
Abstract
Introduction
Previous studies indicate that the prognosis of systemic lupus erythematosus (SLE) is poor in Africa. We surveyed African physicians for their perceptions of factors that impact negatively on optimal SLE care and interventions to improve care in Africa.
Methods
A cross-sectional, online survey of African dermatologists, rheumatologists, nephrologists, and internists was conducted.
Results
Responses from 226 respondents mostly from West Africa and East Africa, majority practicing in university and state-funded hospitals showed that the commonest reasons for late diagnosis of SLE in Africa were lack of awareness of the disease amongst primary care doctors (92.4%), financial constraints (80.3%) and lack of access to health care (62.5%). Consulting traditional healers, the belief of bewitchment, lack of availability of diagnostic tests and concomitant chronic infections, (tuberculosis and HIV) were also perceived to have resulted in diagnostic delays, especially amongst East and West African respondents. The overwhelming majority (>90%) of respondents felt that increased health care and financial resources was the top priority to improving SLE care in Africa. Continuing medical education for generalists, training of specialists and patient education and awareness programs were considered less important interventions to improve SLE care.
Conclusion
The study reveals that the primary reasons for late diagnosis of SLE in Africa are lack of awareness among primary healthcare doctors and financial constraints. Thus, the need for greater financial resources, especially for appropriate medications, medical education and improving patient understanding of the disease through support groups, to improve SLE care and outcomes in Africa.
Systemic lupus erythematosus (SLE) is a prototype systemic autoimmune rheumatic disease that is especially common in women in the childbearing years. 1 The disease affects especially women of African extraction living in Western industrialized countries in whom the disease is also more aggressive than in other ethnic groups. 2
The notion and apparent paradox that SLE is rare in indigenous Africans compared to those of African descent such as African Americans has recently been refuted. 3 Whilst there have been no formal epidemiological studies of SLE in Africa, several recent clinical studies suggest that the disease is far more prevalent than previously thought.4,5 A meta-analysis by Essouma et al. found an estimated pooled SLE prevalence of 1.7% in 28,575 native sub-Saharan Africans, mainly from West Africa. 6 Similar studies from Kenya, Ghana, Zimbabwe, Democratic Republic of Congo show increasing prevalence.7–9
The aggressive nature of SLE, especially renal disease, and associated poorer outcomes in patients of African extraction compared to Caucasians is the result of a combination of genetic and socio-economic factors. 2 The number of genetic risk alleles has been shown to be significantly higher than in Caucasians. 10 Several studies conducted in the United Kingdom (UK) and the United States (US) have demonstrated that the severity of disease and unfavourable outcomes in SLE patients of African descent are associated with financial challenges and the consequent lack of access to healthcare, medications, and social support.9,11 Limited studies from Africa show that poor long-term outcomes of SLE is related to late presentation, high prevalence of lupus nephritis and infections, particularly tuberculosis (TB) and human immunodeficiency virus (HIV) infection.12,13
Given that Africa has the lowest gross domestic product (GDP) of all the continents, and consequently the least access to health care, we surveyed physicians involved in SLE care across Africa on access to investigations, drug therapies and special supportive care, including renal dialysis, relevant to SLE care. 13 Here we report the physician perceptions of SLE care in Africa and factors that negatively impact on optimal SLE care.
Methods and participants
A cross-sectional, online questionnaire-based survey, previously described, 14 of African specialist physicians, mainly rheumatologists, nephrologists, and dermatologists, was conducted over a 3-month period, July to September 2022. Briefly, questionnaires were disseminated using social media platforms and personal email communication. Participation by respondents was deemed as consent to participate in the survey. Data were collected via Google form (Appendix A).
The four main domains of the questionnaire were: (1) Personal/demographics of respondents (2) Availability and turnaround times of special serological tests, histopathology, and imaging relevant to SLE (3) Availability of drugs and specialized care services (4) Perceptions of respondents of the challenges and barriers to optimal SLE care in Africa and measures to improve SLE care.
