
Abstract
Objectives
Psychosis is a rare but severe neuropsychiatric manifestation of systemic lupus erythematosus (SLE). Its prevalence, clinical predictors, and immunopathogenesis remain incompletely understood. This study aimed to estimate the prevalence of psychosis in adult SLE patients and identify associated clinical and immunological risk factors.
Methods
This systematic review and meta-analysis was conducted following PRISMA guidelines. A comprehensive search of PubMed, Embase, and the Cochrane Library was conducted to identify all relevant studies with ≥10 adults through November 2024. Case-series, case reports, narrative reviews and conference abstracts were excluded. Quality assessment employed the Cochrane Risk of Bias Tool for randomized controlled trials and the Newcastle-Ottawa Scale for observational studies. Statistical analysis was performed using the random-effects model, with heterogeneity assessed via I2 statistics.
Results
A total of 65 studies, comprising 31,495 SLE patients, were included. The pooled prevalence of psychosis in SLE patients was 4.5% (95% CI: 3.6%–5.5%) and 20.5% (95% CI: 10.0%–37.6%) among neuropsychiatric SLE (NPSLE) patients. Psychosis frequently occurred within 2 years of SLE onset and was strongly associated with higher SLE disease activity, positive anti-ribosomal P antibodies, antiphospholipid antibodies, and complement consumption. Delusions and hallucinations predominated among clinical presentations. Heterogeneity among studies was substantial.
Conclusion
Observational studies have reported that psychosis in SLE is strongly associated with increased disease activity and immune dysregulation. Anti-ribosomal P antibodies demonstrate a high negative predictive value, offering a valuable diagnostic adjunct. Recognition of psychosis may prompt closer clinical evaluation and, where appropriate, consideration of immunosuppressive treatment.
Keywords
Key messages: • Psychosis affects up to 4.5% of adult SLE patients and 20.5% of NPSLE patients. • Psychosis is linked to disease activity and immune markers like anti-ribosomal P. • Anti-ribosomal P antibodies have high specificity and negative predictive value for SLE psychosis.
Introduction
Systemic lupus erythematosus (SLE) is a complex autoimmune disease characterized by systemic inflammation and multiorgan involvement. 1 Among its numerous clinical manifestations, neuropsychiatric involvement, termed as neuropsychiatric SLE (NPSLE), is particularly challenging to diagnose and manage due to its broad spectrum of presentations and often subtle, overlapping features with other conditions.1–3 The prevalence of neuropsychiatric (NP) manifestations in SLE patients is estimated to range from 9% to 75%.4,5 This wide variability is primarily attributed to the absence of standardized definitions and terminology prior to 1999, when the American College of Rheumatology (ACR) Ad Hoc Committee on NPSLE Nomenclature introduced case definitions for 19 distinct neuropsychiatric syndromes associated with SLE.4,6
Psychosis, while a relatively rare complication, is one of the most severe manifestations of NPSLE. It represents a critical area of interest, due to its profound impact on patients' lives and the complexities surrounding its pathophysiology, diagnosis, and treatment.1–3 Although the association between SLE and psychosis has been recognized for decades, the prevalence and predictors of psychosis in SLE remain inconsistently reported, mainly due to the difficulty of attributing NP events to SLE.4,7,8 The nature of psychosis in SLE is multifactorial, implicating immune-mediated mechanisms, inflammatory processes, and external contributors such as treatment side effects, particularly from corticosteroid use. 7 Furthermore, recent genetic studies, including Mendelian randomization analyses, suggest a potential shared vulnerability between SLE and primary psychotic disorders such as schizophrenia. 9
Given the clinical importance of early recognition and treatment of SLE psychosis, an updated synthesis of its epidemiology and risk factors is urgently needed. This systematic review and meta-analysis aimed to determine the prevalence of psychosis in adult patients with SLE and to identify clinical and immunological predictors associated with an increased risk of psychosis. Additionally, this study evaluates the quality of the included studies.
Methods
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement (PRISMA) guidelines. 10 Given the anticipated variability in study designs and outcomes, we planned both qualitative and quantitative analyses to synthesize the prevalence of psychosis in adult-onset SLE.
Data sources and searches
We conducted a systematic literature search in PubMed/Medline, EMBASE, and the Cochrane Library databases from their inception to November 2024 to identify studies on psychosis in adult-onset SLE. The search strategy included two MeSH terms. Term A was “systemic lupus erythematosus” or “SLE” or “Lupus” and Term B was “psychosis” or “psychotic disorders” or “schizophrenia” or “delusions” or “hallucinations”. Additionally, a manual search of the reference lists of extracted articles and relevant reviews was meticulously performed to ensure the inclusion of any further studies falling within the scope of our review. Only studies published in English were included. The titles and abstracts of all articles retrieved in these searches were reviewed using inclusion and exclusion criteria.
Study selection
Inclusion criteria
Articles eligible for inclusion in this review were required to meet the following criteria: (i) examined psychosis in adult patients with SLE (ii) were original studies, including cross-sectional, case-control, cohort (prospective or retrospective) studies, case series, and randomized controlled trials (iii) included a sample size of 10 or more adult patients diagnosed with SLE (iv) SLE diagnosis was based on recognized classification criteria such as the American College of Rheumatology (ACR) criteria or the Systemic Lupus International Collaborating Clinics (SLICC) criteria (v) The presence of psychosis was defined according to the 1999 American College of Rheumatology (ACR) nomenclature and case definitions for NPSLE on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) or equivalent diagnostic criteria.
Exclusion criteria
Articles meeting the following criteria were excluded from our review: (i) narrative or systematic reviews, meta-analyses, editorials, case reports, and case series that included less than 10 patients; (ii) conference abstracts (iii) articles where full text was not available; (iv) articles published in language other than English.
