
Abstract
Objectives
Systemic lupus erythematosus (SLE) with a high morbidity rate (7% in general and 325/100.000 in reproductive period) was known as “the mother of autoimmune diseases.” But healthcare providers hadn't reliable scales to measure the effectiveness of interventions to improve reproductive health. Women with systemic lupus erythematosus (SLE) express concern about a significant gap in their reproductive and sexual health during medical care due to the lack of a specific scale to measure this concept. This study developed psychometrically specific scale to evaluate this concept in Iranian women.
Methods
The study utilized a sequential-exploratory mixed-methods design, wherein the concept of reproductive health was clarified during the qualitative phase using conventional content analysis (inductive-deductive) to create a pool of RHASLE (Reproductive Health Assessment in SLE) items. During the psychometric process, the face, content, and construct validities of the RHASLE were checked with 650 individuals (320 using exploratory factor analysis [EFA] and 330 using confirmatory factor analysis [CFA]) through interviews and completion of the questionnaire. Convergent and divergent validities were then checked, and the reliability was assessed through stability and internal consistency. Finally, the measurement error, responsiveness, and interpretability of the scale were evaluated and confirmed.
Results
The study's findings revealed that the RHASLE consisted of 5 factors (33 items): physical-psychological disorder (13 items), relaxing feeling (6 items), spirituality (3 items), high-risk pregnancies (5 items), and sexual satisfaction (6 items). These factors explained a total of 99.97% of the variance in the concept of reproductive health. Confirmatory factor analysis confirmed the good model fit, and its validity and reliability were deemed acceptable.
Conclusion
The RHASLE consisted of 27 items with high internal consistency, stability, responsiveness, and interpretability. That was able to get approval of Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN) checklist. Based on the results, RHASLE is a valid and reliable multidimensional scale that encompasses various aspects of reproductive health (physical, sexual, psychological, social, and spiritual).
Statement of significance
Introduction
Systemic lupus erythematosus (SLE) is a chronic, complex autoimmune disease that affects multiple organs. The incidence of SLE has increased tenfold in developed countries over the past 50 years.1–3 Given its similar ethnic makeup to European countries, Iran is an appropriate setting to study the features of SLE, where the mean age of SLE onset is 24 years. 4 SLE has a high morbidity rate of 7%, which is why it is referred to as “the mother of autoimmune diseases.”3–5
Women are nine times more likely to be affected than men, especially during their reproductive years.1–3 During pregnancy, lupus can improve, remain unchanged, or worsen, with a risk of complications. SLE negatively affects physical performance and disease activity, leading to depression and decreased self-confidence, which increases anxiety, worry, and depression in affected women by more than 60% (5%–80%).2,6–9
Persistent pain and fatigue associated with lupus can make it challenging to manage the emotional and physical aspects of sexual relations, leading to sexual dysfunction.4,10
Reproductive health is defined as a state of complete physical, mental, and social well-being in all matters related to the reproductive system. 11 However, more than 60% of women with lupus report concerns about their reproductive health that are not addressed during medical visits and care. 8
There is a significant gap in reproductive health care for women with lupus, and there is a need for healthcare providers to have access to appropriate and reliable scales to measure the effectiveness of interventions to improve the quality of care. Therefore, the development of a scale to measure reproductive health in women with lupus is necessary.
Methods
This study used a sequential-exploratory mixed-methods design that involved two phases: (1) a qualitative phase to generate items for the RHASLE (Reproductive Health Assessment in Systemic Lupus Erythematosus) and (2) a quantitative phase to assess the scale’s psychometric properties.
First phase: Item generation
During the qualitative phase, the study used in-depth interviews to extract reproductive and sexual experiences of married women (or those with a history of cohabitation) with SLE.
Participants
During the qualitative phase of the study, 19 married women with SLE aged 15–49 years were purposefully selected using a maximum variation sampling from the Iran Lupus Association and the Rheumatology Center of Shariati Hospital in Tehran. All participants were sexually active and at least 12 months had passed since their diagnosis by the rheumatology center. Also, sampling in all steps was random by convenient sampling. Data collection was conducted from January 2018 to January 2020 for the first four steps and from May 2022 to January 2023 for the fifth and sixth steps (so it took 33 months). Participants provided verbal and written consent to participate in the study and have their voices recorded. A total of 27 semi-structured, in-depth interviews were conducted with 19 participants, lasting between 60 and 90 min (8 of whom were interviewed twice). The audio files were transcribed and reviewed several times to gain a deep understanding of the women's feelings and experiences. The data were analyzed using conventional content analysis in eight steps based on the approach of Zhang and Wildemuth (2016), 12 as well as MAXQDA10.
