
Abstract
Objective
Little is known about health literacy in childhood-onset systemic lupus erythematosus (cSLE) and how health literacy relates to medication adherence and psychosocial outcomes in this high-risk population. The objective of this study was to evaluate health literacy in adolescents and young adults with cSLE and its association with medication adherence and quality of life.
Methods
Youth 10–24 years with cSLE (n = 48) completed the Brief Healthy Literacy Screen (BHLS) and the Newest Vital Sign (NVS) to assess health literacy. Participants also completed validated measures of medication adherence and quality of life. Descriptive analyses were used to determine levels of health literacy. Bivariate correlations were used to evaluate associations between measures of health literacy with adherence and quality of life. A multivariable regression analyses was used to determine if health literacy was a significant predictor of adherence or quality of life, after adjusting for age, sex, race, and household income.
Results
Inadequate health literacy was common in this population, with 67% of youth categorized as having inadequate health literacy by the BHLS and 42% by the NVS. Higher medication adherence was associated with a higher BHLS score (r=.36, p = .017). BHLS was also significantly associated with better quality of life (r = 0.31, p = .034).
Conclusion
Inadequate health literacy is prevalent among youth with cSLE. Higher health literacy is associated with higher medication adherence and better quality of life, suggesting that attention to health literacy could improve outcomes for this vulnerable population.
Introduction
Childhood onset systemic lupus erythematosus (cSLE) is a chronic, autoimmune condition characterized by widespread inflammation involving multiple organ systems. Compared to adult-onset lupus, patients with cSLE have a more severe disease course with increased morbidity from irreversible organ damage and a 2-fold increase in mortality rate.1,2 Notably, children with cSLE in minority groups are disproportionately affected and experience higher morbidity and mortality. 3
A recognized catalyst to poor health outcomes is lupus-specific knowledge deficit, which influences medication adherence and self-management. 4 As adolescents with lupus gain more autonomy from their caregivers and become more independent in managing their condition, interventions are needed to target knowledge deficits to improve outcomes. An understanding of how health literacy, defined as the “capacity to obtain, process and understand the basic health information and services needed to make appropriate health decisions,” 5 impacts learning for patients with cSLE is necessary when designing such interventions. Accounting for health literacy is especially important in this population due to the complexity of the condition and associated treatments. 6
Prior studies in adolescent and adult patients with chronic health conditions demonstrate an association between low health literacy with nonadherence to medication, poor self-management, 7 disease specific knowledge deficits, 8 lower quality of life9,10 and negative health outcomes. 11 Limited research in cSLE demonstrates a high prevalence of inadequate health literacy 12 while studies in adult-onset lupus show that patients with low health literacy have poor lupus-specific knowledge, and higher health literacy has been shown to influence successful transition to adult care among patients with cSLE.13,14 However, health literacy in youth with cSLE and its relation to medication adherence and quality of life is poorly understood.
The objective of this study was to evaluate the association between health literacy and medication adherence and quality of life in adolescents and young adults with cSLE. We hypothesized that higher health literacy would be correlated with higher medication adherence and quality of life. The results from this study have the potential to inform the design of future quality improvement initiatives focused on increasing use of developmentally appropriate educational materials to improve health outcomes in patients with cSLE.
Patients and methods
Participants and procedures
Study participants included adolescents and young adults with cSLE aged 10–24 years. Inclusion/exclusion criteria were (1) confirmed diagnosis of cSLE by ICD-10 code (2) ages 10 through 24 years (3) English speaking and (4) no significant cognitive dysfunction or developmental delay diagnoses. Eligible participants were invited to participate by study staff during routine pediatric rheumatology outpatient clinic visits at an academic medical center. Written informed consent and/or assent was obtained from caregivers and participants.
Data were collected and stored within Research Electronic Data Capture (REDCap), a secure, HIPAA-compliant web-based application. Questionnaires were administered electronically using an iPad, and participants’ answers were entered directly into REDCap. One questionnaire, the Newest Vital Sign, was administered orally by a member of the research team, and answers (correct or incorrect) were transcribed into REDCap by that individual at the time of administration. Direct entry of data into the electronic database minimized transcription error and missing data points that could potentially bias the study. Study procedures were approved by the hospital’s institutional review board (IRB #230076).
