
Abstract
Objective
Substantial morbidity and mortality affect those with antiphospholipid antibodies (aPLs) and antiphospholipid syndrome (APS), yet patient experiences remain poorly understood. This research investigated patient experiences of aPL/APS diagnosis; effects on daily life; and healthcare and treatment.
Methods
Patients aged ≥18 years with APS per the Revised Sapporo criteria or with ≥1 positive aPL on ≥2 occasions were recruited from a Canadian multidisciplinary APS clinic to participate in semi-structured in-depth interviews. Interviews were conducted virtually and transcribed verbatim for subsequent thematic analysis.
Results
Twenty-one patients with aPLs/APS participated; 95.2% were female, mean (SD) age was 45.6 (15.0) years. Most (71.4%) had APS, and 71.4% had aPLs/APS with SLE. Results are presented around patient experiences of aPL/APS diagnosis, effects on daily life, and healthcare and treatment. Participants described medical complications/physical symptoms and the healthcare, lifestyle, and emotional impacts experienced around the time of aPLs/APS diagnosis. In addition to the physical and psychosocial impacts of living with aPLs/APS, patients reported modified leisure activities, altered employment trajectories, and positive and negative impacts on relationships. Impacts on family planning were also a critical component of the aPL/APS lived experience; participants shared experiences of miscarriage, other pregnancy complications, and medication-related challenges (e.g., with low-molecular-weight heparin injections). Challenging aspects of aPL/APS healthcare and treatment were also discussed, particularly related to the lifestyle, physical, and emotional burden of medication use. Although a lack of resources was described, participants expressed trust in healthcare providers when making management decisions or when seeking information. Suggestions for resources included the need for additional medication-related information, examples to help contextualize management behaviours, and additional information for those with aPLs/APS without SLE.
Conclusion
Patients highlighted how the diverse manifestations of aPLs/APS, accentuated by management-related challenges, impose considerable physical and psychosocial burdens. Results will inform the development of patient resources aligned with patient priorities.
Introduction
Antiphospholipid syndrome (APS) is an autoimmune condition defined by thrombosis or pregnancy morbidity and the presence of persistently positive antiphospholipid antibodies (aPLs).1,2 APS can develop in patients with no underlying systemic autoimmune condition or in those with overarching autoimmune conditions, primarily systemic lupus erythematosus (SLE). Approximately 40% of SLE patients have aPLs 3 ; of these, up to 50%–70% may develop APS after 20 years of follow-up.3,4 SLE patients with APS have a worse prognosis 5 than those without APS. 3
Individuals with aPLs are at risk of developing thrombotic events 4 and pregnancy complications and loss. 6 Patients with thrombotic APS can experience arterial, venous, or small vessel thrombosis presenting most commonly as stroke, myocardial infarction, pulmonary embolism, or deep vein thrombosis. 4 After a first unprovoked event, the annual recurrence rate without anticoagulation is 19%-29%,4,7 so indefinite anticoagulation (e.g., with warfarin) is often recommended.8,9 Those with obstetrical complications can experience recurrent early or late pregnancy losses, placenta-mediated pregnancy complications including early/severe pre-eclampsia, fetal growth restriction, and preterm delivery.6,10 Even with standard of care treatment (low-molecular-weight heparin (LMWH) and/or acetylsalicylic acid (ASA)), a high rate of pregnancy loss and obstetrical complications remain.10–14 Despite limited evidence supporting LMWH/ASA,15–20 previous qualitative research demonstrated that women often prefer taking action by self-injecting LMWH throughout pregnancy even in the absence of a guaranteed good outcome. 21
The diverse manifestations of aPLs/APS can considerably impact patients, but patient experiences of aPLs/APS remain poorly understood. Quantitative studies22–26 have reported quality of life impacts in APS patients; one study assessed the psychosocial burden of APS, but the sample size was small. 27 While existing qualitative studies report experiences of fetal loss,28,29 how patients and physicians navigate the LMWH and/or ASA decision-making process in pregnancy, 21 patient perceptions of APS care, 30 and fatigue, 31 the broad lifecosts (i.e., totality of social, economic, physical, emotional and wellbeing impacts 32 ) of living with aPLs/APS have not been documented. This study used a social constructionist approach to investigate patient lived experiences of aPL/APS (1) diagnosis; (2) effects on daily life; and (3) healthcare and treatment.
Methods
Patients aged ≥18 years with APS per the Revised Sapporo criteria for APS 1 or ≥1 positive aPL (medium to high positive anticardiolipin and/or medium to high positive anti-beta2-glycoprotein 1 and/or positive lupus anticoagulant) on ≥2 occasions were purposefully recruited from a Canadian multidisciplinary SLE/APS clinic (care provided by a rheumatologist, immunologist, and hematologist) to participate in semi-structured in-depth interviews. Participants were identified by the clinical team and approached in clinic or by telephone; we purposefully sampled patients with varied demographic backgrounds (e.g., age, race/ethnicity) and disease characteristics (e.g., with/without SLE per 1997 American College of Rheumatology 33 or 2012 Systemic Lupus International Collaborating Clinics 34 criteria) to ensure maximum variation of experiences. Recruitment continued until thematic saturation was reached.
Prior to recruitment, this study received ethics approvals from a Research Ethics Committee at the University of Waterloo, and the Conjoint Health Research Ethics Board at the University of Calgary. Semi-structured in-depth interviews were conducted virtually from March-July 2023 and lasted an average of 45 min. All interviews were conducted by the first author (female), an experienced qualitative researcher with 15+ years of experience. Participants were told the interviewer’s name, affiliation, and purpose of the research prior to the interview. Interviews were audio recorded with consent, and transcribed verbatim for subsequent thematic analysis using NVivo software independently by the first and second authors.