To enhance the reliability of the qualitative research, the study applied the five criteria suggested by Polit (2020): credibility, dependability, confirmability, transferability, and authenticity. 13
The research team used a deductive-inductive approach to design the research tool. Overlapping items were removed and merged based on the research team's opinion. The codes extracted from the qualitative study were inductively transformed into items, which resulted in 59 items. To complete the items, a deductive approach was used by reviewing sites and databases to search by Persian and English keywords for available tools without a time limit. A total of 13 items were adapted from other studies based on existing questionnaires (general and specific quality of life), resulting in a pool of 72 items. Overlapping and additional items were merged or separated during two revisions by the research team. This led to the design of the initial version of RHASLE with 52 items, which then entered the psychometric phase.
Second phase: Item reduction
The psychometric properties of the RHASLE were evaluated in a six-stage process based on the classical theory of validity and reliability. The sample size varied across different stages and was provided separately for each step. A detailed overview of the development and evaluation of the RHASLE is shown in Figure 1. Production phases of RHASLE scale.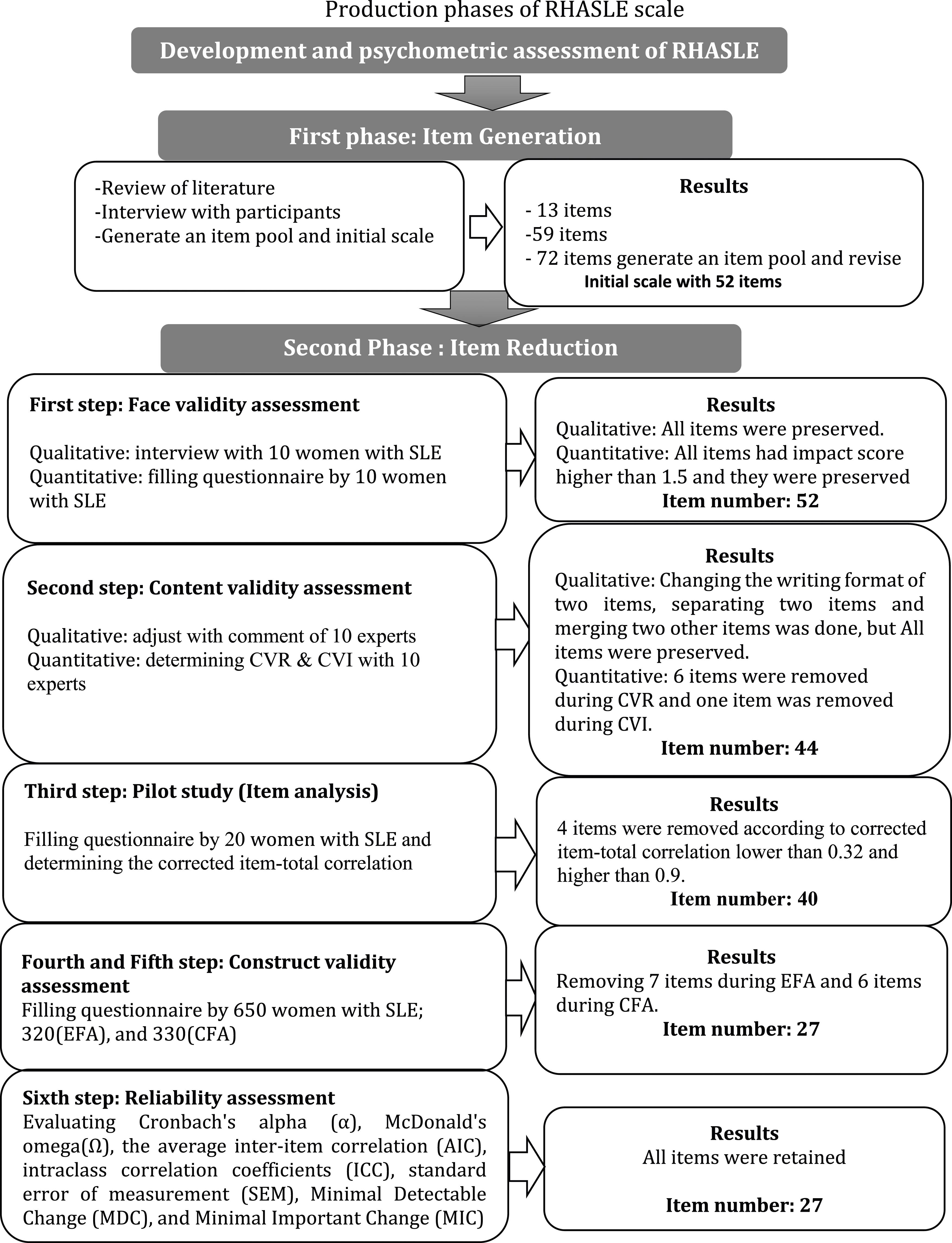
First step: Face validity assessment
To evaluate the face validity of the RHASLE, both qualitative and quantitative methods were used.
