
Abstract
Background
Toxic epidermal necrolysis like lupus erythematosus (TEN-like LE) is a dermatological emergency associated with significant morbidity and mortality. It requires prompt recognition and differentiation from its mimics including drug induced toxic epidermal necrolysis, erythema multiforme, drug rash with eosinophilia and systemic symptoms, and reactive infectious mucocutaneous eruptions.
Objective
To assess systemically the clinical, pathological, and immunological features of patients with TEN-like LE.
Methods
We performed a structured search systematic review from April-May 2024, of studies on TEN-like LE published between 1977 and 2024., searching PubMed, Medline, Embase, SCOPUS, VHL, ProQuest, clinicaltrials.gov, COCHRANE, POPLINE, ISI, mRCT, UC library, and ResearchGate.
Conclusion
There were 16 case series and 52 case reports/conference papers yielding 112 unique cases. The mean age was 43.39 years, and 86.6% of cases were female. TEN-like LE was the presenting manifestation of lupus erythematosus (LE) in 48.21% of patients. Antinuclear antibody (ANA) was positive in all 109 patients where it was reported with SSA/Ro being most commonly positive (60.55%), followed by dsDNA (50%). Lesions were reported to be photodistributed in 78.57%, palmoplantar involvement was seen in 20.54%, and mucosal involvement was seen in 56.25%, with 26.78% patients having significant mucosal involvement. Lupus non-specific lesions were observed in 25% patients. Anemia, pulmonary and GI involvement were positively associated with hemodynamic instability, and anti-Ro antibodies were negatively associated. Positive dsDNA, La positivity, and low C4 were associated with increased odds of systemic involvement, whereas Ro positivity was associated with reduced odds. Seven patients had a paraneoplastic association. TEN-like LE can be the first manifestation of LE in up to half of cases. Photodistribution, lupus non-specific lesions, ANA positivity, or change in ANA type/titre can be important diagnostic clues. Unlike previously believed, mucosal involvement is not uncommon and can be severe.
Keywords
Key points
Why was the study undertaken?
Toxic epidermal necrolysis like lupus erythematosus (TEN-like LE) is a dermatological emergency associated with significant morbidity and mortality. It can be challenging to distinguish from mimics especially drug induced toxic epidermal necrolysis. There are no systematic reviews or diagnostic criteria addressing this condition.
What does this study add?
• This systematic review showed that TEN-like LE was the presenting manifestation of lupus erythematosus (LE) in 48.21% of patients. Photodistribution was seen in 78.57%, lupus non-specific lesions in 25% and mucosal involvement in 56.25%, with 26.78% having significant mucosal involvement.
What are the implications of this study for disease understanding and/or clinical care?
Mucosal involvement can be significant in TEN-like LE unlike previously believed. Distribution of lesions, evolution and presence of supporting non-specific lupus lesions, ANA positivity, histopathological and immunological features can be important diagnostic clues.
Introduction
Toxic epidermal necrolysis-like lupus erythematosus (TEN-like LE) is a rare lupus erythematosus (LE) subtype with clinicopathologic features of TEN. In a study of 9074 patients with cutaneous lupus erythematosus (CLE) and/or systemic lupus erythematosus (SLE), only 6 (0.07%) were diagnosed with TEN-like LE. 1 Both feature widespread blistering, epidermal necrosis, and keratinocyte apoptosis, termed acute syndrome of apoptotic pan-epidermolysis (ASAP). 2 The mechanism involves upregulation of Fas-Fas ligand interactions, cytotoxic T cells, cytokine release, and inflammation, causing epidermal basal cell apoptosis and epidermolysis. 2 While ultraviolet radiation plays a key role in LE, drug metabolism and elevated granulysin are key in TEN. TEN-like LE can occur in preexisting lupus, or as its first manifestation. In preexisting LE, erosive or bullous lesions may be mislabeled bullous LE, a process with tense subepidermal blisters with neutrophilic infiltrate, distinct from the dramatic interface dermatitis of TEN-like LE. Drug-induced TEN also occurs in LE patients, underscoring the importance of clinical judgment and drug causality assessment. For cases without lupus history, TEN-like LE may be mislabeled as SJS/TEN (Steven Johnson Syndrome/Toxic Epidermal Necrolysis, reactive infectious mucocutaneous eruption (RIME) or erythema multiforme (EM). We conducted a systematic review to identify clinicopathological and immunological features to propose diagnostic criteria, as well as predictors of clinically significant sequelae, including mucosal involvement and hemodynamic instability.