Data extraction and quality assessment
After study selection, we extracted the following data from full-text articles: study characteristics (author, source, year of publication, country, study design); sample size; diagnostic criteria for SLE and psychosis; disease duration and activity; prevalence of psychosis along with any reported risk factor; demographics (age, sex); psychotic symptoms, specific clinical characteristics; and the presence of anti-ribosomal P in SLE patients with psychosis.
The risk of bias was assessed independently by two authors (EK, ME), using the Joanna Briggs Institute (JBI) checklist for cross-sectional studies. Newcastle-Ottawa Scale (NOS) was used to evaluate non-randomized trials cohort and case-control studies.11–13 In cases where the score of a specific study differed between the 2 reviewers, an agreement was reached following discussion. Non-randomized trials studies, were considered to be at low risk of bias if 8 or more out of the 9 criteria were met and moderate risk of bias when 7 criteria were met. The scores of each study are presented in Supplementary Tables S1A, S1B, and S1C.
Data synthesis and analysis
This study used aggregated data where possible. The meta-analysis of odds ratios was conducted using the RevMan program (RevMan, 2014) as suggested by the Cochrane Collaboration Group. Statistical calculation of pooled proportions was conducted in R language using the default settings of the “meta” package and the “metaprop” function with a random effects model. 14 Forest plots are presented for each meta‐analysis along with the I2 statistics, which were used to evaluate heterogeneity. 15 This statistic suggests whether chance or study heterogeneity is responsible for the observed variation. Negative I2 values were set equal to zero, and values ranged between 0% and 100%. 15 Heterogeneity can be quantified as low, moderate, and high, with upper limits of 25%, 50%, and 75% for I2, respectively. Often, data did not lend itself to meta‐analysis, and therefore a narrative approach was taken.
Results
Study selection process and characteristics of included studies
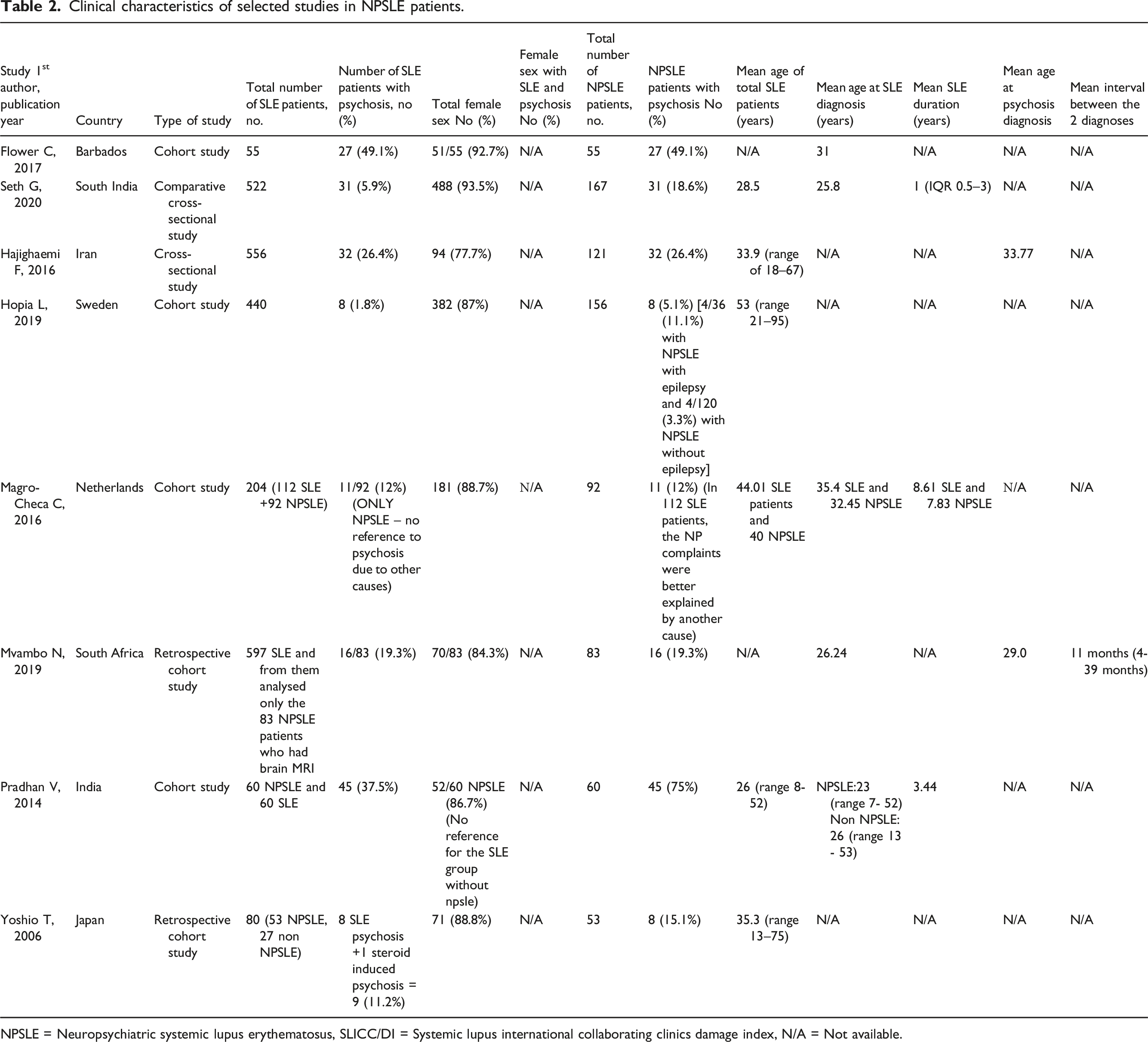
