
Abstract
Objective
This study aimed to detail the disease characteristics of systemic lupus erythematosus (SLE) in individuals who are underweight and assess whether underweight status is associated with SLE disease activity.
Methods
This was a retrospective cohort study involving 218 patients newly diagnosed with SLE. Patients were categorized as underweight (body mass index [BMI] <18.5 kg/m2) or not underweight (BMI ≥18.5 kg/m2). We reviewed disease characteristics including the SLE Disease Activity Index 2000 (SLEDAI-2K) at diagnosis. High disease activity was defined as SLEDAI-2K ≥10. Disease characteristics were compared between those who were underweight and not underweight. We used multivariable logistic regression analysis to determine whether underweight status is associated with high disease activity.
Results
Out of the 218 patients, 35 (16.1%) were underweight and 183 (83.9%) were not. Underweight patients had less renal involvement (5.7% vs 20.2%, p = .040), lower C-reactive protein levels (1.0 [0.3–2.3] mg/L vs 1.2 [0.8–5.0] mg/L, p = .028), and lower SLEDAI-2K scores (6.7 ± 4.6 vs 9.1 ± 5.7, p = .009), and were less likely to be at high disease activity status (22.9% vs 42.6%, p = .028), compared with those who were not underweight. Following adjustment for multiple covariates, being underweight was inversely associated with high disease activity status (adjusted odds ratio = 0.38, 95% confidence interval = 0.16 to 0.92, p = .031).
Conclusion
Patients with SLE who were underweight showed less renal involvement and lower SLEDAI-2K scores compared with those who were not underweight. Moreover, those with SLE who were underweight had a 60% lower risk of exhibiting high disease activity.
Introduction
Obesity is a condition characterized by excessive accumulation of adipose tissue and is associated with chronic inflammation. 1 Adipokines, which are produced by adipose tissue, influence systemic immune responses. 2 Immune cells in turn, produce pro- and anti-inflammatory cytokines and affect homeostasis and metabolism of the adipose tissue. 2 This suggests that obesity can affect immunometabolism and potentially alter susceptibility to autoimmune diseases. 3 A large body of epidemiologic studies has shown that obesity is associated with an increased risk of developing autoimmune diseases. 4 Systemic lupus erythematosus (SLE) is an autoimmune disease that can affect nearly any organ of the body. 5 A prospective cohort study has shown that obese individuals have an 85% higher risk of developing SLE compared with those with a normal body mass index (BMI). 6 Furthermore, in patients with SLE, obesity is associated with higher levels of inflammatory markers 7 and worse patient-reported health-related quality of life.8–10 On this basis, controlled and intentional weight loss is recommended for patients with SLE who are overweight or obese, as it could improve SLE outcomes. 11
However, previous studies reporting associations between obesity and worse disease parameters for SLE did not include patients who were underweight.7–10 Therefore, although it is well-known that obesity (compared with normal weight) is associated with worse SLE disease parameters, it is unclear whether patients with SLE who are underweight have distinct disease characteristics. Considering the link between adipose tissue and autoimmunity, 3 patients with SLE who are underweight might have better disease parameters than those who are not underweight due to less adipose tissue. In this study, we aimed to describe the disease-specific characteristics of patients with SLE who are underweight compared with those who are not, and assess whether being underweight is associated with the disease activity of SLE.
Methods
Study cohort
Patients diagnosed with SLE between 2009 and 2019 at a tertiary referral hospital in Seoul, South Korea, were retrospectively screened for inclusion. Exclusion criteria included: (a) those who did not meet the 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for SLE; 12 and (b) those with missing BMI data. Based on the BMI cut-off provided by the World Health Organization, patients with a BMI of <18.5 kg/m2 were categorized as underweight, and those with a BMI of ≥18.5 kg/m2 were categorized as not underweight. 13 Subsequently, patients with a BMI of ≥18.5 kg/m2 were further categorized into normal weight (18.5 kg/m2 ≤ BMI <25.0 kg/m2) and overweight/obese (BMI ≥25.0 kg/m2). 13
This study was approved by the Institutional Review Board of Gangnam Severance Hospital (No. 3-2020-0114). The requirement for informed consent was waived due to the retrospective nature of this study.
