
Abstract
Background
Patients with cutaneous lupus erythematosus (CLE) can present with one or multiple different subtypes of CLE. There is limited understanding of the prevalence and associated risk factors for having multiple CLE subtype diagnoses.
Objective
This study characterized the frequency and risk factors for having multiple CLE subtypes.
Methods
This was a cross-sectional study of 319 patients with CLE enrolled in the University of Texas Southwestern Cutaneous Lupus Registry seen in outpatient dermatology clinics at the University of Texas Southwestern Medical Center and Parkland Health from January 1, 2009 to December 31, 2021. Demographic and clinical information was collected from each subject and compared using univariate and multivariable logistic regression analyses.
Results
59 subjects (18.5%) were diagnosed with two or more CLE subtypes. Univariate analyses identified statistically significant differences in rates of systemic lupus erythematosus (SLE) diagnosis, history of positive anti-nuclear antibody, arthritis, renal disorder, and serositis in patients with multiple CLE subtype diagnoses. In the multivariable analysis, SLE diagnosis was found to be statistically significant.
Conclusions
Our study showed that almost one out of five CLE patients have multiple CLE subtypes, with SLE diagnosis being a significant risk factor. Clinicians can monitor CLE patients for developing multiple subtypes and account for systemic manifestations and laboratory abnormalities associated with SLE.
Introduction
Cutaneous lupus erythematosus (CLE) is an autoimmune skin disease that can present with or without systemic lupus erythematosus (SLE). 1 The onset of disease typically occurs during reproductive years, between 20 and 50 years. 2 Population studies based in the US and Europe have reported a prevalence of 70 per 100,000, with a greater prevalence in women.2,3 CLE can be further classified into acute, subacute, or chronic CLE subtypes. 4 Acute CLE (ACLE) typically presents with a bilateral malar erythema and has a strong association with SLE. Subacute CLE (SCLE) manifests as annular or papulosquamous skin lesions and can be drug-induced. Chronic CLE (CCLE) has the greatest number of subtypes, with discoid lupus erythematosus (DLE) as the most common form. 1
Prior studies of CLE patient cohorts and existing clinical trials for CLE therapies have treated subtypes of CLE as distinct entities. 5 Among prior literature that has examined the prevalence of having multiple CLE subtypes, the patient populations have predominantly been based in Europe and Asia, with limited available demographic or clinical data for this subpopulation.6–9 Likewise, current CLE treatment guidelines do not differentiate between subtypes, since the existing medication regimens for CLE have primarily been adapted from SLE therapy. 10 Currently, only hydroxychloroquine and glucocorticoids have been specifically approved by the U.S. Food and Drug Administration (FDA) for the treatment of CLE.5,10 Having a better understanding of the prevalence and risk factors of having multiple CLE subtypes may eventually improve therapeutic approaches and management in patients with complex CLE presentations, as first-line treatments for CLE such as anti-malarials have been shown to have varying cutaneous response rates in different CLE subtypes. 11 Consequently, we conducted a cross-sectional study of CLE patients to assess the prevalence and risk factors of having multiple CLE subtypes. We hypothesize that a minority of CLE patients will present with multiple subtypes, with the presence of systemic lupus erythematosus (SLE) being a significant risk factor. The findings of this study will aid clinicians in monitoring for the development of multiple CLE subtypes and its associated risk factors.
Methods
Participants
This was a cross-sectional study of CLE patients seen at Parkland Health and University of Texas Southwestern (UTSW) Medical Center outpatient dermatology clinics between January 1, 2009 to December 31, 2021. For patients with multiple visits, the most recent clinic visit prior to December 31, 2021 was used for data analysis. Patients were required to meet CLE diagnosis via clinicopathological correlation. Patient records and photographs were reviewed to confirm the presence of specific CLE subtypes according to the Gilliam classification scheme. 4 Exclusion criteria included patients below 18 years of age, visits outside of the time frame of interest, absence of CLE diagnosis, and unknown CLE subtype (Supplemental Figure 1). Pediatric CLE patients were excluded due to differences in clinical presentations and progression to SLE as demonstrated in prior literature, as well as limitations in obtaining informed consent from minors. 12 Clinical data for each patient was collected by medical chart review. All patients gave informed consent, which was approved by the UTSW Institutional Review Board.
Demographic and clinical variables
The primary outcome variable was the presence or absence of two or more CLE subtype diagnoses. The predictor variables encompassed both demographic and clinical characteristics. Demographic characteristics included race, ethnicity, age, and sex. Clinical characteristics included SLE diagnosis, smoking history, CLE disease duration, history of positive auto-antibodies, medication status, and age of CLE diagnosis. SLE diagnosis was defined according to the presence of four or more American College of Rheumatology (ACR) criteria for SLE.
