
Abstract
Background and objectives
Systemic lupus erythematosus (SLE) is an autoimmune condition that can highly impact patients’ quality of life (QoL). However, there is a lack of knowledge about SLE, affecting the general population and health care professionals (HCPs) alike. This lack of knowledge has negative implications for patients and the healthcare system, worsening prognosis, negatively impacting QoL, and increasing healthcare utilization. The aim of this paper is to draw attention, according to the perspective of the participants of this study, to the lack of awareness of SLE and its consequences in Spain, and to suggest improvements.
Patients and methods
This qualitative, descriptive, observational, multicenter, and cross-sectional study included 40 patients with moderate or severe SLE, recruited during their routine visits in six university hospitals in Spain. The study also included 11 caregivers and 9 HCPs. All participants were individually interviewed. Data from the interviews were coded and analyzed thematically by two anthropologists following a phenomenological perspective.
Results
Our study identified a lack of disease awareness among primary care physicians, emergency medicine doctors, and other specialists treating SLE symptomatology. This led to diagnostic delays, which had a clinical and emotional impact on patients. Furthermore, symptom awareness was found to be context dependent. Differences in symptom awareness between HCPs and patients led to a mismatch between the severity evaluation made by doctors and patients. Some HCPs did not consider the limitations of the current severity evaluation of SLE, and therefore attributed symptoms potentially caused by SLE to the unfavorable socioeconomic conditions patients lived in. Finally, a lack of social awareness among friends, family members, and romantic partners led to lower social support, increased isolation, and negative physical and emotional impact for patients. Gender differences in the provision of support were identified.
Conclusion
This study highlights the need to increase SLE awareness among patients, HCPs, and the broader public in order to improve patient QoL. Being aware of the clinical and emotional impact of such lack of awareness, as well as the role played by context on the patient experience of SLE, is a crucial step towards achieving this goal.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune condition that, in its moderate and severe stages, can highly impact patients’ quality of life (QoL). However, there is a lack of knowledge about SLE, affecting the general population and health care professionals (HCPs) alike.1–3 The frequently non-specific symptoms of the disease’s onset make its early diagnosis difficult. 4 Furthermore, the “invisibility” of some of SLE’s symptomatology contributes to the lack of understanding by the patients’ social circle. 5 It has been shown that a lack of knowledge about the disease has negative implications for patients and the healthcare system, worsening prognosis, negatively impacting QoL, and increasing healthcare utilization.1,6–8
The aim of this paper is to draw attention, according to the perspective of the participants of this study, to the lack of awareness of SLE and its consequences in Spain, and to suggest improvements. Firstly, we focus on the lack of disease awareness by HCPs. Secondly, we evaluate differences in symptom awareness according to patients’ and HCPs’ perspectives, suggesting that symptom awareness is context dependent. Additionally, we show how patients’ contexts are conceptualized by HCPs. Finally, we delve into the social awareness of SLE. Overall, this paper argues that increasing SLE awareness at each of these levels may benefit patients, improving their lived experience of the disease and their QoL.
Materials and methods
Study design
This paper is based on part of the results of the LupusVoice Study, a qualitative, descriptive, observational, multicenter, and cross-sectional study with 40 patients with moderate or severe SLE. Additionally, the study included 11 caregivers and 9 clinicians, reaching a total of 60 participants. Patients were recruited during their routine visits in six Spanish university hospitals. After obtaining written informed consent, doctors compiled information about patients’ personal characteristics, disease, and treatment, and shared their contact information with two anthropologists, who scheduled and conducted the interviews with patients. On eleven occasions, a caregiver was also interviewed; in these cases, informed consent was given by both patient (written) and caregiver (orally) beforehand. Interview questions were open-ended and aimed to elucidate the lived experience of SLE.
HCPs were recruited by the principal investigators from the participating hospitals: eight rheumatologists and one internal medicine doctor. HCPs were interviewed after almost all patient interviews were conducted, with the aim of complementing their view. Interview questions were also open-ended but covered the themes identified in patient and caregiver interviews.
Sample and recruitment
Patients had a documented diagnosis of moderate or severe SLE, were ≥ 18 years at the time of consent, and had been diagnosed with SLE for at least one year prior to enrollment. A moderate-severe diagnosis was determined by either a SELENA-SLEDAI score ≥ 6, current treatment with a biologic or immunosuppressant, treatment with systemic corticoids at a dose ≥ 7.5 mg/day, or by a Physician Global Assessment (PGA) score > 1.5 (on a scale from 0 to 3). Participation in a clinical trial, a Sjogren’s syndrome and/or primary antiphospholipid syndrome diagnosis, hospitalization at the time of inclusion, holding a managing position in a patient association, or having a cognitive dysfunction were all exclusion criteria. Caregivers were defined as people who accompanied the patient throughout their patient journey. HCPs had to be specialized in the treatment of SLE.