Material and methods
Literature search
Three reviewers (SS, TG, ZT) conducted a systematic review from April-May 2024, searching PubMed, Medline, Embase, SCOPUS, VHL, ProQuest, clinicaltrials.gov, COCHRANE, POPLINE, ISI, mRCT, UC library, and ResearchGate for articles, using terms “TEN like lupus”, “toxic epidermal necrolysis-like lupus erythematosus” and “TEN like lupus erythematosus”. Individual bibliographies were reviewed for relevant articles. We identified 107 articles (case series, case reports, abstracts) published between 1977 and 2024. After removing 24 duplicates, 83 articles underwent full text analysis and 68 articles (64 English, 3 French, 1 Spanish) were selected. Non-English articles were translated using Google translate. (Figure 1). PRISMA diagram.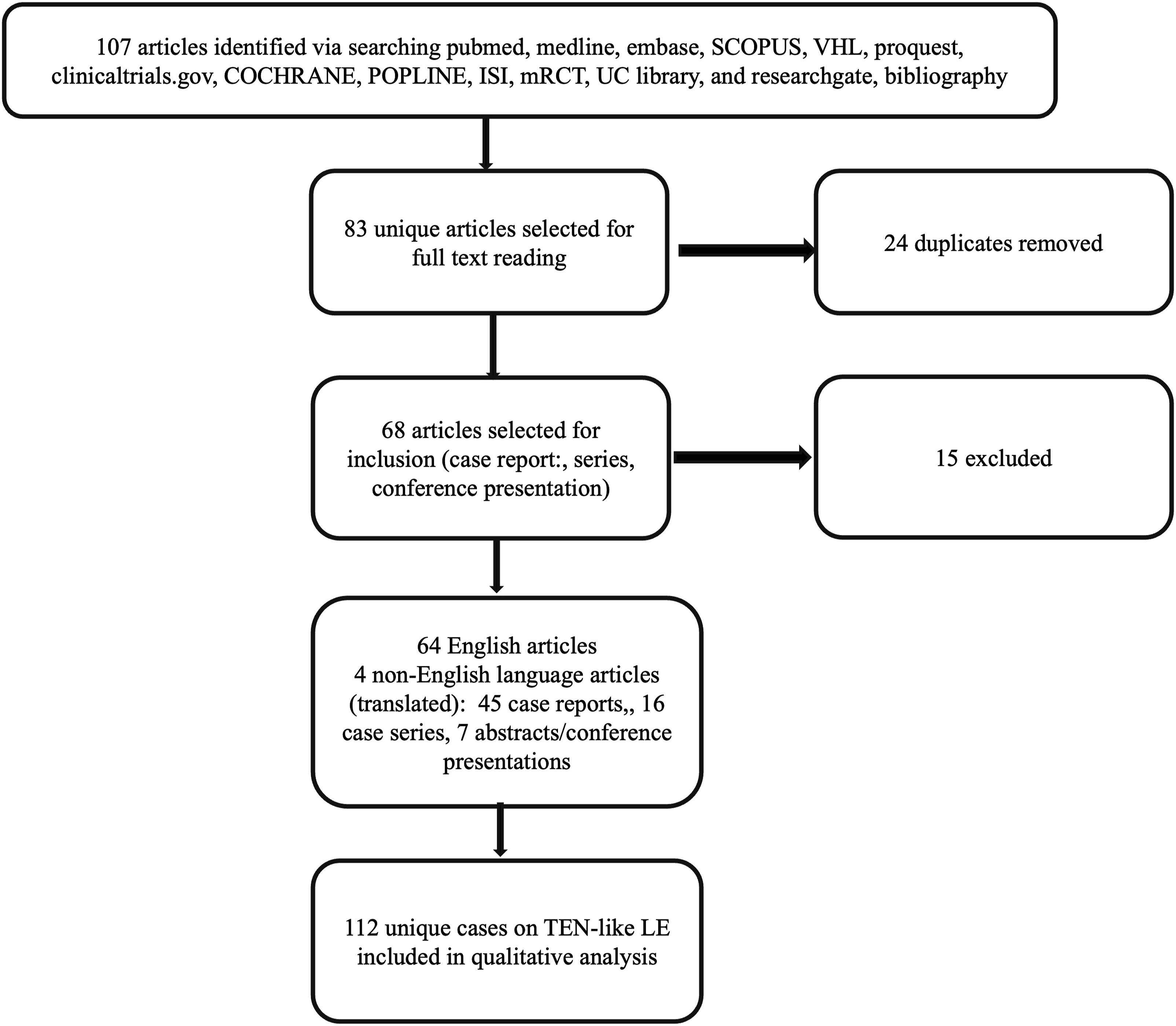
Inclusion and exclusion criteria
Articles describing clinical, pathological, or immunological parameters of TEN-like LE were included (Supplemental Table 1). Articles without a TEN-like lupus final diagnosis, reviews only, and articles without full text were excluded. Overall, 16 case series and 52 individual case reports/conference papers resulted in analysis of 112 unique cases.
Data extraction
Data were collected on age, sex, drug triggers in the last month, connective tissue disease (CTD) history, lesion distribution, lupus non-specific lesions, and palmoplantar and mucosal involvement. Significant mucosal involvement was defined as 3 or more sites affected, author-reported severe involvement, prominent hemorrhagic crusting, or assessed by two-reviewer analysis of case photographs when severity was not defined.
Systemic involvement included renal, cardiac, thromboembolic, gastrointestinal/hepatobiliary, pulmonary, infectious, neuro-psychiatric or paraneoplastic association. Hemodynamic status, mortality, and sequelae were also collected.
Laboratory results were collected for ANA positivity, titer, pattern and specific antibody type, complement, urinalysis, hematological and biochemical panels. When reported, we noted changes from baseline.