13
Patients with both malar and discoid rash, corresponding to ACLE and DLE, were reported as meeting only one ACR criteria instead of two, in order to address their greater potential for meeting SLE diagnosis. Auto-antibodies that were considered in this study include anti-nuclear antibody (ANA), anti-double-stranded DNA (anti-dsDNA), anti-SS-A, anti-SS-B, anti-Sm, and anti-RNP antibodies. Patients were classified into three medication categories, including: 1) no medications or topical medications only, 2) anti-malarials
Statistical analyses
Patient characteristics were recorded as frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Univariate and multivariable logistic regression analyses were performed to identify significant predictor variables associated with multiple CLE subtypes. For univariate analyses, we used Mann-Whitney U test for continuous variables and Chi-squared or Fisher’s exact tests for categorical variables. Two-sided p values <0.05 were considered significant. Predictors in the logistic regression model included variables significant at p < 0.05 from the univariate analyses and variables declared a priori (e.g. SLE diagnosis). Each variable was added to the model in stepwise selection according to these criteria. Predictor variables with a large proportion of missing values and medication status due to collinearity with SLE diagnosis were excluded from multivariable analysis. All statistical analyses were performed using MATLAB version 2022b and SPSS version 25.
Results
Univariate analysis of demographic and clinical characteristics of patients with and without multiple CLE subtypes.
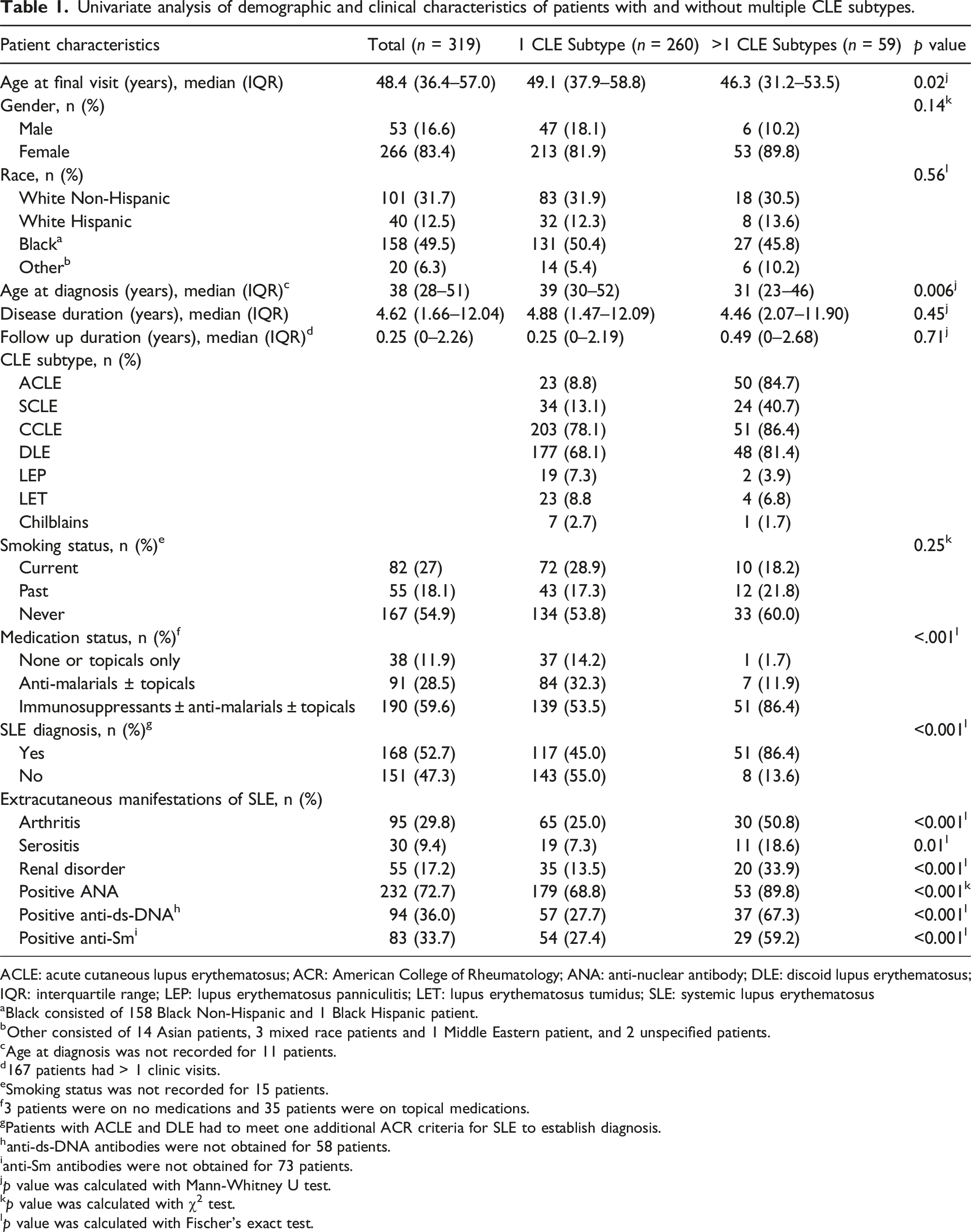
ACLE: acute cutaneous lupus erythematosus; ACR: American College of Rheumatology; ANA: anti-nuclear antibody; DLE: discoid lupus erythematosus; IQR: interquartile range; LEP: lupus erythematosus panniculitis; LET: lupus erythematosus tumidus; SLE: systemic lupus erythematosus
aBlack consisted of 158 Black Non-Hispanic and 1 Black Hispanic patient.
