
Abstract
Background
Depressive and anxiety symptoms are common in childhood-onset systemic lupus erythematosus (cSLE), yet their etiology and course remain unclear. We investigated the frequency of depressive and anxiety symptoms longitudinally in youth with cSLE, and associated socio-demographic and disease factors.
Methods
Participants 8-18 years with cSLE completed baseline measures [demographic questionnaire, Center for Epidemiologic Studies Depression Scale for Children (CES-DC), Screen for Childhood Anxiety Related Disorders (SCARED), and psychiatric interview] and follow-up measures (CES-DC and SCARED) > 6 months later. Prevalence of clinically significant depressive (score >15 on CES-DC) or anxiety symptoms (score
Results
At baseline, of 51 participants with a mean disease duration of 4.3 years (SD 2.7), 35% (n = 18) and 35% (n = 18) had clinically significant depressive and anxiety symptoms, respectively. Anxiety disorder was diagnosed by psychiatric interview in 14% (n = 7), depressive disorders in 6% (n = 3), and post-traumatic stress disorder in 4% (n = 2). Adverse childhood events and first-degree relative with psychiatric condition were present in 40% (n = 20) and 37% (n = 18), respectively. In multivariable regression analysis, baseline depressive symptoms were positively correlated with neighbourhood-level material deprivation (β = 4.2, 95% CI [1.0, 7.3], p = 0.01) and psychiatric condition in a first-degree relative (β = 7.3, 95% CI [2.2, 12.4], p = 0.006). No associations were found between baseline anxiety scores and patient factors. At a median follow-up of 13.5 months (IQR 10.5, 18) for CES-DC (n = 34) and SCARED (n = 44), depressive and anxiety symptoms were persistent (18%, n = 6; 16%, n = 7), and newly present (24%, n = 8; 16% n = 7) at follow-up.
Conclusion
In this sample, depressive and anxiety symptoms were prevalent and persistent. Depressive symptoms correlated with neighborhood-level material deprivation, and family psychiatric history. These findings support routine psychosocial assessment in cSLE, and provision of appropriate resources.
Introduction
Childhood systemic lupus erythematous (cSLE) is a multisystem, chronic autoimmune disease affecting up to 1 per 10,000 children and can be associated with significant morbidity and mortality due to multi-organ inflammation, including neuropsychiatric features. 1 Mood and anxiety disorders occur frequently in children, among the 19 neuropsychiatric syndromes described in SLE by the American College of Rheumatology (ACR) Ad Hoc Committee on Neuropsychiatric Lupus. 2 However, it often remains unclear if depression and anxiety are a manifestation of central nervous system (CNS) involvement, a side-effect of therapy, due to familial or socioeconomic factors. Regardless of etiology, depression and anxiety in cSLE have been associated with increased ambulatory and acute care medical services use, 3 as well as worse quality of life, medication adherence, self-management, and coping skills.3–7
There are few prior studies examining the prevalence of depression and anxiety in cSLE, though those done show high prevalence with wide range from 20%–58%.3,7–17 There is also uncertainty about whether these symptoms meet diagnostic criteria given lack of standard psychiatric interview. There are conflicting data regarding the relationship between depression and anxiety symptoms, and disease outcomes such as SLE disease activity and damage.4,18,19 There are also limited studies assessing association between depression and anxiety symptoms in cSLE with socio-demographic factors. 6 Additionally, most of these studies in cSLE are cross-sectional, and there is a lack of knowledge regarding the patterns of depression and anxiety symptoms over time.
Our previous work showed a high prevalence of self-reported depressive and anxiety symptoms at 35% and 39%, respectively, in cross-sectional study of children with cSLE 20 which were significantly associated with worse quality of life. Despite high rates of depression and anxiety disorders in cSLE and significant impact on daily life, depression and anxiety assessment are not routinely performed by clinicians using standardized instruments. 21 The Center for Epidemiologic Studies Depression Scale for Children (CES-DC) 22 and the Screen for Childhood Anxiety Related Disorders (SCARED) 23 are time and cost-effective mood screening tools that demonstrate good internal reliability and validity.6,13,24 Interestingly, our prior work shows the prevalence of depressive and anxiety disorder, assessed according to gold-standard Diagnostic and Statistical Manual of Mental Disorders-5 criteria, at 5% and 16%, respectively. 20 Reasons for the discrepancy between symptoms and clinical diagnoses may be several, including the overlap between lupus and depression symptoms such as fatigue, medication treatment side-effects, and the presence of subthreshold symptoms that do not indicate a clinical diagnosis, yet still convey risk for a disorder if persistent.
Given the potential for adverse impact on outcomes in cSLE, it is critical to better understand the contributing factors and course of depression and anxiety symptoms, to inform timely and appropriate mental health (MH) intervention. The current study therefore expands on the previous work to investigate: (i) the frequency of depressive and anxiety symptoms longitudinally in youth with cSLE, and (ii) socio-demographic and disease factors associated with these symptoms.
Patients and methods
Patients
We recruited patients aged ≥8 years when seen at the Systemic Lupus Erythematosus (SLE) outpatient clinic at The Hospital for Sick Children between July 2017 and September 2019. Participants were diagnosed with SLE prior to 18 years old and met 1997 ACR or Systemic Lupus International Collaborating Clinics classification criteria for SLE.25,26 At enrolment, participants had an SLE diagnosis for at least 6 months and English-speaking ability for completing psychiatric questionnaires/interviews. Incipient cSLE patients were excluded. Eligible patients were consecutively approached during their routine clinic visits and written informed consent/assent was obtained from participants and their parents. No monetary payment was offered, but community volunteer hours were provided. The study was approved by the Research Ethics Board of The Hospital for Sick Children (REB number 1000056640).