Data gathering and analysis
Patients, caregivers, and clinicians participated in remote semi-structured interviews—2h long for patients and caregivers and 1h long for clinicians—via videocall. Interviews were conducted in Spanish. Semi-structured interviews allowed participants to raise issues of concern while simultaneously covering the researcher’s areas of interest. During the interview, patients completed two patient reported outcome measures (PROMs), the generic EQ-5D-5L and the disease specific Lupus Impact TrackerTM. The information gathered with these PROMs was analyzed descriptively. Interview data were coded and analyzed thematically by two anthropologists following a phenomenological perspective, which aims to elucidate the lived experience of a disease and the conditions shaping said experience.9,10 The analytical process was both inductive and deductive, meaning that themes were identified by topics emerging directly from the data and applying prior knowledge. 11 A vast amount of themes emerging from the LupusVoice Study reached saturation. 12 To be able to present them in depth, this paper solely focuses on those related to the lack of SLE awareness and its impact.
Ethics
Study materials were approved by the Research Ethics Committee of Euskadi on the 8th of June, 2022. The study was given the following code: D3461R0005. All participants were asked to verbally confirm their informed consent and permission for the interview to be recorded and transcribed before the beginning of the interview. All data was pseudonymized to protect participant confidentiality. The study followed the principles outlined in the revised version of the Declaration of Helsinki, Good Clinical Practices.
Results
Patient characteristics
Patient characteristics (n = 40).
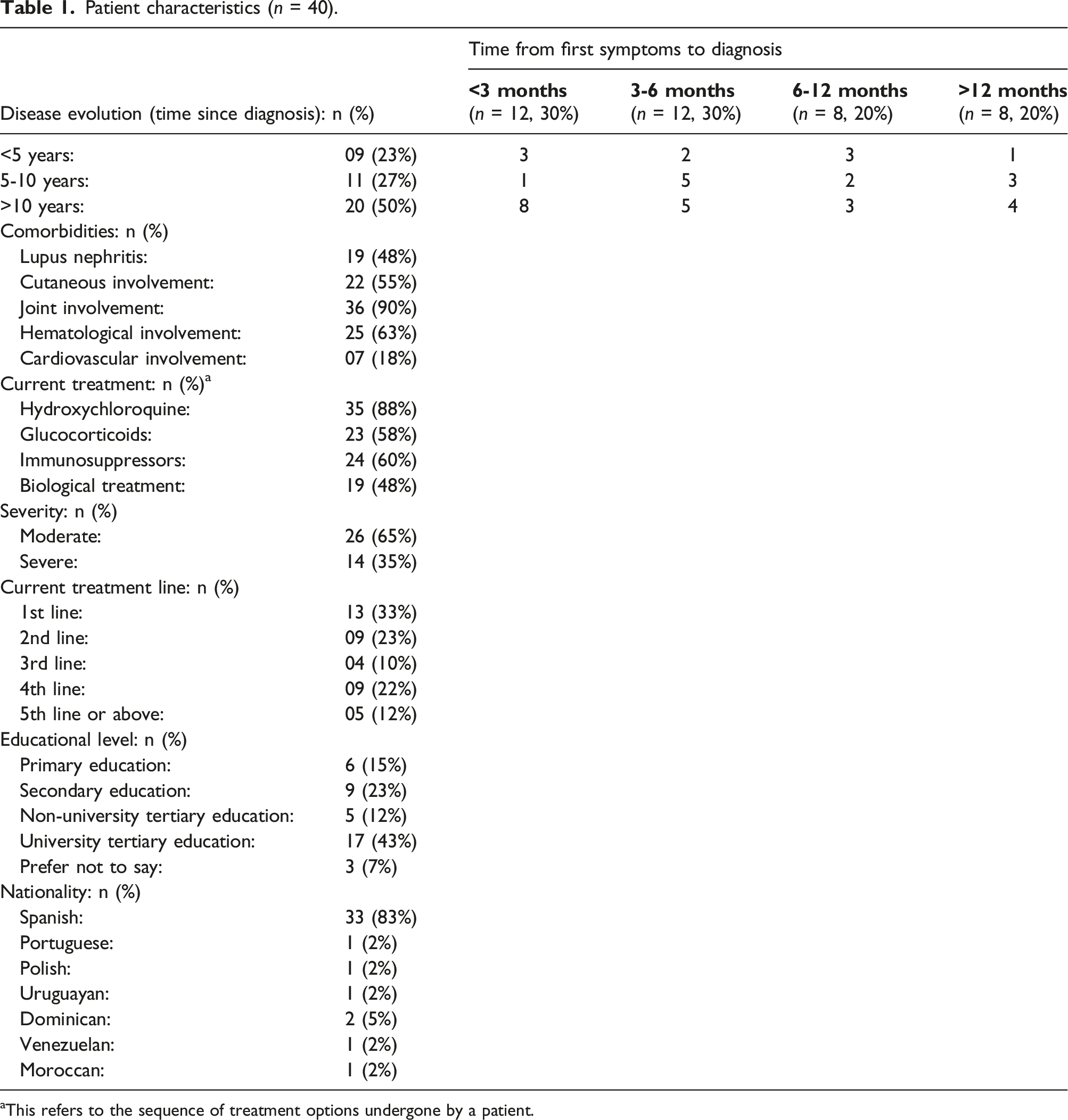
aThis refers to the sequence of treatment options undergone by a patient.
