
Abstract
Background
Systemic Lupus Erythematosus patients (SLE) are at a higher risk of cardiovascular events than the general population. This study aimed to investigate the risk perception of cardiovascular disease (CVD) and to analyze its influence factors among Chinese SLE patients.
Methods
This was a cross-sectional study. Convenience sampling was used to select 201 patients with SLE who had attended the outpatient and inpatient departments of the Department of Rheumatology and Immunology at the First Affiliated Hospital of the University of Science and Technology of China from November 2022 to March 2023. The following were used in the study: the Chinese version of the Attitudes and Beliefs about Cardiovascular Disease Risk Questionnaire, the Social Support Rating Scale, the Connor–Davidson Resilience Scale, the General Self-Efficacy Scale, the Hospital Anxiety and Depression Scale, the Health Literacy Management Scale, and sociodemographic and disease-related data.
Results
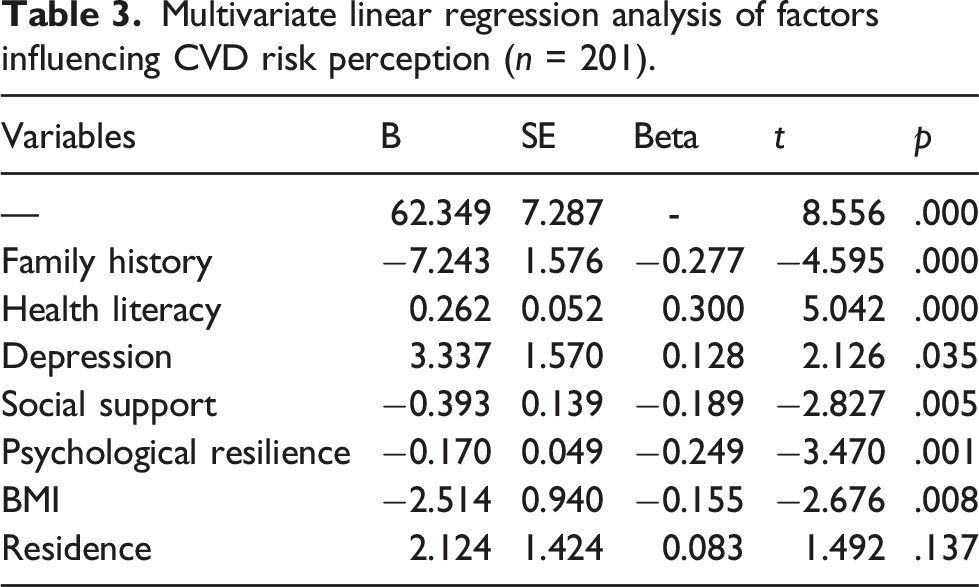
The mean (standard deviation) risk perception score of CVD patients with SLE was 57.18 ± 13.02. A Pearson correlation analysis showed that CVD risk perceptions were positively correlated with health literacy (r = 0.152, p < .05) and depression (r = 0.277, p < .05), and negatively correlated with social support (r = −0.393, p < .05) and psychological resilience (r = −0.374, p < .05). A multiple linear regression analysis showed that body mass index (BMI), family history, health literacy, depression, social support, and psychological resilience were the main factors influencing CVD risk perceptions among Chinese SLE patients (p < .05).
Conclusions
Body mass index, family history, health literacy, depression, social support, and psychological resilience influenced CVD risk perceptions among Chinese SLE patients. Healthcare workers should objectively and accurately assess the levels of CVD risk perception among SLE patients, identify the risk factors of CVD, adopt effective health risk communication strategies to help patients develop appropriate risk perceptions, and raise risk awareness to adopt active coping approaches to reduce risk.