Study design and procedures
Our study was conducted at The Hospital for Sick Children in Toronto, Canada, and builds upon previously published cross-sectional data examining the prevalence of depression and anxiety disorders by psychiatric interview, and the validity of self-report screening measures. 20 Our manuscript reports on additional cross-sectional and longitudinal data from the study. Our study consisted of three visits: (i) consenting and demographic data collection; (ii) baseline psychiatric data collection and medical chart review; and (iii) follow-up psychiatric data collection. Baseline psychiatric data collection involved completing self-report measures of depression and anxiety, and an in-person diagnostic psychiatric interview, which was conducted by a trained child and adolescent psychiatrist (MQ) or clinical psychologist (AD). These members were trained in the use of the instrument and blinded to the self-report screening scores. Follow-up psychiatric data collection involved self-report measures only, completed at least 6 months after the baseline visit. Study visits took place at the time of routine outpatient SLE clinic visits. Participants who met diagnostic criteria for depressive or anxiety disorders on interview or had positive self-report screen results at any study visit were offered referrals to the Department of Psychiatry for further assessment and/or treatment.
Study measures
Center for epidemiologic studies depression scale for children (CES-DC) questionnaire
The CES-DC is a widely used free self-reported depression inventory consisting of 20 items. It assesses current depressive symptoms in healthy and unwell children and adolescents aged 8-17 years, asking about symptoms experienced within the past week. The CES-DC has four factors: depressed affect, somatic complaints, positive affect, and interpersonal problems. Responses are scored on a 4-point Likert Scale ranging from 0 to 3, with total score ranging 0-60. A score of >15 points indicate clinically significant depressive symptoms (necessitating further evaluation to confirm a depressive disorder). 22
Screen for child anxiety related disorders (SCARED) questionnaire
The SCARED questionnaire is a validated self-report anxiety inventory for children and adolescents aged 8-18 years old. It consists of 41 items describing anxiety symptoms in the past 3 months. Both child and parent versions were collected, but only the child-reported questionnaire was analyzed in this study. Each item is rated on a 3-point Likert Scale from 0 to 2, with higher scores indicating more severe anxiety symptoms. A total score ranges from 0 to 82, and scores
Psychiatric interview data
Psychiatric diagnoses data were collected utilizing the Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime Version 5 (K-SADS- PL-5) psychiatric interview. 27 The K-SADS-PL-5, validated in both research and clinical settings, consists of a main interview and six disorder-specific supplements, 28 and provides gold standard diagnostic assessment of psychiatric disorders in accordance with DSM- 5 criteria. The interview component allows the parent (and child) to provide information on psychiatric history and symptoms, and social/educational functioning history. The Depression (Current) supplement (K-SADS-Dep-C), Anxiety supplement, and post-traumatic stress disorder (PTSD) section of the K-SADS-PL-5 were used to determine if symptoms reach diagnostic threshold. Thoughts of death, suicidal ideation, and previous suicidal attempts were also collected during the interview.
Socio-demographic data
Participants were asked to complete a demographic questionnaire to indicate age, gender, ethnicity, parental marital status, personal and family history of psychiatric conditions, and personal history of treatment for depression or anxiety. Self-reported ethnicity of participants was collected for general description and grouped into the following 9 Canadian Census categories: East Asian, South Asian, Southeast Asian, Hispanic/Latin American, Middle Eastern, White (European descent), Black (African, Afro-Caribbean, African-Canadian descent), Other, or Mixed. Postal codes were collected via chart review to determine neighbourhood-level measures of marginalization according to the 2016 Ontario Marginalization Index (ON-Marg). 29 The Postal Code Conversion File was used to translate patient 6-digit postal codes to dissemination areas, for which marginalization index scores were assigned. 30 We derived the ON-Marg material deprivation subindex as an indicator of poverty, income, housing quality, educational attainment, and family structure of the community at the level of the census dissemination area. 31 We also derived the ON-Marg ethnic concentration subindex, which indicates the proportion of recent immigrants or people identifying as ‘visible minorities’ or both, which measures populations who may experience marginalization related to racism and discrimination. 30 The presence of adverse childhood events (ACEs) was determined from the K-SADS-PL-5 interview (traumatic events), and baseline questionnaire (divorced parents).
Clinical data
The following clinical data were collected from medical record review at demographic data collection time: SLE diagnosis date, history of SLE features including major organ involvement (central nervous system or lupus nephritis), SLE Disease Activity Index (SLEDAI) 2K, 31 SLE medications including corticosteroids and immunosuppressants, presence of other chronic conditions, history of psychiatric diagnoses and psychotropic medication use. CNS lupus history was defined as diagnosis of central nervous system NPSLE per ACR on chart review. 2
Additionally, interim data on mental health care (i.e., referrals and psychotropic medications prescribed), between baseline and follow-up psychiatric data collection timepoints, were collected through chart review.
Statistical analysis
Descriptive statistics were used to tabulate demographic and disease characteristics, depressive and anxiety symptom frequency based on CES-DC and SCARED scores for the baseline and follow-up visits, and the frequency of psychiatric disorders at the baseline visit determined by the K-SADS-PL-5 diagnostic interview. Linear regression models were used to examine patient demographic and disease factors associated with baseline depression and anxiety symptoms. Univariate linear regression examined associations between continuous outcome variables for CES-DC and SCARED scores, and the following patient factors: age, gender, ethnic concentration, neighborhood-level material deprivation, history of an adverse childhood event and a psychiatric condition in 1st degree relative. SLE disease factors included: disease duration, history of major organ disease, disease activity (SLEDAI-2K), current glucocorticoid use, and comorbid medical condition. Factors with univariate associations reaching significance of p < 0.2 were included in separate multivariable models for depression and anxiety. p-values of <0.05 were considered significant. Study data were entered manually and managed using secure REDCap electronic data tool hosted at The Hospital for Sick Children and analyzed using STATA 15 software.