Disease awareness
According to all HCPs, there is a delay in the diagnosis of SLE occurring due to two factors: lack of awareness of SLE and an overwhelmed healthcare system without enough time for doctors to properly assess patients. According to patients’ and HCPs’ perspectives, the lack of awareness is present in primary care, in the emergency department (ED), and among specialists potentially treating SLE symptomatology. In our sample, 30% of patients were reported to be diagnosed within 3 months after the first medical consultation, 30% within 3 to 6 months, 20% within 6 to 12 months, and 20% after a year.
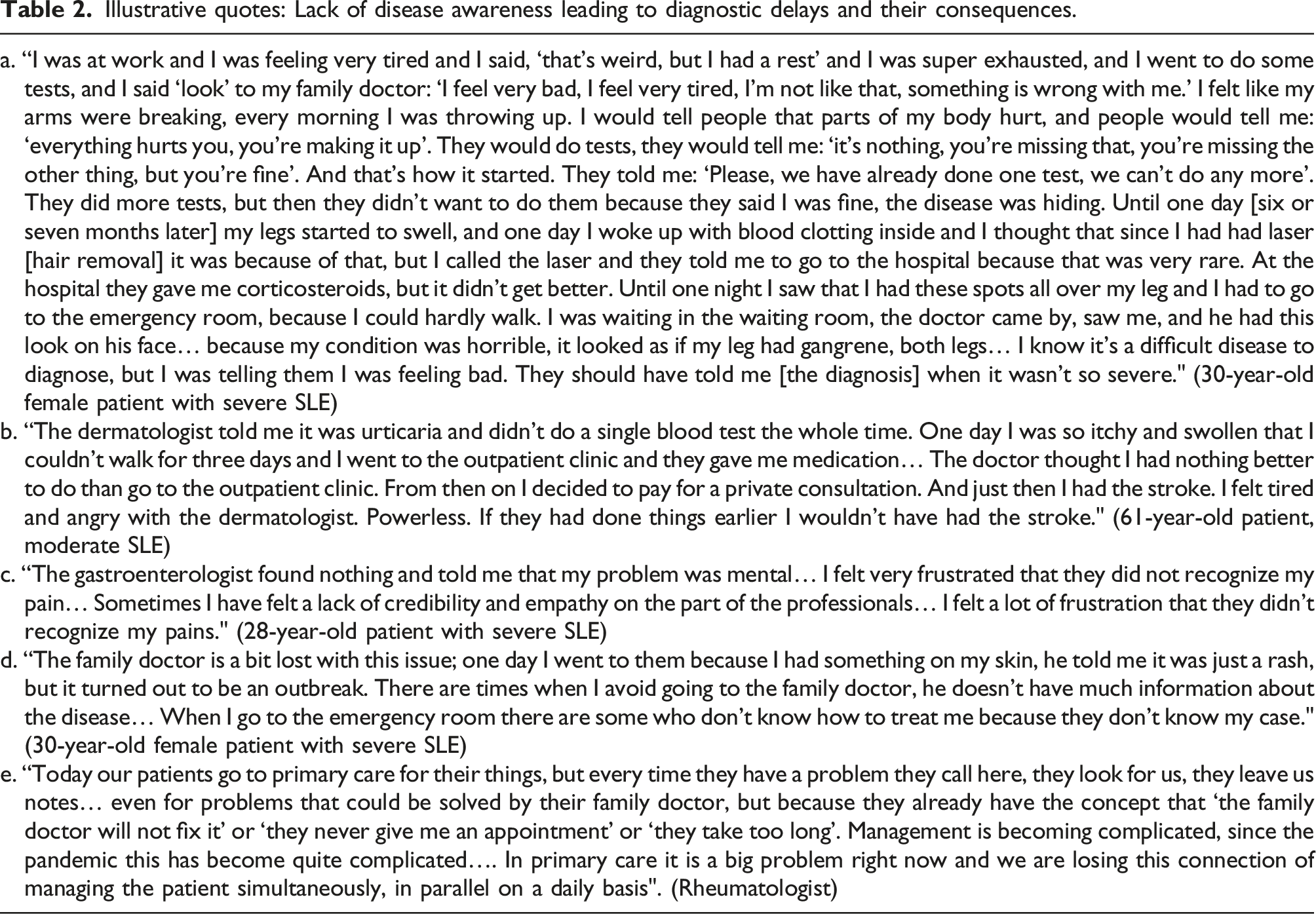
Although our sample had a self-reported mean diagnostic time of approximately 3 months, 33% of the patients complained about how long it took to be diagnosed, highlighting that they had to insist about not being well and had to visit several specialists and the ED without receiving the correct diagnosis. Rather than time, it was the number of visits to the doctors—including to the ED—the number of tests undertook, and the number of times they were dismissed, which constituted a delayed diagnosis as far as patients were concerned.
According to HCPs, a delayed diagnosis can worsen SLE prognosis, increasing disease activity, cumulative organ damage, and the risk of early mortality. Furthermore, a delayed diagnosis may diminish disease control and complicate finding the right medication. Sometimes, a delayed diagnosis implies a misdiagnosis, which may be treated with unnecessary treatments that can cause short- and long-term side-effects.