Histopathological information was collected: presence and extent of skin necrosis, inflammation, mucin, basement membrane thickening, and direct immunofluorescence (DIF). Biopsy-proven lupus nephritis was noted as renal involvement. TEN-like ACLE resembles exaggerated ACLE with interface dermatitis and inflammation, additional supportive features include positive staining for mucin and positive DIF at the dermo-epidermal junction (DEJ). The following changes were compatible with a pathological diagnosis of LE: vacuolar interface dermatitis with 1 or more of these features: dermal lymphocytic infiltrate, mucin, basement membrane thickening or DIF positivity (Granular IgG, IgM, and/or C3 blinding at the DEJ). TEN-like changes were required to have at least partial- or full-thickness epidermal necrosis since hallmark of TEN is widespread keratinocyte necrosis involving the epidermis with minimal inflammatory infiltrate.
Statistical analysis
Multivariate logistic regression tested predictors of mucosal involvement (> or < median of 2 sites), rash duration (> or < median of 20 days), and hemodynamic instability. The stepwise process began by narrowing significant bivariate predictors for each outcome through bivariate logistic regression. Tested predictors included age, systemic involvement (gastrointestinal (gi), cardiovascular, renal, musculoskeletal, pulmonary) mucosal site (nasal, eye, lip, genital), ANA titer >1:160, ANA pattern (speckled, homogenous, nucleolar, dsDNA, RNP, Ro, La, Smith), complement deficiency (C3, C4), cancer, anemia, leukopenia, CLE vs SLE, history of LE vs not, and the fulfillment of SLICC (Systemic Lupus Erythematosus International Collaborating Clinics ) vs not. Among this list, significant univariate relationships were then analyzed in adjusted multivariate analysis. Variables with a low number of observations and perfect relationships with the outcome were excluded, as these associations are not statistically reliable. Data were analyzed using SAS University (SAS Institute, Cary NC). Significance was reported when p < .05.
Results
Demographics
Comparison amongst different subgroups.
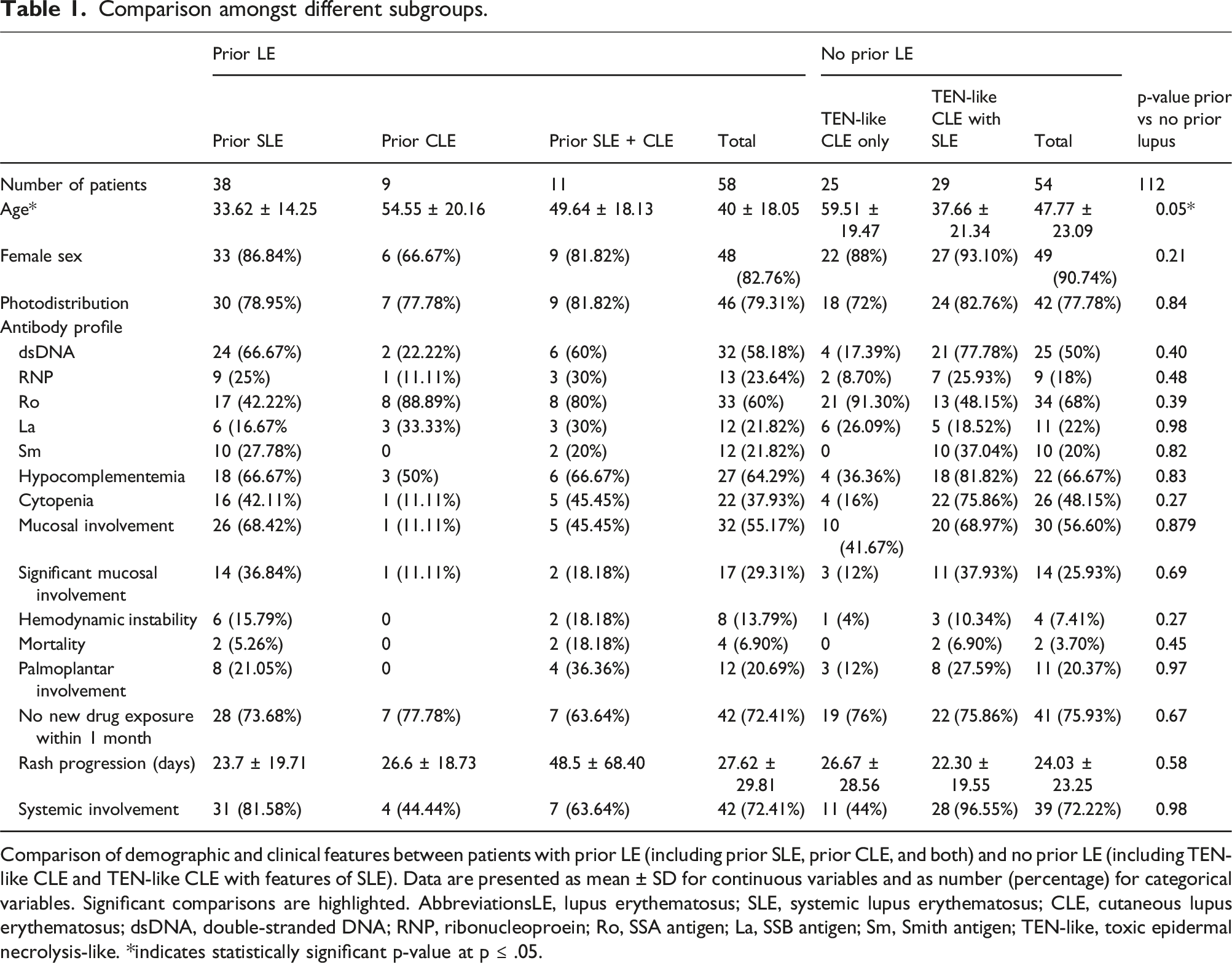
Comparison of demographic and clinical features between patients with prior LE (including prior SLE, prior CLE, and both) and no prior LE (including TEN-like CLE and TEN-like CLE with features of SLE). Data are presented as mean ± SD for continuous variables and as number (percentage) for categorical variables. Significant comparisons are highlighted. AbbreviationsLE, lupus erythematosus; SLE, systemic lupus erythematosus; CLE, cutaneous lupus erythematosus; dsDNA, double-stranded DNA; RNP, ribonucleoproein; Ro, SSA antigen; La, SSB antigen; Sm, Smith antigen; TEN-like, toxic epidermal necrolysis-like. *indicates statistically significant p-value at p ≤ .05.