Covariates and outcome
The following covariates at the time of SLE diagnosis were reviewed: age, sex, BMI, presence of hypertension, diabetes mellitus, and dyslipidaemia, SLE clinical manifestations (mucocutaneous, musculoskeletal, hematologic, renal, serositis, neuropsychiatric, or vasculitis), positivity of anti-double-stranded DNA (dsDNA) antibody (Ab), anti-Sm Ab, anti-U1RNP Ab, anti-Ro Ab, and anti-La Ab, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) levels, C3 and C4 levels, and the SLE Disease Activity Index 2000 (SLEDAI-2K). 14 The outcome of interest was high disease activity status, defined as a SLEDAI-2K score of ≥10 at diagnosis.15,16
Statistical analysis
Continuous variables are expressed as mean (±standard deviation) or median (interquartile range) for normal or non-normal distribution, respectively, and categorical variables are expressed as numbers (%). To compare disease-specific characteristics between patients who were underweight and those who were not, Student’s independent t-test or Mann–Whitney U test was used for continuous variables with normal or non-normal distribution, respectively. To compare disease-specific characteristics between patients who were underweight, normal weight, and overweight/obese, one-way analysis of variance or Kruskal–Wallis test was used for continuous variables with normal or non-normal distribution, respectively. Bonferroni test was used for post-hoc analysis. To compare categorical variables between groups, χ2 test or Fisher’s exact test was used. The association between underweight status and high disease activity status of SLE was assessed via logistic regression analyses, using the underweight status as the independent variable and high disease activity as the dependent variable. Model 1 was univariable, model 2 was adjusted for age and sex, and model 3 was adjusted for age, sex, hypertension, diabetes mellitus, and dyslipidaemia. Odds ratios (ORs) and 95% confidence intervals (CIs) for high disease activity status in patients who were underweight were estimated