Illustrative quotes: Lack of disease awareness leading to diagnostic delays and their consequences.
Symptom and context awareness
The study identified a mismatch between the severity evaluation made by doctors and patients. To be included in the study, patients needed either a SELENA-SLEDAI ≥ 6, to be taking biologics, immunosuppressants, or systemic corticoids at a dose ≥ 7.5 mg/day, or a Physician Global Assessment (PGA) > 1.5 (in a scale from 0 to 3). The distinction between moderate or severe was determined by the treating physicians. To be considered moderate, generally patients had to have a SELENA-SLEDAI ≥6 and ≤10, a BILAG B or C, treatment with methotrexate or azathioprine, and minor organic affectation such as moderate arthritis, as well as pericarditis and pleuritis without complications. The following criteria were generally used to classify patients as severe: a SELENA-SLEDAI >10, a BILAG A, organic affectation such as pericarditis with tamponade and effusion, lupus nephritis, or severe or refractory arthritis. For their part, patients perceived the severity of their disease according to its impact on QoL.
Differential impact of each item of the Lupus Impact Tracker between severe and moderate patients.
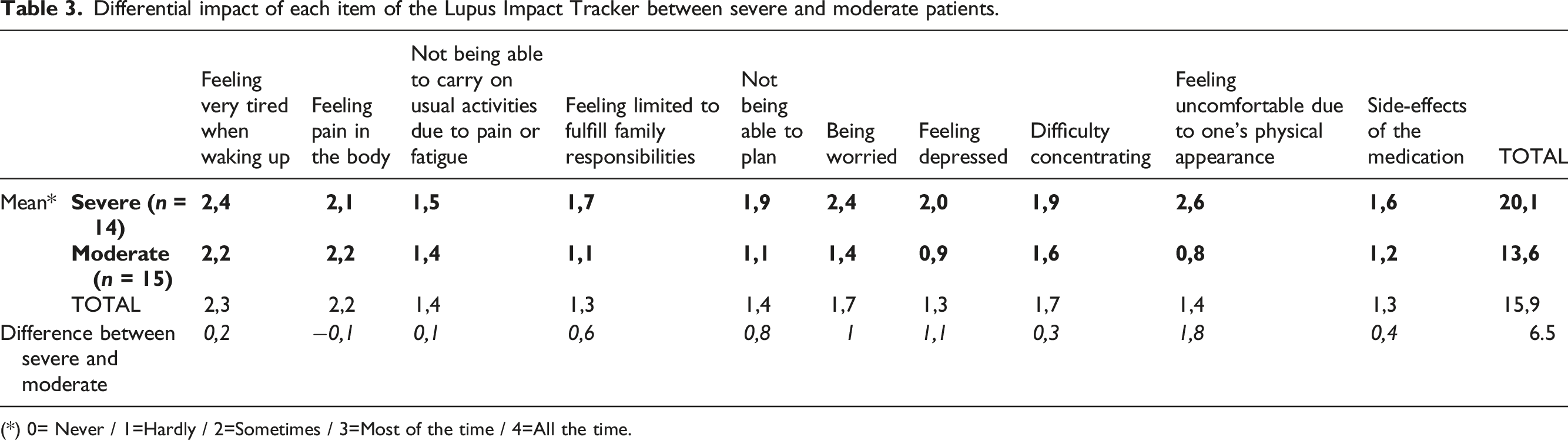
(*) 0= Never / 1=Hardly / 2=Sometimes / 3=Most of the time / 4=All the time.
Results from the EQ-5D-5L questionnaire.
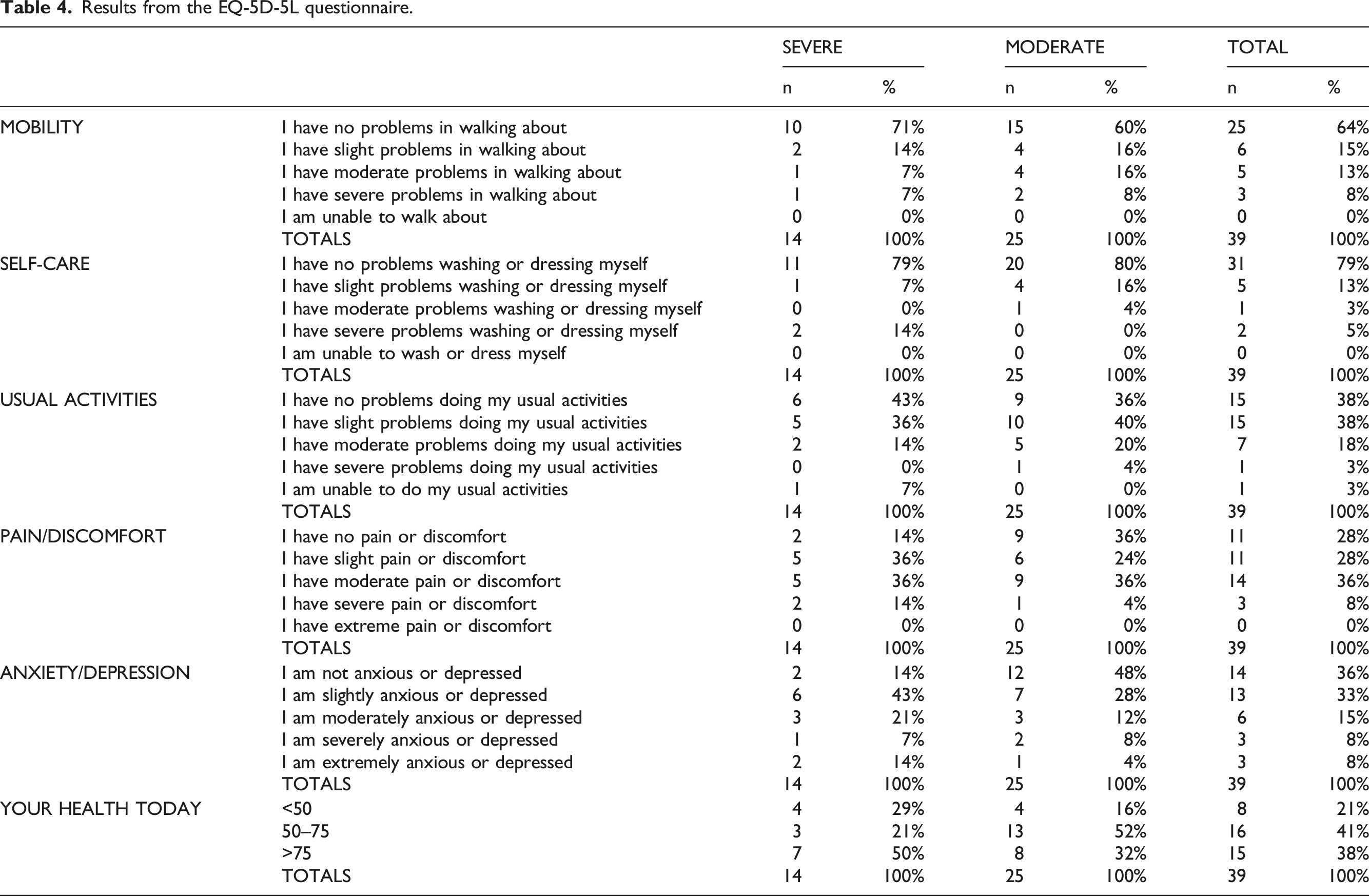