Qualitative face validity assessment
Ten married women with SLE were asked to answer the items and provide feedback on the level of difficulty, appropriateness, relevance, and ambiguity of the items. The time required to complete the questionnaire was also calculated. The scale was revised based on the women's opinions.
Quantitative face validity assessment
The item impact index was utilized to eliminate inappropriate phrases and determine the comprehensibility of each phrase. Ten women with lupus who did not participate in the qualitative face validity stage were included in the study. The scores were rated on a 5-point Likert scale ranging from 1 (non-comprehensible) to 5 (completely comprehensible). The researcher calculated the impact score of each item separately using the following formula: Frequency (%) × Comprehension. Where the frequency represents the number of people who gave a score of 4 and 5 to each item, and the comprehension represents the ability to understand the item based on the Likert scale. If the impact score exceeded 1.5, the phrase was considered suitable for further analysis. 14
Second step: Content validity assessment
The content validity of the RHASLE was evaluated using both qualitative and quantitative methods.
Qualitative content validity assessment
Ten researchers and experts (five specialists in reproductive health specialists and gynecologist and five rheumatologists) were asked to review the scale and provide expert opinions on grammar, proper wording, appropriate item allocation, and grading. 15 The scale was revised based on their feedback.
Quantitative content validity assessment
Two weeks later, the content validity index (CVI) was evaluated to assess the simplicity, relevance, and clarity of the RHASLE items. However, CVI alone cannot evaluate the chance agreement. Therefore, the Kappa statistic corrected with K* was used, as recommended by Polit and Beck (2006). K* provides an index of chance agreement between raters regarding the relevance of the item. To calculate K*, the probability of chance agreement was first calculated using the following formula: Pc = [N!/(A! (N-A)!)] × 0.5N, where N is the total number of raters and A is the number of agreements regarding the item relevance. Ten experts evaluated the simplicity, relevance, and clarity of each item of the RHASLE using a 4-point Likert scale (1 = not relevant, 2 = somewhat relevant, 3 = relevant, 4 = completely relevant). The item-CVI score (I-CVI) was calculated by dividing the number of experts who gave that item a score of 3 or 4 by the total number of experts. K* was then calculated using the following formula: K* = ((I-CVI) - PC)/(1 - PC). According to Polit and Beck view, a minimum of three raters is required for Kappa calculation. In this study, 10 raters were involved, and a Kappa value greater than 0.74 was considered good and acceptable. Moreover, the optimal criterion for I-CVI content validity was a numerical value of 0.78 or higher. For scale-CVI (average I-CVIs for the entire scale), a score of 0.90 or higher was favorable. 16
Third step: Pilot study (item analysis)
Twenty married women with SLE were asked to review the instrument for ease of completion, comprehensibility, clarity, and acceptability. The instrument was revised based on their feedback until no further problems were identified. Overall, the RHASLE was found to be easy to complete, taking approximately 15 min. Item analysis was conducted to identify potential problems with individual items or the scale as a whole. Items with correlation coefficients less than 0.32 or greater than 0.9 were removed. 17
