
Abstract
Objective
To evaluate the potential of chimeric antigen receptor T-cell (CAR-T) therapy in revolutionizing the treatment of systemic lupus erythematosus (SLE) and to outline necessary future steps for its implementation.
Methods
A careful literature search was conducted for relevant English language papers on pubmed.
Results
Preliminary data suggest that CAR-T therapy could significantly improve SLE outcomes. Demonstrating remarkable clinical and serologic improvements in SLE patients, with all treated patients achieving remission and discontinuing conventional steroids and immunosuppressive drugs. To realize this potential, it is imperative to advance our understanding and application of CAR-T therapy. Rigorous research is necessary to validate current findings, and clinical trials must be conducted to assess both the short- and long-term efficacy and safety across diverse populations. Identifying appropriate patient populations is crucial, as CAR-T may also address compliance issues. Despite its current high cost, the financial burden is comparable to the long-term costs of severe SLE treatment. Strategies to reduce costs, including production efficiencies and outpatient treatment options, are under exploration. Early intervention could enhance its feasibility and impact on long-term prognosis.
Conclusion
CAR-T therapy holds promise for altering the prognosis of SLE and potentially offering a cure. However, substantial efforts are required to validate its efficacy, ensure safety, identify suitable patient cohorts, and reduce financial barriers. This development represents an exciting advancement in SLE treatment, necessitating urgent and focused research and clinical application.
Introduction
The outlook for patients with systemic lupus erythematosus (SLE) treated with conventional immunosuppression, corticosteroids and hydroxychloroquine has hardly changed in the last 30 years 1 ; this is particularly true for patients with lupus nephritis. 2 Unlike the treatment of rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis, the number of biologic drugs available for the treatment of SLE is restricted. In the United Kingdom (UK), only rituximab [anti CD20] and benlysta [anti B-cell activating BAFF] are readily available. In the United States (USA), anifrolumab (anti interferon alpha receptor) is also approved by the Federal Drug Administration [FDA] and in China telitacicept, [anti B-cell activating factors BAFF and1 APRIL] is also officially sanctioned.
The strategy of B-cell depletion in SLE is over two decades old. Most of these treatments have been developed for haematological malignancy. The first used in SLE was rituximab and later successful trials with Obinutuzumab (both anti CD-20). Later chimeric antigen receptor – T cells (CAR-T) were utilized. The most recent development is bispecific T-cell engagers (BiTE).
CAR-T was developed for the treatment of lymphomas. 3 The treatment has been attempted in aggressive and hard-to-treat SLE.4–6 The numbers of patients treated to date is small; the principal report so far has come from Schett et al. in Germany where one to 3-year follow-up of eight patients has been reported. The results are most remarkable.
The patients are lymphodepleted prior to CAR-T treatment with cyclophosphamide and fludarabine. Their T-cells are genetically modified to identify the CD19 marker present on a wide variety of B-cells, and plasma cells. Dramatic clinical and serologic improvements have been reported (anti-dsDNA antibodies and C3 levels all normalise by 3–6 months). At 6 months all the patients met the definition for remission in lupus and conventional steroids and immunosuppressive drugs were stopped. This result is truly notable, and we are unaware of any other therapy which has achieved such a response. However, clearly this treatment should only be attempted in highly specialised centres.
The immune system that “re-emerges” after treatment is remarkably normal. There is minimal effect on previous vaccinations antibody levels and patients respond to tetanus toxoid, pneumococcal and SARs-Cov-2 vaccines. Lupus associated autoantibodies previously present in these patients have not re-emerged after 1 year of follow-up.4–6
It remains an article of faith that physicians would like to cure lupus, it is clear that neither conventional immunosuppression, nor biologic drugs available have that capacity. In contrast, CAR-T therapy as reported might, just might be the first approach where using the word cure is realistic.
Considerations and future steps
We need to consider, urgently, what else needs to be done and how to achieve this, so that talk of cure is not a false hope for our patients or an unrealistic goal for physicians.
It is possible the response of the patients might partly be due to lymphodepletion. It would be ideal to perform a controlled study comparing CAR-T therapy plus fludarabine and cyclophosphamide to a “dummy procedure” plus fludarabine and cyclophosphamide; however, such a study would have questionable ethics considering the lack of data regarding fludarabine in lupus.