Results
There were 89 patients initially approached for participation in this study (Figure 1). 17 patients declined to participate. Five patients were excluded from the study for having incipient lupus status, as they did not meet either ACR or SLICC classification criteria. Sixty-seven patients consented to participate in the study and completed demographic/disease data collection. Of these, 16 patients did not proceed with the study due to: failure to attend the baseline psychiatric evaluation (n = 14), clinic cancelled with patient not re-booked (n = 1), and interview limited by English proficiency (n = 1). Fifty-one patients who completed the baseline visit (including psychiatric interview, CES-DC, and SCARED-child questionnaires) were included in the final analysis. Flow diagram per Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) guidelines illustrating the enrolment of patients in the study and follow-up data.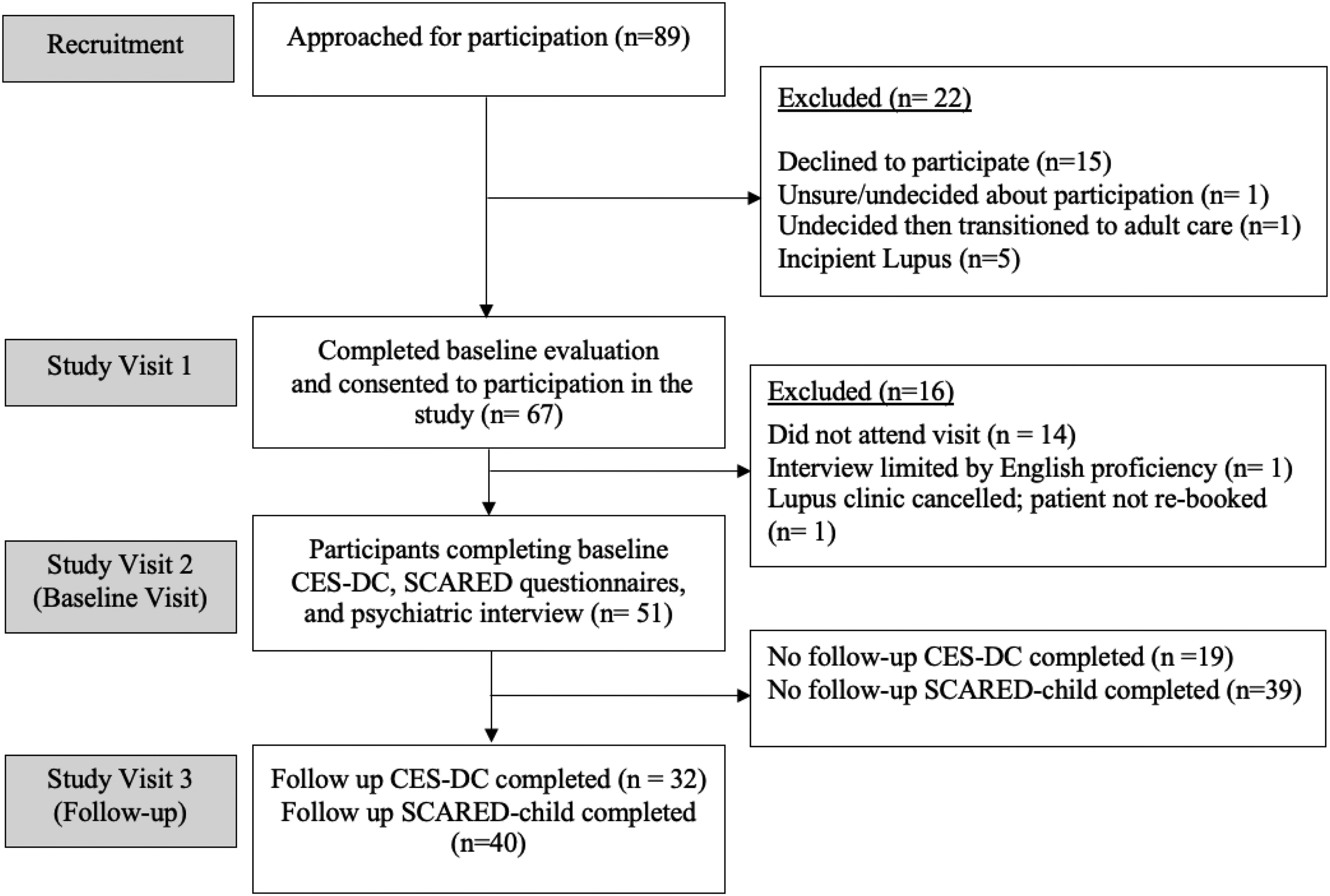
Demographic and disease characteristics of the cSLE sample
Baseline demographic and disease characteristics for patients with cSLE (n = 51).