The interview guide (available upon request) was informed by our previous research on patient experiences of SLE, lupus nephritis (LN), and pregnancy and APS,21,32,35 and was designed to explore experiences of diagnosis, daily life, healthcare and treatment, and aPLs/APS resources/supports. Themes and sub-themes emerged from the data deductively (i.e., based on research objectives) and inductively (i.e., derived from the data). The first author developed an initial theme code set which was reviewed by the second and third authors. During proofing, the theme code set was refined by the first author and a final theme code set was used to code all transcripts using line-by-line open coding. The first and second authors discussed findings and discrepancies in coding to ensure consistency in the analysis. No participants dropped out of the study following the interviews.
A trained patient partner was involved in the research protocol design, and they reviewed the interview guide prior to the start of interviews.
Results
Participant summary
Patient characteristics.
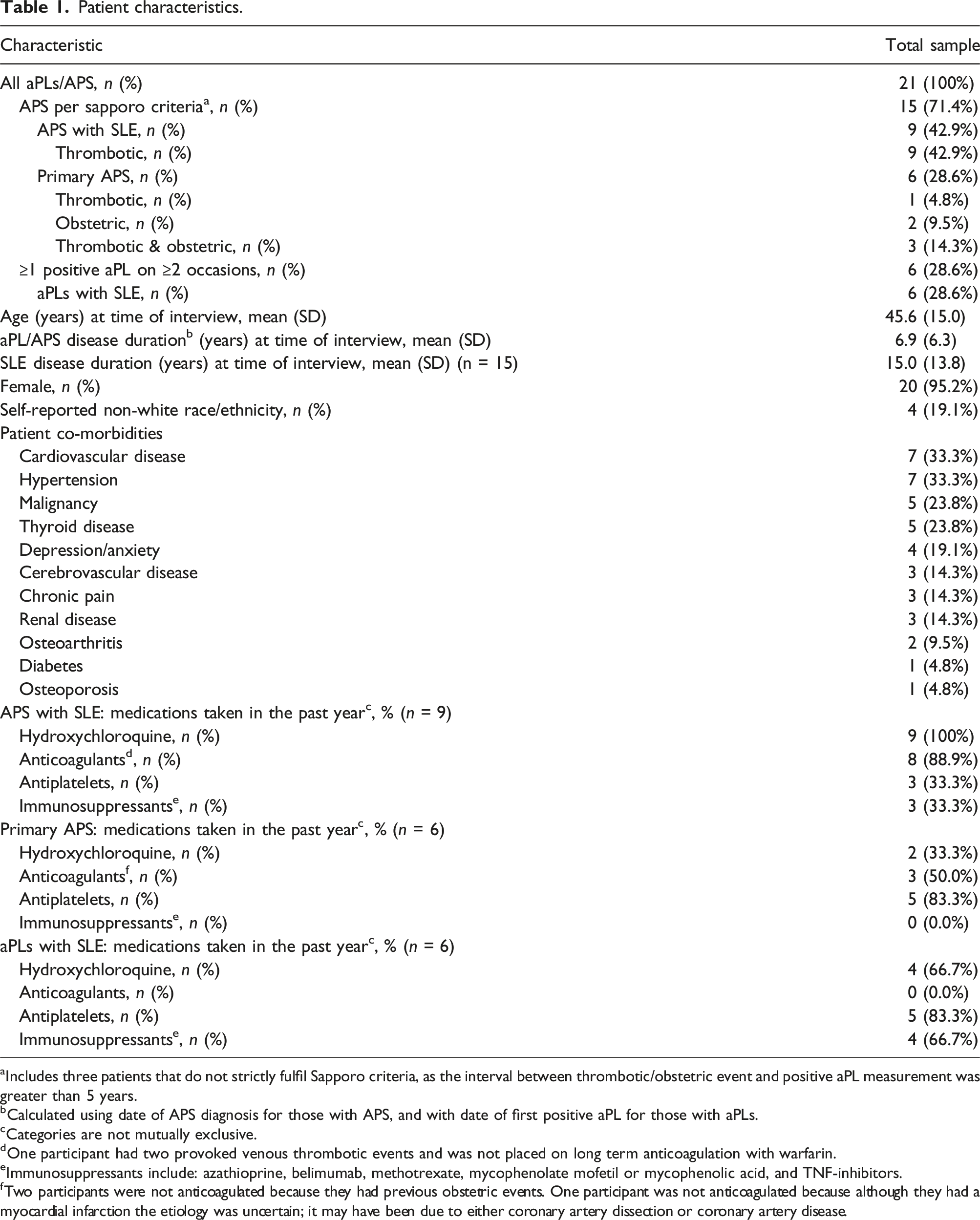
aIncludes three patients that do not strictly fulfil Sapporo criteria, as the interval between thrombotic/obstetric event and positive aPL measurement was greater than 5 years.
bCalculated using date of APS diagnosis for those with APS, and with date of first positive aPL for those with aPLs.
cCategories are not mutually exclusive.
dOne participant had two provoked venous thrombotic events and was not placed on long term anticoagulation with warfarin.
eImmunosuppressants include: azathioprine, belimumab, methotrexate, mycophenolate mofetil or mycophenolic acid, and TNF-inhibitors.
fTwo participants were not anticoagulated because they had previous obstetric events. One participant was not anticoagulated because although they had a myocardial infarction the etiology was uncertain; it may have been due to either coronary artery dissection or coronary artery disease.
