
Abstract
In response to racial inequities in systemic lupus erythematosus (SLE), we aimed to identify practical recommendations for increasing engagement and inclusion of Black adults in SLE research. We used a qualitative, interpretive description approach and recruited 30 Black adults diagnosed with SLE in Michigan to participate in semi-structured interviews. Theme development focused on what factors influenced research perceptions and how research did not meet participant needs and expectations. We developed five main themes: (1) Ethical and equitable research. Participants shared how the impacts of past and present-day racism impacted their willingness to participate in research. (2) Trusting researchers to conduct studies and translate findings to health care. Participants had concerns related to researcher intentions and expressed the importance of communicating research outcomes to participants and translating findings to health care. (3) Drug trial beneficence. When considering drug trials, several people did not consider the potential benefits worth the risk of side effects, and some said they would need to consult with their doctor before agreeing to participate. (4) Altruism. Participants explained how the desire to help others was a motivating factor for participating in research and donating biological samples. (5) Research priorities. Participants described a need for better treatments that value their overall health and well-being. Findings indicate that researchers can center the perspectives of Black people with SLE across the research life cycle—beyond a focus on adequate racial diversity among study participants.
Keywords
Introduction
Black people, including African Americans, are underrepresented in research, 1 which is a barrier to health equity. Race categorizes people based on physical features like skin tone to create a social hierarchy. 2 The first phase of the Human Genome Project demonstrated that race does not have a genetic basis, and there is more genetic variation within races than between them. 3 In American society, race represents an imperfect proxy for exposure to discrimination and environmental injustice. 4 For example, exposure to air pollution and heavy metals is worse in predominantly Black communities relative to White communities, independent of poverty level.5,6 These implications of race are important to clinical research and medicine because pharmaceutical side effects, treatment efficacy and acceptability, and disease pathophysiology can vary across social strata and depend on access to care 7 and epigenetic risk factors. 8
Underrepresentation of Black people in research on systemic lupus erythematosus (SLE) is especially a concern due to the stark racial inequities in SLE. SLE is more common among Black people relative to White people; in Michigan, 112 out of 100,000 Black adults have SLE relative to 48 out of 100,000 White adults. 9 Additionally, Black people are more likely to be impacted by SLE at a young age, 10 have comorbid conditions like nephritis, chronic renal failure, and congestive heart failure, 11 have a worse quality of life, 12 and have higher mortality rates 13 than White people. There are also notable racial inequities related to pain assessment and pain treatment, 14 which is a prominent feature of SLE. For example, healthcare providers are more likely to underestimate pain among Black people than White people due to false, racist beliefs and implicit bias.14,15
Addressing underrepresentation of Black communities in research is complex due to multiple and overlapping factors. For one, unethical research practices have exploited Black people, including the infamous Tuskegee Syphilis Trial 16 and the use of Henrietta Lack’s cells without her or her family’s consent,17,18 which continues to influence research perceptions in Black communities. In addition to these historical events, underrepresentation is also likely due to common realities of today. For example, parachute research—where researchers drop into a community to collect data that advances their careers and then leave without acknowledging the contribution of community members or reporting results back to the community 19 —is not uncommon and may contribute to community members feeling like there is no benefit to research participation. Black people are also more likely to experience discrimination and implicit bias in health care, 20 which may translate to avoiding research opportunities that occur in healthcare settings. Furthermore, Black communities are heterogenous, and racial identity intersects with other social identities in ways that can produce distinct barriers to research participation. 21 It is important to emphasize that study participation is one dimension of underrepresentation, and Black people are underrepresented in science and medicine career fields, 22 which limits their influence on the development of research questions, treatments and interventions, and study protocols.
Qualitative research encourages participants to elaborate on their personal experiences and provides an opportunity to reduce inequities in SLE. 23 Overall, the focus on Black perspectives within SLE research participation is limited in prior work. For example, studies have used racially diverse and predominantly White samples to conduct focus groups about research participation among those with SLE.24–26 These studies revealed how health status, physician involvement, logistics, altruism, and participant benefits among other factors influence perceptions of research and willingness to participate in research. More recently, a study conducted focus groups in Chicago, Illinois, and Boston, Massachusetts, with Black people who have SLE and their caregivers to identify barriers to trial participation using critical race theory. 27 In this study, motivating factors for trial participation included a desire to help others, referrals from physicians, and endorsements from trusted community members. Barriers to participation included feeling like a guinea pig, strict study exclusion criteria, concerns related to randomization, and racism in medicine and research.