using those who were not underweight as the reference. Statistical significance was set at a p value of <0.05. All analyses were performed using SPSS software (version 25.0; IBM Corporation, Armonk, NY, USA).
Results
Patients’ characteristics
Characteristics of patients with SLE.
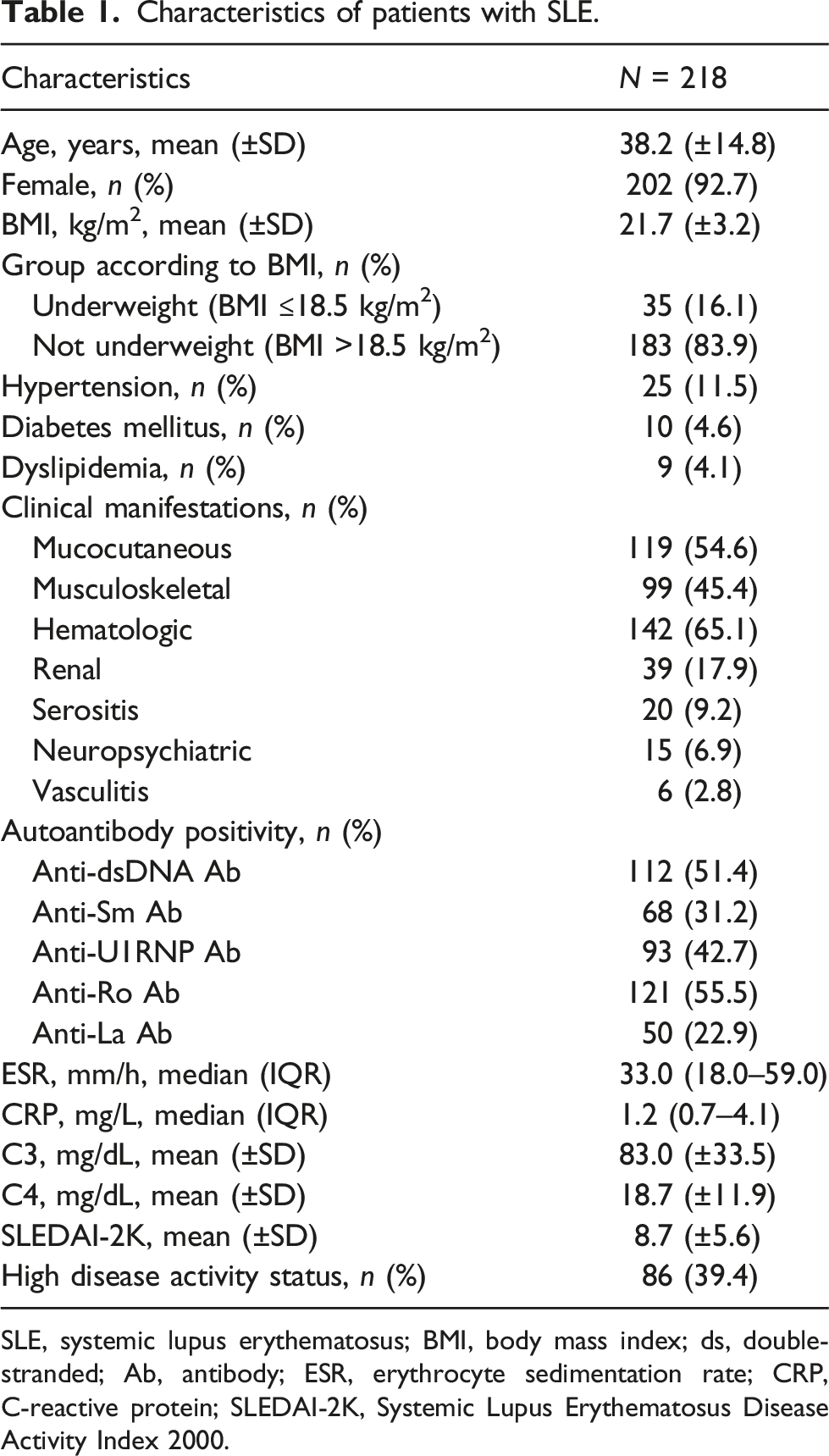
SLE, systemic lupus erythematosus; BMI, body mass index; ds, double-stranded; Ab, antibody; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000.
Comparison between patients who were underweight and who were not underweight
Characteristics comparison between patients with SLE who were underweight and those who were not.
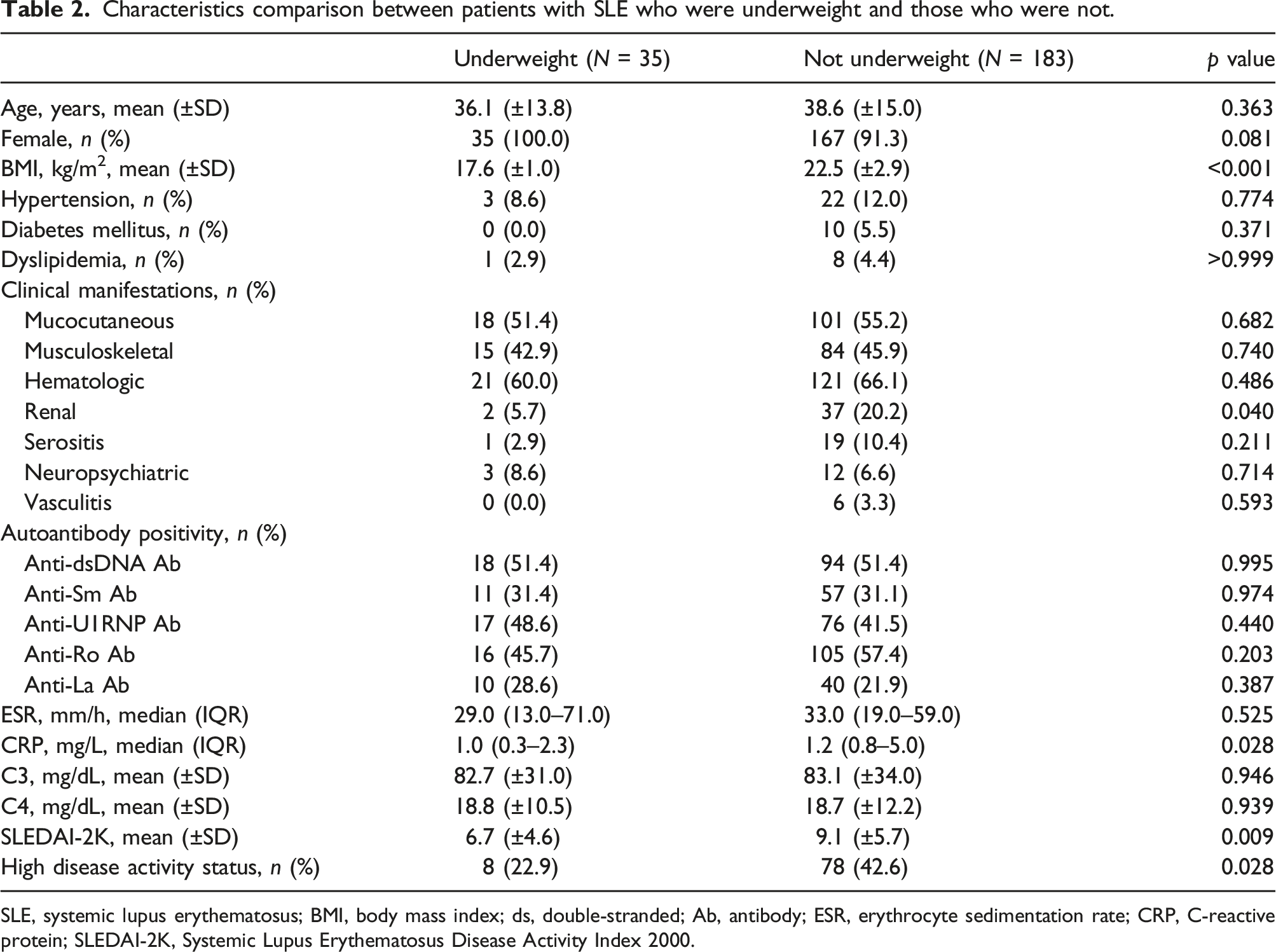
SLE, systemic lupus erythematosus; BMI, body mass index; ds, double-stranded; Ab, antibody; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000.
Comparison between patients who were underweight, normal weight, and overweight/obese
Characteristics comparison between patients with SLE who were underweight, normal weight, and overweight/obese.