Diagnosis
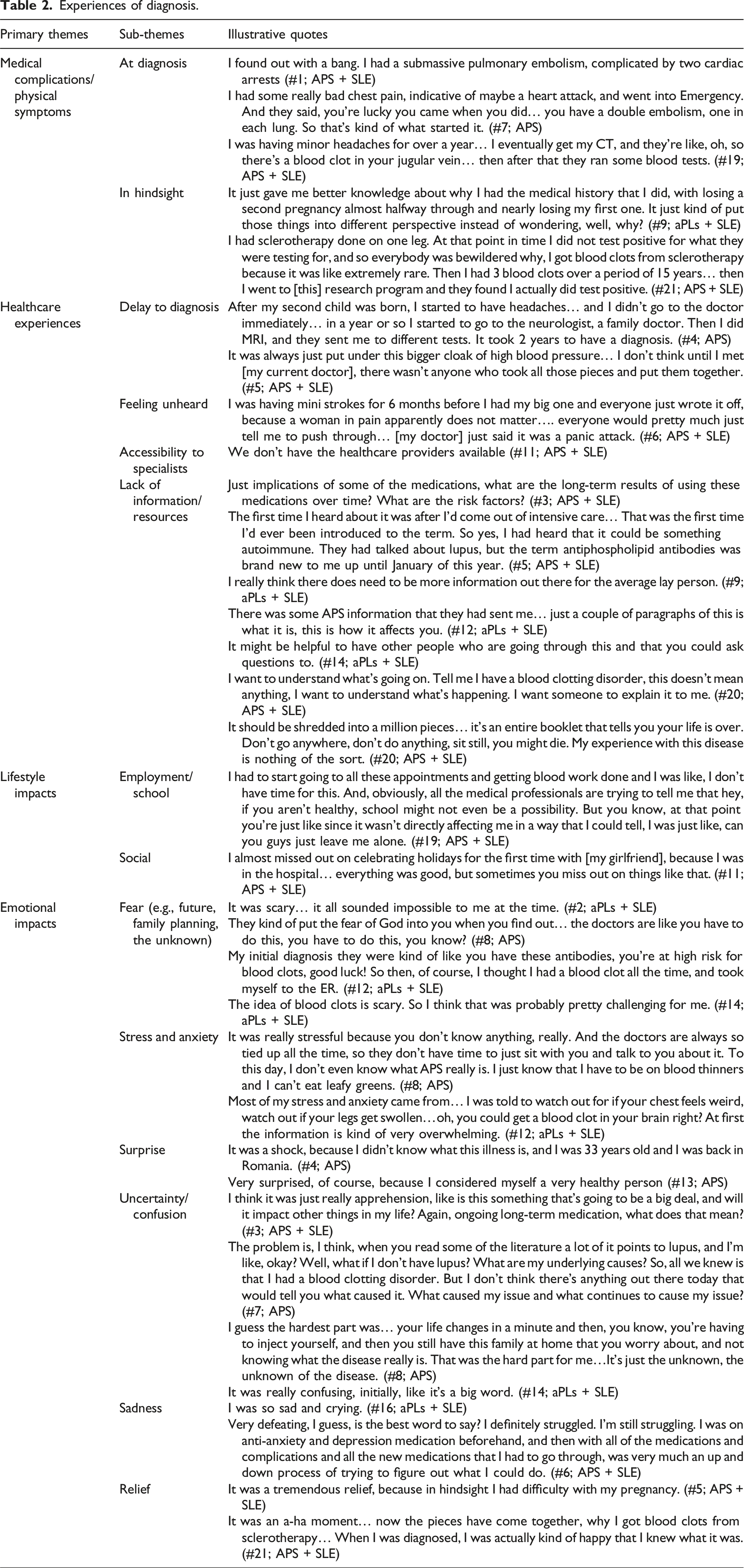
Interviews began with a discussion of aPL/APS diagnosis. The primary themes were: medical complications/physical symptoms, healthcare experiences, lifestyle impacts, and emotional impacts (Figure 1; Table 2; Supplemental Table 1). Overview of themes emerging through qualitative analysis. Experiences of diagnosis.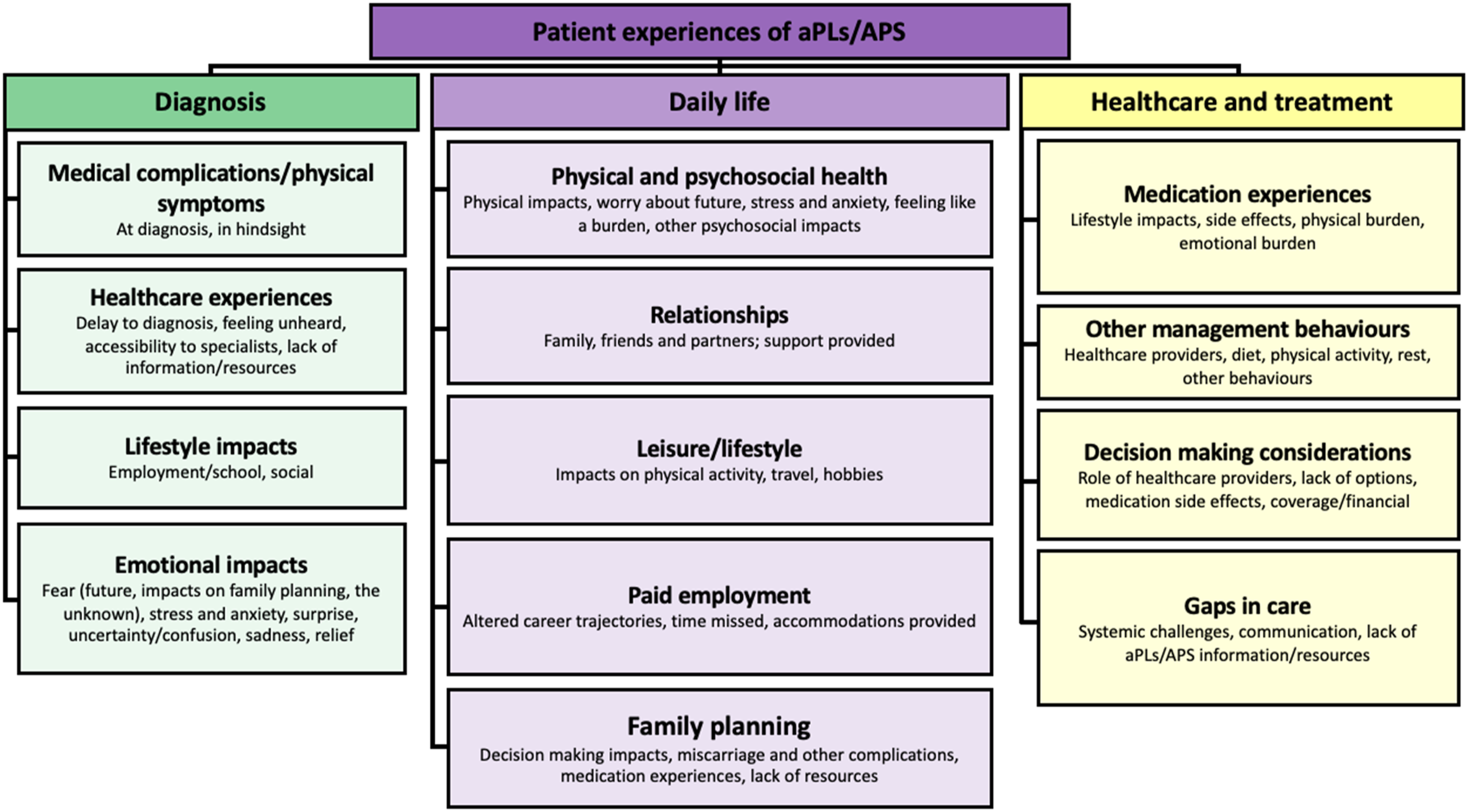
Medical complications/physical symptoms
Participants shared diverse aPL/APS diagnosis experiences. Thrombotic or obstetric complications were reported both around the time of diagnosis and before diagnosis, with detailed data provided in accompanying tables (Table 2; Supplemental Table 1). Uncertainty around how they were diagnosed also emerged (n = 5); for example, amongst those with aPLs or who received a diagnosis following bloodwork.
Healthcare experiences
Identified healthcare challenges around diagnosis included experiencing a delay to diagnosis (n = 8), feeling unheard by healthcare providers (n = 3; everyone would just tell me to push through… [My doctor] said it was a panic attack (#6; APS+SLE)), and limited accessibility to specialists (n = 3). Ten participants described their lack of aPLs/APS knowledge at diagnosis, and many (n = 10) shared that they were not provided resources to help them through diagnosis. Amongst participants that reported receiving resources, physician support (n = 7), handouts (n = 5), and websites (n = 1) were identified. When asked about suggestions for resources at diagnosis, most (n = 13) emphasized the need for additional aPL/APS information. Specifically, medication-related information (Being able to work with somebody who knows how warfarin works in relation to vitamin K (#8; APS)), information from credible sources (something that’s been approved by trained physicians (#19; APS + SLE)), examples to help contextualize management behaviours (Can I sit on the couch and watch a movie?