Measures
Demographic data including age, gender, race, ethnicity, city, state, zip code, insurance type, education level, employment status, caregiver level of education and annual household income were obtained via a questionnaire developed for the study.
Health literacy was assessed using two measures: the Brief Health Literacy Screen (BHLS) and the Newest Vital Sign (NVS). The BHLS is a three-item validated tool to identify patients with inadequate health literacy 15 which has been tested in adolescent patients.16,17 The questions are: “How often do you have someone (like a family member, friend, hospital/clinic worker or caregiver) help you read hospital materials?”; “How often do you have problems learning about your medical condition because of difficulty understanding written information?”; and “How confident are you filling out forms by yourself?” Likert-scale response choices, scored from 0 to 4, ranged from all of the time to none of the time for the first two questions, with reverse scoring for the third question. The categorical scoring algorithm defines inadequate functional health literacy as scores of 0–6, marginal functional health literacy as scores of 7–9 and adequate functional health literacy as scores of 10–12. 18 In this analysis, we report the summed score of the three questions, and we used a summed score of ≤9 as the clinical cutoff for inadequate health literacy, in line with previous studies.17,19,20
The NVS is a valid and reliable, six-item screening tool verbally administered that assesses both reading comprehension and numeracy using a nutrition label from an ice cream container. Total scores range from 0 to 6. Scores of 0-1 are categorized as indicating a “high likelihood of limited literacy,” scores 2-3 indicate the “possibility of limited literacy” and scores 4–6 indicate “adequate literacy.” 21 The NVS has been used and validated in children as young as 10 and those with SLE.22,23 For our analysis, we considered scores <4 as inadequate health literacy, in line with prior studies. 23
The Medication Adherence Self-Report Inventory (MASRI) was used to measure medication adherence. The MASRI is a 12-item questionnaire of self-reported medication adherence measuring both frequency and timing of medication administration. It includes a visual analog scale from 0–100% used to estimate adherence rate during the preceding 1 month. Higher percentages on the scale indicate a greater degree of medication adherence. 24 The MASRI has been found to be both reliable and valid in a cohort of patients with SLE that included adolescents. 25 Although questions regarding the frequency of medication administration were asked in accordance with the validation study methods, only results from the visual analog scale score were used in the analysis of this study, in line with previous studies of adolescents with SLE.26,27
Quality of life was measured using the Pediatric Quality of Life inventory Rheumatology Module (PedsQL-RM), which is a valid and reliable tool used in children as young as eight years of age with rheumatologic diagnoses, including SLE. 28 It is composed of 22 items comprising five dimensions: pain and hurt; daily activities; treatment; worry; communication. Each dimension has three to seven questions with a scale of 0 (never a problem) to 4 (almost always a problem). Scaled scores range from 0–100, and higher scores indicate a better quality of life with fewer problems or symptoms. 28
Finally, we asked participants about their preferred method of receiving educational information about their diagnosis, medications, etc. Options included the following: during their clinic visit with provider, an additional virtual visit with provider, additional visit with another provider (nurse, social worker), paper handout at the end of clinic visit, website, case examples to practice scenarios to learn the information and discuss at next visit, application on phone, talking to other patients with lupus (like a group visit) or videos. Participants were asked to rank these options from 0 (most preferred) to 9 (least preferred).
Statistical analysis
We inspected data for outliers and identified two scores on the MASRI that were >3 standard deviations from the mean, so these were removed from further analysis. We used descriptive analyses to determine levels of health literacy. We used bivariate correlations to evaluate the association between measures of health literacy (BHLS and NVS) with adherence (MASRI) and quality of life (PedsQL). In addition, we used independent t-tests and analysis of variance to determine whether demographic factors were related to health literacy. Finally, we conducted multivariable regression analyses to determine if health literacy was a significant predictor of adherence or quality of life, after adjusting for age, sex, race, and household income.