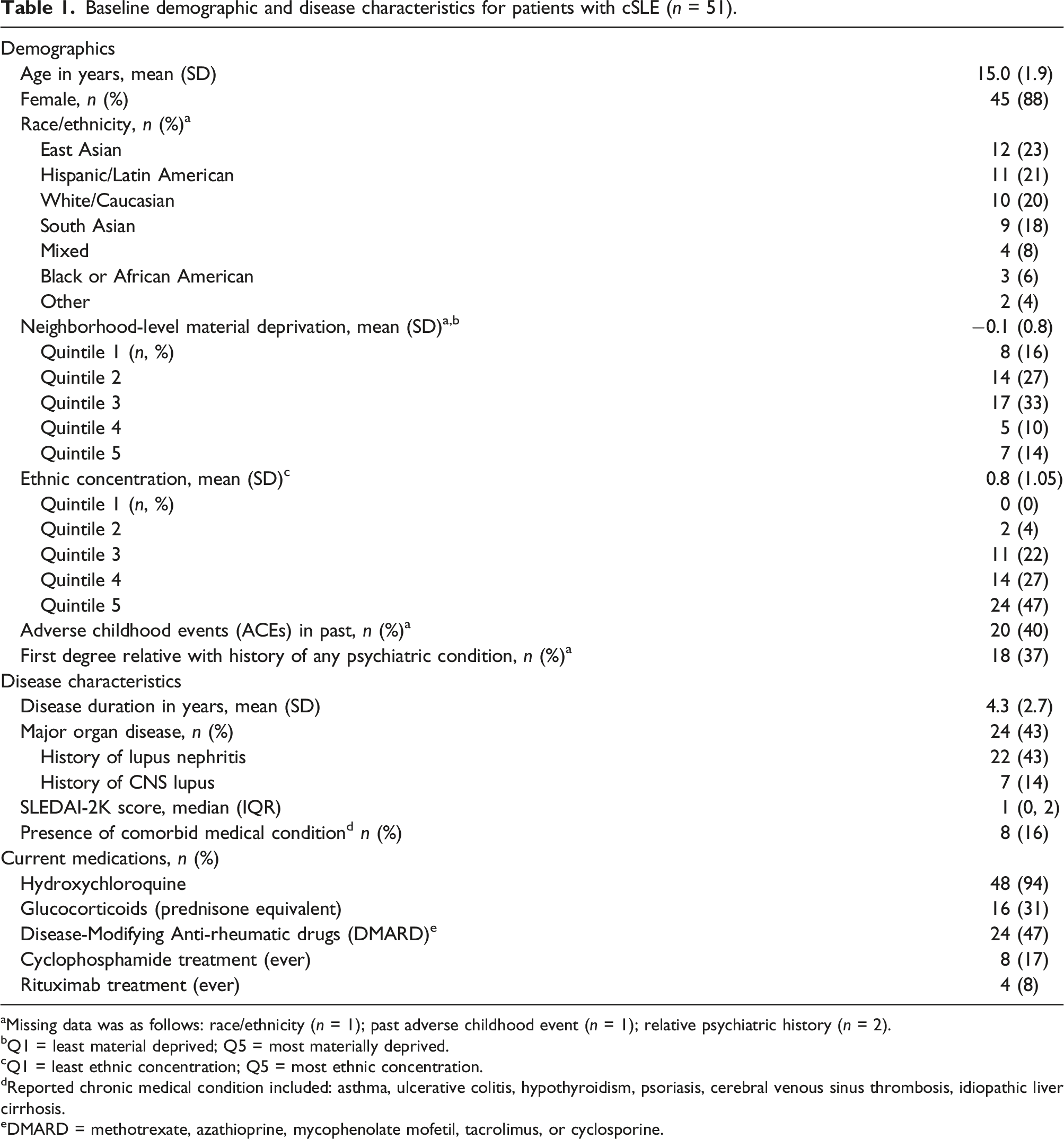
aMissing data was as follows: race/ethnicity (n = 1); past adverse childhood event (n = 1); relative psychiatric history (n = 2).
bQ1 = least material deprived; Q5 = most materially deprived.
cQ1 = least ethnic concentration; Q5 = most ethnic concentration.
dReported chronic medical condition included: asthma, ulcerative colitis, hypothyroidism, psoriasis, cerebral venous sinus thrombosis, idiopathic liver cirrhosis.
eDMARD = methotrexate, azathioprine, mycophenolate mofetil, tacrolimus, or cyclosporine.
Psychiatric characteristics of the cSLE sample
Baseline psychiatric characteristics for patients with cSLE (n = 51).
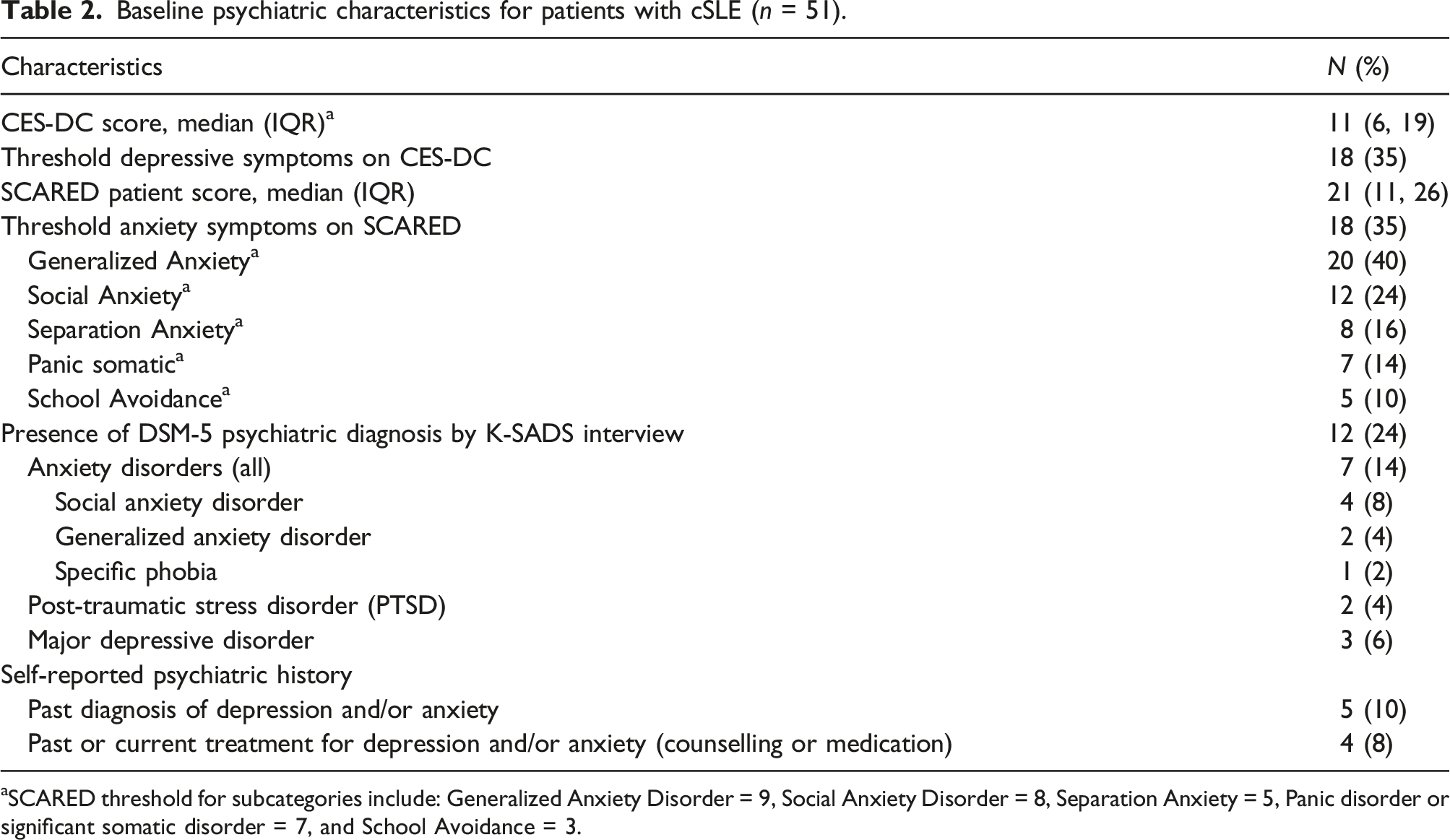
aSCARED threshold for subcategories include: Generalized Anxiety Disorder = 9, Social Anxiety Disorder = 8, Separation Anxiety = 5, Panic disorder or significant somatic disorder = 7, and School Avoidance = 3.