There is value in extending this work to other geographic and socioeconomic contexts that may influence perceptions of research within Black communities. Additionally, study participation is one important area for addressing underrepresentation, but there are many aspects of research that would benefit from greater inclusion and engagement of Black communities who experience inequities in SLE pathology and care. This study aimed to identify opportunities to improve engagement and inclusion of Black communities across the research life cycle using a qualitative, interpretive description approach and semi-structured interviews with Black adults who have SLE in Michigan, USA. Michigan provides a unique setting for this area of research because the Black population is the largest minority racial/ethnic group in the state. 28
Participants and methods
We used an interpretive description design, 29 which is a qualitative research approach that permitted us to translate our findings into pragmatic recommendations for SLE research. The University of Michigan Institutional Review Board approved this study.
Reflexivity
Three primary preconceptions informed our study: (1) SLE incidence, morbidity, and mortality are higher among Black people relative to White people; (2) the unequal and unjust distribution of opportunities, resources, and social capital as a direct result of public policies and social norms plays a role in health inequities and the lack of diversity among research participants; and (3) symptoms like pain and fatigue among Black people may not be adequately addressed by healthcare providers due to a combination of the lack of objective measures for these symptoms, implicit bias, racism, and SLE treatment guidelines that tend to focus on markers of inflammation and immune function. Our research team included a rheumatologist (JMK) and a social epidemiologist (RSB) who interacted with members of the study population in other settings, including health care clinics and lupus-related education events.
Participants and data collection
Investigators with expertise in social determinants of health, health equity, qualitative research, rheumatology, and chronic pain developed the semi-structured interview guide for this study (Supplemental Table 1). Participants had to be adults, self-identify as Black or African American, live in Michigan, and be diagnosed with SLE. Recruitment methods included creating a study page on UMHealthResearch.org, snowball sampling, sharing study information with lupus advocacy groups (e.g., Lupus Detroit), Facebook advertising, posting study flyers in public areas, and sending emails to those who previously participated in SLE research through Michigan Medicine.
Recruitment lasted from October 2021 to July 2022. At the start of this study, we aimed to recruit between 20 and 30 participants to ensure data saturation based on earlier work. We monitored data saturation during data collection and did not end study recruitment until we determined that the data were saturated.
Research assistants with training in qualitative research and semi-structured interviewing conducted the interviews remotely via video- and teleconference software that complied with the Health Insurance Portability and Accountability Act (HIPAA). On average, interviews lasted 71 min (range = 23–153 min). Research assistants transcribed and de-identified the interviews.
Analysis
We used an inductive, thematic analysis approach. 30 First, we open-coded the transcripts. Next, we generated memos and diagrams that reflected meaningful data segments and data relationships within participants. We then created categories across participants by focusing on factors that influenced research perceptions and how research did not meet participant needs and expectations. On 9 November 2022, we presented these categories to the Community Advisory Board for Lupus Care and Research (Lupus CAB), which was composed of Black women with SLE, and other representatives of Black communities in Michigan. In the discussion that followed, Lupus CAB members agreed with our data interpretations and depictions. They also provided additional context to some of our findings, which we integrated within the results that follow.
After meeting with the Lupus CAB, we translated our categories into preliminary themes and a corresponding coding scheme. Using MAXQDA 2022 (VERBI Software, 2020), we applied the coding scheme so that each data segment in the transcripts was assigned to one or more of these themes. As we applied the coding scheme to the transcripts, we refined the themes so that they captured any data segments that conflicted or were not adequately represented in the initial coding scheme. This process resulted in five main themes that we considered final after presenting them in May 2023 to Lupus CAB members, who had no suggested changes.
Results
Five themes that describe opportunities to improve engagement and inclusion of Black communities in SLE research.