Fourth and fifth steps: Construct and structural validity assessment
Exploratory factor analysis (EFA)
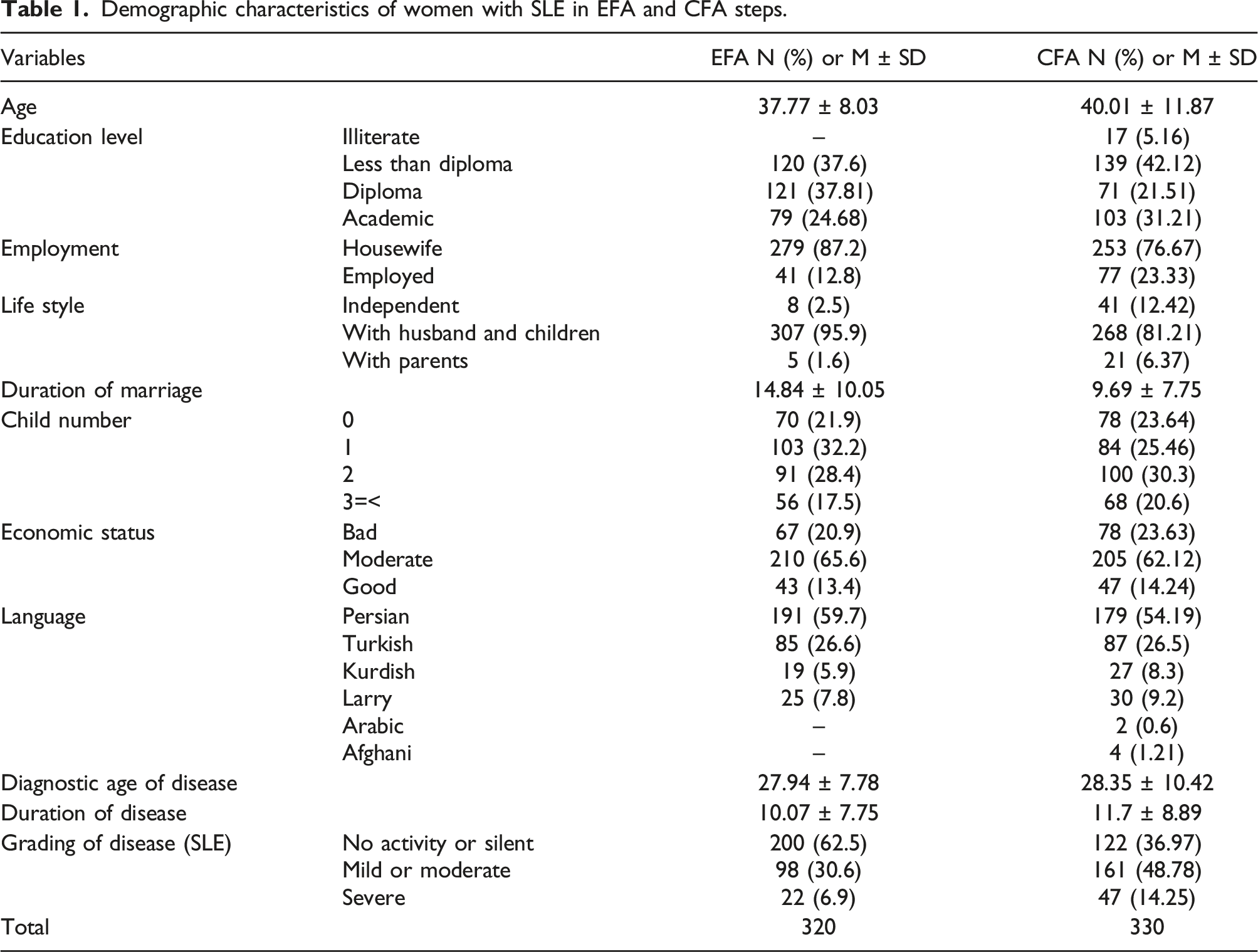
The construct validity of the RHASLE was evaluated using maximum likelihood in factor analysis, followed by varimax rotation using the Psycho package in R-Studio software. To perform this step, between 3 and 10 women were needed for each item.18,19 A total of 320 married women with SLE completed the instrument on a 5-point Likert scale ranging from “always” to “never”. The questionnaires used in this stage included two parts: a demographic questionnaire (age, education, occupation, language, length of marriage, living situation, number of children, duration of illness, and age of diagnosis) and disease activity status (according to the SLEDAI). The RHASLE consisted of 40 items aimed at extracting reproductive health factors of married women with SLE based on a 5-point Likert scale (ranging from “always” to “never”). The Kaiser–Meyer–Olkin (KMO) and Bartlett's tests were used to assess the appropriate number of studied samples and the factor analysis model. An excellent KMO value was interpreted as being above 0.9. 20 To extract the factors, Horn’s parallel analysis and exploratory graph analysis (EGA) were performed using R-Studio software. Horn's parallel analysis has been found to provide consistent results in determining the exact number of factors and the main scale. This method generates eigenvalues by generating a random matrix of the same rank and variable type as our data set, which takes into account the sampling error inherent in the data set. Then, the real values of the matrix were compared with the randomly generated matrix. The exact number of factors was determined by counting the number of components that account for more variance than the derived components using random data. 20 Items with absolute loading values above 0.3 and item commonalities above 0.2 were considered appropriate. 21
Confirmatory factor analysis (CFA)
The factor structure for the RHASLE (33 items) was analyzed using maximum likelihood (EFA) in Amos 24. The sample size for this stage was selected based on the ratio of 5–20 samples per observed manifest and latent variable, following the guidelines of Hair and Black (2014). 22 A total of 10 samples for each item were selected from the 33 items of the RHASLE, and a total of 330 married women with SLE were included in the study using a convenience sampling method. 23
Most common goodness-of-fit indices were included: chi-square (X2) test, chi-square/degree-of-freedom ratio (X2/df) < 3, Comparative Fit Index (CFI) > 0.90, Incremental Fit Index (IFI) > 0.90, Tucker‐Lewis Index (TLI) > 0.90, Parsimonious Normed Fit Index (PNFI) > 0.50, Parsimonious Comparative Fit Index (PCFI) > 0.50, and root mean square error of approximation (RMSEA) < 0.08 using AMOS24.21,22
Convergent and divergent validity
Convergent and divergent validity of the scale were evaluated by AMOS24 software using the average variance extracted (AVE), maximum shared squared variance (MSV), and composite reliability (CR).19,23