We identified 3359 articles through electronic database searches and 40 through manual searches. Study selection was conducted in two sequential stages in accordance with PRISMA guidelines. After removal of duplicates, titles and abstracts of 2539 records were screened for relevance. At this stage, 2144 records were excluded because they clearly did not meet the predefined inclusion criteria. Subsequently, the full texts of 395 articles were assessed for eligibility, of which 330 were excluded. Ultimately, 65 studies fulfilled the inclusion and exclusion criteria and were included in the final qualitative synthesis (Figure 1). These studies were conducted in Asia (n = 22), Europe (n = 23), the USA (n = 17), and Africa (n = 4). Study designs included 43 cohort studies, 19 cross-sectional studies, 2 case-control study, and 1 mixed design (cross-sectional and retrospective cohort). Tables 1 and 2 summarize the clinical characteristics of the included studies for SLE and NPSLE, respectively. PRISMA flowchart describing the study selection process. The main clinical characteristics and results of identified studies are summarized. NPSLE = Neuropsychiatric systemic lupus erythematosus, SLICC/DI = Systemic lupus international collaborating clinics damage index, N/A = Not available. Clinical characteristics of selected studies in NPSLE patients. NPSLE = Neuropsychiatric systemic lupus erythematosus, SLICC/DI = Systemic lupus international collaborating clinics damage index, N/A = Not available.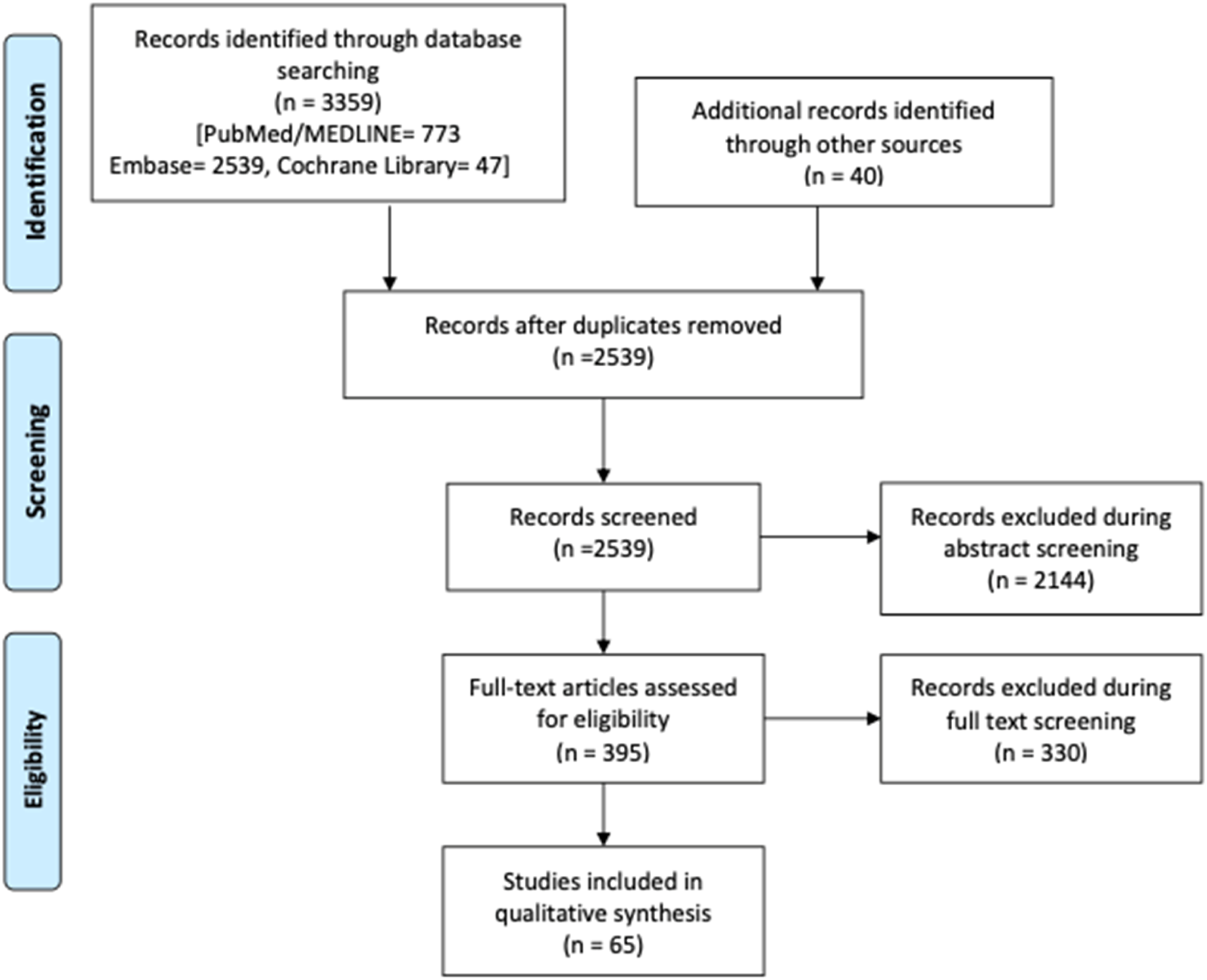
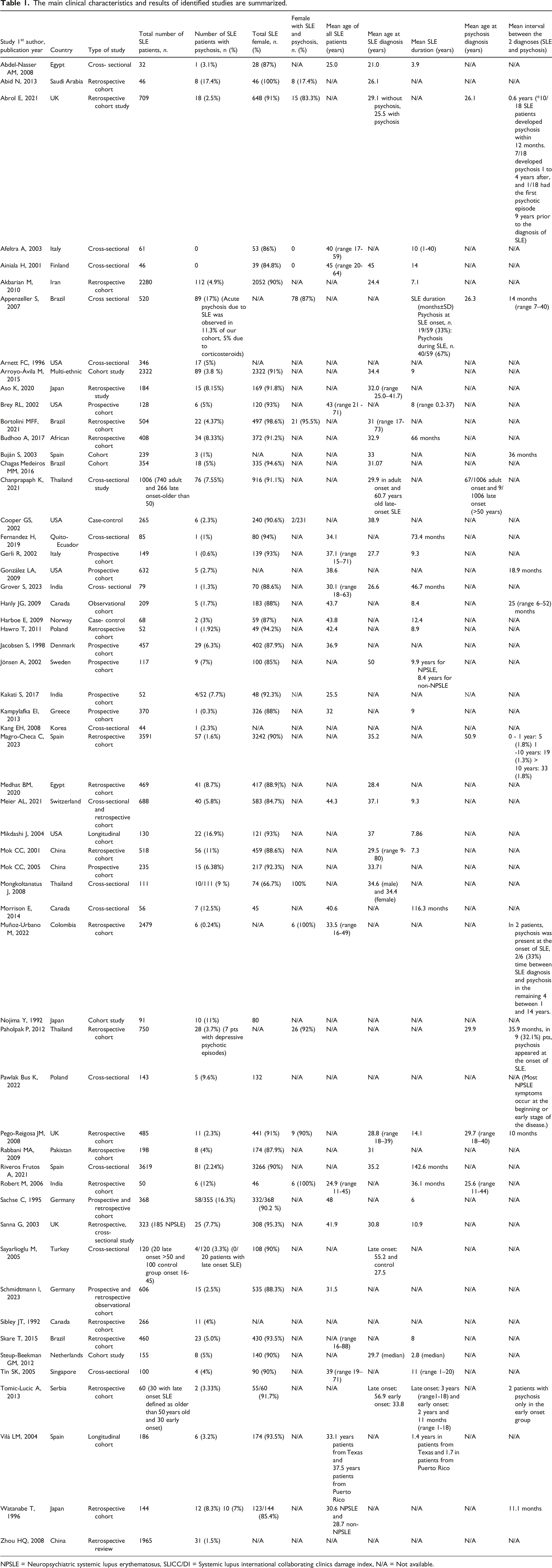
Among these 65 studies, a total of 31,495 patients with SLE were reported, of whom 18,832 (59.8%) were female. The mean age of patients with SLE was 37 years, while the mean age at psychosis diagnosis was 40.7 years. The mean age at SLE diagnosis was 28.8 years, with a mean interval of 19.2 months between SLE diagnosis and the onset of psychosis.
Most studies classified SLE according to the 1982 or 1997 ACR criteria or the 2012 SLICC criteria. Psychosis was diagnosed based on the 1999 ACR nomenclature for NPSLE, the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV or DSM-5), and, in some cases, the International Classification of Diseases (ICD-10). Several studies assessed psychiatric symptoms using validated scales, such as the Brief Psychiatric Rating Scale (BPRS) or structured clinical interviews. However, in a few studies, the authors did not specify the diagnostic criteria (Supplemental Tables S2A and S2B).