bOther consisted of 14 Asian patients, 3 mixed race patients and 1 Middle Eastern patient, and 2 unspecified patients.
cAge at diagnosis was not recorded for 11 patients.
d167 patients had > 1 clinic visits.
eSmoking status was not recorded for 15 patients.
f3 patients were on no medications and 35 patients were on topical medications.
gPatients with ACLE and DLE had to meet one additional ACR criteria for SLE to establish diagnosis.
hanti-ds-DNA antibodies were not obtained for 58 patients.
ianti-Sm antibodies were not obtained for 73 patients.
jp value was calculated with Mann-Whitney U test.
kp value was calculated with χ2 test.
lp value was calculated with Fischer’s exact test.
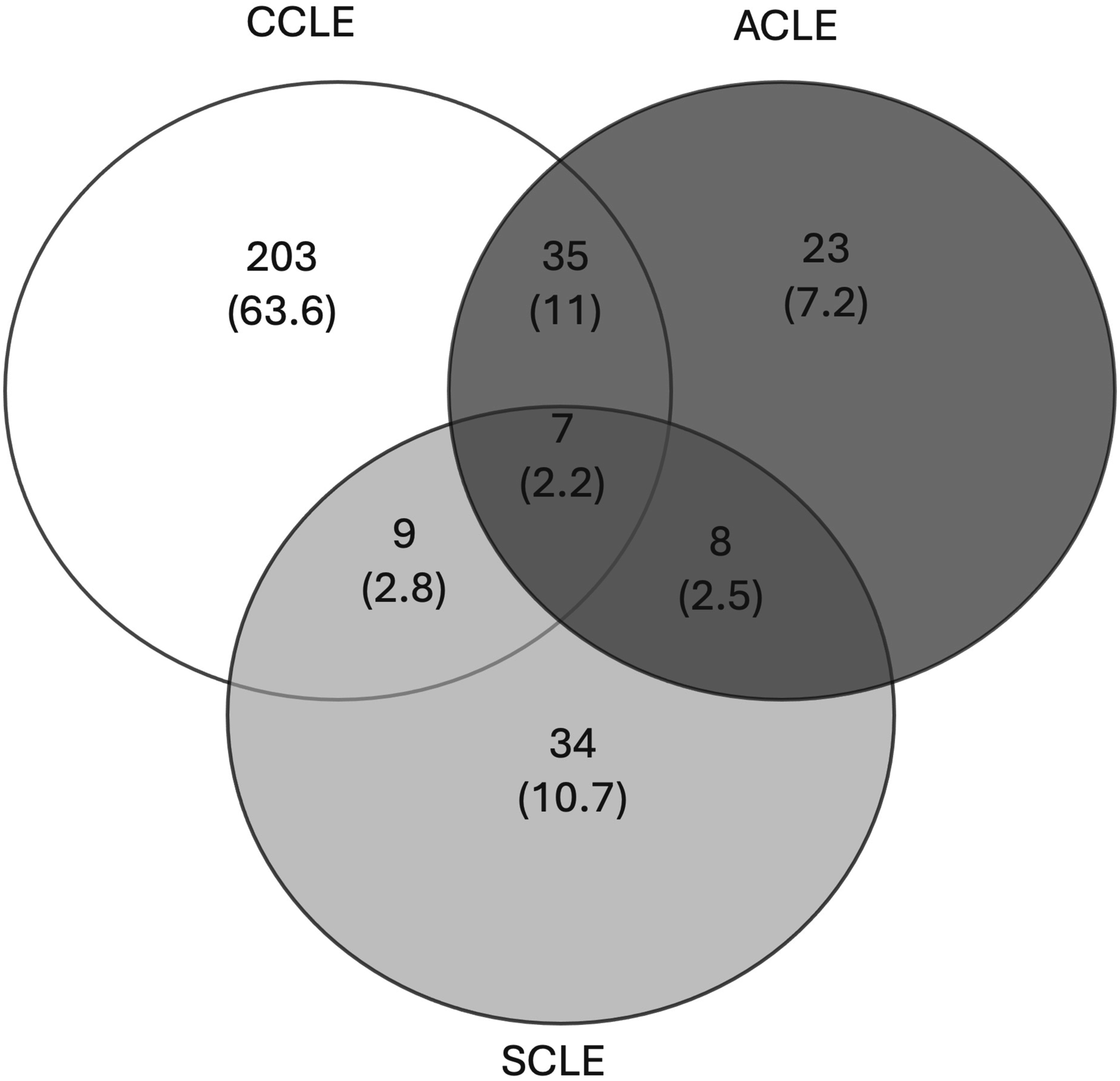
CLE subtype distribution. The Venn diagram depicts the number and percentage (noted in parenthesis) of patients with one and multiple CLE subtypes (n = 319). Abbreviations: ACLE: Acute Cutaneous Lupus Erythematosus; CCLE: Chronic Cutaneous Lupus Erythematosus; SCLE: Subacute Cutaneous Lupus Erythematosus.
Univariate analysis
Univariate analyses were performed to identify risk factors associated with multiple CLE subtype diagnoses. Clinical risk factors associated with an increased likelihood of having multiple