Results
Participant demographics
Adolescent and young adult participant demographics.
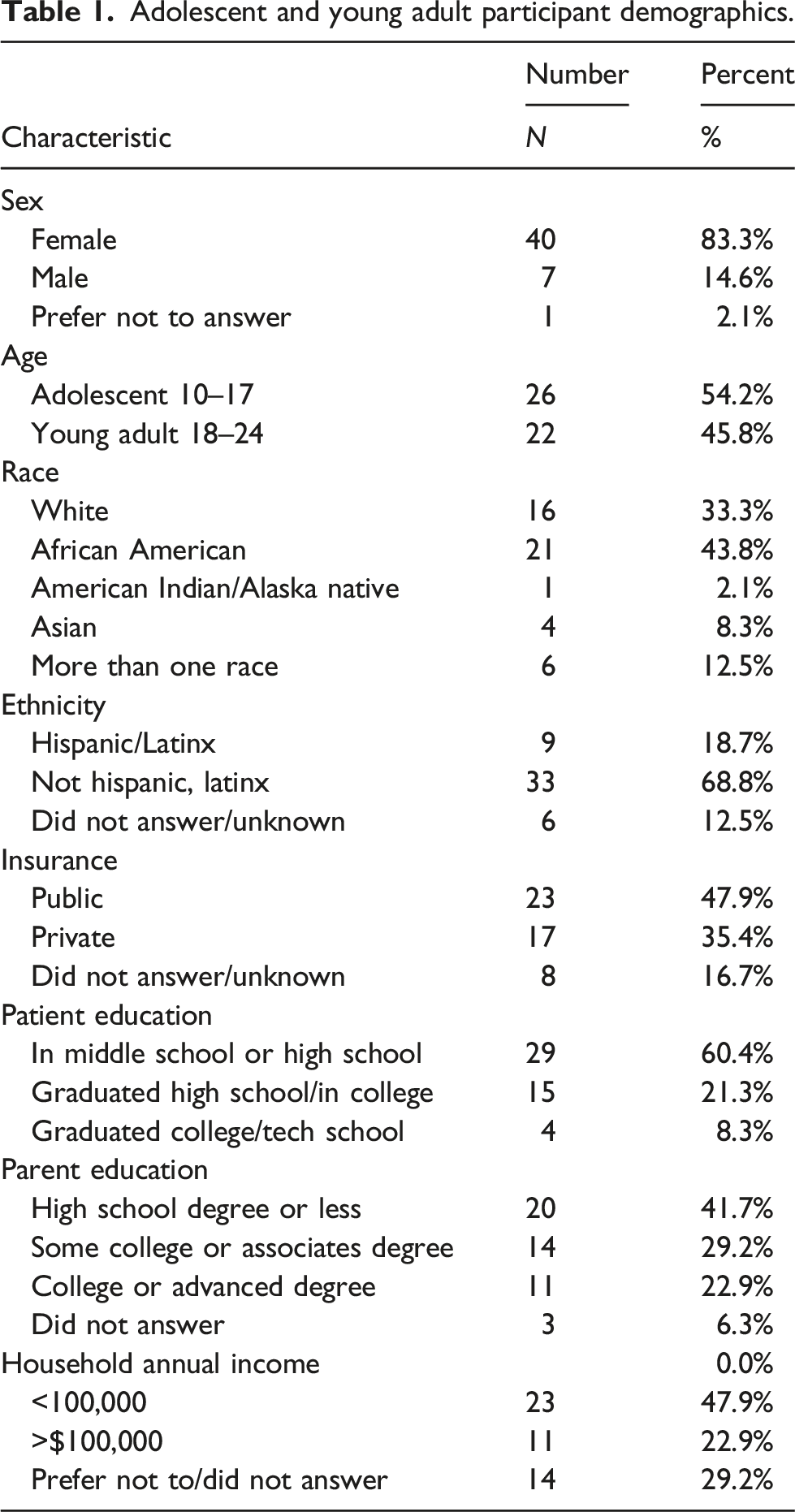
Demographic details of the cohort are outlined in Table 1. Most of the participants were female and there was a relatively even distribution between adolescents aged 10–17 and young adults 18–24. Most participants identified as African American and non-Hispanic. Public insurance represented almost half of the cohort. Patient education level was primarily in middle school/high school while parent education level was primarily high school degree or less. Annual household income was evenly distributed.