Introduction
Systemic lupus erythematosus (SLE) is a classic chronic systemic autoimmune disease involving any organ system. It can lead to significant morbidity and even mortality.1,2 The overall global incidence of SLE ranges from 1.5 to 11 per 100,000 person-years, and the global prevalence ranges from 13 to 7713.5 per 100,000 individuals. 3 The heart is one of the organs affected by SLE, and the cardiovascular system is one of the most frequently involved organ systems. Cardiovascular disease (CVD) caused by atherosclerosis is the most common related disease. The pattern of death in SLE is distributed in a bimodal pattern, with the first peak of death mainly due to SLE activity and infection and the second primarily due to CVD caused by atherosclerosis. 4 Previous studies have shown that SLE patients tend to have a higher prevalence of CVD.5,6 SLE patients were identified to have a twofold to threefold higher risk of stroke and myocardial infarction than in the healthy population. 7 Baragetti et al. followed SLE patients and healthy people for 5 years and indirectly predicted the progression of SLE-related CVD by observing the incidence of carotid plaque in patients. They found that the incidence of carotid plaque in SLE patients was as high as 32%, while the incidence of carotid plaque in healthy people was only 4%. 8 Although the current treatment of SLE can reduce the mortality of patients due to disease activity, CVD remains the primary cause of death for SLE patients. Therefore, preventing and treating CVD in SLE patients needs attention.
Risk perception was first introduced in the study of consumer behavior by Professor Raymond Bauer of Harvard University in 1960. 9 Later, it was gradually applied to the field of health and was found to be an important influence on health behavior.10,11 However, there is no uniform definition of risk perception in the medical and health fields. Most scholars have emphasized its subjective characteristics, which was the influence of an individual’s intuitive judgment and personal experiences on the perception of risk. 12 Studies have confirmed that overestimating one’s risk of illness or health problems can lead to a chronic state of stress, while underestimating risk can discourage individuals from adopting coping behaviors and preventive measures and can also lead to unhealthy behaviors. 13 However, studies have also reported that being in a state of chronic stressful stress causes individuals to perceive society as risky and instead respond positively to threatening events. 14 Thus, there needs to be more consistency in the relationship between people’s perception of risk and their health behaviors and outcomes. It is certain that a correct assessment of risk by patients is importance to their health.
Previous studies have shown that many patients with SLE did not consider themselves to be at a high risk for development coronary artery disease. 15 Studies have also reported that women with SLE underestimate their CVD risk factors and that if healthcare providers identified and discussed CVD risk factors with them, that could increase their awareness of CVD risk and cause them to adopt risk-reducing behaviors. 16 In addition, the evidence suggested that individuals who were health literate would engage in healthier behaviors to reduce the incidence of CVD. 17 Currently, studies on the perceived risk of CVD among SLE patients have been limited to Western countries; more studies on the perceived risk of SLE in China need to be conducted. The current status of the perception of CVD risk among SLE patients and its influencing factors are unclear. Therefore, the aim of this study was to investigate the risk perception of CVD among Chinese SLE patients and to analyze the possible factors influencing them. By objectively and accurately assessing the CVD risk perceptions of SLE patients, healthcare workers can identify high-risk groups early, provide targeted health education and guidance, and provide an empirical basis for developing strategies to communicate risk.
Methods
Study design
This was a cross-sectional study conducted between November 2022 and March 2023.
Setting and participants
Two hundred and one SLE patients attending the Department of Rheumatology and Immunology outpatient and inpatient departments at the First Affiliated Hospital of the University of Science and Technology of China were recruited as study subjects. Inclusion criteria were age ≥18 years, diagnosis of SLE according to the 2019 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) classification criteria for SLE, 18 and clear consciousness. Exclusion criteria were those who had combined psychiatric or cognitive impairment, had a severe visual or hearing impairment, or had cardiovascular system disease.
Measurements
The measurement tools used in this study were the Social Support Rating Scale (SSRS), the Connor–Davidson Resilience Scale (CD-RISC), the General Self-Efficacy Scale (GSES), the Hospital Anxiety and Depression Scale (HADS), the Health Literacy Management Scale (HeLMS), the Attitudes and Beliefs about Cardiovascular Disease Risk Questionnaire (ABCD), and the demographic and disease-related data.
Social support rating scale
The scale was developed and designed by Xiao to measure the social support of individuals. 19 The scale has 10 entries and three dimensions, including the subjective support dimension, the objective support dimension, and the utilization of the social support dimension. The total score ranges from 12 to 66, with a total score of less than 45 indicating a low level of social support and more than 45 indicating higher levels of social support. In this study, the Cronbach’s alpha coefficient for this scale was 0.793.