Relationship between depressive and anxiety symptoms, and demographic or disease characteristics
Association between CES-DC depression symptom scores and patient characteristics (n = 51).
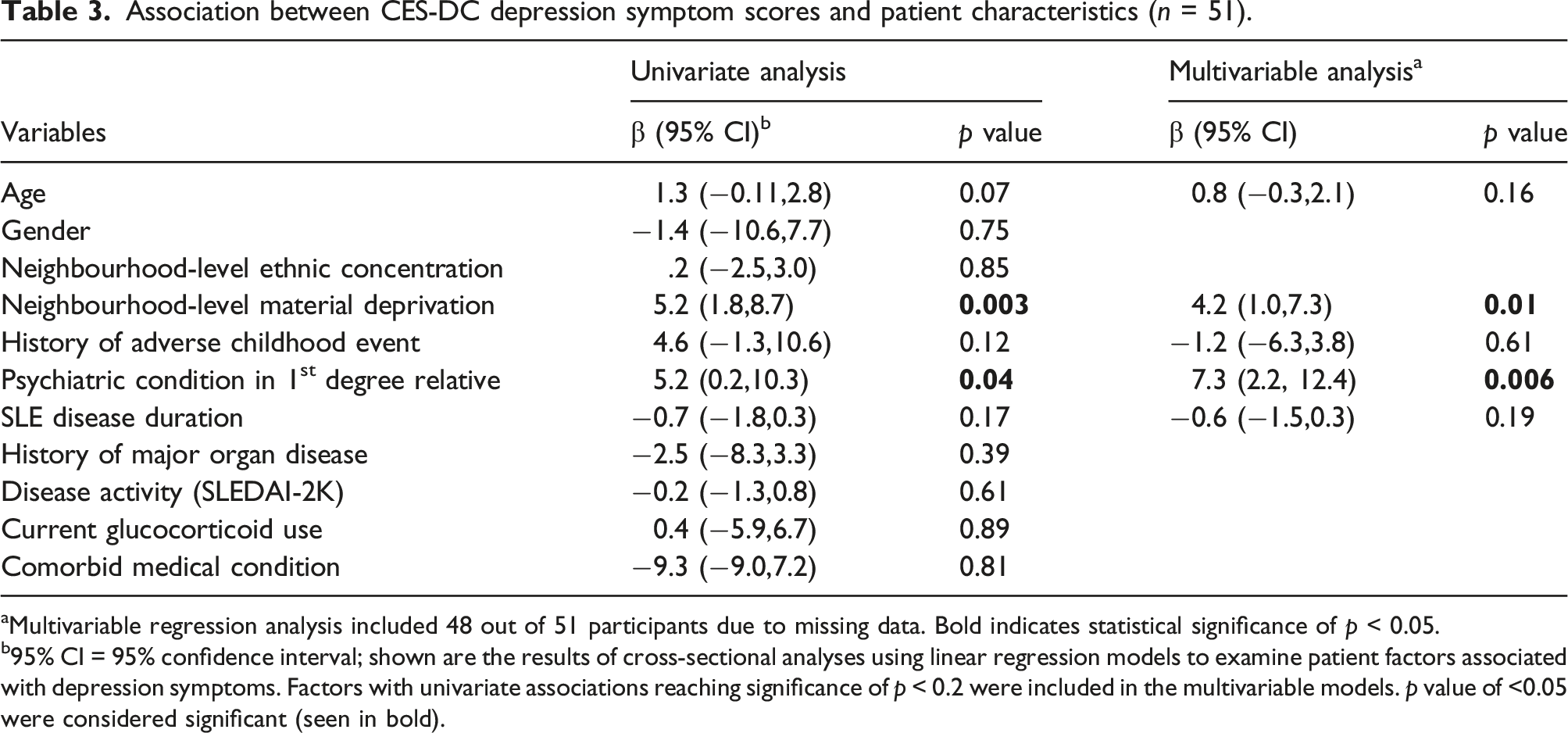
aMultivariable regression analysis included 48 out of 51 participants due to missing data. Bold indicates statistical significance of p < 0.05.
b95% CI = 95% confidence interval; shown are the results of cross-sectional analyses using linear regression models to examine patient factors associated with depression symptoms. Factors with univariate associations reaching significance of p < 0.2 were included in the multivariable models. p value of <0.05 were considered significant (seen in bold).
Association between SCARED anxiety symptom scores and patient characteristics (n = 51).