Schett et al. report that three out of the eight patients received tocilizumab for cytokine release syndrome (CRS). Various case reports and a small pilot study have reported on the efficacy of tocilizumab in patients with lupus. 7 It is unclear if interleukin-6 blockade contributed to the improvement of these patients. A comparative trial with tocilizumab would be problematic considering the weak data supporting its use in lupus.
Efficacy and safety in diverse (ethnically, clinically and serologically) populations needs to be confirmed by other centres. Long term follow-up [>5 years] is required to establish if CAR-T therapy is potentially curative for all, or a subset of patients.
In a large population-based study in SLE, five and 8- year survival was reported as 91% and 89% respectively. 8 In a previous a meta-analysis infections were the first cause of death. 9 More recently cardiovascular disease has been reported as the most common cause of death. Both are associated with disease activity, immune dysregulation, organ damage and immunosuppressive treatment. 10 Antiphospholipid positivity is also significant CV risk factor. A recent case study describes the sustained disappearance of these antibodies after treatment with CAR-T. 11 It is therefore reasonable to predict that CAR-T would make a significant impact on SLE associated mortality by reducing disease activity’ preventing organ damage, treating immune dysregulation (including eliminating pathological antibodies), and preventing use of immunosuppressive treatment. Thus far there have been no reports of death in patients with SLE treated with CAR-T.
In patients with acute B-cell lymphoblastic leukaemia (B-ALL) treated with CAR-T, race and ethnicity have no impact on treatment response regarding overall survival or neurotoxicity. 12 This contrasts with responses in patients with myeloma. Hispanics have been shown to have lower best overall response rates and non-Hispanics, particularly black patients were found to be more likely to develop CRS. Nonetheless, there was no difference in overall survival. 13 These associations have yet to be examined in autoimmune diseases and CAR-T therapy.
Prevalence of the most common adverse effects reported in haematology oncology literature are; persistent B-cell depletion/hypogammaglobulinemia (25–74%), late severe cytopenia (3%–17%) and infections (9–80%). 14
In the lupus cohort treated with CAR-T there was one serious infection reported requiring inpatient treatment. 5
Who should receive CAR-T therapy?
Currently only young patients with severe treatment resistant lupus have received CAR-T therapy. Once more is known regarding efficacy and safety it may also be appropriate for those with moderate disease. CAR-T therapy offers long term remission after one treatment, it could be considered as a solution for patients with poor compliance. Non-adherence in lupus is a significant, often under-diagnosed issue. Measurements of hydroxychloroquine levels have demonstrated non-adherence in approximately 10%. 15 However, other studies have reported up to 76% non-adherence. 16 Compliance could be resolved by one observed infusion of CAR-T. However, it may be unethical, or at the very least, unjust to provide potentially curative treatment preferentially to those with poor compliance as opposed to patients actively and reliably engaged in the management of their disease.