… more situational examples… (#12; aPLs+SLE)), and information for those without SLE (A whole different resource instead of always focusing on the lupus patients (#7; APS)) were identified. Other suggestions included ensuring resources are produced in lay language, avoiding fearmongering (it’s an entire booklet that tells you your life is over. Don’t go anywhere, don’t do anything, sit still, you might die. (#20; APS+SLE)), and support groups.
Lifestyle impacts
Challenging lifestyle impacts around diagnosis were also identified (It was 1 month going to the doctor almost every day (#16; aPLs + SLE)). Specifically, challenges balancing employment/school (n = 4) and social impacts (n = 4) emerged: Having all your family members being like, ‘what’s wrong with you? It can’t be that bad.’ (#8; APS)
Emotional impacts
The emotional burden of diagnosis emerged (It’s been a traumatic experience (#7; APS)). Seven participants identified fear, particularly related to future impacts, family planning, and the unknowns surrounding aPLs/APS. Similarly, participants shared feelings of stress and anxiety (n = 6), associated with their medical complications or lack of knowledge about aPLs/APS. Although surprise (n = 5), confusion (n = 4), and sadness (n = 2) were articulated, feelings of relief were also shared (n = 5), particularly as participants identified that the diagnosis helped ‘explain some things that happened in my past (#9; aPLs + SLE): Discovering there was an underlying cause… was really quite comforting. (#5; APS + SLE)
Two participants (both with SLE) reported that they experienced no emotional impacts as the aPL/APS diagnosis ‘was never a shock’ (#11; APS + SLE).