History
A total of 54 patients had TEN-like LE as the first manifestation of LE, while 58 had prior lupus. Four cases were associated with CTD (systemic sclerosis, indeterminate autoimmune disease, Evans syndrome, Sjogren’s syndrome). New drug exposure occurred in 29 cases (25.89%). Half of patients had one or more constitutional symptoms, including fever (31, 27.68%), joint pain (33, 29.46%), and fatigue/malaise (19, 16.96%). Photosensitivity was reported in 33 patients (29.46%). Median disease progression was 21 days (mean 25.63).
Examination
Photodistributed lesions occurred in 88 cases (78.57%), palmoplantar involvement in 23 (20.54%), and lupus non-specific lesions (chilblains, oral ulcers, facial edema, alopecia, nailfold capillary changes, urticarial vasculitis) in 28 (25%).
Logistic regression: Predictors of >2 mucosal sites.
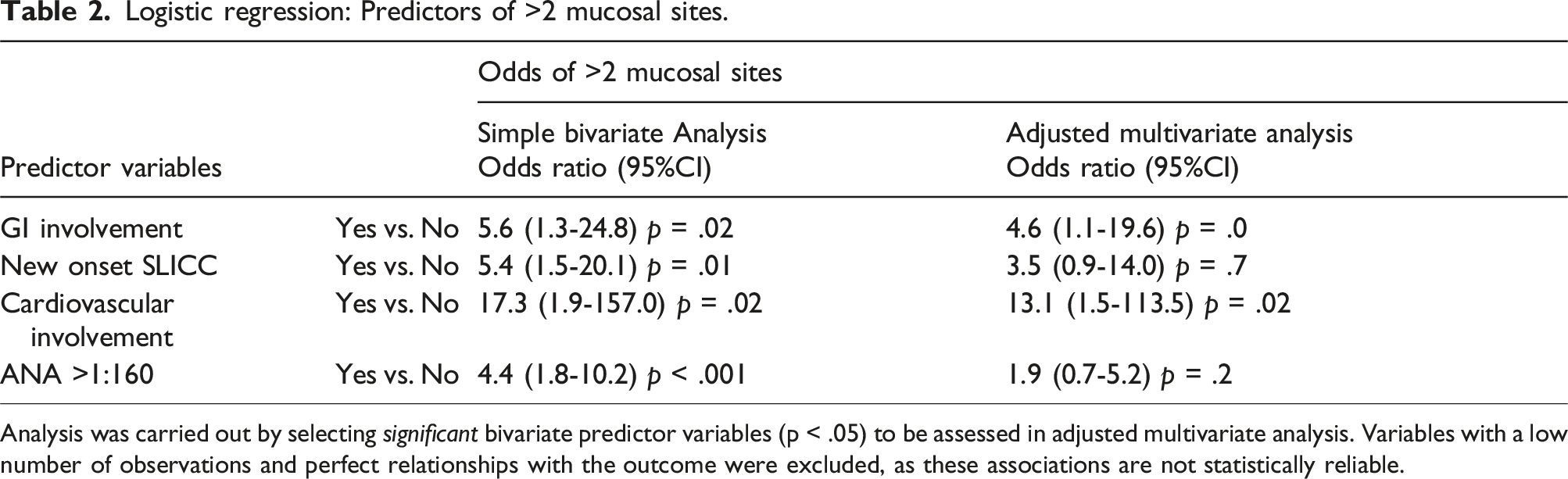
Analysis was carried out by selecting significant bivariate predictor variables (p < .05) to be assessed in adjusted multivariate analysis. Variables with a low number of observations and perfect relationships with the outcome were excluded, as these associations are not statistically reliable.
Logistic regression: Predictors of Mucosal Severity.