Findings of the first three domains have been recently published. 14 Here, we present the findings of the fourth domain only. African regions were defined according to the United Nations Organization groupings into North, South, East, West and Central Africa (Appendix B). 15 The study was approved by the Biomedical Research Ethics Committee of the University of Kwa-Zulu Natal (BREC:00004044/2022).
Statistical methods
Responses are expressed as numbers and percentages. Unpaired t test or Mann Whitney test was used to compare continuous variables between two groups depending on whether the data were distributed normally or skewed, respectively. Chi square for trend test was applied to test for differences between the four regions. A p value <.05 was regarded as statistically significant. All statistical analyses were performed using MedCalc Statistical Software version 22.019 (MedCalc Statistical Software version 19.2.6 (MedCalc Software bv, Ostend, Belgium; https://www.medcalc.org; 2024).
Results
Characteristics of African physicians and responses to delays in diagnosis of systemic lupus erythematosus in Africa.
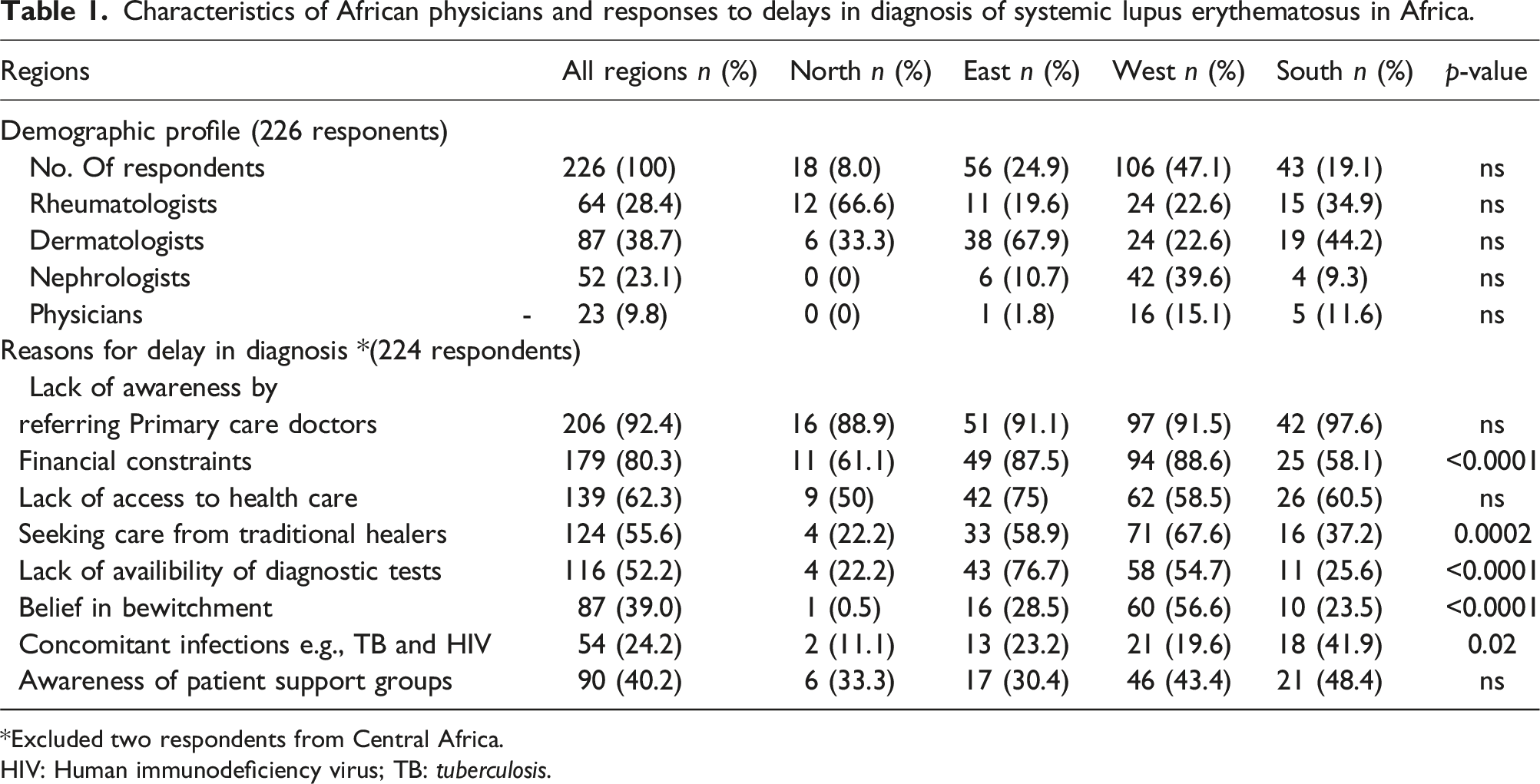
Excluded two respondents from Central Africa.