To establish convergent validity, the average variance extracted (AVE) should be greater than 0.5 or less than the composite reliability (CR), and the maximum shared variance (MSV) should be less than the AVE [33]. To establish divergent validity, the Heterotrait–Monotrait Ratio (HTMT) matrix was used, following the more recent approach by Heseler. To achieve divergent validity, all values in the HTMT matrix should be less than 0.85. 24
Sixth step: Reliability assessment
Reliability was evaluated using internal consistency, stability, and absolute reliability approaches, as well as AMOS24 software. Internal consistency was assessed using Cronbach's alpha (α), McDonald's omega (Ω), and average inter-item correlation (AIC). A value of α or Ω greater than 0.7 and an AIC value between 0.2 and 0.4 were considered acceptable for internal consistency. To assess stability, intraclass correlation coefficients (ICCs) of the RHASLE were calculated using a two-way random-effect model. The retest method was used for 20 women with lupus with a 2-week time interval. 19 An ICC value greater than 0.8 was considered acceptable for stability. Additionally, absolute reliability was evaluated using the standard error of measurement (SEM) calculated with SEM = SD Pooled × √(1-ICC). 19
To evaluate responsiveness, the minimal detectable change (MDC) was calculated using MDC95% = 1.96 × SEM × √0.2, and the minimal important change (MIC) was calculated using MIC = 0.5 × ∆SD. To interpret MIC, the limit of agreement (LOA) was calculated using LOA = d ± 1.96 × SD difference. If the MIC is smaller than the MDC or does not fall within the LOA, the scale will be considered responsive. Interpretability was assessed by determining the ceiling and floor effects and MDC. 17
Multivariate normality and outliers
The normal distribution of the data was evaluated in two ways: univariate and multivariate distribution. Univariate normal distribution was assessed using skewness (±3) and kurtosis (±7), while multivariate normal distribution was assessed using the Mardia’s coefficient, which should be less than 8. Outlier data were evaluated through two methods: univariate and multivariate outliers. Univariate outliers were evaluated using distribution charts, while multivariate outliers were evaluated using the Mahalanobis p < .001. 20
Ethical considerations
The study was conducted as part of a PhD thesis on reproductive health and was approved by the Ethics Committee of Tehran University of Medical Sciences (code of ethics: IR.TUMS.96.9513151002). The research was conducted in accordance with the principles of the Declaration of Helsinki. Participants were informed of the study's objectives and assured that their information would be kept confidential, and their unwillingness to participate would not affect their care.
Results
First phase: Item generation
During the qualitative analysis of interviews, 1050 primary codes were obtained from meaning units, which were repeatedly analyzed, deleted, and integrated. As a result, 930 codes were removed, and the remaining 120 codes were divided into 14 subcategories and 6 categories: physical suffering, psychological stress, challenging fertility, adaptation to illness, need for a supporter, and spirituality. These categories were used to design 59 items. Additionally, 13 items were adapted from existing texts and questionnaires, resulting in a pool of 72 items. During two revision stages, the research team merged or separated overlapping and additional items, resulting in 52 items being selected for RHASLE.