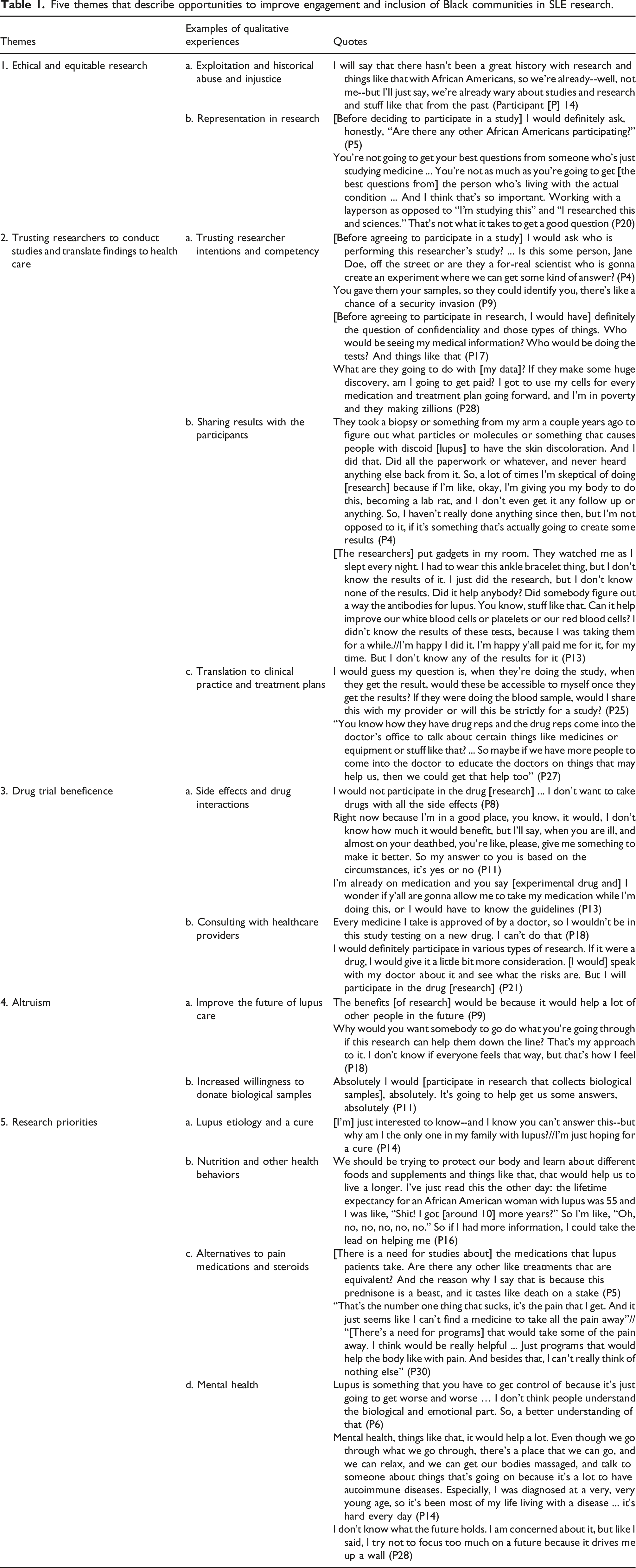
Theme 1: Ethical and equitable research
Participants shared how historical abuse and injustice influenced their perceptions of research (e.g., “I don’t want [researchers] to Henrietta Lacks me”—Participant [P] 28), and the perceptions of research among Black communities. For example, participants were concerned that they would be treated like a “lab rat” (P4 and P28) or a “guinea pig” (P1, P5, and P23). Participants also questioned whether research had meaningful benefits for Black people: [Black women] always seem to get excluded from the benefits of any program or research that they normally have so that part is always kind of concerning. But I believe if they are actually able to find a cure or some significant improvement in something then, yeah, continue to throw money at it ... otherwise you're just padding the pockets of scientists who play around in the lab and go on sabbatical (P28).