Daily life
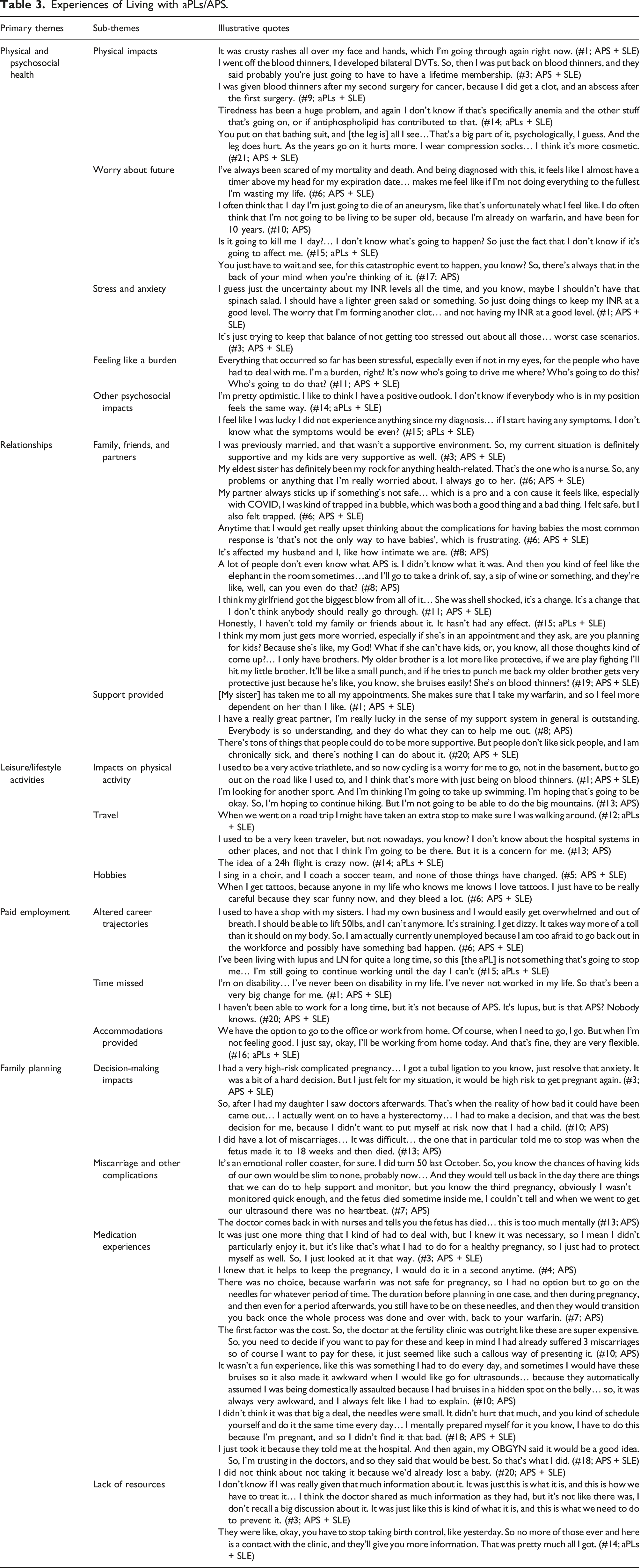
Experiences of Living with aPLs/APS.
Physical and psychosocial health
Physical symptoms that impact daily life were described (n = 12). Participants acknowledged that symptoms could result from other co-morbidities (it’s always APS vs SLE (#3; APS+SLE)); this was emphasized by a participant with APS and SLE who shared that ‘it’s really hard to tell what’s left over from my stroke. I don’t know if I would count that as the same as my APS? (#6;APS+SLE)
The most frequently mentioned psychosocial impact was worry about the future (n = 17); fear of mortality, experiencing a ‘catastrophic event’ (#17; APS), or that relatives will be impacted by aPLs/APS were articulated. Stress and anxiety (n = 13) emerged, particularly around the potential for medical complications, participating in everyday activities (cycling is a worry… related to being anticoagulated, and having a fall (#1; APS+SLE)), and uncertainty around international normalized ratio (INR) levels. Two APS participants shared that they felt like a burden. Other psychosocial impacts (n = 9) include frustration, sadness, optimism, and feeling fortunate to have experienced minimal impacts.
Relationships
Positive and negative impacts on relationships were described. Impacts on family and friends were shared (n = 16); while some relationships were strengthened, others deteriorated: My relationship with my family has become stronger, my relationship with the family that I’m potentially marrying into has become weaker. (#11; APS + SLE)
Amongst family specifically, participants shared caring and empathetic relationships, though tensions due to feeling that parents/siblings were acting overprotective emerged. My mom starts to say ‘oh poor girl.’ (#16; aPLs + SLE)
Relationships with partners were also impacted (n = 10); participants shared supportive experiences as well as tensions that led to impacts on intimacy and even separation: When I was pregnant my partner was not super supportive.(#10; APS)
Finally, participants described how relationships with children were impacted (n = 5). Participants shared worries that children would be impacted by aPLs/APS, feeling like they are overprotective (he doesn’t want me to drive (#13; APS)), and altered parent-child interactions: I’ll bump myself and I’m bruised for months and my kids are like ‘Mummy, what is that?’ (#8; APS)
While emotional, transportation, and financial support from family, friends, and partners were described (n = 14), examples of feeling unsupported also emerged (people don’t like sick people, and I am chronically sick (#20; APS+SLE)). Four participants reported feeling socially excluded due to their illness: Being social is more difficult... I don’t want to go out as much. (#1; APS + SLE)
Participants (n = 5) also shared that due to the rare nature of aPLs/APS, family/friends lacked understanding and are unsure of how to provide support: They don’t understand… it isn’t out there, and it’s really an unknown thing. (#9; aPLs + SLE)
Three participants described that relationships are not affected, and one (aPLs + SLE) indicated that they had not told family or friends as it has not affected their life.
Leisure/lifestyle activities
Participants also described altering physical activity (n = 7) due to risks associated with taking anticoagulants, physical symptoms ( Before my stroke [I did] an aerial silks class. I can’t do that anymore… if I’m hanging upside down something could happen. (#6;APS + SLE)
Similarly, participants reported impacts to travel (n = 5) due to sedentary periods in transit, challenges securing travel insurance (e.g., while taking warfarin), or the unknowns related to hospitalization in another country. Other impacts on hobbies (n = 2), and sedentary behaviours (n = 1) were described (going to a restaurant and sitting down for an hour (#14; aPLs+SLE)). Seven participants, with aPLs and APS, reported no impacts to leisure activities.