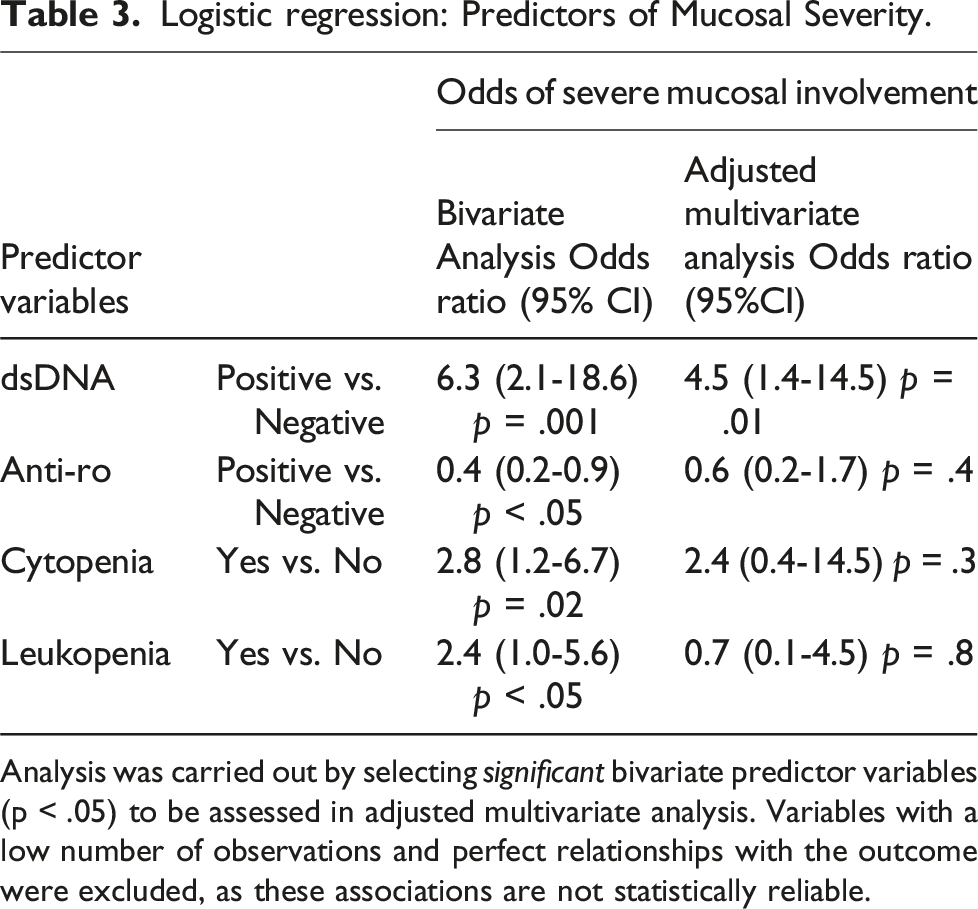
Analysis was carried out by selecting significant bivariate predictor variables (p < .05) to be assessed in adjusted multivariate analysis. Variables with a low number of observations and perfect relationships with the outcome were excluded, as these associations are not statistically reliable.
Laboratory evaluation
Immunology
ANA was positive in all 109 cases where reported, with SSA/Ro (66, 60.55%) and dsDNA 56 (50%) antibodies being most common. See table for ANA patterns and titer. Complement consumption was seen in 67.12 % of reported cases.
Pathology
Histopathologic features of both TEN and LE were seen in 65 patients (61.32% of 106 reported cases), LE-only features in 23.58%, and TEN-only features in 15.09%. Mucin deposition was positive in 80% of the 25 reported cases. DIF was positive for lupus changes in 44 (39.29%).
Hematology
Cytopenia occurred in 48 patients (42.86%), with anemia reported in 33 (29.46%) and leukopenia in 41 (36.61%).
Microbiology
Viral workup was reported in 30 patients and positive in 2 (both Herpes Simplex Virus-1 (HSV-1)).
Systemic involvement
Logistic regression: Odds of hemodynamic instability.
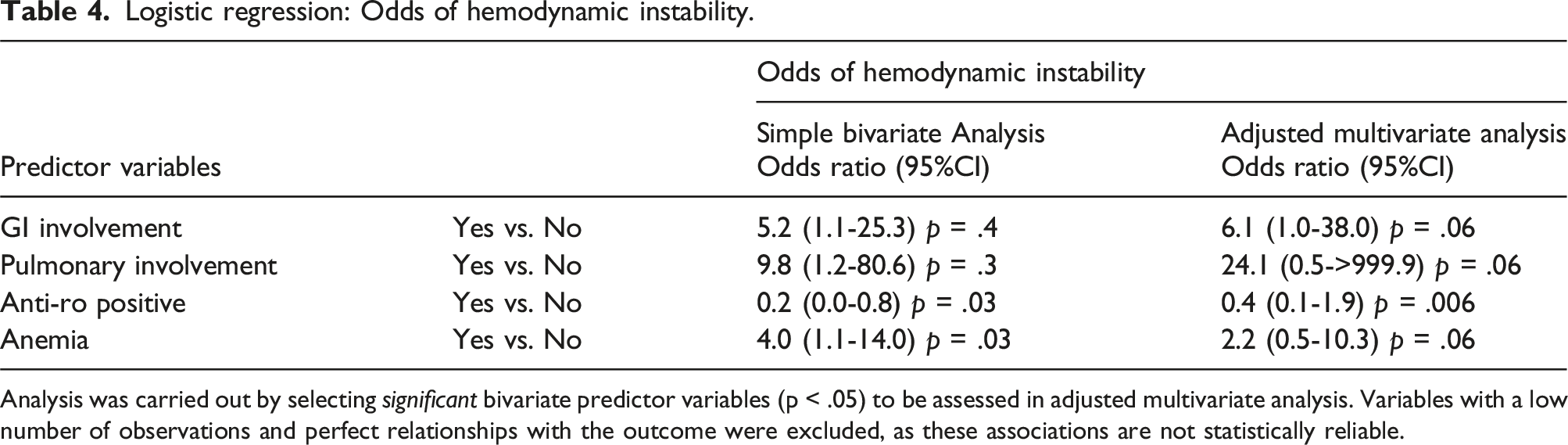
Analysis was carried out by selecting significant bivariate predictor variables (p < .05) to be assessed in adjusted multivariate analysis. Variables with a low number of observations and perfect relationships with the outcome were excluded, as these associations are not statistically reliable.