However, if we investigate the results of the EQ-5D-5L questionnaire further, we can observe that this does not apply to all patients. From the total amount of patients who were classified as severe by their doctors, 50% told the interviewer that they were in good health and marked a score above 75. Of the total amount of patients classified as moderate by their doctors, 16% told the interviewer that their health was poor and indicated a score of less than 50. These patients’ perceptions of their health did not match the severity evaluation given by their doctors.
According to the data from the interviews and PROMs, pain and fatigue are one of the reasons for this mismatch. Even though, according to patients, pain and fatigue are very debilitating symptoms with a high impact on QoL, they are not necessarily correlated with disease activity, and therefore not considered in the severity classification of SLE. In other words, symptom awareness differs for patients and HCPs.
Illustrative quotes: symptom awareness as context dependent.
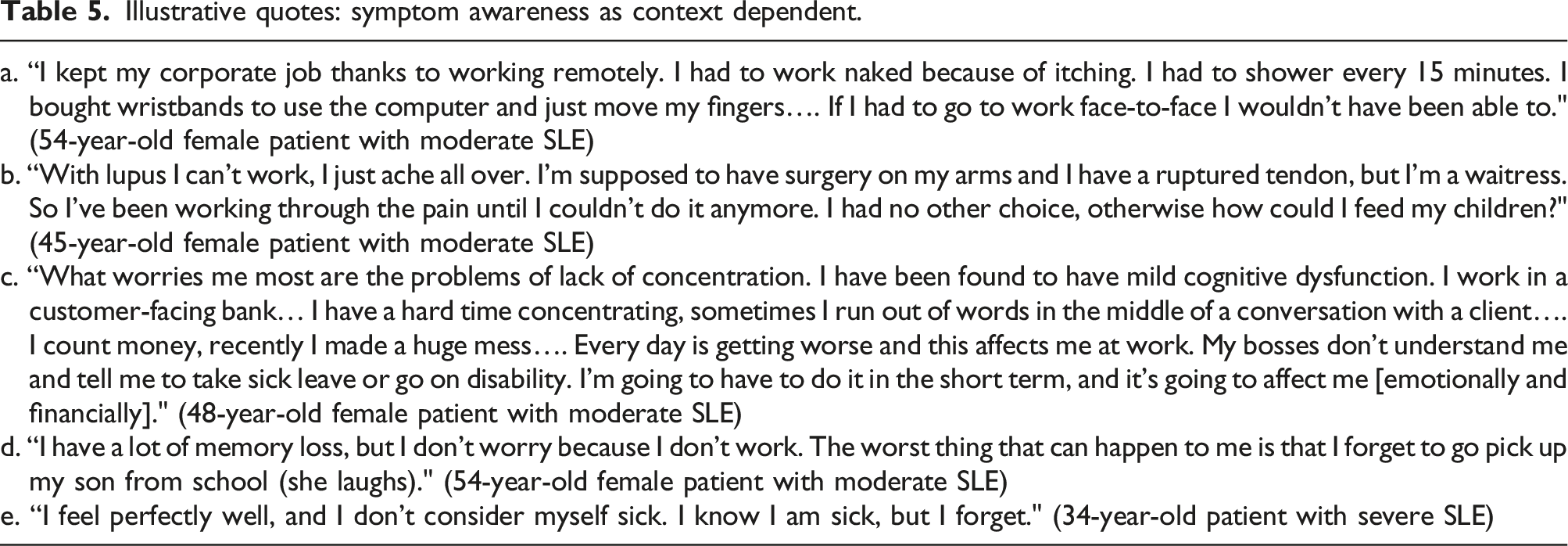
Symptom awareness is also context dependent regarding mild cognitive dysfunction. Some of our patients reported experiencing forgetfulness, difficulty maintaining conversations, and an increased tendency to make mistakes. Those with demanding jobs requiring high levels of concentration were afraid of making mistakes. Mild cognitive dysfunction not only diminished their productivity and increased their fatigue, but also caused problems with management and clients. In the worst cases, patients were worried and anxious about being reprimanded, asked to obtain sick leave, or being fired. Instead, mild cognitive dysfunction was not regarded as a problem by those who did not have a job, arguing that it had no impact on their QoL.