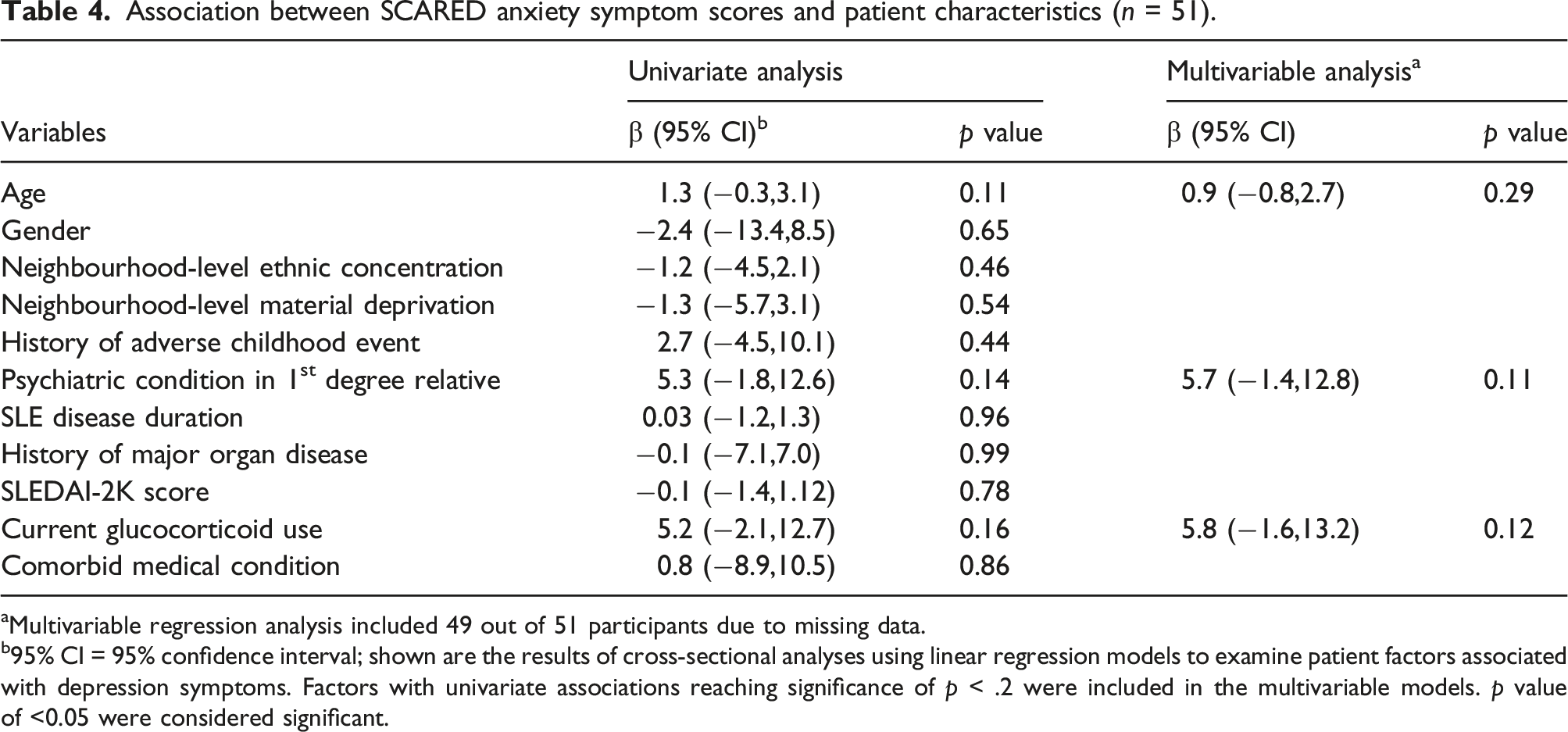
aMultivariable regression analysis included 49 out of 51 participants due to missing data.
b95% CI = 95% confidence interval; shown are the results of cross-sectional analyses using linear regression models to examine patient factors associated with depression symptoms. Factors with univariate associations reaching significance of p < .2 were included in the multivariable models. p value of <0.05 were considered significant.
No significant associations were found between SCARED anxiety scores and any characteristics in the univariate or multivariable regression analyses (Table 4).
Course of depressive and anxiety symptoms at follow-up assessment
Of the 51 patients who completed the baseline CES-DC and SCARED questionnaires, 32 (63%) completed follow-up CES-DC and 40 (78%) completed follow-up SCARED questionnaires. Missing follow-up data was due to patients transitioning to adult care and missed survey completion at clinic visits. The median time between baseline and follow-up questionnaires was 13.5 months IQR (8.5, 19). Median CES-DC and SCARED scores at follow-up visit were 12 IQR (8,24) and 18.5 IQR (11.5, 29.5) respectively. Interim data were assessed for 51 patients between interview and follow-up visit.