Positive dsDNA, La, and low C4 were associated with increased odds of systemic involvement (excluding paraneoplastic association), whereas Ro positivity was associated with reduced odds. Hematological systemic involvement was most common, followed by musculoskeletal and renal. (Supplemental Table 2)
Association with malignancy
Paraneoplastic associations were seen in 7 (6.25%) patients, including lung and breast cancer, as well as uterine leiomyosarcoma, esophageal adenocarcinoma, colorectal adenocarcinoma, and cholangiocarcinoma. Only one had prior subacute cutaneous lupus erythematosus (SCLE); six had new-onset LE. All were positive for SS-A/Ro, and 1 also had SS-B positivity. Two (28.57%) were male, compared to 13 (12.38%) in the non-paraneoplastic group. Mean age was 73.69 years, as compared to 41.37 years in patients without malignancy. ANA titre was available for only 3 patients (1:80, 1:160, 1: 1260). None had mucosal involvement or met SLICC criteria. All had SCLE-like lesions during their course.
Sub analysis based on history of lupus
Fifty-eight total patients had prior LE, 31 (53.45%) of which with current dsDNA positivity. Six patients with prior dsDNA positivity had increased titer (magnitude unavailable), and two had new-onset dsDNA positivity (1 CLE, 1 SLE). Titers and changes were unavailable for the rest. Two cases with prior dsDNA positivity became negative during the TEN-like LE episode and acquired a new antibody (SS-A/Ro in both, and U1RNP in 1). Complete characteristics and comparisons are available in Table 1.
Discussion
TEN-like LE is a severe spectrum of LE-associated cutaneous features secondary to exaggerated interface dermatitis, often triggered by ultraviolet exposure in patients with LE or other predisposition. 3 Type 1 interferon and autoreactive cytotoxic T lymphocytes trigger proinflammatory cytokines, causing interface dermatitis and keratinocyte apoptosis. 4 This review serves to clarify TEN-like LE diagnosis and its differentiation from SJS/TEN, which is critical for guiding prognosis and therapy. This review provides diagnostic guidance and proposes TEN-like LE diagnostic criteria.
The demographics in our analysis of TEN-like LE cases align with previously reported findings, where patients tended to be younger and predominantly female compared to SJS/TEN patients.5,6 This female predominance mirrors SLE, where up to 90% of affected individuals are female. Differences in sex hormones, immune system, gene regulation, and environmental factors between genders may explain sex differences. 7 Since TEN-like LE is an exaggerated immunological response in lupus, a similar pattern is expected; however, more insight into the cellular biomarkers, blood transcriptomics, and genetic factors would further clarify pathogenesis.
Similar to the data reported by Truong et al., and Tankunakorn et al., we found that TEN-like LE was the initial manifestation of lupus in around half of TEN-like LE cases.1,5 It has been posited that TEN-like LE can be differentiated from SJS/TEN based on its more limited mucosal involvement,5,8 though mucosal involvement is not unique to SJS/TEN. 10 In a retrospective study of 9 patients with TEN-like LE, 66.67% had mucosal involvement, with 22.22% considered severe. 9 Similarly, our review found 56% of cases had mucosal involvement, with 26.78% classified as significant. TEN-like LE affected the lips and oral mucosa most commonly, but genital, ocular, and nasal mucosa involvement was also noted. SJS/TEN can affect the oropharynx, conjunctiva, genitalia, and anus, making mucosal involvement an unreliable differentiator. 10
TEN-like LE typically begins as a photodistributed eruption, 9 whereas TEN is usually generalized. Nine cases of photodistributed TEN have been reported, eight of which had a plausible temporal drug exposure, including one involving long-term hydroxychloroquine use.11,12 It is difficult to determine if these were true TEN or first-episode TEN-like LE, underscoring the importance of long-term follow-up to avoid missing TEN-like LE. In true drug-induced photodistributed TEN, intense UV exposure may act as “second hit” in predisposed individuals.
Most cases reviewed included a skin biopsy, helpful in distinguishing TEN-like LE and TEN. The hallmark of TEN is widespread keratinocyte necrosis involving the entire epidermis with minimal inflammatory infiltrate. 13 Although TEN-like ACLE demonstrates similar apoptotic keratinocytes, it also has features of acute cutaneous SLE, 14 including interface dermatitis with vacuolization and lymphocytic infiltrate, indicating a more inflammatory process. 15 Further supportive findings include positive staining for mucin and positive DIF at the DEJ,14,15 seen in 80% and nearly 40% of cases, respectively. For equivocal cases, investigating for vacuolar changes, inflammatory infiltrates, staining for mucin and DIF, along with serologic markers, may aid diagnosis. Zeimer et al also summarized above as specific epidermal and dermal changes associated with TEN-like LE and SJS/TEN. 8 A deep tangential biopsy can be helpful when TEN-like LE is suspected, to provide the largest yield to assess for findings consistent with LE.