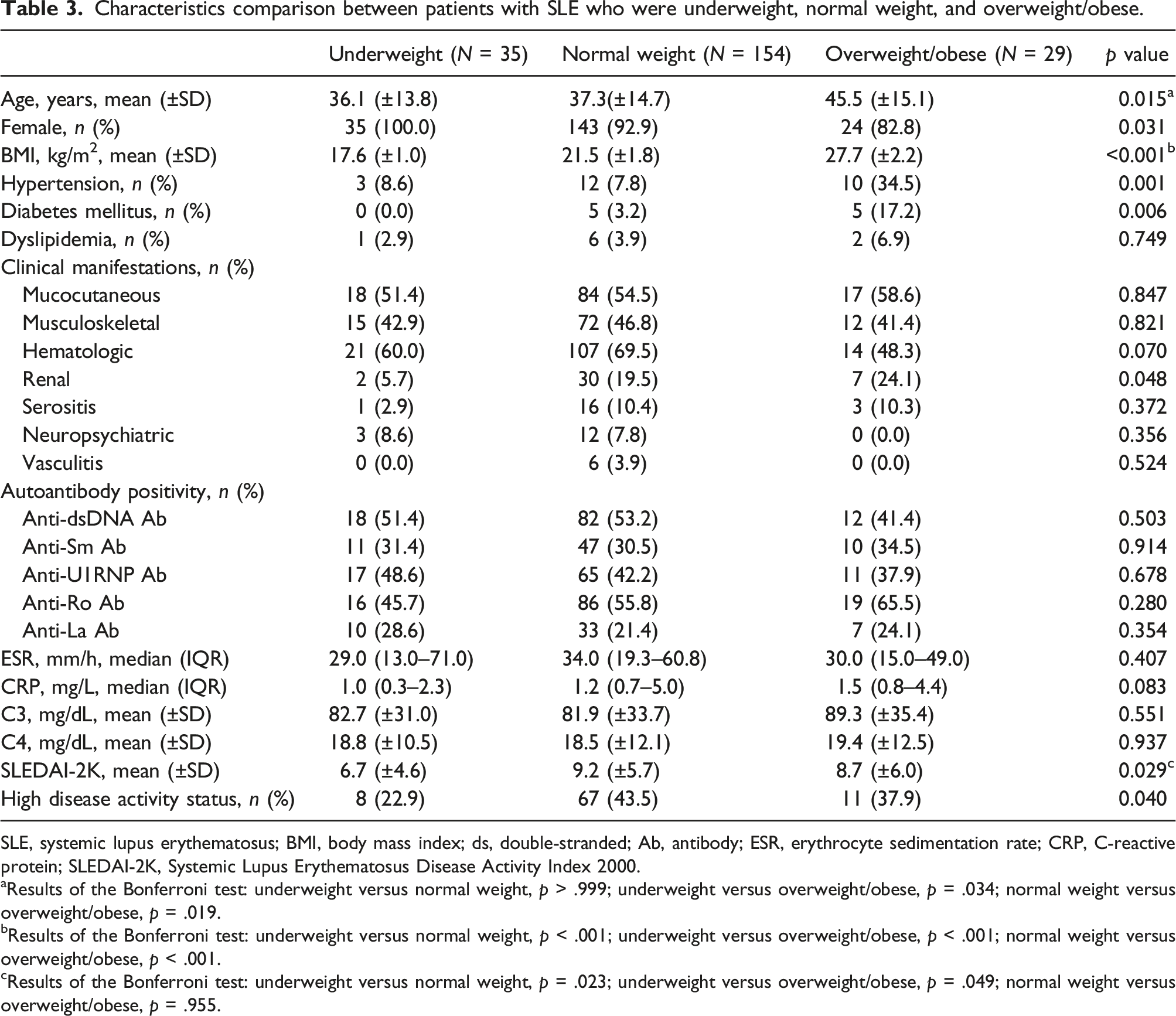
SLE, systemic lupus erythematosus; BMI, body mass index; ds, double-stranded; Ab, antibody; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000.
aResults of the Bonferroni test: underweight versus normal weight, p > .999; underweight versus overweight/obese, p = .034; normal weight versus overweight/obese, p = .019.
bResults of the Bonferroni test: underweight versus normal weight, p < .001; underweight versus overweight/obese, p < .001; normal weight versus overweight/obese, p < .001.
cResults of the Bonferroni test: underweight versus normal weight, p = .023; underweight versus overweight/obese, p = .049; normal weight versus overweight/obese, p = .955.
Association between underweight status and high disease activity status
Association between underweight and high disease activity status in patients with SLE.
