
Abstract

Dear Editor,
A perceived lack of informational support from healthcare providers can impact quality of life in patients with lupus nephritis (LN). 1 While the accessibility of online information has increased, 2 it can generate mis/disinformation which may provoke anxiety 3 and alter decision-making.4,5 To increase understanding of how clinicians/advocacy organizations can better support patients with LN, we surveyed LN patients on how they access and trust health information sources.
Patients ≥18 years with biopsy-proven ISN/RPS Class II, III, IV, V or mixed Class III/V or IV/V LN 6 were recruited (n = 62, 53.4% response rate) from a Canadian cohort between 11/2022-07/2023. Respondents completed an online survey 4 regarding how frequently they accessed health information sources for LN information and their level of trust in each source at LN diagnosis and currently. Respondents self-reported if they had experienced obstacles in accessing information. The percentages accessing and trusting each source at the time of LN diagnosis and currently were compared using McNemar tests.
Mean (SD) age was 46.1 (14.5) years, mean (SD) LN duration was 15.0 (11.8) years, 87.1% were female, and 56.5% reported non-White race/ethnicity. Most received hydroxychloroquine (88.7%) and/or immunosuppressants/biologics (67.7%) in the past year. Most had Class III (11.3%), IV (46.8%), V (11.3%) or mixed (21.0%) LN; 8.1% had dialysis, and 6.5% had a renal transplant.
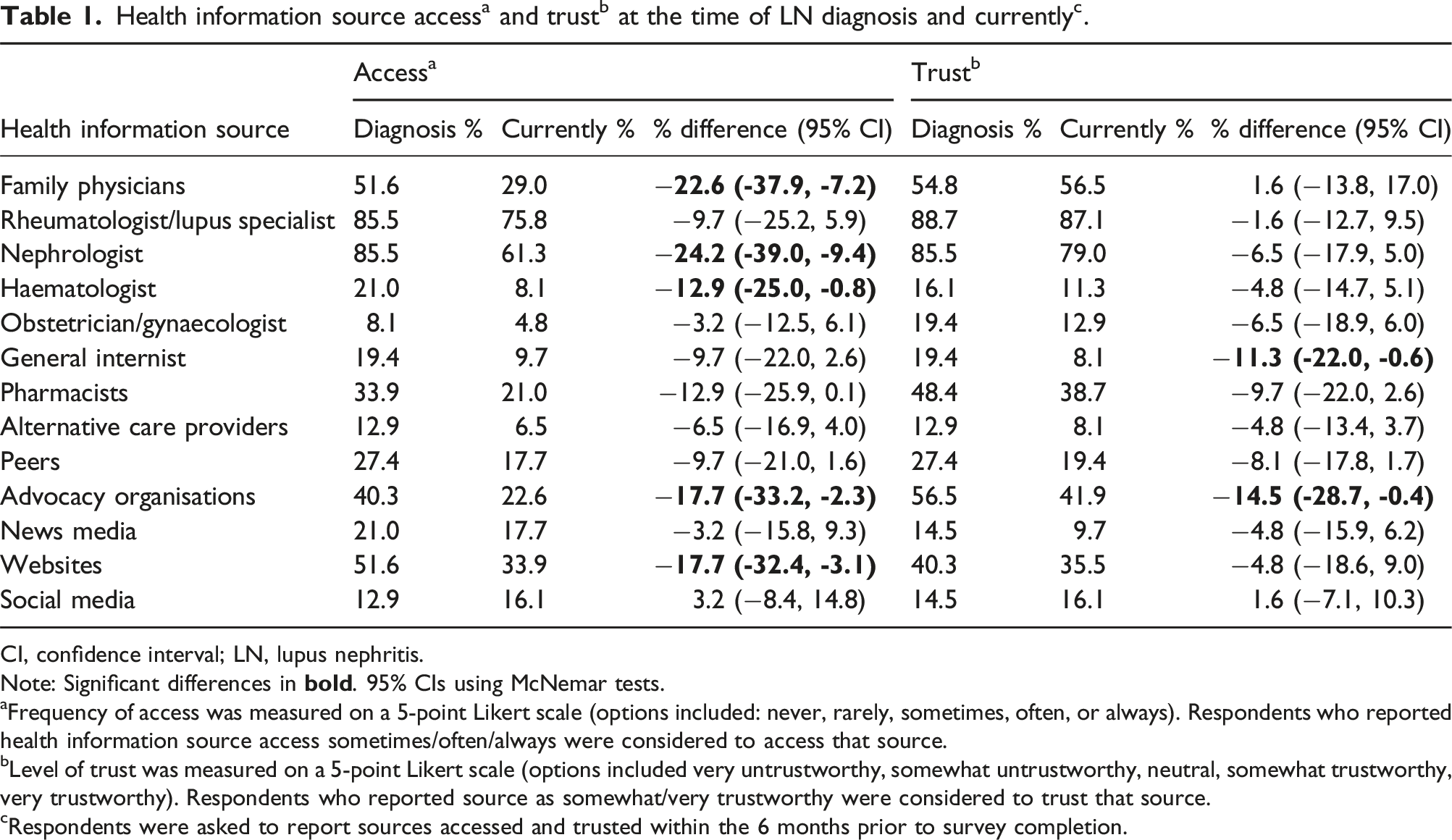
CI, confidence interval; LN, lupus nephritis.