Prevalence of inadequate health literacy and demographic correlates
Inadequate health literacy, defined as a BHLS score ≤9, was identified in 67% of participants, and 42% were classified as having inadequate health literacy using the NVS (score <4).
There was no significant difference in health literacy assessed with the BHLS in terms of gender, race/ethnicity, insurance type (public/private), parental education, or household income. However, there was a significant association with age, such that older adolescents reported higher health literacy (r = 0.29, p = .047).
On the NVS, we observed a significant difference related to race/ethnicity. In Black/African American youth, the NVS mean score was 3.2 compared to the mean in adolescents of other race or ethnicity, which was 4 (t = −2.36, p = .023). Additionally, there was a notable difference in NVS score related to income, in which adolescents with an annual household income >$100.000 reported a higher NVS score (mean = 4.8) compared to an annual household income of <$100,000 (mean score = 3.4, t = −2.28, p = .030). There was no significant difference in NVS scores related to age, insurance, or parental education.
Associations between health literacy, medication adherence, and health-related quality of life
Medication nonadherence, defined as a MASRI visual analog score of ≤80% was reported by 26% of participants. Mean health-related quality of life was 76.6 (
Bivariate correlations indicated that the BHLS score was significantly associated with higher self-reported medication adherence (r = 0.36, p = .017) and health-related quality of life (r = 0.31, p = .034). In contrast, the NVS score was not significantly related to adherence (r = 0.31, p = .052) or quality of life (r = -.01, p = .958).
Summary of regression model predicting adolescents’ quality of life.
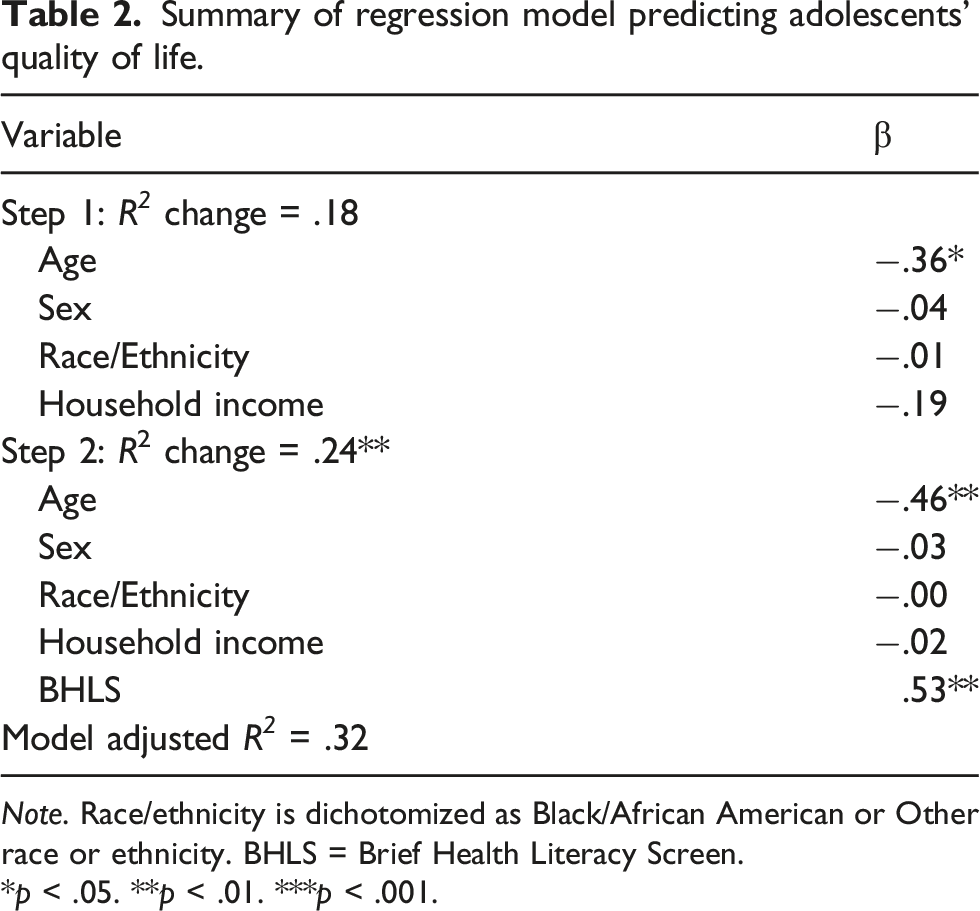
Note. Race/ethnicity is dichotomized as Black/African American or Other race or ethnicity. BHLS = Brief Health Literacy Screen.