SLE disease activity was assessed using the SLE Disease Activity Index (SLEDAI), including its modified versions (SLEDAI-2K and SELENA-SLEDAI). Some studies utilized the SLICC/ACR Damage Index (SDI) to evaluate long-term organ damage, including neuropsychiatric involvement. Other tools included the British Isles Lupus Assessment Group (BILAG) index, the European Consensus Lupus Activity Measurement (ECLAM) scale, and the Modified Systemic Lupus Activity Measure (SLAM), which were used in select studies to capture various aspects of disease severity.
Prevalence of psychosis in adults with SLE
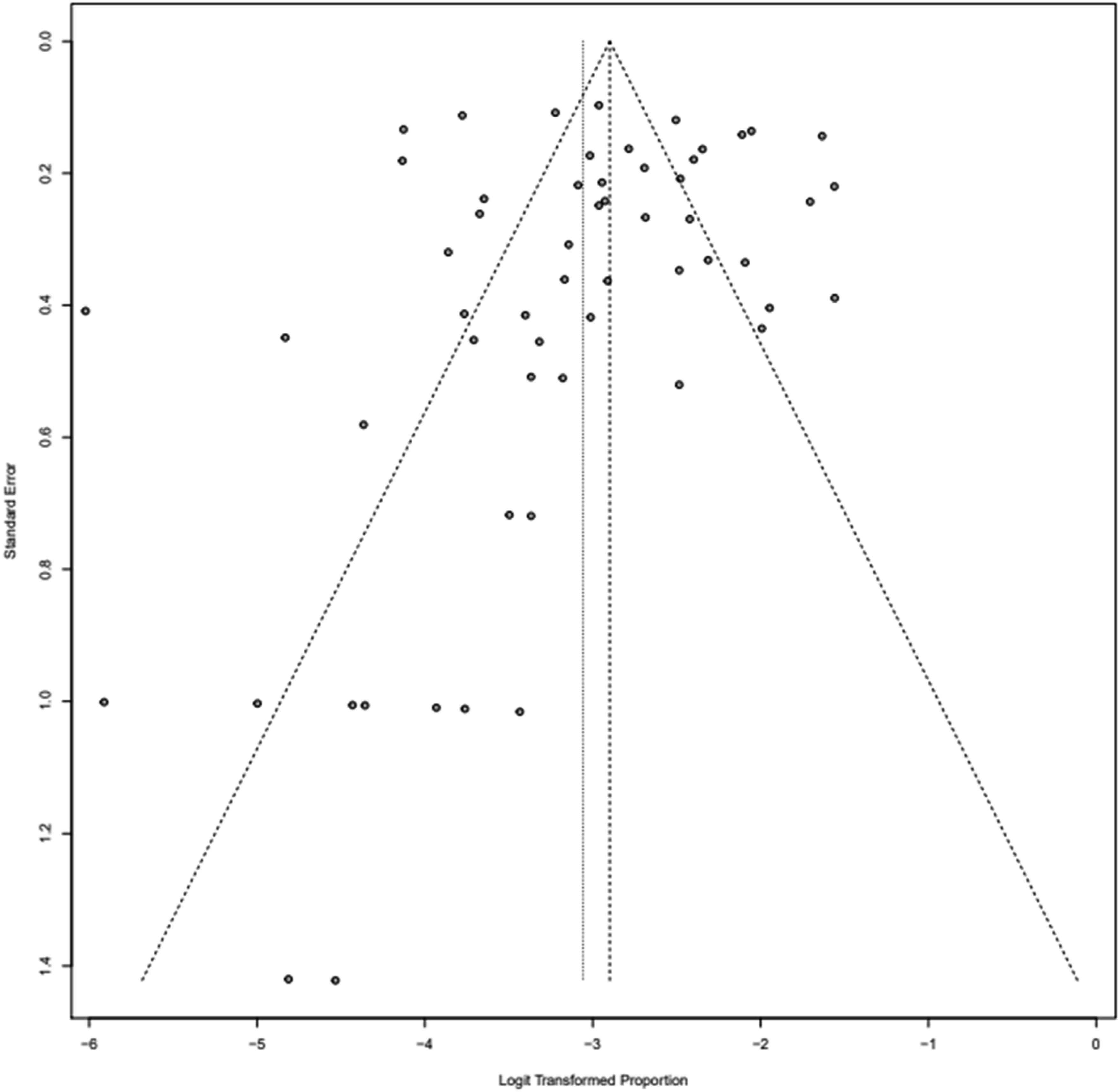
Figure 2 shows the pooled prevalence of psychosis in non-selected populations of adult patients with SLE, based on the meta‐analysis of 57 available studies comprising 30,134 patients.1–5,7,8,16–65 The pooled prevalence was 4.5% (95% confidence interval [CI] = 3.6%–5.5%). However, high heterogeneity was observed (I2 = 91%, Figure 3). Prevalence of psychosis in SLE patients. Funnel plot.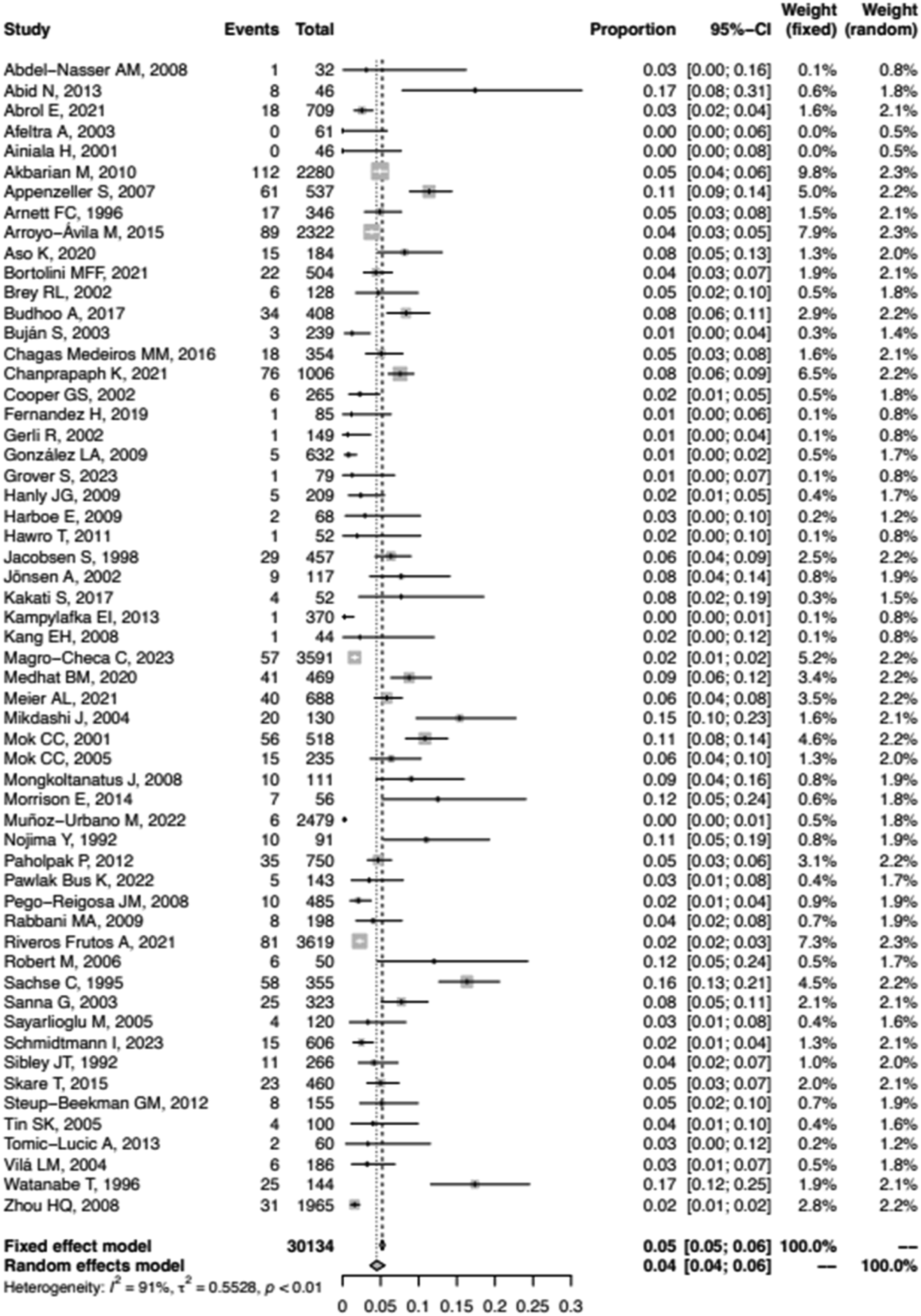
Prevalence of psychosis in adults with NPSLE
Figure 4 presents the pooled prevalence of psychosis in adult patients with NPSLE, based on a meta-analysis of 8 studies involving 926 patients.66–73 The estimated prevalence was 20.5% (95% CI: 10.0%–37.6%), with high heterogeneity (I2 = 95%). Prevalence of psychosis in NPSLE patients.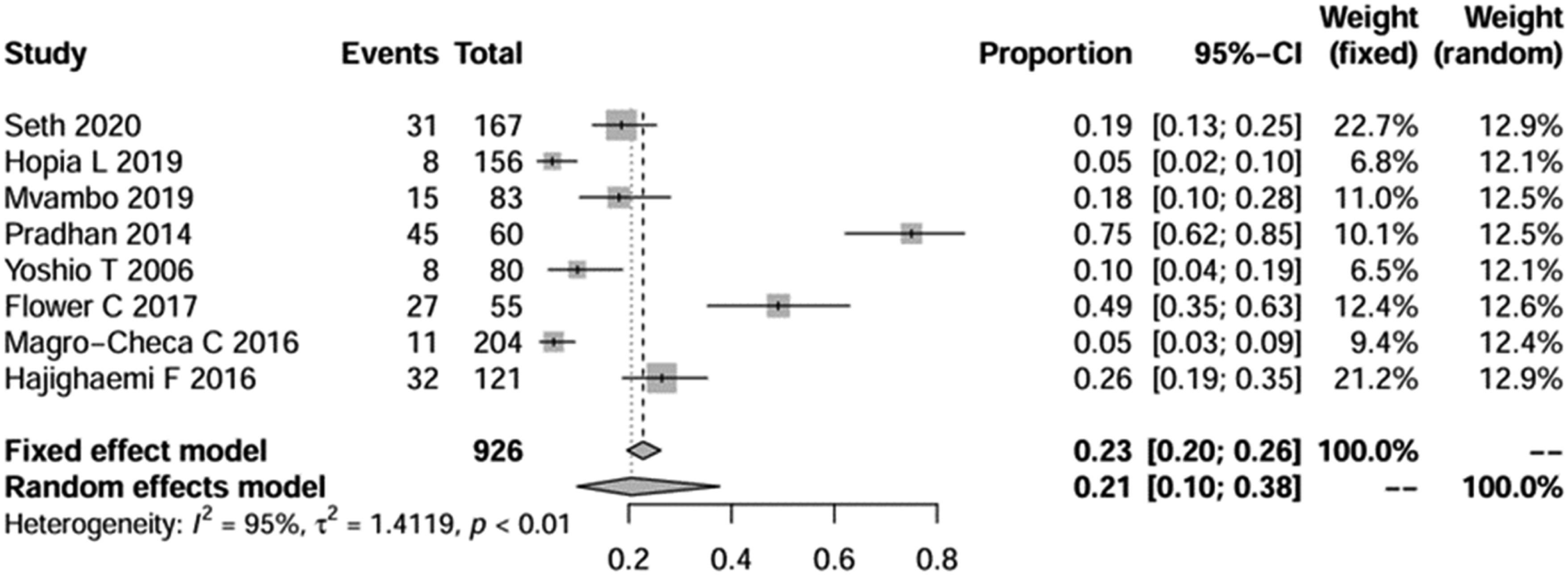
Ethnic and demographic differences among SLE patients with psychosis
Sex-specific data were available from 9 studies, including 2075 females and 226 males with SLE. In a random-effects meta-analysis, the odds of psychosis in females compared with males were not significantly different (OR 0.85, 0.42-1.73, p = .163).
Ethnic variations in SLE psychosis suggest underlying genetic and environmental influences. Several studies reported a higher prevalence among African American patients compared to Caucasians, though statistical significance varied. 28 African Blacks had significantly more psychosis than Indian patients in South Africa (34.5% vs 10.9%, p = .013). 70 Hispanic subgroups also differed, with Texas Hispanics showing higher psychosis rates than Puerto Rican Hispanics. 64