Serologic findings in TEN-like LE closely mirror those of SLE, including high ANA titers and lupus-specific antibody positivity. 1 Lupus-specific antibodies including anti-dsDNA (present in 70% of SLE patients), anti-Smith (30%), anti-Ro/SSA (30%), anti-La/SSB (20%), and anti-U1 RNP (25%) can indicate disease presence and severity. 16 Decreased complement (C3, C4, and CH50) may also indicate active SLE flares.17,18 Markers of active disease such as hypocomplementemia, and elevated inflammatory markers (erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)) have also been observed in TEN-like LE. 1 In a retrospective evaluation of 9 patients with TEN-like LE, anti-Ro antibodies were found in 8 individuals, anti-dsDNA in 4, anti-RNP in 3, and anti-La and anti-Sm in 2. One patient had elevated anti-dsDNA antibodies and hypocomplementemia, and another had hypocomplementemia and leukopenia. All were negative for Mycoplasma and Herpes virus. 9 Similarly, in our review, only 2 patients had positive viral workups. Evaluation for infectious etiology is important in cases where EM or RIME cannot be ruled out.
Unlike TEN-like LE, SJS/TEN does not exhibit a unique serologic profile, and the prevalence of ANA positivity in SJS/TEN remains unclear. However, recent studies have proposed elevated complement in SJS/TEN, 19 along with a transient rise in anti-SSA antibodies during acute SJS/TEN. 20 This differs greatly from the strong correlation between high ANA titers and presence of autoantibodies seen in TEN-like LE, serving as a crucial distinguishing factor between SJS/TEN and TEN-like LE.
Mislabeling TEN-like LE changes as SJS/TEN risks both undertreating the underlying etiology and unnecessarily avoiding bystander medications, some of which may be essential for treatment of various systemic issues. In equivocal cases, clinical diagnostic clues, laboratory work-up, and drug causality assessment are recommended.
Paraneoplastic
There are several proposed mechanisms for pathogenesis of paraneoplastic rheumatological disorders.21,22 Malignant cells may produce cytotoxins which can trigger inflammation at target sites, or an underlying infectious trigger may predispose to both neoplasm and rheumatological disorder. Alternatively, anti-tumor response may entail production of antibodies against self-antigens (such as dsDNA) expressed by tumor cells undergoing apoptosis, eliciting an autoimmune response. 23 It is possible that the tumor expresses antigen similar to SS-A/Ro, as suspected by the prevalence of this antibody and SCLE like lesions in paraneoplastic TEN-like LE in our analysis.
Our review found that 7.14% of TEN-like LE cases occurred in patients with known cancers, raising the possibility of TEN-like ACLE as a paraneoplastic dermatosis. The link between lupus and its many variants and cancer has been discussed throughout the literature, with recent studies reporting diagnosis of malignancy within an average of 5 years of SLE diagnosis. 24 The reported rate of malignant neoplasms was 3.6/1000 (95% CI, 1.5-8.8) patient years, while those of benign tumors is 14.6/1000 (95% CI 8.9-22.5) patient-years. The crude incidence odds ratio for malignant neoplasm was 3.5 (95% CI, 1.5-7.9). However, the incidence of paraneoplastic SLE remains rare, 25 with reported associations with colorectal cancer, leukemia, cholangiocarcinoma, breast cancer, ovarian cancer and thyroid cancer.23,25–27
Similarly, SCLE has been reported in the setting of malignancy (approximately 37 cases), most commonly breast and lung. 28 Given these known instances of paraneoplastic LE and a significant number of cases in our review associated with cancer, TEN-like LE may represent a paraneoplastic process in some patients. Older age, minimal or no mucosal involvement, SCLE lesions, presence of SS-A antibodies and features of underlying malignancy such as asthenia, weight loss, known ongoing malignancy may be important clues to this association.
Diagnostic clues
Though TEN-like LE can present very similarly to TEN, several clues can aid in differentiating the two. The temporal absence of a known drug trigger, as well as photodistribution, observed in close to 80% of TEN-like LE cases, are important clues. A thorough physical exam, including examination for lupus non-specific lesions of chilblains, oral ulcers, facial edema, alopecia, nailfold capillary changes, and urticarial vasculitis. In the context of a patient with a clinical picture of epidermal necrolysis, these are suggestive of an autoimmune process, such as TEN-like ACLE.
Additionally, the clinical course of the eruption differs: TEN-LE is characterized by a slower progression over days to weeks versus the rapid evolution of TEN over hours to days. A comprehensive review of systems is also helpful. Patients with TEN-like ACLE may exhibit symptoms of SLE–several cases demonstrated photosensitivity, joint pain, fever, and fatigue, in contrast to prodromal flu-like symptoms of TEN, which typically precede the skin eruptions by days. These clinical tools, in conjunction with serologic and histologic testing, help ensure that the diagnosis of TEN-like ACLE is not missed.