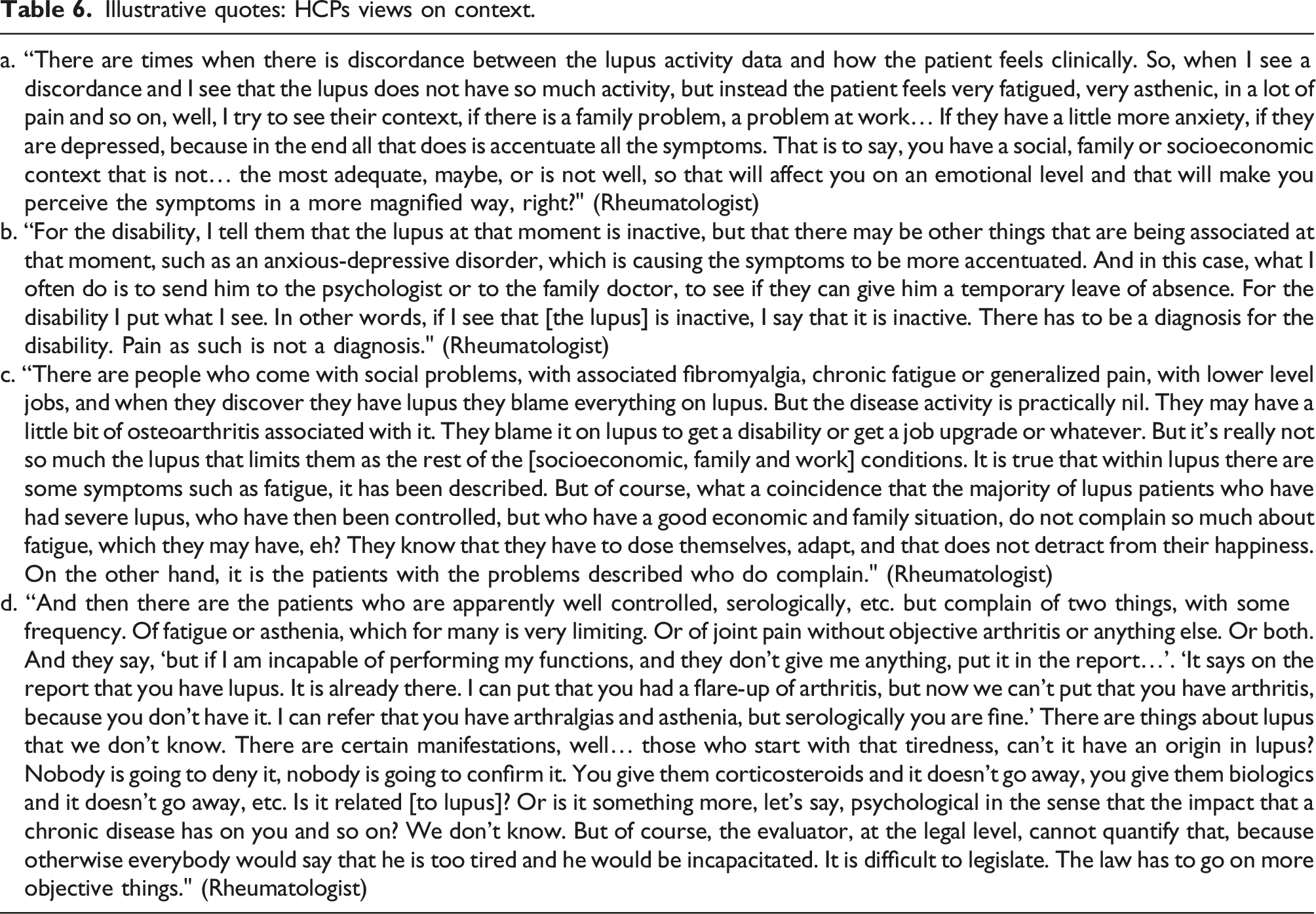
Illustrative quotes: HCPs views on context.