Symptoms of SLE patients with psychosis
Psychotic symptoms were described in only 8 studies, with delusions and hallucinations being the most commonly reported manifestations. Abrol et al. noted paranoid delusions (36.8%), grandiosity (26.3%), and both auditory (57.1%) and visual hallucinations (38.1%). 17 Mikdashi et al. described disorganized thinking, catatonia, and bizarre behavior, particularly in patients with active disease and high SLEDAI scores. 43 Muñoz-Urbano et al. reported cognitive dysfunction, auditory command hallucinations, paranoia, and mania, while Pego-Reigosa et al. found hallucinations or delusions with paranoid ideation in 80% of psychotic SLE patients.48,52
Natural history and timing
Psychosis often appeared early in the disease course.7,23,48,50,52 In Pego-Reigosa et al., 60% of patients had psychosis as the initial SLE manifestation, and 80% developed it within the first year. 52 Similarly, Paholpak et al. reported that 30.6% of psychotic episodes occurred at disease onset, with a 2.9% relapse rate over 44 months. 50
The majority of studies reported that psychosis was more prevalent in childhood-onset SLE (<18 years) than adult-onset, and more common in adult-onset than in late-onset SLE (>50 years).23,27,36,42 However, Chagas Medeiros et al. found no significant differences across age groups. 26
Primary SLE psychosis versus corticosteroid-induced psychosis
One study sought to differentiate primary SLE psychosis from corticosteroid-induced psychosis. Appenzeller et al. attributed 59 cases to primary central nervous system (CNS) SLE, 28 to corticosteroid use, and 2 to unrelated psychiatric disorders. 7
Association between disease activity, autoantibodies and psychosis
Multiple studies have shown a strong link between SLE disease activity and psychosis, supporting an immune-mediated mechanism.7,23,38,43,48,52 High baseline disease activity was predictive of psychosis.43,48,52 Pawlak-Bus et al. reported that neuropsychiatric symptoms primarily affected younger patients with active disease. 51 Appenzeller et al. found that psychosis at disease onset was significantly associated with disease activity (p = .001; OR = 2.4), emphasizing the role of inflammatory flares in triggering neuropsychiatric events. 7