HIV: Human immunodeficiency virus; TB: tuberculosis.
The most common reasons for late diagnosis of SLE in Africa in the opinion of the respondents were lack of awareness by referring primary care doctors (92.4%), followed by financial constraints (80.3%) and lack of access to health care (62.5%). Other reasons were consulting traditional healers (55.6%) and belief of bewitchment (39.0%). Just over half the respondents also perceived that lack of availability of diagnostic tests hampered early diagnosis and a quarter felt concomitant infections including TB and HIV resulted in diagnostic delays. East and West African respondents were most affected by financial constraints and lack of availability of diagnostic tests compared to North and Southern African respondents. Consulting traditional healers and belief in bewitchment were perceived especially in West Africa as factors contributing to late diagnosis. Significantly more respondents from Southern Africa felt that concomitants chronic infections, TB and HIV, contributed to delay in diagnosis of SLE. Less than half the respondents were aware of SLE patient support groups, and these were mostly found in Southern (48.4%) and West Africa (43.4%), and the least in East Africa (30.4%) (Table 1).
Responses of 224 African physicians regarding reasons for poor outcomes and measures needed to improve care in SLE patients in Africa.
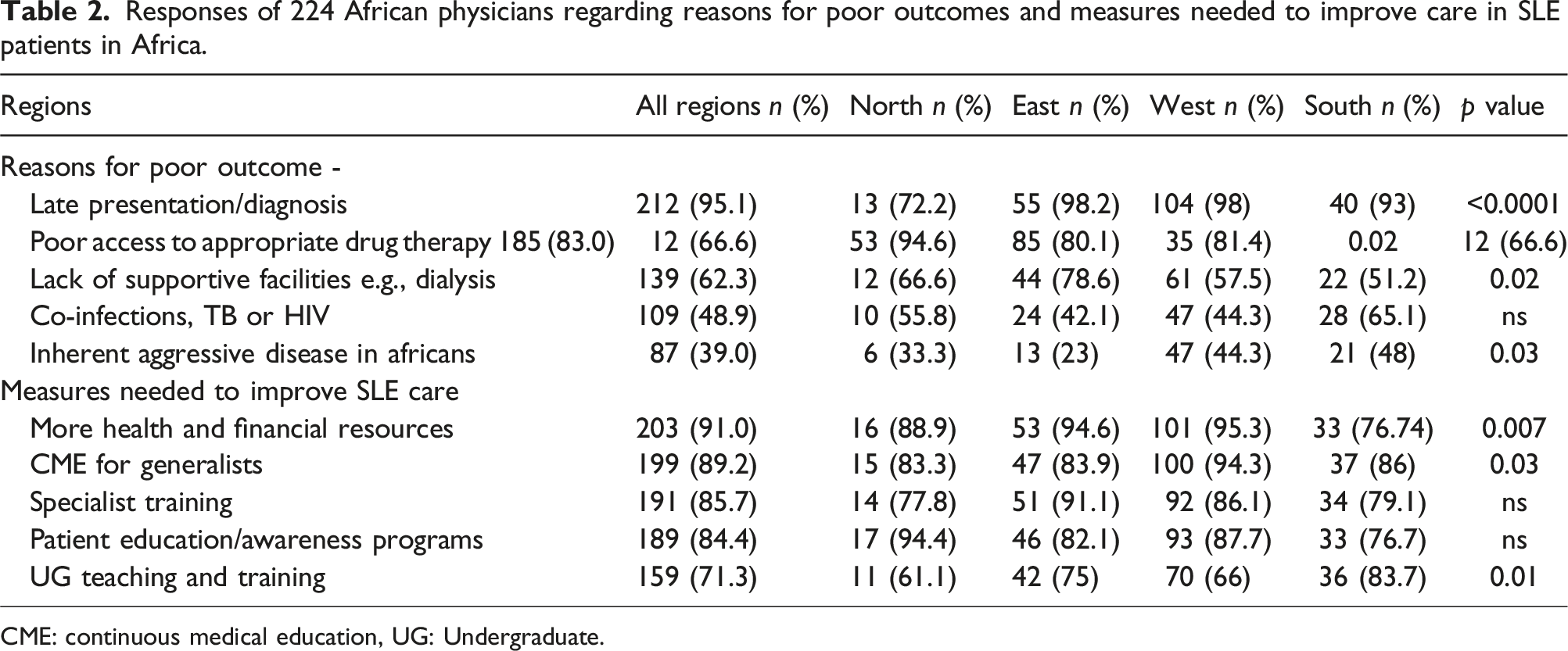
CME: continuous medical education, UG: Undergraduate.
Respondents felt that various measures were needed to improve SLE outcomes, especially increased financial and health resources (91%), continuing medical education (89.2%) for generalists, specialist training (85.7%) and patient education (84.8%). Notable differences between the regions were that East and West African respondents expressed a greater need for financial and health resources and specialist training compared to the other regions and the need for patient education was deemed to be significantly more important in North Africa than the other regions.
Discussion
This online survey of specialists involved in the care of SLE patients in Africa revealed a wide range of factors that were perceived to negatively impact SLE outcomes on the continent. External factors were considered most important and included poor awareness of SLE, inadequate financial and health care resources, lack of access to diagnostic tests and medications specifically for SLE and general supportive care facilities. Inherent ethnic and genetic factors were less important determinants of poor outcomes in SLE.