Social awareness
Forty-six percent of patients in our sample reported having family members and friends who were unsupportive due to not understanding SLE because of its “invisibility.” This was especially true when pain and fatigue were the main symptoms. This perceived lack of social understanding took place at different levels.
Firstly, in intimate relationships, 37% of the patients reported being in a relationship and not feeling understood by their partners. Furthermore, 7% reported not being in a relationship and fearing they would not be understood by potential partners; according to them, this thought deterred them from pursuing intimate relationships. Finally, 56% reported being in a relationship and feeling supported and understood by their partners.
Sixty-three percent of HCPs perceived a gender bias in the understanding and support provided by partners. According to them, lack of social awareness of SLE made male partners take SLE less seriously, making female patients feel less supported and understood. In contrast, lack of disease awareness increased the worry of female partners, who fretted over male patients. Of the three male patients in our sample, only one had a partner; they were both interviewed, and the described dynamic applied to them. However, HCPs perceived that younger men were more involved as caregivers—they attended medical appointments with their partners more frequently and they proactively participated in them—than older men.
Friendship was the second level at which the perceived lack of social understanding was identified. Only 38% of patients declared feeling understood and supported by their friends. On the contrary, 47% reported not feeling understood and supported, and 15% feared that they would not be understood and supported. Those patients with a more “visible” disease—such as those with joint deformation—reported feeling more understood and supported because of it.
SLE prevented 59% of the patients from keeping up with their social circle. According to them, lack of SLE awareness meant family members and friends were less likely to accommodate the needs of the patient. Additionally, many patients refrained from socializing to avoid embarrassing questions and insensitive comments. According to patients, this increased their isolation, which in turn worsened their emotional and psychological wellbeing.
Discussion
According to the HCPs interviewed, diagnostic delays in SLE are due to a combination of lack of disease awareness by both patients and doctors—especially in primary care—and an overburdened healthcare system that limits the time spent with each patient.
Several authors have drawn attention to the existence of systematic delays in the early detection of SLE.6,13–17 One study identified a delay of 47 months since symptom onset in a cohort in Germany. 6 Another study with an American cohort reported an average of 5.6 years from the time patients noticed symptoms until they received a formal diagnosis. 14 Several studies have also identified worse health outcomes caused by a diagnostic delay. One study with a German cohort found that the longer the time to diagnosis, the higher the disease activity, disease-related damage and fatigue, and the lower the health-related QoL. 6 Another study with a Danish cohort reported that a delayed diagnosis in patients with lupus nephritis increased the risk of progression to end stage renal disease. 18 Diagnostic delays have also been found to favor an accelerated accumulation of damage, a decrease in quality of life and fatigue, and an increase in mortality in a cohort spanning North and Latin America, Europe, and Asia. 8 Furthermore, a delayed diagnosis has been linked to an increase in health care utilization and flare rates in an American cohort. 7
The mean self-reported time to diagnosis in our sample was much shorter—3 months—than those identified in the previous studies. This may be explained by several factors. First, our study calculated time to diagnosis since first doctor visit, while the rest started at symptom onset. Second, our study included only moderate or severe patients, which may be faster to diagnose than mild ones. Third, patients may have consulted doctors about symptoms much earlier but without these symptoms ever being attributed to SLE. Regardless, 53% of the patients perceived a delay in their diagnosis due to the large number of times they had visited their doctors. This suggests that to consider the impact of a delayed diagnosis, we should not only consider a certain timeframe, but also the frequency of consultations within that timeframe. A study with a British cohort found that patients with SLE attributable clinical features who were ultimately diagnosed with SLE consulted more frequently during the five years prior to their diagnosis compared to a control group. 4 Many of our patients also reported having consulted their doctors many times before diagnosis. And while it seems to be clear that a diagnosis delayed in time can have worse health outcomes for patients, this data suggests that a high number of visits before reaching a diagnosis also has negative consequences, impacting the emotional wellbeing of patients, fostering distrust towards the healthcare system, and increasing the economic burden of SLE.
Therefore, increasing awareness of SLE among HCPs may be a step towards reducing diagnostic delays and their consequences. 19 To this end, more qualitative studies understanding the SLE education needs of HCPs are needed. 3
Several studies have drawn attention to the discrepancies between patient and physician assessment of SLE severity.20–23 In a cross-sectional study with a Peruvian cohort, patients were found to assess disease activity higher than their HCPs due to patients scoring according to how they perceived SLE affected them rather than according to disease activity. 20 Another study reported that patients’ predominant concerns focused on fatigue and function, while physicians’ concerns centered on SLE-related organ complications. This study highlighted that the three highest ranked patient concerns (fatigue, pain, and feeling worn out) were ranked significantly lower by physicians. 22 Our study also showed discrepancies between patient and physician assessment of disease severity, agreeing with the literature and providing new information for Spain.