Second phase: Item reduction
In the face validity step, all item scores were above 1.5 and were considered suitable. In the qualitative content validity step, two negative items were changed to positive ones, two items were separated, and two other items were merged based on the expert panel's opinions, while the number of items remained constant. In the quantitative content validity step, six items were removed due to a CVR less than 0.4. One item with a score of 0.6 was removed based on CVI, and one item with a score of 0.49 was removed based on Kappa. Thus, the scale entered the initial reliability step with 44 items.
Third step: Pilot study (item analysis)
In this step, four items (3, 7, 13, and 32) were removed due to not meeting the desired criteria, resulting in the instrument entering the construct validity stage with 40 items. The Cronbach alpha coefficient of the instrument was 0.897.
Fourth and fifth steps: Construct validity assessment
Sociodemographic profile of participants
Demographic characteristics of women with SLE in EFA and CFA steps.
Results of EFA on the five factors of RHASLE (N = 320).
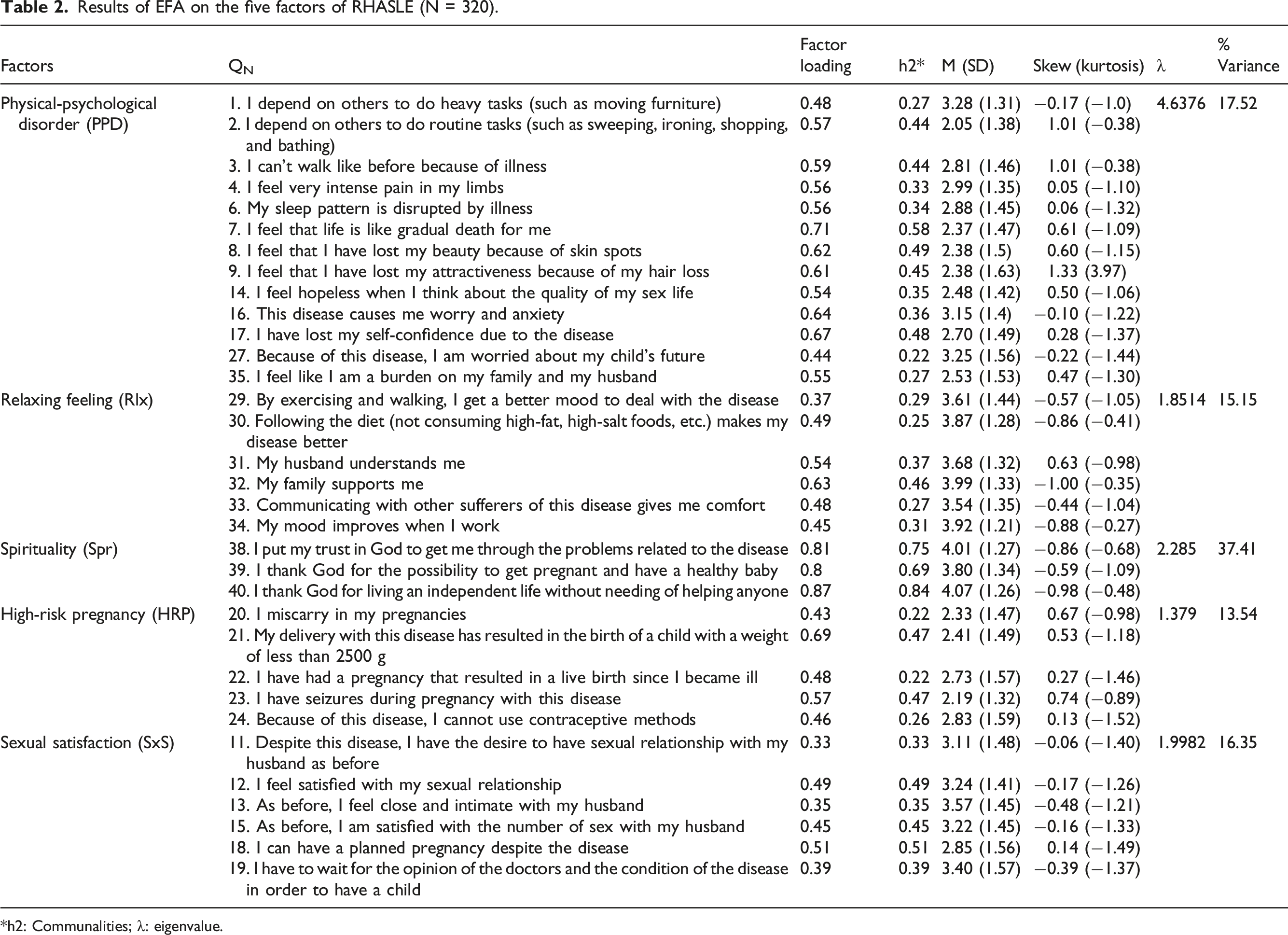
*h2: Communalities; λ: eigenvalue.