Participants interpreted the underrepresentation of Black people in research as a weakness and as evidence that the scientific community does not care about their lives or well-being. Participants emphasized the importance of Black representation when finalizing research questions, recruiting study participants, and translating research results to benefit everyone. There were also participants who did not mention inequity or unethical practices when considering their views of research. In one case, a participant expressed that randomization would prevent her from feeling like she was categorized based on social status.
Related to research equity and representation, participants talked about how they and members of their community may not have access to research opportunities due to factors like “limited resources” (P11). When we presented our preliminary findings to the Lupus CAB, members elaborated on why the Black community may have lower access to research opportunities: “In my community, a lot of the African Americans, they don’t [go to an academic research hospital]. They go to the smaller hospitals for a variety of reasons. So, from what I've heard when I'm out in the community, they're not asked to be in research studies, and if they are asked, they don't quite understand it because the person that's asking them doesn't explain or give them literature they can take back to read or share with their doctors” (Lupus CAB member).
Theme 2: Trusting researchers to conduct studies and translate findings to health care
Participants talked about trusting researchers to conduct studies and translate research findings to improve SLE care. The intentions of researchers, their qualifications, and their competency in data handling and security were influential when participants considered future research participation. One participant listed the questions that she would have before agreeing to participate in research, let alone whether she would trust the answers that researchers provide: “[Before agreeing to participate in a study that collects biological samples] I'd need to know everything that they're doing, and how they're testing it, and what the outcome would be, and what they're doing with the outcome. Whether or not they tell me the truth is a totally different story” (P1).
As a slight contrast to this, another participant said that “having a biorepository of samples is key” because it allows researchers to repurpose data for other conditions like “Raynaud’s or leukemia or something like that” (P24).
Participants also talked about the importance of receiving information about research outcomes. Participants affirmed that researchers are busy, but they want basic study progress updates and summaries of study findings sent via “phone,” “email,” “flyers,” or “letters” (P4, P14, P16, P17, P21, and P24). Participants emphasized that these updates should use terms and language that they can understand without needing expertise in medicine. One participant who provided a skin biopsy when participating in a prior study explained that the lack of follow-up after that experience made her skeptical of participating in research again.
Beyond wanting to know the results of a study for their own understanding, participants also talked about wanting to know how research will translate to better health care. As one person explained: “Are you going to research this information, have us take these medications, give you all the data and then you take it and go on and mark up the price of it to where it's unaffordable for the people who actually did the study? And now I can't access it until it’s in this generic form 300 years later and I'm no longer on the Earth. So that’s always the concern, like the intentions. Are you actually here to help people?” (P28).
During our discussion with the Lupus CAB, members elaborated on the importance of data transparency and keeping study participants informed due to the history of unethical research. For example: “It's definitely transparency of, ‘This is what we're going to do at every step’, so the patient knows what's happening, what they're going to be doing to their body. Because in addition to the Tuskegee experiment, I always think about Henrietta Lacks as well, with them taking her cells without her knowledge or permission. And now her cells are used 100 times over by these pharmaceutical companies being able to develop different cures or help in the process of researching different types of illnesses” (Lupus CAB member).
Theme 3: Drug trial beneficence
When discussing research, participants expressed caution when weighing the risks and benefits of drug trials. For example, some said being blinded to drug versus placebo group assignment would be a deterrent or feel like “Russian roulette” (P20). Several participants—including those who were willing to participate in other types of research—felt that the anticipated adverse effects of an experimental drug were not worth the risk. Participants were also worried that an experimental drug would be incompatible with their existing treatment plan, as one person described: “I don't want to throw anything off. That would just be my only concern. I just don't want it to interact with what I'm currently taking now and can make me sick or throw my numbers off” (P22).
However, participants also acknowledged that they would be willing to participate in a drug trial when experiencing a symptom flare or if they were “desperate” (P24). While not currently willing to participate in an experimental drug study, one participant said she would have when her symptoms were worse, when she was in a “flare” (P6). Others clarified that they would only consider participating in a drug trail after first seeking input from a doctor like their rheumatologist.