Paid employment
Ten participants (n = 4 aPLs, n = 6 APS) experienced no impacts to employment due to aPLs/APS as they were already retired when diagnosed, have experienced no symptoms, have not missed time at work due to symptoms, or felt supported by employers. Seven described time missed due to thrombotic events, surgery (e.g., heart surgery), being on disability, or maintenance behaviours (e.g., bloodwork). Altered career trajectories were reported (n = 7), though difficulty differentiating between impacts of APS versus other co-morbidities was acknowledged: I have lupus and APS, it’s hard to separate those... Probably it has affected certain career choices, just more with the fatigue, and you know APS is part of that. (#3; APS + SLE)
Ten participants felt that employers and colleagues were understanding, and six described accommodations (e.g., working from home, taking time off). Despite feeling supported, one participant articulated the need to ‘overcompensate so it didn’t create an issue’ and the implicit challenges associated with chronic illness: Companies say they’re supportive but… if they had to choose between two people, who would they choose? Someone who’s never had issues. (#3; APS + SLE)
Family planning
Past and future impacts on family planning were discussed. Six participants shared they had never been pregnant; their aPLs/APS diagnosis was identified as one factor in this decision: One of the reasons we decided to not have any children was lupus at first, but this new diagnosis also. (#15; aPLs + SLE)
All other female participants had been pregnant; four became pregnant following diagnosis, and one was diagnosed during pregnancy. Amongst those who were pregnant prior to diagnosis (n = 9), experiences of pregnancy complications impacted family planning: Because of the issues… we’d always wanted four kids, we stopped after two. (#9; aPLs + SLE)
Experiences of miscarriage (n = 5) and other complications (n = 5) were discussed (I had a blood clot go through my lungs (#18; APS + SLE)), and participants shared how aPLs/APS impacted decision-making. Specifically, fear of pregnancy impacts (n = 5) and passing on their illness(es) (n = 4) were identified (I would be doing a disservice to a future child (#14; aPLs + SLE)). Two participants (both with APS) underwent tubal ligations after experiencing pregnancy complications. Eight participants identified that aPLs/APS did not impact family planning; amongst those who shared why, they identified age at diagnosis, that they were not yet considering having children, or that they did not want children regardless of their diagnosis.
Challenges during pregnancy with LMWH were described. Seven participants identified using injectable blood thinners; while two ‘didn’t think it was a big deal’ (#18; APS + SLE), physical impacts (e.g., pain [n = 3], bruising [n = 2]) and stress and anxiety (n = 3) around taking the shots were described. Six indicated they ‘would do anything’ (#4; APS) for a child and had no choice to maintain their/their fetus’ health. Nine participants had not been provided resources to help them through family planning with aPLs/APS.
Healthcare and treatment
Experiences of healthcare & treatment.
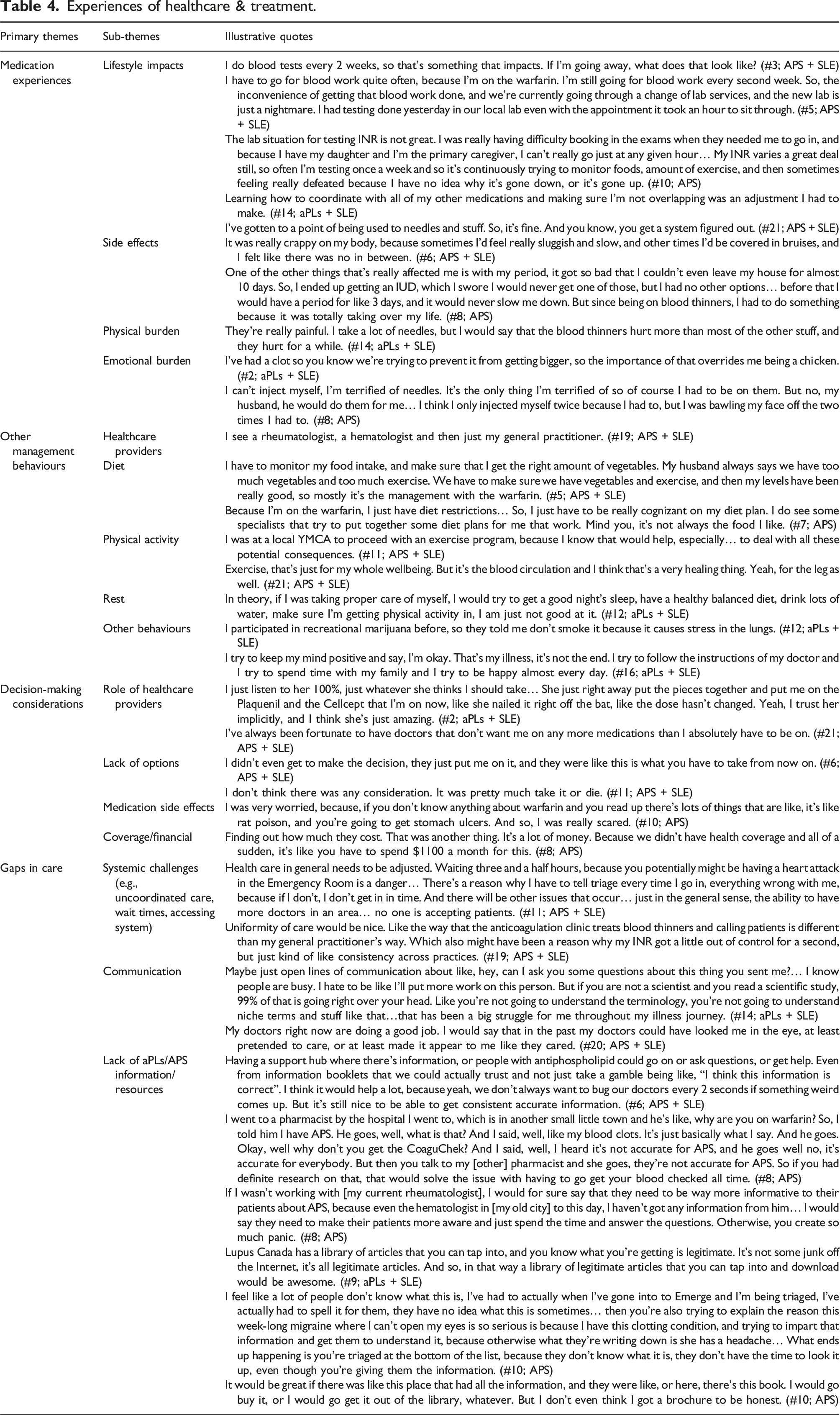
Medication experiences
Various aspects of healthcare and treatment were discussed, particularly around the burden associated with medication use. All participants (n = 21) shared experiences of managing their aPLs/APS with medication, including aspirin (n = 12), warfarin (n = 11), LMWH (n = 6), and other medications (n = 11).