Of the 16 patients who scored positive for depressive symptoms threshold at baseline, 9 (56%) patients completed follow-up assessment, of which 6 (67%) had persistent depressive symptoms. Of the 35 patients who scored negative for depressive symptoms, 23 (66%) completed the follow-up assessment, of which 7 (30%) presented with new positive depressive symptoms. Overall, out of 32 patients who completed the CES-DC at both baseline and follow-up visits, 22 (69%) screened the same as baseline, 7 (22%) scored worse (negative to positive), and 3 (9%) scored better (positive to negative) for depressive symptoms (Figure 2). Depressive and anxiety symptoms scores at baseline and follow-up assessment.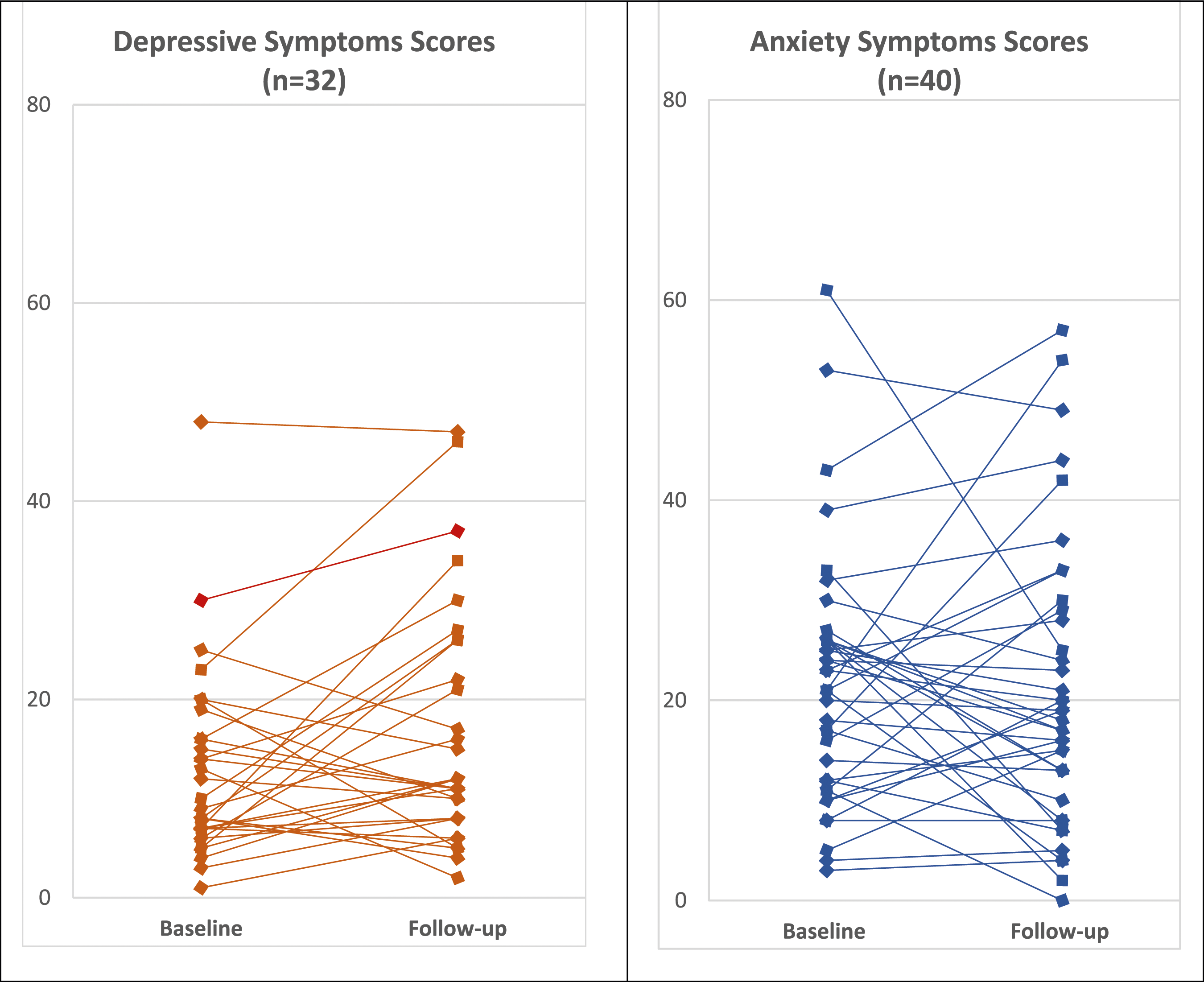
Of the 19 patients who scored positive for the anxiety symptoms threshold at baseline, 16 (84%) patients completed the follow-up assessment, of which 7 (44%) had persistent anxiety symptoms. Of the 32 patients who scored negative for anxiety symptoms, 24 (75%) patients completed the follow-up assessment, of which 6 (25%) presented with new positive anxiety symptoms. In summary, out of 40 patients who completed the SCARED at both baseline and follow-up visits, 25 (62%) screened the same as the baseline, 6 (15%) scored worse (negative to positive), and 9 (23%) scored better (positive to negative) for anxiety symptoms (Figure 2).
In the interim period between baseline and follow-up visits, 10 (20%) patients were referred to any mental health services including adolescent medicine (n = 8), psychiatry (n = 4), social work (n = 1), other counsellor (n = 1). External referrals for community services occurred for 5 patients. Two (20%) patients were prescribed psychotropic medication, specifically antidepressant, by a psychiatrist.
Discussion
Our study assessed frequency, possible risk factors, course of depressive and anxiety symptoms longitudinally, and intervention/referral rates in a cSLE population. Several important findings emerged including high rate of depressive and anxiety symptoms, risk factors of first degree relative with a psychiatric condition and material deprivation, persistence and worsening of depressive and anxiety symptoms over time, and low intervention and referral rates. This is the first study to assess depressive and anxiety symptoms longitudinally and highlights the importance for early screening and referral for support especially for those with risk factors.
First, this study demonstrates high frequency of depressive and anxiety symptoms in a cSLE population at baseline and follow-up which is consistent with prior research in cSLE populations2,7,12–17,32 and other pediatric rheumatic diseases such as juvenile idiopathic arthritis 33 and juvenile dermatomyositis. 17 The prevalence for depression disorder is reported in 11.2%, and 8.3% for anxiety disorder in the healthy general North American pediatric population, when diagnosed with gold standard structured interview with close age and gender matching. 34 Systematic review demonstrates variation in prevalence rates likely due to variation in mood screening tools, sampling sizes, and self-report versus in-person interviews. 11 The prevalence of anxiety disorders ranges from 20%–50% in youth with other chronic medical conditions as well (i.e.. type 1 diabetes (T1DM), asthma, inflammatory bowel disease, and sickle cell disease). 35 There is documented similar high prevalence of depressive and anxiety symptoms between SLE and T1DM. 4 Stressors from living with a chronic condition may explain these findings, however, we did not find depressive or anxiety symptoms to be associated with SLE disease-related factors (such as disease duration, activity, major organ disease or glucocorticoid use) after multivariate analysis. The COVID-19 pandemic and quarantining may have impacted participants’ mood in our follow-up. Similar mental health behaviours were found to be worse in those with cSLE and other childhood rheumatic diseases during the pandemic. 36
We did find that socio-demographic factors such as having a first-degree relative with a psychiatric condition and experiencing neighborhood-level material deprivation increased the risk for depressive symptoms in cSLE patients. However, this association was not observed for anxiety symptoms. The relationship between genetic factors, as well as low socio-economic status and increased risk of mental health disorders is known in the general Canadian youth population.37,38 Socioeconomic status also has a bi-directional effect on mental health symptoms. Low socio-economic status has been shown to negatively affect psychosocial functioning and illness adaptation in cSLE patients. 39 Unfortunately, disparities in MH services among low-income populations is another ongoing concern, thus early mood screening and the ability to provide additional MH resources for those with a first-degree relative with MH conditions or low-income cSLE patients is recommended.