*p < .05. **p < .01. ***p < .001.
Finally, we asked patients how they would prefer to receive medical information regarding their diagnosis and treatment plan (i.e., during their clinic visit, a second clinic visit, via a phone application, videos, etc.). Forty-one of the participants completed this ranking section. The most preferred method of receiving healthcare information was during their clinic visit with 37% ranking this as their number one choice. The second most preferred method was a phone application, with 32% of participants ranking this as their second choice.
Discussion
Health literacy in cSLE patients is poorly understood given limited research in this area. The majority of participants in this cohort (67%) reported inadequate health literacy based on a validated screening measure, the BHLS. This is a higher rate compared to previous studies using the same BHLS scoring and cut off. For example, in a similar aged population with asthma, only 25% of participants reported inadequate health literacy. 17 Another study of adolescents seeking care for psychosocial issues demonstrated inadequate health literacy in only 40% of participants. 16 While these are not the same populations, they are similar aged and with a chronic issue, but the prevalence of inadequate health literacy in our cohort is striking in comparison.
Using a different screening measure, the NVS, 42% of our cohort reported inadequate health literacy. Previous studies using the NVS as a screening tool have shown mixed results. One group evaluating health literacy in spina bifida adolescents identified 46% of their participants with inadequate health literacy, 29 and in a separate study of adolescents and adults with kidney disease, inadequate health literacy was noted in 50% of participants. 23 However, a different group found 69% of adolescents with sickle cell disease to have inadequate health literacy using the NVS 30 and another study of cSLE in younger patients (ages 8–19 years) demonstrated 64% with inadequate health literacy. 12 Additional studies in adolescent populations are needed to further evaluate these varied results.
In considering demographic and socioeconomic factors related to health literacy, we observed a significant difference in the NVS as it related to race. Specifically, Black/African American youth had a lower mean score compared to youth who identified as other races or ethnicities. In addition, there was a significant difference in NVS scores related to annual household income, which was used as a proxy for socioeconomic status (SES). It is well known that patients from minority populations with cSLE experience higher disease burden and disproportionately have more significant morbidity and mortality. 3 If there is a higher likelihood of having inadequate health literacy in this minority group, and those with a lower SES, more attention could be focused on these patient populations to continue to combat the health inequities that exist. On the other hand, it could be that the NVS is a biased measure and does not accurately assess health literacy in minoritized populations, as this was not the case in the BHLS. Conversely, it could be more sensitive in detecting inequities as it relates to health literacy given that the cSLE population is more similar to the sickle cell population from a race/ethnicity perspective and much higher rates were detected in the other cSLE study utilizing the NVS.
There were 25% more participants that reported inadequate health literacy using the BHLS compared to the NVS. We used scores of ≤9 as the cut off for inadequate health literacy with the BHLS, while scores of 7–9 indicate marginal functional health literacy. 18 If only categorizing those patients with a score of less than seven, the number of participants with inadequate health literacy with that cut off would have been lower and more closely related to the number as indicated by the NVS screening tool. The BHLS is a subjective measure of health literacy whereas the NVS primarily assesses reading comprehension and numeracy. As the NVS involves math and orally administering the question with verbal responses, several patients became nervous or uncertain in their responses. Additionally, many did not know how to appropriately read a nutrition label. This is highly concerning, particularly for those with lupus nephritis in which food label comprehension is important for their disease management, but also with regards to numeracy skills for interpreting and adhering to one’s medication plan. These problems were also highlighted in another study in cSLE patients with inadequate health literacy using the NVS. 12 While this is important to consider, the NVS may not be the ideal tool to screen for health literacy in our patient population, particularly the younger adolescents, given the medium in which it is delivered and the potential anxiety associated with administration of the NVS. The BHLS is a brief, three question, easily administrable tool that could be used to evaluate health literacy in cSLE. It may be a better screening tool to use in clinical practice as it was associated with both medication adherence and quality of life.