Connor–Davidson resilience scale
The CD-RISC was developed by Connor and Davidson and revised by Yu and Zhang.20,21 It was validated for good reliability and validity in assessing the psychological resilience of subjects. Twenty-five items of the CD-RISC were used to assess the dimensions of resilience, self-improvement, and optimism. A 5-point Likert scale is used, with each item having a score of 0 to four and a range of 0 to 100, and the higher the total score, the higher the level of psychological resilience. A score of ≤60 indicates a poor level of psychological resilience, 61–69 indicates an average level of psychological resilience, 70–79 shows a good level of psychological resilience, and ≥80 indicates an excellent level of psychological resilience. In this study, the Cronbach's alpha coefficient of the scale was 0.823.
General self-efficacy
The GSES is a questionnaire that was developed by German scholars Schwarzer et al. 22 to examine the general self-efficacy of individuals. Its Chinese version was revised by Zhang et al. 23 The scale has only one dimension, consisting of 10 items, and is rated on a 4-point Likert scale (1 “not at all correct” to 4 “completely correct”) with a total score of between 10 and 40. The higher the score, the stronger the self-efficacy of the individual. In this study, the Cronbach’s alpha coefficient for this scale was 0.876.
Hospital anxiety and depression scale
Zigmond and Snaith first proposed the HADS and is primarily used to assess the level of anxiety and depression in hospitalized patients. 24 Seven of the questions on the scale relate to anxiety, and the other seven relate to depression. There are four levels of response to each question, which relate to degree, corresponding to a score of 0–3. Scores for problems of anxiety and depression are summed separately, with 0–7 referring to asymptomatic, 8–10 to suspicious, and 11–21 to being present. In this study, the Cronbach's alpha coefficient for this scale was 0.864.
Health literacy management scale
The HeLMS was developed by Professor Jordan et al. at the University of Melbourne, Australia, and a Chinese version was developed and tested for reliability by Sun et al. in China. 25 The scale has good reliability. The scale consists of four dimensions with a total of 24 entries: information acquisition ability (9 items), communication and interaction ability (9 items), willingness to improve health (4 items), and willingness to pay (2 items). Each entry has five rating options and is assigned a score of 1 to 5, respectively, with a total score of 24 to 120. Patients with a score of greater than or equal to 80% of the total score for each dimension were considered to have health literacy in this dimension, and those with a total score equal to or greater than 80% of the total score (≥96) were considered to have health literacy, and those with a total score of less than 80% of the full score (<96) were supposed to have a low level of health literacy. In this study, the Cronbach's alpha coefficient for this scale was 0.754.
The attitudes and beliefs about cardiovascular disease risk questionnaire
The ABCD scale was developed by Woringer et al. based on the Health Belief Model and the Transtheoretical Model to assess CVD risk perception. 26 It was translated and revised by Liu et al., who then produced a Chinese version with the following four dimensions containing 27 items: CVD knowledge, perception of risks, perception of benefits, and healthy eating intention.27 The dimension of knowledge was measured using a dichotomous response option (yes/no questions), while the other three dimensions were measured using a 5-point Likert scale (1 “completely disagree” to 4 “completely agree”). The total scale scores ranged from 18 to 81. The higher the score, the higher the perceived risk of CVD prevention. In this study, the Cronbach's alpha coefficient for this scale was 0.825.
In this study, we also collected the demographic data of SLE patients, including their gender, age, education, marital status, employment status, smoking history, alcohol history, home location, body mass index (BMI), duration of disease, and any family history of CVD. Family history of CVD was defined as at least one first-degree relative or at least two second-degree relatives having or currently suffering from CVD. 28
Data collection
Patients were screened strictly following the inclusion and exclusion criteria for the study subjects, and questionnaires were administered. Before conducting the study, its purpose, significance, and process were explained to the subjects. Patients were informed of their right to voluntarily fill in the questionnaire or withdraw from the study at any time. Questionnaires were administered after the patients signed the informed consent form. All questionnaires were collected on-site by uniformly trained investigators. When collecting the questionnaires, the researchers carefully checked the contents of the survey content to ensure that the questionnaires were completed with accuracy and completeness.