The association between anti-ribosomal P (anti-P) antibodies and psychosis in SLE has been well documented, with several studies reporting significant correlations.1,3,17,20,30,33,39,40,49,52,66 Among 3962 SLE patients across these studies, 111 (2.9%) had psychosis. Of the 94 psychotic patients tested for anti-P, 36 (38.3%) were positive. In contrast, only 284 of 2102 non-psychotic SLE patients tested positive (13.5%). These findings indicate that anti-P antibodies have low sensitivity (38.3%) and positive predictive value (11.2%), but high specificity (86.5%) and negative predictive value (96.9%) for SLE psychosis. Thus, a negative anti-P result strongly argues against psychosis being attributable to SLE (Supplemental Table S3). Abdel-Nasser et al. reported high sensitivity (100%) and specificity (80.6%) for anti-P in detecting psychosis, 1 while Arnett et al. found a significantly higher prevalence of psychosis in anti-P–positive patients (13%) versus anti-P–negative patients (3%) (p = .005; OR = 4.43). 20 Similar associations were reported by Seth et al., Hanly et al., and Nojima et al..33,49,66 Watanabe et al. further observed that IgA and IgM anti-P levels peaked at psychosis onset and declined with remission, suggesting a role in disease monitoring. 65 However, not all studies were consistent. Kampylafka et al. identified only one anti-P–positive case among 16 psychotic patients, 3 and Brey et al. found no significant association between anti-P and psychiatric manifestations. 39 These discrepancies underscore the variability across studies. Overall, while anti-P antibodies show high specificity and are useful in ruling out SLE psychosis when absent, their low sensitivity limits diagnostic utility.
Beyond anti-P, several other autoantibodies have been linked to psychosis in SLE. Abrol et al. reported high frequencies of ANA (94.4%), anti-RNP (50.0% vs 26.5%, p = .033), and anti-dsDNA (44.4%) in patients with SLE psychosis, while anti-cardiolipin antibodies were significantly less common (5.6% vs 30.0%, p = .032). 17 Antiphospholipid antibodies were also associated with psychosis, as shown by Appenzeller et al. (OR = 3.2, p = .004) and Sanna et al. (OR = 2.2, p = .01).4,7 Notably, antiphospholipid antibodies were more frequent in SLE psychosis than in corticosteroid-induced psychosis (OR = 2.2, p = .01). 7 Tin SK et al. identified a correlation between brain-reactive autoantibodies (BRAA) and neuropsychiatric symptoms, including psychosis, though these antibodies are not commercially available, and their findings remain unvalidated. 62