CLE subtypes included age at diagnosis, SLE diagnosis, medication status, history of positive auto-antibodies, and all ACR criteria excluding discoid rash (Table 1). Patients with multiple CLE subtypes (median age: 31 years, IQR: 23-46) were diagnosed at a younger age compared to patients with one CLE subtype (median age: 39 years, IQR: 30-52, p = .006). They were also more likely to be diagnosed with SLE (86.4% vs 45%, p < .001) and manifest various ACR criteria for SLE diagnosis, including arthritis (50.8% vs 25%, p < .001), renal disorder (33.9% vs 13.5%, p < .001), and serositis (18.6% vs 7.31%, p = .01). Likewise, they were also more likely to have a history of auto-antibodies, including ANA (89.8% vs 68.8%, p < .001), anti-ds-DNA (67.3% vs 27.7%, p < .001), and anti-Sm (59.2% vs 27.4%, p < .001). Lastly, patients with multiple CLE subtypes were more likely to be treated with combination therapy involving immunosuppressants, anti-malarials, and/or topicals (86.4% vs 53.5%, p < .001) (Table 1).
Multivariable analysis
Multivariable analysis of patient factors associated with multiple CLE subtypes.
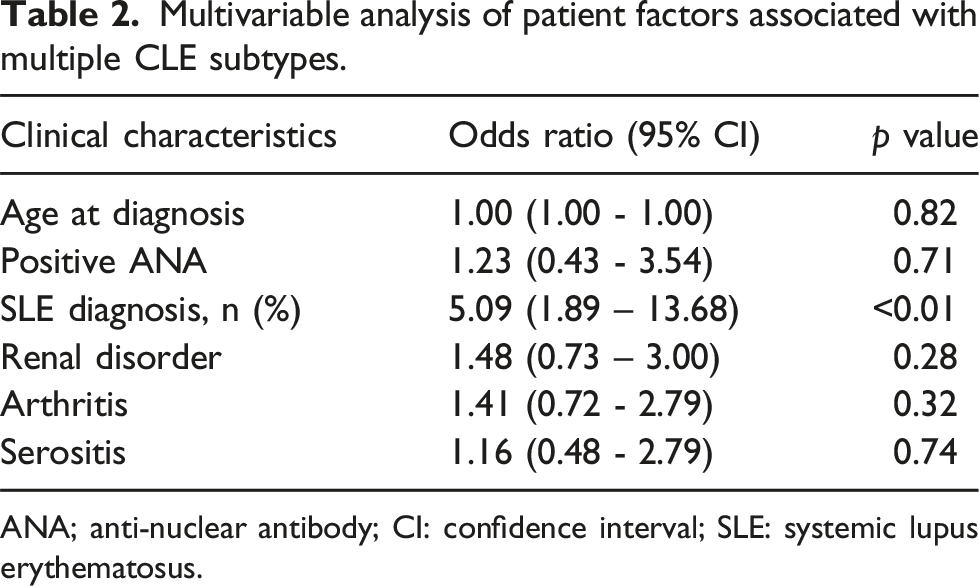
ANA; anti-nuclear antibody; CI: confidence interval; SLE: systemic lupus erythematosus.