Statistical analysis
SPSS 23.0 was used for data processing and statistical analyses. Variables conforming to a normal distribution were expressed as mean ± standard deviation. A univariate analysis was performed using t test and ANOVA to compare differences in the perception of CVD risk between two or more independent groups of patients with different demographic information. A Pearson correlation analysis was used to analyze correlations among health literacy, depression, anxiety, social support, psychological resilience, self-efficacy, and risk perception. The statistically significant variables in the univariate analysis were used as independent variables. Risk perceptions were used as dependent variables, and multiple linear regression was used to analyze factors influencing the SLE patients’ perceptions of their risk of developing CVD. A statistically significant difference was indicated by p < .05.
Results
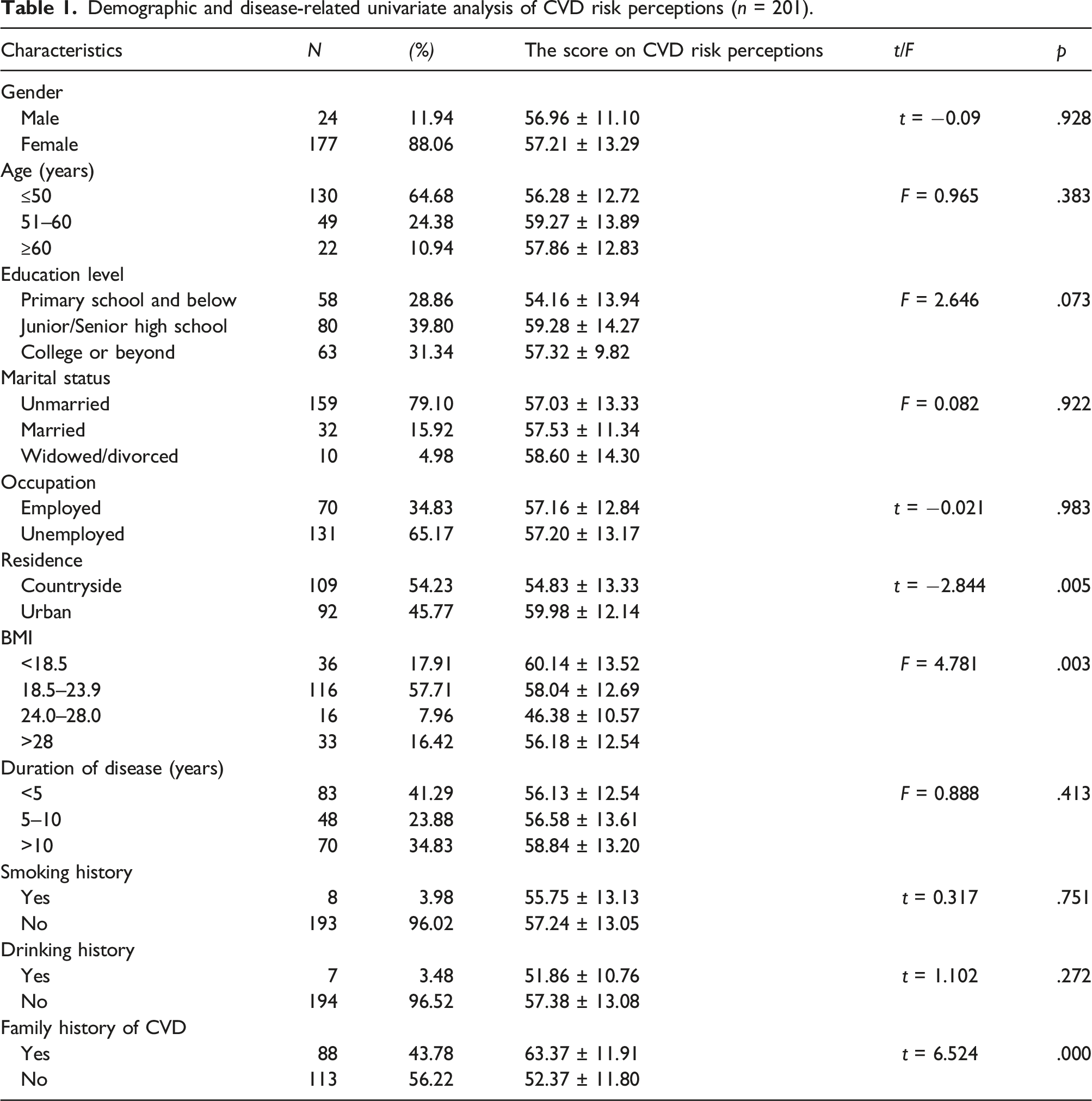
Sociodemographic and disease-related characteristics of the participants
Demographic and disease-related univariate analysis of CVD risk perceptions (n = 201).