Complement dysregulation appears to play a significant role. Studies by Aso et al., Magro-Checa et al., and Muñoz-Urbano et al. reported associations between SLE psychosis and low C3 (OR = 28.6, p < .001), low C4 (OR = 3.8, p < .05), and low CH50 (OR = 9.2, p = .001).22,41,48 Magro-Checa et al. further found that among NPSLE patients, those with psychosis had greater complement activation and more frequent low levels of C1q, C3, and C4. 69 Serum C3 was the only independent predictor of new-onset psychiatric symptoms after corticosteroid treatment.
Other manifestations of SLE patients with psychosis
SLE psychosis often coexists with other systemic and neurological manifestations, reflecting widespread immune dysregulation. Patients with psychosis had a higher risk of SLE encephalopathy, suggesting overlapping CNS involvement. 25 Cognitive impairment was frequently reported; in one study, 135 of 185 patients with neuropsychiatric damage developed cognitive dysfunction or major psychosis (HR 2.53, 95% CI: 1.56–4.11; p = .0002). 31 Seizures were also significantly associated with psychosis, 36 and leukopenia was more common among affected patients. 60
Hypoalbuminemia was linked to corticosteroid-induced psychosis (p = .03; OR = 2.2). 7
MRI findings in SLE psychosis often showed small-vessel disease, white matter hyperintensities, and cerebral atrophy, supporting vascular and inflammatory contributions. 70 Interestingly, the absence of malar rash (p = .002) and photosensitivity (p = .01) was associated with psychosis, implying distinct immunopathogenic pathways. 7 Compared with corticosteroid-induced cases, patients with SLE psychosis were more likely to exhibit additional CNS symptoms (p = .03; OR = 2.1). 7 Hopia et al. reported a threefold increase in psychosis among NPSLE patients with epilepsy (p = .0006), suggesting a link between seizure activity and psychosis. 67 These findings underscore the need for comprehensive neurological assessment in SLE patients with psychosis.