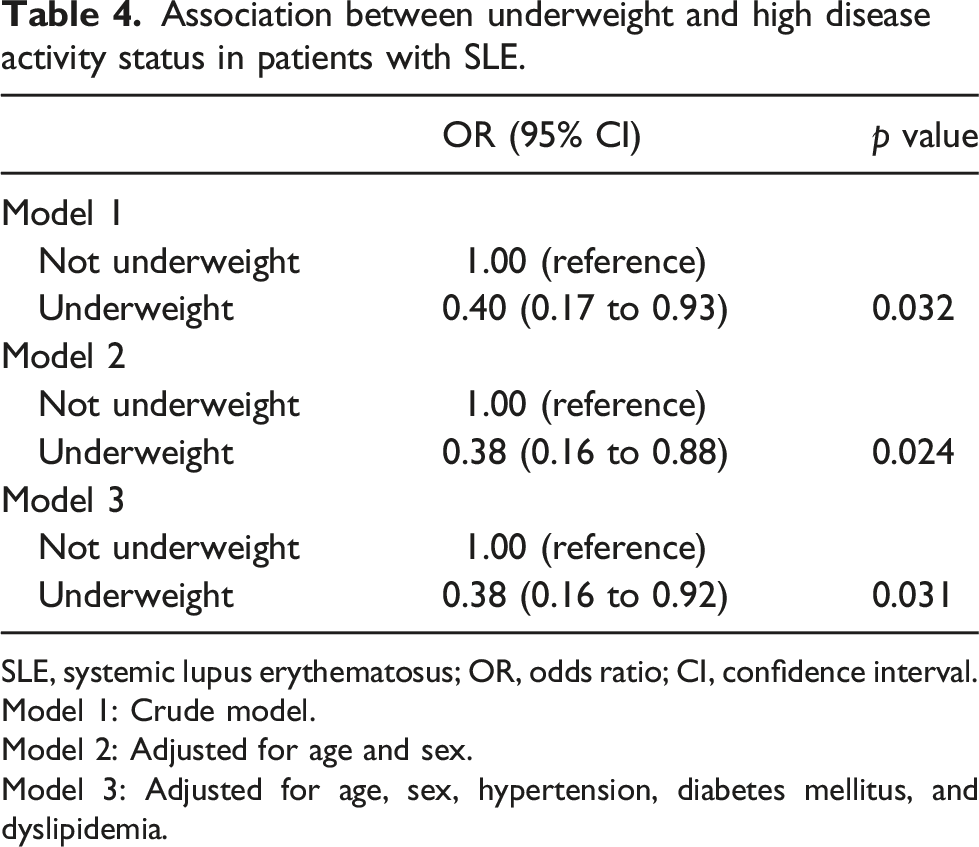
SLE, systemic lupus erythematosus; OR, odds ratio; CI, confidence interval.
Model 1: Crude model.
Model 2: Adjusted for age and sex.
Model 3: Adjusted for age, sex, hypertension, diabetes mellitus, and dyslipidemia.
Discussion
In this study, we investigated for the first time whether patients with SLE who are underweight display distinct characteristics compared with those who are not underweight. We found that those who were underweight less commonly had renal involvement and had lower SLDEAI-2K scores compared with those who were not underweight. Moreover, after adjusting for multiple covariates, being underweight, as compared with not underweight, was inversely associated with a high disease activity status of SLE.
Among the various adipokines secreted by adipose tissue are leptin and adiponectin. 4 Leptin promotes proliferation of monocytes, boosts the number of naïve T cells, and facilitates the differentiation of memory T cells into type 1 T helper cells, while suppressing type 2 T helper cells.17–19 These lead to an increase in pro-inflammatory cytokines such as interleukin (IL)-2, IL-6, IL-12, interferon-γ, and tumor necrosis factor (TNF)-α, along with a decrease in anti-inflammatory cytokines such as IL-4 and IL-10, thereby facilitating inflammation and autoimmune diseases.4,17–19 In contrast, adiponectin promotes the production of anti-inflammatory cytokines, such as IL-10 and IL-1 receptor antagonist, and reduces pro-inflammatory cytokines, such as IL-6 and TNF-α, thereby exhibiting anti-inflammatory properties.20–23 Individuals who are underweight have lower plasma leptin levels and higher plasma adiponectin levels than those who are normal weight or obese. 24 This could explain the inverse association between underweight status and high disease activity observed in our study.