Examples of the cost of lupus treatment per annum in the UK according to the British national formulary 2024. 17
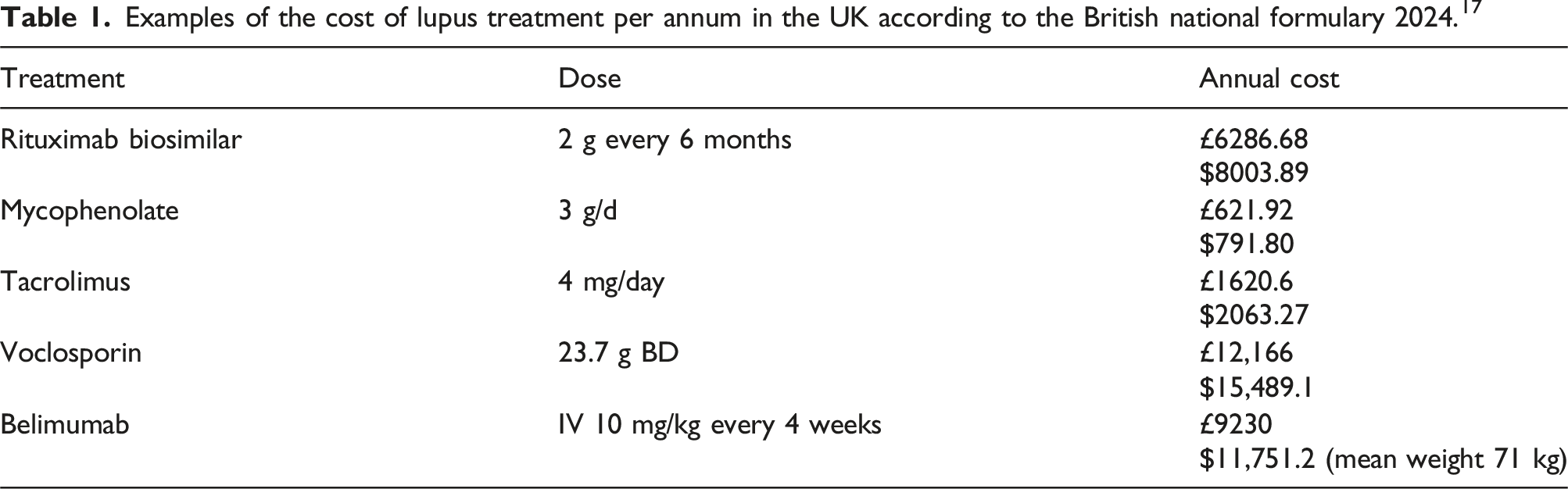
A retrospective study examining costs associated with lupus patients from 2005 to 2017 found unadjusted mean costs in the year of diagnosis were £14, 125 ($17,564), £8323 ($10,349) and £5221 ($6492), for severe, moderate and mild SLE, respectively. Ten years after diagnosis the annual cost for patients with severe lupus had increased to £26,916 ($33,469) in 2017. 19 In 2024 that equates to £34,642 ($43,074). In the USA it has been reported that the annual cost 1-year post diagnosis of severe lupus is £54,897 ($68,260). 20 Although CAR-T therapy is expensive, over a long period the differential compared to standard immunologic/ biologic treatment becomes much less daunting, perhaps even comparable after 10 years.
There are currently six FDA approved CAR-T products. Four of them target CD-19; Axiczbtagene ciloleucel is indicated for refractory (r) and relapsed (R) large B-Cell lymphoma (LBCL) and R follicular lymphoma (FL). Brexucabtagene autoleucel is indicated for r/R B-ALL, r/R mantle cell lymphoma (MCL). Both products contain a CD-28 costimulatory domain
Tisagenlecleucel is indicated for r LBCL, r FL and r/R B-ALL, Lisocabtagene maraleucel is indicated for r/R LBCL both containing a 41-BB costimulatory domain. Two products Idecabtagene vicleucel and Ciltacbtagene autoleucel target B-cell maturation antigen and are indicated for r/R multiple myeloma. 14 In the report from Schett and his colleagues they used an investigational autologous CD-19 CAR–transduced CD4- and CD8-enriched T cells, MB-CART19.1.
Future directions
Next steps.
The trial by Schett et al. needs replication to validate the data, supporting further trials. Controlled randomised trials comparing best current care to CAR-T for diverse populations with severe lupus are necessary.
Cost reduction is also crucial. CAR-T is now being manufactured in India at 10% of the USA price. 21 Current inpatient admissions from real world data range from a median of 12–21 days. 22 CAR-T is delivered in specialist centres that have the facilities, expertise and appropriate accreditation. Currently there are 17 centres in the UK accredited by JACIE (Joint Accreditation Committee ISCT-Europe and EBMT). Ensuring appropriate standards for stem cell transplantation and cellular therapy. 23 These centres can now be utilised for rheumatology patients in addition to the haematology patients. Outpatient CAR-T therapy is being explored. A recent systematic review found no significant difference in safety, efficacy and quality of life between outpatient and inpatient administration of CAR-T. 24
Timing of CAR-T therapy is another important consideration. Could treatment be considered at diagnosis? Until now it has only been used after multi-treatment failure. Early intervention is increasingly recognised as the best strategy to prevent irreversible organ damage. 25 Treatment with CAR-T close to diagnosis could potentially have a huge impact on prognosis and long-term morbidity. It also may reduce the risk of comorbidities such as cardiovascular disease, osteoporosis and infection.
The recent development of CAR -T therapy is an exciting advancement for SLE treatment. Existing data are very limited but offer great encouragement that SLE might one day be cured. Much work needs to be done to ensure this hope may be realised.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.