Note: Significant differences in
aFrequency of access was measured on a 5-point Likert scale (options included: never, rarely, sometimes, often, or always). Respondents who reported health information source access sometimes/often/always were considered to access that source.
bLevel of trust was measured on a 5-point Likert scale (options included very untrustworthy, somewhat untrustworthy, neutral, somewhat trustworthy, very trustworthy). Respondents who reported source as somewhat/very trustworthy were considered to trust that source.
cRespondents were asked to report sources accessed and trusted within the 6 months prior to survey completion.
Most respondents (66.1%) identified no obstacles in accessing information, though challenges communicating with healthcare providers (24.2%), financial (8.1%), language (3.2%) and technology barriers (1.6%) were identified.
Trust was highest amongst rheumatologists/lupus specialists and nephrologists, highlighting the standard of care this sample receives and the role of these physicians in providing trusted information. 7 The observed decrease in access to many sources after diagnosis is likely related to a reduced need for information.
Access to and trust in advocacy organisations decreased after LN diagnosis; it is unclear why trust decreased, though this is consistent with previous work documenting a decrease in access/trust in advocacy organisations during COVID-19. 4
Our study was limited as we recruited a small sample from a single lupus specialist clinic; hence, results may not reflect the general LN population. While our sample represented several racial/ethnic backgrounds (40.3% Asian/South Asian/East Asian, 3.2% Black, 1.6% Indigenous, 3.2% Latin/Hispanic, 6.5% Middle Eastern, 1.6% Mixed, 43.5% White), only 3.2% reported language barriers to accessing information. Next steps include surveying a larger sample; a sample with more diverse sociodemographics may also report additional obstacles.
Findings demonstrate that rheumatologists/lupus specialists and nephrologists are the most accessed and trusted sources by patients with LN, highlighting the importance of this therapeutic alliance. Despite being more trusted, advocacy organisations were less accessed than other sources (e.g., websites), and access and trust in advocacy organisations decreased with disease duration. Understanding how patients with LN access and trust health information will inform targeted delivery of accessible information to help optimise patient experiences.
Footnotes
Author contributions
FSC, SJE, SG, AB and AEC contributed to the conception or design of the study. FSC, MRWB, KC, SJE and AEC contributed to the acquisition of data. All authors contributed to data analysis and/or interpretation. FC is responsible for the overall content of this work and accepts full responsibility for the work as guarantor, had access to the data and controlled the decision to publish.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FSC and SJE have no conflicts of interest to disclose, FSC and SJE have no conflicts of interest to disclose. MRWB has received consulting fees from AbbVie, AstraZeneca, Janssen, GSK and Sanofi-Genzyme. KC has received consulting fees from Novartis and speaker fees from Alexion. AB is an employee of GSK, SG former employee of GSK. AB also holds stock/shares in GSK. AEC has received grant/research support from GSK, and consulting fees/honoraria from AstraZeneca, Bristol Myers Squibb, GSK, Otsuka and Roche.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by GSK (GSK Study 218747). AEC holds The Arthritis Society Chair in Rheumatic Diseases at the University of Calgary.