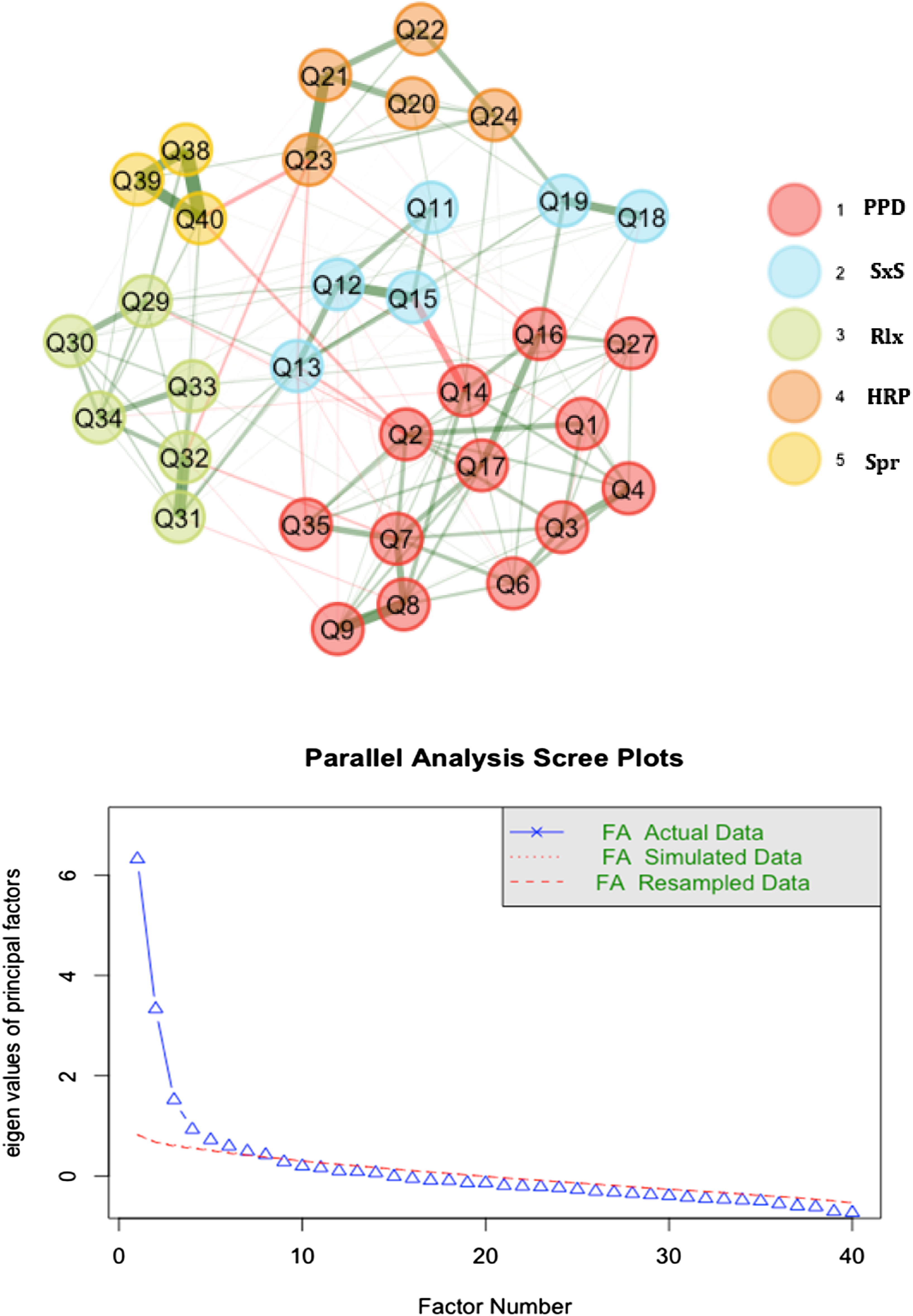
Exploratory graph analysis and parallel analysis scree plots.