Theme 4: Altruism
Participants said they were interested in research because of its potential to improve SLE prevention and treatment in the “long run” (P4) and help “somebody down the line” (P16). Participants wanted to help others avoid the challenges of SLE (e.g., “I just don’t want anybody to have to go through what I went through”—P6). Participants stated that research is valuable because it can help make advancements (e.g., “We’re not going to advance anything in this world unless somebody wants to know more about something. So, you always have to have research”—P24). One participant described how she felt her participation in research could inform treatments that “specifically cater to African Americans because we do get lupus at a higher rate” (P5). Participants also described their interest in donating biological samples like blood and skin to help improve SLE care. For example, a participant shared how SLE had already taken “enough blood, sweat, and tears” (P17), so she was willing to donate biological samples for the sake of SLE research.
Theme 5: Research priorities
During the interviews, participants identified four areas of interest for future research. Participants want research that explains the cause of lupus and they want a “cure” for lupus (P1, P9, P13, P14, P16, P19, P24, and P28), although some considered that unlikely. Related to lupus etiology, one participant highlighted the need for better diagnostic testing (i.e., “not just a symptom checklist … a definitive blood test or tissue test”—P24).
Participants shared that there is a need for more mental health research because the severity of symptoms like fatigue, the worsening of symptoms, and the uncertainty associated with SLE could be mentally “overwhelming” (P28). Participants also talked about wanting to know more about how nutrition and diet affect lupus, as well as an interest in other lifestyle factors like “exercise” (P19), “yoga” (P24), and “meditation” (P29). During our discussion with the Lupus CAB, one member elaborated that behavioral interventions may increase the representation of Black people in SLE trials given the hesitancy towards experimental drugs within Black communities: “When you're talking about these drug therapies, that's a whole ‘nother can of worms. And we just came out of COVID. Folks didn't even want to get the vaccine, so you know they ain't going to do a trial. So, I don’t know the answer to that challenge. But I think that non-drug therapies could definitely be increased just by making sure that people are aware … I definitely think we can get the numbers increased on that” (Lupus CAB member).
Lastly, participants talked about their desire for alternatives to pain medications and glucocorticoids due to the side effects and inefficacy associated with these therapies. One participant described how she was motivated to do her own research about SLE due to the drawbacks of existing treatment options: “[Doctors] want to [automatically prescribe] steroids or pain meds. I just feel like there's not enough answers to the problem, like what is the root cause of it and what to do to manage it better, or what other options are there besides what they're giving us?” // “I don't like how they just automatically pin narcotics, opioids onto you because that stuff leads to long-lasting effects also. So, you're giving me this to treat a disease that's chronic and incurable. And then you're tacking on medicine that is also going to become a long-term debilitating effect for me” (P4).
Discussion
In this qualitative study, we interviewed Black adults with SLE to describe factors that influenced their research perceptions and how research did not meet their needs or expectations. We identified five themes: (1) Ethical and equitable research, (2) trusting researchers and application to health care, (3) drug trial beneficence, (4) altruism, and (5) research priorities. Previous qualitative work has characterized SLE research perceptions among Black people, with a focus on increasing clinical trial participation. 27 Our results extend these findings by illuminating the ways in which Black participants in our study wanted to be engaged and included in the development of research questions, result dissemination, and translating results to improve SLE care.
In this study, participants expressed a desire for more transparency and communication from researchers, including how a study is progressing and how their data benefited SLE care or prevention. Participants also highlighted research areas that would improve their quality of life with SLE, specifically, behavioral treatments, opioid alternatives, and a focus on mental health. These findings align with community-engaged research principles that center participant priorities before, during, and after a study. 31
Applications of this could include establishing an advisory board that consults with a research team as part of a long-term program of work. When engaging with community partners, investigators can affirm that systemic racism continues to affect the quality of care that people may receive. When talking to people about an upcoming or actively recruiting study, research teams can clarify how they will protect participants against unethical practices while openly acknowledging historical injustices like the Tuskegee Syphilis Trial. When researchers disseminate study results, scientific journals and conferences are often prioritized, but dissemination plans can include newsletters and seminars for study participants and their communities. The translation of scientific discoveries to health care can take decades. However, research institutions have the capacity to benefit people with SLE more immediately. For example, creating and sharing educational resources that support symptom management; or coordinating research efforts like recruitment and dissemination events with local organizations that offer food, financial assistance, and counseling services.