The early non-specific protean manifestations of SLE often result in delays in diagnosis,16,17 Moreover, the complexity of symptoms and signs of SLE are often challenging to primary health care professionals. Previous studies showed that SLE patients often have frequent consultations before diagnosis is confirmed and the average delay to diagnosis of up to 5.5 years has been reported in Germany and US studies.18–21 Delays to diagnosis are known to impact negatively on health-related quality of life, mortality and increase in health care costs. 22 Not surprisingly, most respondents in the present study felt that the lack of awareness of the disease amongst primary care doctors was the most frequent reason for delays in SLE diagnosis. The lack of awareness is further compounded in Africa by the misperceptions that SLE is rare on the African continent.6,12
Financial constraints were cited as the second most common reason for delays in diagnosis in Africa. This is not surprising given that both direct and indirect costs for SLE patients have been shown to be as much twice that for the general population in a US study.23,24 The cost drivers being higher number of health care visits and costly investigations and medications, coupled with associated loss of work potential. Given that Sub-Saharan Africa has 19 of the 20 countries with the lowest estimated GDP globally, 25 it is therefore not unexpected that SLE survival rates in Africa are worse than in wealthy western industrialised countries. 26
The impact of socio-economic conditions on morbidity and mortality has been repeatedly demonstrated in US and UK studies where affluent, mostly Caucasian SLE patients, have a better prognosis and survival compared to less affluent, mostly people of African descent. 27 Moreover, health care resources vary on the African continent, with East and West Africa regions having less resources compared to North and Southern African regions and therefore patients in the former regions are less likely to be diagnosed and have optimal management of SLE. For example, a recent survey showed that North Africa had the equivalent to 1.21 rheumatologists/100 000 population, whereas East or West Africa had 0.004 and 0.12 rheumatologists/100 000 population, respectively. 28 Other than the financial constraints, serological tests such as ANA, dsDNA, and complement (C3/C4) and renal histopathology are not readily available locally in many countries and are sent to South Africa and Europe.14,29 This results in increased costs and prolonged turnaround times for results which potentially delays and compromises patient care.
