dedicated to CAM therapies, Christian Boiron (one of the founders of the Boiron company that produces homeopathic over-the-counter remedies) epitomizes this perspective: I do believe that homeopathy will have a bright future, because it is and it will be a genuine pharmacological and medical field, without having the toxicity and side effects of allopathic medicine. Thus, homeopathy may be the possible future of medicine! When the action mechanism of infinitesimal dose will be fully understood, it may be very possible that homeopathy will be the most important pharmaceutical domain worldwide! (Popa, 2018)
As various scholars have noted, biomedicine has a regime of hope as one of its main logics (Brown, 2003; Moreira and Palladino, 2005). This is an optimistic discourse in which new and better treatments are always imagined, justifying current research and development by promising a future cure for various diseases. Promissory discourse and its high hopes are necessary, since various actors must be mobilized (e.g., patients, health advocacy groups, state representatives, etc.) so that a specific project can move forward, pointing to the performative effect of future thinking (Brown, 2003). We suggest that the future-oriented thinking that some proponents of homeopathy exhibit displays an alignment with the biomedical regime of hope. This rhetoric may take on a scientific technological veneer when references are made to “quantum medicine” or “energy medicine” as future explanations, or it may have a less specified formulation. In any guise, it confers importance upon future projections for legitimizing present action. Advocates imagine a future in which homeopathy will be accepted by the biomedical establishment due to the emergence of an explanatory theory or due to its efficacy in the treatment of various illnesses. In so doing, proponents lend credence to their current practice, either by appealing for an open-minded attitude toward the future state of scientific knowledge or by envisioning novel approaches to the ideal treatment of human ailments.
Conclusion
Previous studies have addressed some of the temporal dimensions of CAM practices and discourse, noting that a desire for longer consultations may be one of the motives for which patients consult a CAM therapist (Cant and Calnan, 1991) or that the temporal experience of CAM treatments may have its ups and downs (Broom and Tovey, 2008). In this article, we have advanced this line of inquiry by identifying seven different types of time work, structured along three dimensions, that contribute to constructing homeopathy’s cultural legitimacy in Romanian public discourse. Our approach builds on an understanding of legitimacy as an ongoing discursive process in which those who try to legitimize an action offer justifications in terms of desirable and appropriate attributes that resonate with widely shared societal values and expectations.
Based on our findings, we suggest that argumentative time work plays an important role in constructing homeopathy’s cultural legitimacy by invoking a cultural repertoire of values concerning time and linking them to several widely shared conceptions of health and illness. To paraphrase Flaherty’s (2011) notion of “doing time” through confronting and mastering temporal experience, the defenders of homeopathy strive to establish its legitimacy by “talking time” and exerting temporal agency, while making use of culture as a “tool kit” (Swidler, 1986). Talking time takes the controversy associated with homeopathy beyond health-specific knowledge claims, by appealing to cultural understandings of temporality as a basis for delineating similarities and differences between homeopathy and biomedicine.
The significance of our findings is twofold. First, we demonstrate the usefulness of time work as a conceptual tool for the study of legitimation, with special application to healthcare. Moreover, we synthesize disparate insights regarding the importance of time and temporal experience in the assessment of medical encounters, and we integrate these observations into a coherent analytical framework that can be applied to the investigation of other phenomena. As directions for future research, we intend to continue our study of legitimation through time work tactics in current controversies related to vaccine hesitancy and climate change denial.
Second, the substantive focus of our research also expands the theoretical implications of the time work concept, as initially formulated by Flaherty (2003), from the study of subjective temporal experience to the study of public discourse and other forms of rhetoric. From an empirical standpoint, we also observe a dimension of time work that was not part of the original formulation: the manipulation of temporal modalities (past, present, and future) in efforts at persuasion. Our findings suggest that temporal modality should be added to the dimensional structure of the time work concept in future studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.