The potential for community-engaged approaches to advance health equity is well established.32–35 However, in addition to researcher commitment, these approaches require institutional investment and incentives.36,37 This is because community engagement takes added time and resources relative to conventional research models. It can also be difficult to quantify success using metrics or timetables that coincide with funding or academic promotion requirements.
Participants explained how historical events and medical racism made them distrust research and question whether research only benefits the careers and lives of researchers. At the same time, participants affirmed the need for greater representation of Black people in SLE research to reduce inequities. Our results are consistent with prior studies that describe how skepticism and mistrust impact research perceptions,24,27 including the influence of historical injustices that targeted Black communities. Researchers can implement anti-racist approaches in their work. Examples include clarifying the use of race as a social construct within analyses, valuing the input of people who are underrepresented in research (including investigators, research staff, and people with SLE), and tailoring or supplementing research activities so that people from under-resourced communities receive education and resources that support their quality of life in the short term.
Our results also contrast with prior qualitative work about research perceptions among people with SLE. In a predominantly White sample, 25 some participants were more willing to participate in research if their disease activity was stable. However, in our study, participants were less willing to participate in drug trials when their disease activity was stable and more likely to participate when experiencing a symptom flare or “desperate.” It is possible that race modifies the influence of health status on research participation and requires further study.
Our study has limitations. Black communities are not homogenous, and our findings are not generalizable to all Black adults who have SLE. The intersection of race with other social factors that we did not consider, like gender or socioeconomic status, may influence results. However, the purpose of qualitative research is not to generalize to all communities but rather to describe the perspectives of participants in detail. Study participants had a variety of prior experience with research, which is a strength of this study because it contributes to the richness of our data across multiple viewpoints. While we did not identify qualitative differences in perspectives, motivations, or concerns based on prior research participation, it may be worth considering in future research. Finally, it is possible that the results of this study, which represent self-identified Black and African American adults in Michigan, could reveal insights about improving research engagement and inclusion of other sociodemographic groups that are marginalized in society and face discrimination, racism, or colorism. However, we do not recommend that researchers extrapolate our findings to make assumptions without evidence from within specific communities.
Conclusions
We interviewed Black adults with SLE to identify opportunities for improving engagement and inclusion in SLE research. Findings indicate that there are opportunities to center the perspectives of people with SLE within research and ensure representation of Black communities across the research life cycle—beyond a focus on adequate racial diversity among study participants.
Supplemental Material
Supplemental Material - A qualitative study on opportunities to improve research engagement and inclusion of Black adults with systemic lupus erythematosus
Supplemental Material for A qualitative study on opportunities to improve research engagement and inclusion of Black adults with systemic lupus erythematosus by Johari Summerville, Nikki Farahani, Bhaavna Yalavarthi, Deena Aboul-Hassan, Sia Rajgarhia, Lillian Z Xiao, Christine Yu, Daniel J Clauw, Joanne M Kahlenberg, Melissa DeJonckheere, and Rachel S Bergmans in Lupus.
Footnotes
Acknowledgments
The authors would like to thank the community of lupus advocates in Michigan. This work would not have been possible without the contributions of study participants and members of the Community Advisory Board for Lupus Care and Research, including Crystal Ford, Kathy Garland, Sharon Harris, Shannon Hester, Anita Johnson, Tonya Jones, Toya Oglesby, and Tiffani Stokley. Board members received financial compensation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JMK reported receiving grants from Bristol Myers Squibb and Janssen; grants and personal fees from ROME Therapeutics and Ventus Therapeutics; and personal fees from AstraZeneca, Gilead, Exo Therapeutics, Lupus Therapeutics, GlaxoSmithKline, and EMD Serano outside the submitted work. RSB reported receiving personal fees from Tonix Pharmaceuticals Inc for consulting outside the submitted work. No other disclosures were reported.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this work was obtained from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) of the National Institutes of Health under awards T32-AR007080 (RSB) and K24-AR076975 (JMK). NIAMS was not involved nor placed any restrictions regarding publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.