The relationships between CVD risk perception and health literacy, depression, social support, and psychological resilience in Chinese patients with SLE.
Correlation analysis of CVD risk perceptions (n = 201).
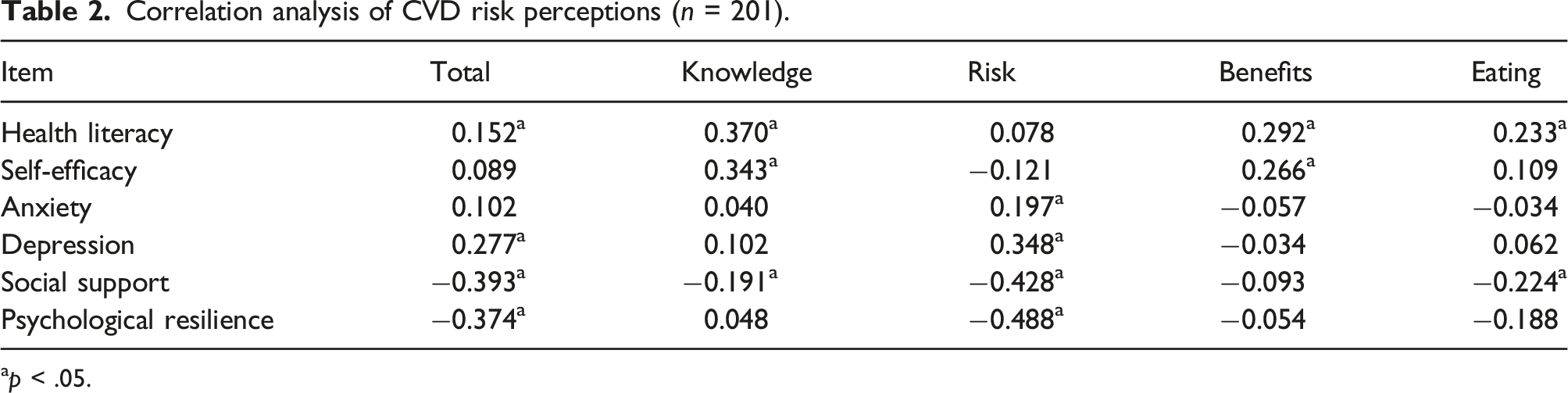
ap < .05.
Factors influencing perceptions of cardiovascular disease risk among systemic lupus erythematosus patients
Multivariate linear regression analysis of factors influencing CVD risk perception (n = 201).
Discussion
Various studies have confirmed that patients with SLE present with a higher incidence of cardiovascular events, while CVD is the leading cause of death in SLE patients.7,8 In addition, an incorrect perception of risk by patients can adversely affect an individual’s health. 13 Therefore, accurately measuring CVD risk perceptions may provide a basis for future efforts to identify high-risk individuals early in the clinical process, and improve patient awareness of the risk of developing CVD and the need to adopt risk-reducing behaviors. This study aimed to investigate the risk perception of CVD and to analyze its influence factors among Chinese SLE patients.
The results of the present study were similar to those of previous studies. Overall, the CVD risk perception of SLE patients is not very high. Studies have shown that the female SLE patients underestimated their risk factors for CVD. 16 Studies have also reported that there was a significant association between healthcare provider counseling and the perceived risk of CVD occurring in SLE patients and that CVD counseling by healthcare providers not only improved SLE patients' awareness of CVD risk factors but also had a significant impact on their self-perception of their CVD risk status. 29 This study analyzed the influencing factors of risk perception in SLE patients.