Traditional healers play a significant role in health care in sub-Saharan Africa.4,30–33 Respondents from especially West and East Africa perceived that seeking care from traditional healers, coupled with cultural beliefs on bewitchment, impacted negatively on time to diagnosis. This is consistent with a recent combined qualitative and qualitative study of health-seeking behavior in patients with systemic autoimmune rheumatic disease in Ghana 30 which found that about a quarter of patients attributed illness to spiritual factors, particularly those with neuropsychiatric symptoms, and attended prayer camps and consulted herbal clinics. A qualitative South African study found that patients felt that spirituality played a significant role in coping with the disease. 33 Spiritual connotations of illness have been similarly observed in a qualitative study of diabetes in Ghana where witchcraft and sorcery were implicated as causes of the disease and Church prayers were seen as spiritual mediation. 34
The highest burden of HIV worldwide is in sub-Saharan Africa and affects especially young women. 35 Given that several of the clinical and laboratory features of HIV overlap with SLE, diagnosis of either disease or co-existence of the two diseases can often be a diagnostic and management challenge.36,37 This is reflected in the present study where almost 50% of respondents, especially respondents from Southern Africa which has the highest burden of HIV, felt HIV/TB coinfections were an important reason for diagnostic delays and poor outcomes in SLE.
As regards measures to improve SLE care, the overwhelming majority (>90%) of respondents felt that increased health care and financial resources was top priority. Continuing medical education (CME) for generalists, training of specialists and patient education and awareness programs were considered less important interventions to improve SLE care. These findings are understandable given that infectious diseases dominate the landscape, and chronic non- communicable diseases are not considered a priority especially in sub-Saharan Africa.12,38
A major limitation of the survey was the discordant response rates from the different regions, with only two responses from Central Africa and relatively low response rates from North Africa, considering that this region has the highest concentration of rheumatologists. 28 The overall response from the rheumatology fraternity represents less than 10% of rheumatologists in the continent. 28 A further limitation was we did not explore patient adherence to therapy. Another limitation is the inherent biases associated with subjective responses that are influenced by individual experiences and perceptions of individual respondents.
In summary, the commonest perceived reasons for late diagnosis in SLE in Africa were lack of awareness of SLE by referring primary health care doctors and financial constraints. Respondents felt that the most important interventions required to optimize and improve SLE outcomes in Africa were greater financial and health resources, providing education for both health care professionals and patients, the latter including support groups. This study highlights the need for greater financial resources, especially for appropriate medications, medical education and improving patient understanding of the disease through support groups.
Supplemental Material
Supplemental Material - Physician perceptions of challenges and barriers to optimal care of systemic lupus erythematosus in Africa
Supplemental Material for Physician perceptions of challenges and barriers to optimal care of systemic lupus erythematosus in Africa by Farhanah Paruk, Dzifa Dey, Anisa Mosam, Oluwaytoyin Christina Amira and Mohammed Tikly and Adam Metzler in Lupus
Footnotes
Acknowledgments
The authors would like to thank all the participants who contributed to this study.
Author contributions
All authors participated in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. All authors had full access to the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Study Conception and design: Paruk F, Dey D, Mosam A, Amira O, Tikly M. Analysis and interpretation of data: Paruk F, Tikly M. Final write up: Paruk F, Dey D, Mosam A, Amira O, Tikly M.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.