In interpreting our data, it should be noted that only three patients were obese (BMI ≥30.0 kg/m2). That is, majority of the patients who were not underweight were normal weight (18.5 kg/m2 ≤ BMI <25.0 kg/m2; n = 154) or overweight (25.0 kg/m2 ≤ BMI <30.0 kg/m2; n = 26). In general, Asian populations have lower BMI than non-Asian populations. 13 The low frequency of patients who were obese in our study population could be due to the inclusion of only Asian populations. Hence, our data could not be extrapolated to those who are obese. In contrast to our observation of lower SLEDAI-2K scores in patients who were underweight than in those who were not, previous studies that included patients who were normal weight, overweight, and obese reported no difference in SLEDAI-2K scores among these weight groups.7,10 However, as patients who were underweight were not included in those studies,7,10 the results from the previous studies could not be extrapolated to patients who are underweight. Taken together with our data, the association between obesity and disease activity does not seem to apply to patients with SLE when confined to those who are not underweight (normal weight, overweight, or obese), but only applies to those who are underweight.
However, certain findings are consistent regardless of the inclusion of the patients who are underweight. A previous study has shown that CRP levels are higher in patients with SLE who are obese than in those who are overweight or normal weight. 7 Similarly, we found that CRP levels were higher in patients with SLE who were not underweight than in those who were underweight. Observational and experimental studies have also indicated an association between obesity and lupus nephritis.10,25–27 An observational study reported that lupus nephritis is more common in patients who are obese, followed by overweight and normal weight patients. 10 Experimental studies using an SLE mouse model reported that higher leptin levels 25 and lower adiponectin levels,26,27 both of which are seen in individuals with obesity, 24 are associated with more severe renal involvement. Likewise, we also found that renal involvement was more common in patients with SLE who were not underweight than in those who were. Our data further support the previous findings, indicating that the associations between obesity, CRP levels, and renal involvement also extend to patients who are underweight.
In our study, we assessed the clinical characteristics of SLE and BMI at the time of SLE diagnosis in a cross-sectional manner. Therefore, all included patients were naïve to specific SLE treatment. This is one of the strengths of our study as it excludes potential confounding by use of different medications among patients. As all patients were newly diagnosed with SLE, we focused on high disease activity status as our primary outcome of interest, rather than low disease activity status or remission, which are outcomes defined and validated for the goal of treat-to-target approach. 28 Our logistic regression analysis, adjusted for multiple covariates, revealed that underweight status was associated with a 60% lower risk of having high disease activity (adjusted OR = 0.38). Considering that high disease activity status (SLEDAI-2K score ≥10) is associated with worse longitudinal outcomes, such as higher time-adjusted disease activity, flare, glucocorticoid exposure, and damage accrual,15,16 the 60% lower risk of high disease activity status in patients who are underweight is clinically meaningful.
This study has some limitations. First, we lack data on patient-reported health-related quality of life, which makes it unclear whether patients who are underweight have better health-related quality of life than those who are not. Second, we lack data on waist circumference and were unable to analyze whether disease parameters of SLE differ according to abdominal obesity status. Third, the exact mechanism underlying the inverse association between the underweight status and high disease activity status remains elusive and needs further investigation.
In conclusion, we found that in patients with SLE who were underweight, renal involvement was less common and the SLEDAI-2K score was lower than in those who were not underweight. Moreover, underweight status was associated with a 60% lower risk of having high disease activity. These findings suggest that patients with SLE who are underweight present distinct disease characteristics compared with those who are not underweight. In terms of disease activity, weight control towards underweight status could potentially be beneficial for patients with SLE.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the faculty research grant of Yonsei University College of Medicine (6-2023-0075).
Data Availability Statement
All data generated or analyzed during this study are included in this article.