Forty percent of our participants reported an ACE in the past, with 4% meeting PTSD criteria. While ACEs were associated with higher depressive symptom scores in univariate analysis, they were not associated in multivariate analysis. This may be due to overlapping features of ACEs with family history of psychiatric condition and material deprivation, thus future study is needed. Comorbid major depressive disorder is common in people with PTSD, and US data shows 14%–43% of children have experienced at least one trauma, with up to 8% of girls and 2.3% of boys experiencing PTSD. 40 While our study did not focus on PTSD, future studies are needed to examine the relationships between ACEs and PTSD diagnosis in the cSLE population.
We found that over one third of cSLE patients who screened positive for depressive symptoms at baseline remained positive at follow-up, while 20% of those who initially screened negative screened positive at follow-up. Although fewer patients performed worse for anxiety symptoms and anxiety symptoms were not found to be correlated with patient factors, depressive and anxiety symptoms were highly correlated, highlighting the need for close monitoring for both in this population. Chronic psychosocial stress may cause subthreshold symptoms to progress to diagnostic threshold severity in susceptible individuals. This may increase risk of future MH disorders, 41 suicidality, and interpersonal difficulties42,43 particularly in transitional age youth and young adults when combined with ACE and/or psychosocial adversity. Chronic stressful events can activate various physiological responses including the hypothalamic-pituitary adrenal (HPA), neuro-endocrine-immune axes, and sympathetic nervous system 44 linking to inflammatory disorders and putting cSLE patients at risk for depression and anxiety disorders. 45 Therefore, early screening, monitoring, and long-term follow-up of subthreshold symptoms is crucial in this population. Early intervention psychological support should be offered for those with high-risk features.
Self-report questionnaires, such as the CES-DC and SCARED, could offer a low-cost and feasible method of screening for depressive and anxiety symptoms in a busy pediatric rheumatology clinic given the long wait times for psychiatric consultation. Research has shown that self-reported formal mental health screening is feasible in a busy cSLE subspecialty clinic and useful to identify those with depressive or self-harm symptoms. 46 Mental health screening has also been found to be acceptable among adolescents and young adults with cSLE in a multi-center study, and depressive/anxiety symptoms correlated with patient-related outcomes, including fatigue and pain interference, increased pain severity, decreased mobility and peer relationships. 47
Our cSLE population also demonstrated low psychiatric intervention rates with only 1 in 5 referred for MH follow-up services (including psychiatry, adolescent medicine, social work, and counselling). While the exact reason for poor referral rate in our study was not collected, possible reasons for poor referral rates may be due to mild symptoms, long wait time, limited services available, or patient/parent refusal. A previous North American survey of pediatric rheumatologists highlighted barriers to MH services, including limited staff and MH provider resources, with 45% of respondents indicating inadequate treatment of depression and anxiety in adolescents with SLE. 21 Only 31% of responding pediatric rheumatology centers reported having a social worker or psychologist. Inadequate connections to MH services (35%) and inadequate follow-up of MH referrals (52%) were additional barriers to MH care. 48 Our study further illustrates this gap in services and reports low numbers of community MH referrals also. Improved provision of psychological support, including community-based care, which is proportionate to the patient’s needs is required for children with SLE, and could bridge this gap in mental healthcare in this population. 49 Improved supports may include psychoeducation/self-help resources for some, or further counseling for others. For those with depressive or anxiety disorders, cognitive behavioral therapy is the preferred psychological therapy.
Limitations and strengths
Limitations include potential overestimation of depressive and anxiety symptom frequency due to self-report measurements, given patients with active SLE potentially also experience these symptoms. However, the low disease activity of our cohort may have minimized this effect. A healthy control group was not included which may have helped assess the impact of cSLE itself on mental health symptoms. Selection bias may have occurred among those choosing to participate, and there was decreased rate of follow-up for those positive on the CES-DC depressive symptom screen possibly due to lower mood state resulting in potential attrition bias. Interviews were not performed by one interviewer which may have introduced interviewer bias, though we minimized biases by limiting the interviewers to two. Neighborhood-level material deprivation measurement error is also a potential risk. Lastly, there was variable timing and a smaller sample for follow-up assessments due to missed appointments and questionnaire administration; however, this likely approximates the real-world capture of screening data in this cSLE population.
The strengths of our study include utilizing validated screening tools, assessing a wide range of socio-demographic and disease-related risk factors, evaluating longitudinal course of depressive and anxiety symptoms in an ethnically diverse cSLE cohort with good follow-up and retention of patients.
In conclusion, our study shows that clinically elevated depressive and anxiety symptoms by self-report questionnaires are frequent in the cSLE population, despite low disease activity, and symptoms may persist or progress over time to screen positive. There is a need for early screening especially for those with risk factors (1st degree relative with psychiatric condition, or those with material deprivation). To reduce these symptoms, social determinants of health including poverty should be addressed. Clinicians should facilitate routine mood screening in their clinics to support early referral for psychological support and, where indicated, specialist MH assessment and treatment. Long-term studies of the relationship between mood disorders and cSLE disease course, and how to optimize depression and anxiety disorder identification and early intervention in cSLE, are warranted.
Footnotes
Acknowledgements
We would like to acknowledge Dr Earl Silverman, Fatima Ahmad, and Frank Silverio for their support in this project.
Author’s note
Any underlying research materials related to this manuscript can be accessed by contacting Paris Moaf at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Knight has received financial support as the Canada Research Chair in Mental Health and Chronic Disease of Childhood.