Additionally, our study underlines the importance of pain and fatigue as symptoms prompting a discrepancy between patient and physician assessment, and argues that awareness of these and other symptoms, such as those resulting from cognitive dysfunction, is context dependent. In this way, our study has identified that cognitive dysfunction has a major impact on the QoL of those patients conducting mentally demanding jobs. In contrast, in a recent quantitative study with a Dutch cohort, cognitive dysfunction was found to be highly prevalent, but with a low impact on QoL. 24 We hypothesize that the discrepancy may be due to the importance of symptom awareness being context dependent. Further quantitative studies are needed to gauge whether the impact of cognitive dysfunction on patients is related to their contexts. If so, contexts should be taken into consideration and analyzed as a risk factor when evaluating cognitive dysfunction in patients with SLE.
The mismatch in the severity evaluation of SLE has real implications for the QoL of those patients who suffer from pain and fatigue but who do not show signs of disease activity. We have seen that the impact of these symptoms on QoL is context dependent, which is not to say that context causes these symptoms by worsening mental health, but rather, makes more salient the impact on their QoL. Nevertheless, our study shows that some HCPs do conceptualize unfavorable contexts as causing unexplained pain and fatigue due to worsening the mental health of patients. Such conceptualization can place a higher burden on patients, who are left not only without a solution to their problems, but also without validation from their HCPs. In a recent study, patients were found to desire to feel validated in their experiences by their HCPs, a desire that, if fulfilled, was perceived by patients to be positively associated with improvements in their condition. 25 In this sense, attributing SLE symptoms such as pain and fatigue to mental health problems caused by unfavorable contexts may contribute to the stigmatization of disadvantaged populations and may preclude the possibility of improving their QoL.
Consistent with the current literature, our study stresses that a lack of social awareness of SLE has a negative impact on patients’ QoL, intensifying their sense of isolation, and worsening their emotional wellbeing.26,27 Several studies have demonstrated that patients’ QoL was compromised when lacking validation and support by their social network.28–30 Trivialization and lack of understanding of SLE, as well as patient stigmatization by family, friends, and physicians, intensified patients’ sense of isolation. 31 Few studies have analyzed the consequences of the lack of social awareness of SLE on intimate relationships. One study with a South African Black cohort drew attention to the concerns of women with SLE, who worried their partners would commit infidelity as a result of the esthetical and physical impact SLE had had on their bodies. 32 Another study focused on the impact of SLE on intimate relationships at the time of diagnosis, revealing patients’ worry about the possibility of not finding a partner. 33 Our study showed that for several patients, these perceptions and worries continued to be present a long time after diagnosis, impacting their emotional wellbeing. Furthermore, several women in our study who had a partner complained about the lack of understanding and support received from them. This matches the work of Schattner and colleagues, who explain that many of the women they interviewed encountered skepticism on the part of their caregivers, consequently experiencing stress, shame, and disempowerment. 34
To the best of our knowledge, there is not much literature regarding the topic of gender differences in SLE beyond the clinical impact they may have. Some studies have identified a gender bias in the diagnosis of SLE, with women frequently waiting two years longer than men to be diagnosed. 35 A study on arthritis in Latinas in the United States identified that women faced a greater burden and psychological distress than men when they were ill themselves or their spouse was ill, and that support providers tended to be other female family members, especially daughters. 36 Our study, conducted almost 30 years after the aforementioned one, seems to indicate that this gender bias in the experience of SLE is still valid for Spain today.
However, and in contrast to the literature, our study also highlights that many of the women interviewed felt understood and were happy with the support provided by their partners. Moreover, HCPs perceived that younger men were more involved as caregivers than older men. Further research is needed to explore whether a shift in male caregiver attitudes is occurring in Spain, as well as the implications it may have on SLE patients’ experience and QoL.
Conclusion
According to patients and HCPs, lack of SLE awareness may delay diagnosis, considered not only in terms of a timeframe but also in terms of the frequency of medical visits. Continuing education for GPs and specialists is essential to reduce diagnostic delays. Our study has identified a mismatch between the severity evaluation of SLE by patients and HCPs. It has also argued that patients’ contexts should not be perceived by HCPs as a causal factor for mental health problems magnifying symptoms. Increasing awareness of the living conditions of patients and the constraints they put on them may help overcome such perception. This would ensure that patients feel validated instead of blamed for the socioeconomic conditions they live in. Finally, our study has shown that lack of social awareness of SLE has a negative impact on patients’ QoL. To address it, it may be beneficial to create awareness campaigns and to involve family members in the treatment of SLE whenever possible. Overall, increasing awareness of SLE at these different levels may improve the lived experience of patients with SLE and their QoL.
Footnotes
Acknowledgments
We would like to thank all study participants for kindly sharing their experiences with us. We also extend our gratitude to the study coordinators, who ensured this study was smoothly executed.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RRR and CSM are employees of A Piece of Pie and have received research funding from AstraZeneca to conduct this study. JSH, MG, and NBR are employees of AstraZeneca. ERA has received honoraria from GSK. All other authors report no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was fully financed by AstraZeneca. As authors of the manuscript, AstraZeneca employees JSH, MG, and NBR have participated in the design of the study and the revision of the final manuscript.