The results of this study showed that BMI was one of the factors influencing CVD risk perceptions among SLE patients. Boo et al. evaluated the effect of cardiovascular risk factors on CVD risk perceptions among Korean patients with rheumatoid arthritis and showed that obesity did not affect risk perceptions. 30 This was not consistent with the findings of this paper. An analysis of the reasons for the difference may be related to differences in the study population and types of diseases. The mortality, incidence, and prevalence rates of CVD continue to increase globally. 31 Obesity directly contributes to the development of CVD. 32 BMI was consistently positively associated with CVD. 33 This study showed that the level of CVD risk perception was lower in patients with a high BMI, and other studies have confirmed that the level of knowledge of CVD is a predictor of CVD risk perception. 34 Therefore, healthcare workers should make SLE patients more knowledgeable about risk factors for CVD occurrence and the need to maintain BMI at normal levels. In addition, the family history of CVD was another influencing factor for CVD risk perception. As is known to all, a family history of myocardial infarction and stroke increases the risk of CVD. 35 Studies have reported that a parental history of CVD significantly increased the likelihood that patients would perceive themselves to be at a high risk of developing CVD. 30 Other studies have also confirmed that patients with a family history of CVD had a higher perception of CVD risk. 36 These studies are consistent with the results of this study. This may be due to the fact that patients with a family history can receive information and witness complications from relatives, thus they had more aware of the disease and potential role of genetics. 37
Not surprisingly, health literacy was another influencing factor for CVD risk perception. Health literacy refers to an individual’s ability to access, understand, and process basic health information and services and to make sound health-related decisions. 38 Tang et al. found a positive correlation between health literacy and perceptions of the risk of recurrence among first-episode ischemic stroke patients, similar to the results of our study. 39 Patients with low health literacy may lack the knowledge to make informed health-related choices and control risk factors. 40 However, risk perception is based on the patient's perception of the disease and a certain level of knowledge about it. 41 Therefore, healthcare workers need to accurately identify patients with low health literacy, prompt them to acquire scientific knowledge about disease risks, improve risk perception awareness, and adopt positive health behaviors to prevent or even delay the occurrence of CVD.
Risk perception is a complex concept influenced by sociocultural factors, disease risk factors, and emotions. 42 This study found that the factors influencing CVD risk perceptions among SLE patients also included psychological resilience, social support, and depression. First, psychological resilience was a protective factor in the patient’s risk perception. A study showed that high levels of psychological resilience might have a protective effect on the patient's condition, which was consistent with the results of the present study. 43 Psychological resilience can help patients face their condition with a positive attitude and give them the ability to evaluate the level of risk accurately. 44 Second, social support was also a protective factor in the patient's risk perception. The results of this study are consistent with those of previous studies.45 Social support reflects the closeness of personal and social ties. 46 A high degree of social support for patients indicates that they can receive material, informational, and emotional help and support from various sources and channels. Therefore, when faced with multiple risk factors, patients will be less likely to experience adverse psychological reactions such as worry, tension, and anxiety, and their risk perception level is relatively low. Third, in our study, we found a positive association between the CVD risk perception of SLE patients and depression. This is similar to the results of previous studies.47,48 Studies have confirmed that mood affects people's risk perceptions, with people perceiving relatively less risk when in a positive mood and more risk when in a negative mood. 49 Therefore, healthcare workers should identify depressed patients early and enhance attention and intervention for psychological problems.
There are several limitations. First, the sample size was small, and it was a single-center cross-sectional study. Second, the impact factors in this study needed to be more comprehensive and remain to be explored. Future multicenter longitudinal studies will be conducted to provide a theoretical basis for targeted clinical interventions. Third, patient data were collected anonymously, and we no longer have more channels to obtain laboratory test data from patients, so we will consider this issue in future research.
Conclusion
In conclusion, our study showed that BMI, family history, health literacy, depression, social support, and psychological resilience were factors influencing perceptions of CVD risk among SLE patients. To play a crucial role in ensuring that patients maintain a proper lifestyle and pay attention to their daily diet, sleep, and exercise, healthcare providers must train and counsel SLE patients about CVD. In addition, it is essential to accurately assess the CVD risk perceptions of SLE patients, improve their awareness of CVD, increase their levels of health literacy, social support, and psychological resilience, place more emphasis on addressing psychological problems, improve depression, prevent and delay the occurrence of CVD, and improve quality of life to improve a poor prognosis.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank all participants. The authors also thank all of the nurses in the Department of Rheumatology and Immunology at the First Affiliated Hospital of the University of Science and Technology of China for their help in recruiting participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Anhui Province (1808085MH298).