Medication-related lifestyle impacts (n = 14) were described. The challenges of coordinating medication (My life is almost ruled by my medication (#6; APS+SLE)), monitoring diet, and the frequency of appointments for measuring INR were emphasized; challenges with lab accessibility (e.g., wait times, communication) were highlighted. To reduce the lifestyle burden associated with lab visits, four participants identified the potential for at-home INR testing. While one had purchased an at-home testing device, hesitation around accuracy emerged (n = 2; I’m not sure I’d trust that (#1; APS+SLE)).
Medication side effects (n = 9) were also discussed (Warfarin itself is a good medication. I’m annoyed that I can’t get tattoos very often (#11; APS+SLE)). Similarly, the physical burden (e.g., pain/bruising related to taking injectable blood thinners) (n = 6) and measuring INR (n = 2) was shared. The medication-related emotional burden (n = 7) was described; participants shared the ‘constant reminder of disease’ (#20; APS + SLE), fear of needles, and stigma associated with warfarin use.
Other management behaviours
Participants reported seeing rheumatologists (n = 19), hematologists (n = 14), family physicians (n = 11), and other healthcare professionals (n = 10; nephrologists, pulmonologists, gynecologists, dermatologists, physiotherapists, neurologists) for their aPLs/APS. They identified physical activity (n = 7) for both overall health and to ensure blood circulation, monitoring diet (n = 4) for overall wellbeing, and rest (n = 2). Six participants shared other behaviours including monitoring sleep posture, meditation, smoking cessation, avoiding stress, maintaining a positive mindset, and avoiding high-impact activities.
Decision-making considerations
When asked about factors that contribute to medication decision-making (e.g., changing/starting a new medication), the role of healthcare providers was most frequently identified (n = 17). Some participants felt they had no choice (n = 5; it was pretty much take it or die (#11; APS)), and others (n = 4) described the role of potential side effects (I don’t want to create more issues than I already have (#7; APS)). A lack of coverage (n = 2), and other factors (n = 7) including family planning considerations, safety, time, choosing the mildest possible medication, and balancing medication with other lifestyle factors were also identified: As I start going to work… if I forget it more often, how much does that increase my risk? (#14; aPLs + SLE)
Gaps in care
Most participants (n = 18) expressed an overall positive impression of their care, though concerns regarding certain healthcare providers were articulated ([My family doctor]’s not as invested as he used to be (#6; APS + SLE)). When gaps in care were discussed, systemic challenges (n = 6; e.g., uncoordinated care) were shared. Though many (n = 10) spoke positively about communication with physicians, some (n = 6) highlighted communication-related challenges: Doctors treat us like infants, like we can’t be intelligent enough to be the head of our own medical team. (#20; APS + SLE)
When asked about other suggestions to improve care, ten participants indicated they did not have enough information about aPLs/APS; the need for increased accessibility to information (n = 8) for themselves (You’re just sort of paddling blind (#13; APS)), society, and healthcare providers (I would like to have a [family] doctor that knows this syndrome (#4; APS)) was shared. Finally, the need for additional emotional support/support groups (n = 7), and accessibility to healthcare providers (n = 7) were identified ([My physician’s] just like… ask your specialists (#6; APS + SLE)).
Discussion
This study explored patient experiences of aPL/APS diagnosis, daily life, and healthcare and treatment; participants highlighted how the diverse manifestations of aPLs/APS, management-related challenges, family planning experiences, and lack of aPLs/APS supports/resources impose considerable physical, lifestyle, and psychosocial impacts on themselves and their social networks.
While this research is unique in its qualitative exploration of the lifecosts 32 of aPLs/APS, the physical, psychological and emotional impacts identified are similar to those in qualitative studies assessing patient experiences of venous thromboembolism. 36 For example, the shock experienced at diagnosis,36–38 fear of future,36,39 impacts to daily life,36,38,40 and the need for additional information36,41 have been documented amongst those with thrombotic complications more broadly. Participants also shared the burden associated with anticoagulation; challenges around managing diet, maintaining INR levels, and frequent laboratory visits have been described elsewhere. 42 While the emotional burden and lifestyle impacts (e.g., on family planning) echo results from previous qualitative studies with SLE 32 and LN 35 patients, experiences ranging from minimal physical or lifestyle impacts to major thrombotic/obstetric complications emerged in our results due to the diverse manifestations of aPLs and APS. Healthcare providers should be aware of the emotional burden associated with an aPLs/APS diagnosis regardless of a patient’s disease severity; most (n = 17) participants articulated worry about their future following diagnosis, even if they had not experienced a clinical event.