Proposed diagnostic criteria
There are currently no standardized criteria for the diagnosis of TEN-like lupus, complicating formal diagnosis. Utilizing the clinical, histologic, and serologic features noted during this review, we propose two sets of criteria: one for patients who have a known diagnosis of LE, and one for those without known history of LE. This differentiation is important for distinguishing classic TEN from TEN-like LE in patients who already carry a diagnosis of LE. (Figure 2) Suggested preliminary diagnostic criteria for TEN like LE.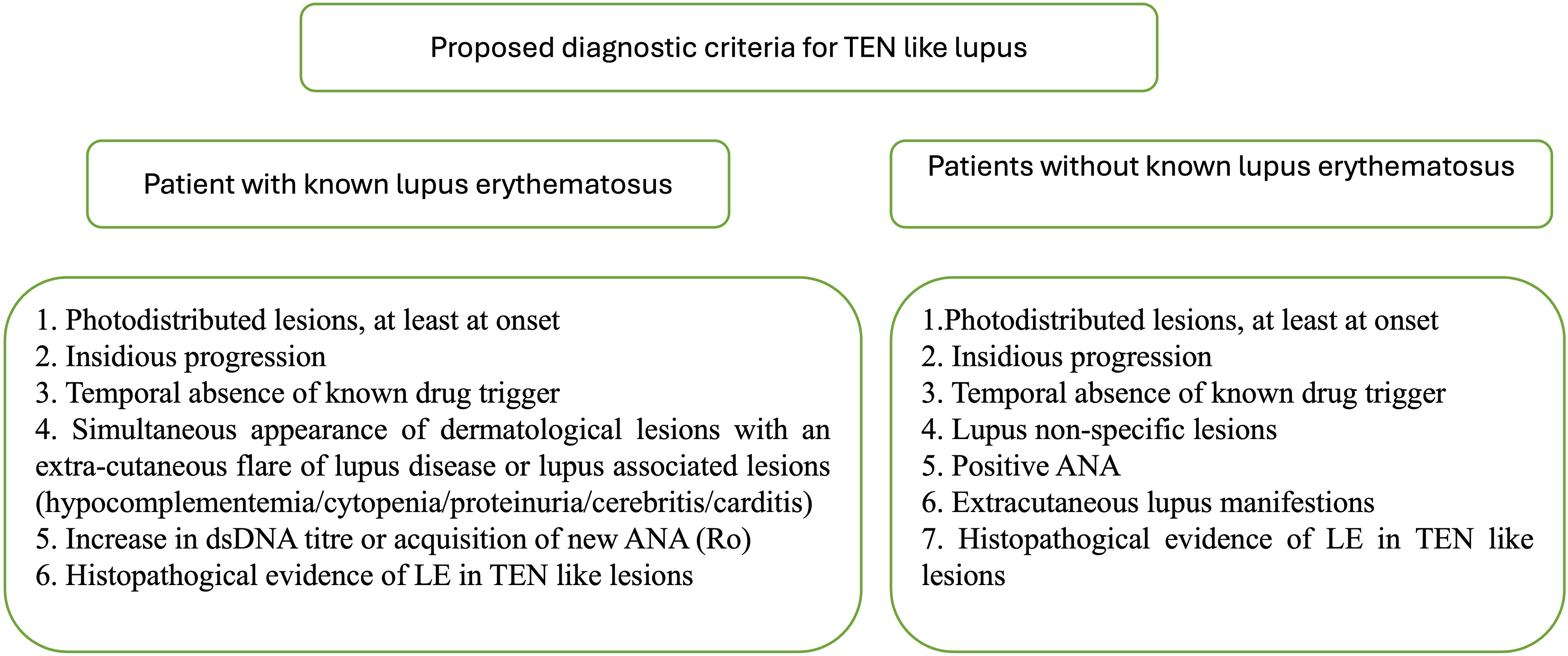
limitations
The main limitations of the study are its retrospective nature and inconsistent reporting across cases, with some lacking data points of interest. SLEDAI (SLE disease activity index) and SLICC/ACR were not reported for all the cases, so authors applied SLICC based on available data. A drug causality algorithm could not be applied, due to reliance on individual reports rather than registry data. We assessed new drug exposure within the typical 1-month latency period for TEN, though latency may rarely be longer. Cases of Rowell’s syndrome were excluded, as there is some uncertainty about if it is a separate condition entirely, or on the TEN-like LE spectrum. 29 Further consensus on nomenclature is warranted.
Supplemental Material
Supplemental Material - Clinical, pathological and immunological features of toxic-epidermal necrolysis like lupus erythematosus: A systematic review and proposal for diagnostic criteria
Supplemental Material for Clinical, pathological and immunological features of toxic-epidermal necrolysis like lupus erythematosus: A systematic review and proposal for diagnostic criteria by Sweta Subhadarshani, Taylor Griffith, Zachary Thornton and rew Nicholas in Lupus.
Footnotes
Author contributions
Sweta Subhadarshani: Conceptualization, Methodology, Data curation, Writing- Original draft preparation, Supervision. Taylor Griffith: Methodology, Data curation, Writing- Original draft preparation. Zachary Thornton: Data curation, Writing- Original draft preparation. Andrew Nicholas: Data curation, Writing- Original draft preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.