Discussion
In this cross-sectional study of 319 CLE patients, we found that multiple CLE subtype diagnoses occurred in 18.5% of patients, with SLE diagnosis being a significant risk factor. The prevalence of having multiple CLE subtype diagnoses was found to be lower in our patient population compared to prior cohort studies based in Asia and Europe, which ranged from 22 to 35%.6–9 These differences may be due to variations in both sample sizes and clinical characteristics of the CLE patient groups, as many of these studies included patient cohorts comprised of over 1000 individuals and had higher proportions of patients diagnosed with ACLE. In contrast to previous literature, we also found that SLE diagnosis was a significant risk factor for having multiple CLE subtypes. Though some studies did demonstrate a higher prevalence of having multiple CLE subtype diagnoses in CLE patients with systemic disease, this was not found to be statistically significant.7,9 However, the studies that demonstrated these findings had differing groups of comparison, examining patients with isolated CLE versus CLE with laboratory SLE, as well as patients with isolated CLE, isolated SLE, or CLE with SLE.7,9
Although the presence of systemic symptoms and a history of positive auto-antibodies were considered statistically significant in the univariate analysis, these risk factors are accounted for in the ACR criteria for SLE diagnosis, which likely explains why these variables were ultimately not significant in the multivariable logistic regression analysis. CLE subtype diagnoses are also included in the criteria for SLE diagnosis, though this factor was adjusted by considering the presence of malar and discoid rash as meeting one ACR criteria for SLE.
Given that a sizeable proportion of CLE patients have been diagnosed with two or more subtypes, these results affirm the importance of considering complex CLE presentations in population-based studies, as well as clinical trials. it would be valuable for clinicians to monitor for the development of multiple CLE subtypes and account for potential associated risk factors, such as SLE diagnosis. Assessing patients for systemic symptoms and laboratory abnormalities (such as auto-antibodies) may be useful tools in the surveillance of developing multiple CLE subtypes. With regards to disease management, patients with multiple CLE subtypes may require multimodal treatment involving a combination of topicals, anti-malarials, and/or immunosuppressants, given its association with SLE diagnosis.
Limitations of this study include the single-center nature, which limits generalizability. The frequency of ACLE also may have been underestimated, as ACLE diagnosis was confirmed primarily through careful history taking and often not clinically observed, given the transient nature of the disease. We were also unable to follow the temporal progression of developing multiple CLE subtypes, as the majority (93.2%) of patients with multiple CLE subtypes had already been diagnosed at initial presentation. Though alternative classification criteria for SLE diagnosis have been proposed by the Systemic Lupus International Collaborating Clinics and European League Against Rheumatism/American College of Rheumatology in recent years, the 1982 ACR criteria was selected for our study to account for consistency in SLE diagnostic criteria throughout the length of follow-up, which preceded the advent of these new criteria.14,15
This single-center cross-sectional study found that nearly 1 in 5 patients with CLE have multiple subtype diagnoses, with SLE being a significant risk factor. Future directions include prospective studies that examine the temporal progression of multiple CLE subtypes and its associated risk factors, since the majority of patients in the UTSW Cutaneous Lupus Registry were already diagnosed with multiple subtypes at initial presentation. We also plan to examine whether having multiple subtypes affects patient outcomes, such as treatment response, quality of life, and other domains.
Supplemental Material
Supplemental Material - Systemic lupus erythematosus is a risk factor for having multiple subtypes of cutaneous lupus erythematosus
Supplemental Material for Systemic lupus erythematosus is a risk factor for having multiple subtypes of cutaneous lupus erythematosus by Grace Lu, L Steven Brown and Benjamin F Chong in Lupus
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Chong is an investigator for Biogen Incorporated. He is a consultant for Bristol Meyers Squibb, EMD Serono, Biogen Incorporated, Amgen Incorporated, and Lupus Research Alliance. He also receives royalties from MAPI Research Trust and served as a chairperson for a seminar sponsored by Amgen Incorporated and a speaker for Cesas Medical. The other authors have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number K23AR061441 (BFC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the University of Texas Southwestern Medical Center at Dallas, its affiliated academic and health care centers, and the National Institutes of Health.
IRB status
Reviewed and approved by University of Texas Southwestern IRB.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.