Our sample included patients with aPLs and APS, with/without SLE. While our analysis did not account for differences between groups, the varied experiences of those with aPLs and APS should be acknowledged. For example, diagnosis experiences varied amongst those with aPLs and APS. Some participants had received an APS diagnosis following a thrombotic/obstetric event, while some with aPLs described uncertainty around how they were diagnosed, or were diagnosed based on bloodwork alone. Despite the varied diagnosis experiences, the emotional burden of an aPL diagnosis (e.g., anticipatory fear) remains; of course, I thought I had a blood clot all the time (#12, aPLs + SLE). Similarly, participants with aPLs and APS shared worry about future impacts; for some with APS, this was rooted in previous catastrophic events, and having to ‘wait and see’ if complications arise (#17; APS). Those with aPLs may never experience medical complications, 43 making the ‘wait and see’ experience particularly unique. Some participants reported few or no lifestyle impacts; for example, 66.7% of those with aPLs reported no impacts to paid employment due to aPLs. This is unsurprising as individuals with APS or aPLs/APS and SLE are more likely to experience a higher burden of illness resulting in more substantial lifestyle impacts.
Impacts on pregnancy and family planning were a critical component of the aPL/APS lived experience. Experiences of pregnancy in SLE, 44 and in patients with aPLs/APS21,28,29 have previously been explored; feelings of uncertainty (e.g., around future pregnancy) and the lack of APS information that emerged in previous studies28,29 were consistent with our participants’ experiences. Further, attitudes around anticoagulant use were similar to previously documented APS patient experiences of LMWH in pregnancy 21 ; participants expressed they would do anything to ensure a healthy pregnancy, and described ‘trusting in the doctors’ (#18; APS + SLE) when making medication-related decisions.
Participants’ experiences with aPL/APS supports and resources were limited. A lack of information/resources was reported at diagnosis (n = 13), during pregnancy/family planning (n = 9), and around medication decision-making (n = 10). This is consistent with studies on patient experiences of other autoimmune disease, where participants have reported a lack of information amongst patients,35,45 in society,35,45,46 and compared with other chronic illnesses (e.g., diabetes35,46). Given the lack of resources and the reported medication experiences (e.g., lifestyle impacts, emotional burden), patient decision-making aids around treatment options are needed. Amongst the available resources, participants requested more lay language information, medication-related information, examples to help contextualize management behaviours (e.g., situational examples about sedentary behaviours, information regarding at-home INR testing devices), and targeted information and resources for both those with aPLs and APS with and without SLE. These findings suggest a critical need for advocacy organizations to develop and disseminate more patient resources. Increasing the availability and accessibility of credible aPLs/APS information and incorporating the patient perspective when designing and disseminating resources should be prioritized to ensure supports/resources are meaningful to those affected. 47
While our interview guide asked about patient experiences of aPLs/APS, participants shared experiences related to SLE and other co-morbidities. This may stem from the complexity of the disease and how its manifestations often overlap with other illnesses. The multimorbidity experience has been echoed in other qualitative work,35,48 as patients do not necessarily make sense of their illness(es) based on clinical diagnoses alone. 49 Interactions between chronic illness(es) and their treatments can compound the physical and psychosocial burden, emphasizing the value of person-centered versus single disease-oriented management approaches. 50
Results of this study are not generalizable given the qualitative approach and sample size, however the objective was to provide an in-depth exploration of the broad experiences of individuals with aPLs/APS. This study also has several limitations. Our results may not fully reflect aPL/APS patient experiences as recruitment occurred from a single APS specialty clinic. Second, while we aimed to sample for maximum variation and include participants with diverse demographic, obstetric and thrombotic experiences, our sample included one male and only 19.1% were of non-white race/ethnicity. Eliciting perspectives from a broader range of patients with varying demographic and clinical characteristics will be important future research. Third, experiences that participants attributed to aPLs/APS may have been due to medication side effects, other autoimmune conditions, or other co-morbidities and not aPLs/APS directly. Fourth, some participants were diagnosed 25+ years ago, and recall bias around early illness experiences may exist. Fifth, while virtual interviews can help ensure participant comfort, reduce geographical barriers and time constraints, and provide other qualitative benefits including documenting facial expressions and body language, eight participants chose to keep their camera off, so body language was not visible during their interviews. Finally, though this exploratory study provides insight into aPL/APS patient experiences, generalizable comparisons between subgroups (e.g., aPLs vs APS; aPLs/APS with vs without SLE) are not possible due to sample size. Further investigating the differences between how patients with various disease manifestations and demographics experience aPLs/APS (e.g., through a large-scale survey) is important.
Through semi-structured in-depth interviews this research paints a more complete picture of the aPL/APS lived experience. Results underscore the use and usefulness of alternative epistemologies for contextualizing the experiences of individuals with aPLs/APS, contributing to the potential for policy and practice change.
Supplemental Material
Supplemental Material - A qualitative investigation of the experiences of patients living with antiphospholipid antibodies
Supplemental Material for A qualitative investigation of the experiences of patients living with antiphospholipid antibodies by Francesca S Cardwell, Alexandra O Kobza, Susan J Elliott, Paul S Gibson, Nancy Soliman, Leslie Skeith, Ann E Clarke and Megan RW Barber in Lupus.
Footnotes
Acknowledgments
The data within this manuscript were presented at ACR Convergence 2023 (abstract number 1208). We would like to acknowledge the meaningful contributions of Christine Sperling, our patient partner, APS ACTION (![]() ), as well as the Canadian Venous Thromboembolism Research Network (CanVECTOR) for making this work possible.
), as well as the Canadian Venous Thromboembolism Research Network (CanVECTOR) for making this work possible.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FSC, AOC, SJE, PSG and NS have no conflicts of interest to disclose. AEC has received grant/research support from GSK, and consulting fees from AstraZeneca, Bristol Myers Squibb, GSK, Otsuka, and Roche. LS has received grant/research support from CSL Behring, and honoraria from Leo Pharma and Sanofi. MRWB has received consulting fees from AbbVie, AstraZeneca, Janssen, GSK and Sanofi-Genzyme.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the M.S.I. Research Foundation. AEC holds The Arthritis Society Chair in Rheumatic Diseases at the University of Calgary.
Ethical statement
Data availability statement
To ensure participant anonymity no data are publicly available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.