Discussion
This systematic review and meta-analysis provides a comprehensive evaluation of psychosis in SLE, assessing its prevalence and clinical and immunologic features. To our knowledge, this is the first systematic review aiming to examine the prevalence of psychosis in SLE patients while also investigating clinical characteristics. Our findings indicate that psychosis is an uncommon but serious neuropsychiatric manifestation of SLE, with a pooled prevalence of 4.1% in SLE patients and 20.5% among those with NPSLE. Ethnicity appears to play a role, though further studies are needed to clarify whether this is due to genetic, cultural, or other factors. Additionally, childhood-onset SLE was associated with a higher prevalence of psychosis.23,26,27,36,42
Psychosis in SLE often presents early in the course of disease, with studies indicating that a significant proportion of psychotic episodes occur within the first year of onset. This early onset may be attributed to a more aggressive disease course and increased immune-mediated damage seen in patients with early SLE. The heightened inflammatory milieu, driven by SLE-related autoantibodies and complement activation, may contribute to neuronal dysfunction and trigger neuropsychiatric manifestations such as psychosis. In childhood-onset SLE, the immune system may respond differently compared with adult-onset SLE, leading to a higher prevalence of neuropsychiatric symptoms. Furthermore, the presence of autoantibodies, including anti-ribosomal P and antiphospholipid antibodies, may exacerbate the risk of psychosis early in the disease, highlighting the importance of immune dysregulation in these cases. The lower prevalence of psychosis in late-onset SLE, apart from a less aggressive autoimmune response, may be due to the presence of comorbidities that can mask neuropsychiatric symptoms. Understanding the early onset of psychosis in SLE can aid in timely diagnosis and intervention, ultimately improving patient outcomes.74–80
Among autoantibodies, anti-P and antiphospholipid antibodies are most frequently implicated.1,3,4,7,17,20,30,33,39,40,49,52,66 Anti-P antibodies may directly impair neuronal protein synthesis, contributing to psychosis. Their low sensitivity and PPV and high specificity and NPV suggest that anti-P antibodies are not useful for diagnosing SLE psychosis when present, but they may be useful for ruling it out when absent. This limits their standalone diagnostic utility and warrant cautious interpretation in clinical practice. Antiphospholipid antibodies promote endothelial dysfunction and microvascular thrombosis, potentially disrupting the blood–brain barrier and facilitating neuroinflammation.
Complement abnormalities—especially low C3 and C4—have also been linked to psychosis, suggesting that immune complex–mediated neuronal damage plays a key role in pathogenesis.22,48,69 Together, these findings highlight the multifactorial nature of SLE psychosis, driven by complex interactions between systemic inflammation, autoimmunity, and neurovascular injury.
Distinguishing between primary SLE psychosis and corticosteroid-induced psychosis may be challenging for clinicians. Our findings indicate that SLE psychosis is more common in the early disease course, often within the first year of diagnosis,7,23,26,27,36,42,48,50,52 whereas corticosteroid-induced psychosis tends to develop later in the course of disease, with Appenzeller et al. identifying hypoalbuminemia and high-dose steroid therapy as key risk factors for the latter. 7 This distinction is crucial for guiding treatment, as immunosuppressive therapy is beneficial for SLE psychosis, whereas steroid tapering is required for drug-induced psychosis.
Our findings should be interpreted with caution given some limitations. Firstly, a major limitation of this review is the very high heterogeneity observed across the meta-analyses, as shown by the I2 statistic. Although random-effects models were used, such substantial heterogeneity limits the interpretability of the pooled prevalence estimates, which should therefore be interpreted with caution. The heterogeneity likely reflects differences in study design, definitions of psychosis, attribution methods for SLE-related psychosis, and variability in patient characteristics such as ethnicity, disease duration, disease activity, and treatment exposure. Potential sources of bias include misclassification due to non-standardized diagnostic criteria, including lack of standardized psychiatric assessments, selection bias and incomplete control for confounding factors, such as concomitant psychiatric disorders, medication effects, and socioeconomic status. Future studies using standardized definitions and attribution frameworks, along with stratified analyses by key clinical and demographic variables, may help reduce heterogeneity and improve the reliability of prevalence estimates. An additional limitation is the considerable variability in how psychosis was attributed to SLE across studies, with only a minority clearly distinguishing primary SLE psychosis from corticosteroid-induced or other secondary causes, which may have biased prevalence estimates and associations with immunological markers. Adoption of consensus-based attribution criteria, alongside prospective assessment of medication exposure and competing etiologies, may help reduce misclassification and improve the validity of future prevalence estimates. Finally, this review may be subject to publication bias, given that grey literature was not searched. Nevertheless, the risk was partially mitigated by a systematic and comprehensive search of three major bibliographic databases.
Conclusion
In conclusion, psychosis in SLE, although uncommon, reflects significant underlying immune dysregulation and disease activity. Psychosis typically arises early in the disease course, often within the first 2 years following SLE diagnosis, highlighting a critical window for vigilance. Anti-ribosomal P antibodies were identified as a specific biomarker of SLE psychosis. However, their low sensitivity and inconsistent findings across studies limit their standalone diagnostic utility and warrant cautious interpretation in clinical practice. Future research should focus on clarifying underlying mechanisms and developing precision medicine approaches for NPSLE.
Supplemental material
Supplemental material - Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis
Supplemental material for Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis by Konstantinos Parperis, Panagiotis Zis, Marina Evangelou, Avgoustina Kyriakou, Eleni Koliou, Heraklis Pantelidakis, Andreas Chatzittofis in Lupus
Supplemental material
Supplemental material - Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis
Supplemental material for Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis by Konstantinos Parperis, Panagiotis Zis, Marina Evangelou, Avgoustina Kyriakou, Eleni Koliou, Heraklis Pantelidakis, Andreas Chatzittofis in Lupus
Supplemental material
Supplemental material - Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis
Supplemental material for Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis by Konstantinos Parperis, Panagiotis Zis, Marina Evangelou, Avgoustina Kyriakou, Eleni Koliou, Heraklis Pantelidakis, Andreas Chatzittofis in Lupus
Supplemental material
Supplemental material - Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis
Supplemental material for Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis by Konstantinos Parperis, Panagiotis Zis, Marina Evangelou, Avgoustina Kyriakou, Eleni Koliou, Heraklis Pantelidakis, Andreas Chatzittofis in Lupus
Supplemental material
Supplemental material - Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis
Supplemental material for Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis by Konstantinos Parperis, Panagiotis Zis, Marina Evangelou, Avgoustina Kyriakou, Eleni Koliou, Heraklis Pantelidakis, Andreas Chatzittofis in Lupus
Supplemental material
Supplemental material - Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis
Supplemental material for Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis by Konstantinos Parperis, Panagiotis Zis, Marina Evangelou, Avgoustina Kyriakou, Eleni Koliou, Heraklis Pantelidakis, Andreas Chatzittofis in Lupus
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article is available in the article.
Supplemental material
Supplemental material for this article is available online.