Our finding that lower health literacy (using the BHLS) was correlated with lower medication adherence supports previous studies in patients with other chronic illnesses that indicate lower health literacy is associated with medication nonadherence.7,31–33 In a disease that often requires multiple medications, some more than once daily or in varied formulations, it is important to focus efforts on understanding health literacy in this patient population and how to relay the information in a developmentally appropriate manner for improved understanding. Adherence to medication is imperative for disease control and positive health outcomes in cSLE, so identifying ways to improve this is necessary.
Health literacy (as assessed with the BHLS) was also strongly associated with quality of life, even after adjusting for demographic factors. This is in line with previous studies in patients with other chronic illnesses showing positive correlations among higher health literacy and quality of life.9,34–36 While we cannot evaluate causation in this cross-sectional study, it is possible that that higher health literacy leads to less disease burden and therefore a better quality of life. By being health literate or being able to process and understand health information and services, such as one’s disease process and why medications are necessary for treatment, adherence to medications and instructions provided by health care teams are more likely to be followed through given the baseline understanding and importance in doing so. With that comes improved disease, less burden and better health related quality of life.
It is imperative to help bridge this gap of inadequate health literacy in successful ways for patients to understand their disease and management plan. Limited studies in cSLE indicate that adolescents desire developmentally appropriate education about their condition.37,38 Several studies have looked at interventions to improve aspects of health literacy in other diseases with varied success. Use of web based education materials have shown better medication adherence, 39 and group training interventions have shown improvements in health-related knowledge, confidence in making decisions, 40 ability to identify disease symptoms and choose appropriate action. 41 However, use of a tele-homecare intervention did not show significant differences in functional health literacy in one study 42 and video interventions alone in another did not show improved comprehension. 43 This illustrates the multiple formats available, tried, and variety of outcomes. Certainly, health literacy universal precautions are encouraged and important, but how to provide information regarding disease and treatment in our patient population in an effective manner is a separate issue. The ranking question in this study showed the most preferred method of receiving information regarding their disease and management is during the clinic visit, while the next preferred method is use of a phone application. This reflects the generation’s desire to receive information in the moment without additional visits or steps to do so, while also demonstrating use of their most used accessory, their cell phone, could be another avenue to target for such interventions.
Additional clinical support and resources could be prioritized for those patients with lower health literacy to ensure understanding of their disease and management plan to ultimately improve their health outcomes. While health literacy universal precautions are necessary, identifying patients with low health literacy could also be helpful to prioritize resources and additional education efforts to ensure understanding, even when universal health literacy precautions are used.
This study has several limitations. Although this sample represents almost half of the cSLE patients at our institution, it is only representative of a single institution patient population, which may not extrapolate to other populations. The relatively small sample size limited power to assess multiple covariates. There are limitations in collecting disease activity and medication details in our current electronic medical given the lack of standard note templates. A larger, multi-center, longitudinal study is necessary to evaluate these findings further.
In summary, this study evaluates health literacy levels in patients with cSLE as it relates to medication adherence and quality of life and found that higher health literacy is associated with better medication adherence and quality of life. Given the well documented association of inadequate health literacy and poor health outcomes, assessing health literacy in this patient population, and prioritizing additional support and educational resources to this subset of patients could lead to improved health outcomes.
Footnotes
Acknowledgments
We thank all the patients for their participation in this study. We also thank Brooke Fine, Kailey Miller and Cheryl Stewart for their contributions to questionnaire administration.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.