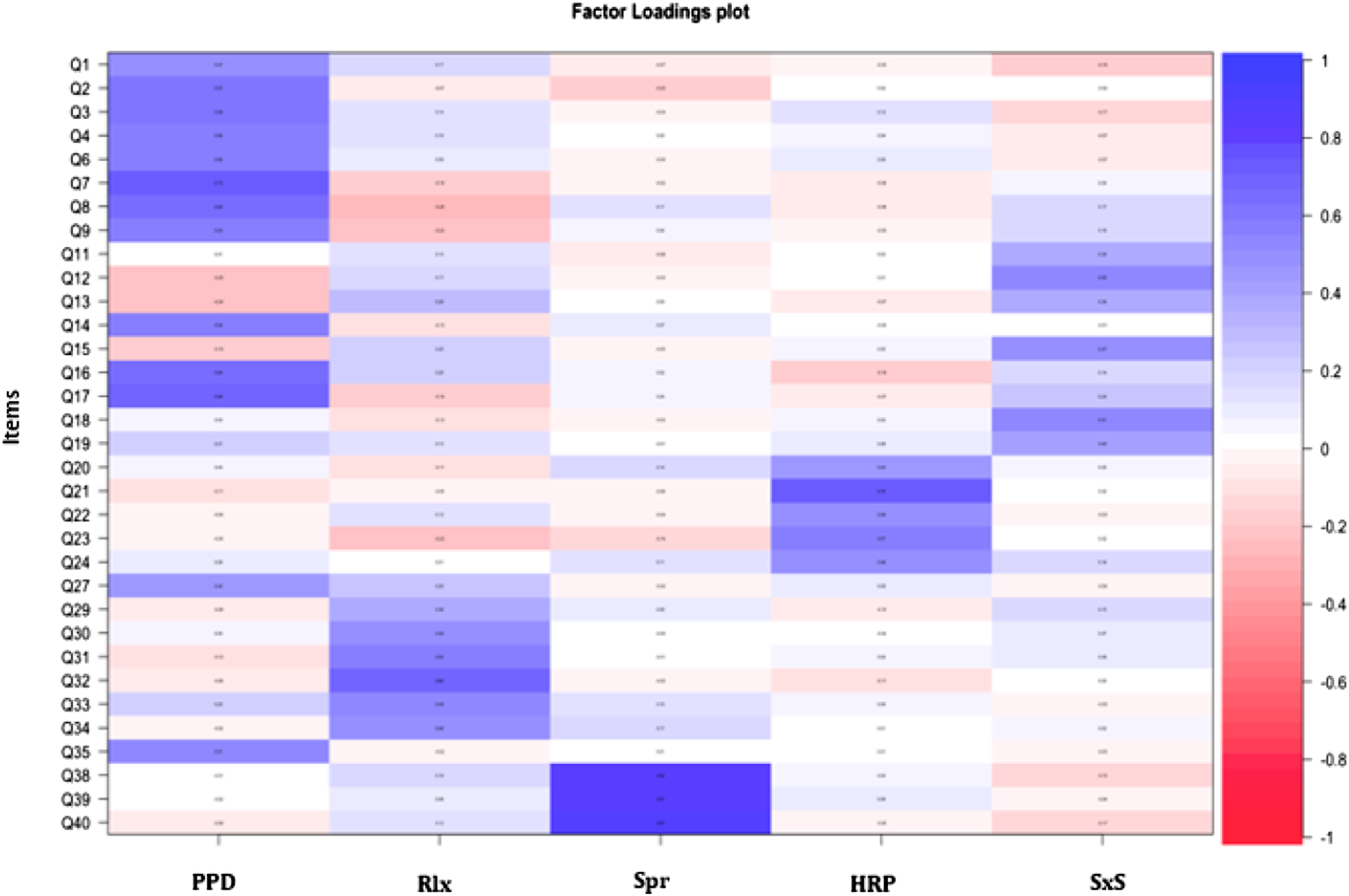
Loading strength of items in factors.
The construct validity of the model was evaluated through CFA, and the fit indices of the model were found to be within the acceptable range, confirming the model (Figure 4 and Supplemental Table 1). The scale factors were found to be convergent, and the results of AVE, MSV, and CR analyses were used for convergent and discriminant validity. All items had discriminant validity, and the results of HTMT showed no warnings for discriminant validity. First-order CFA of RHASLE scale (n = 330).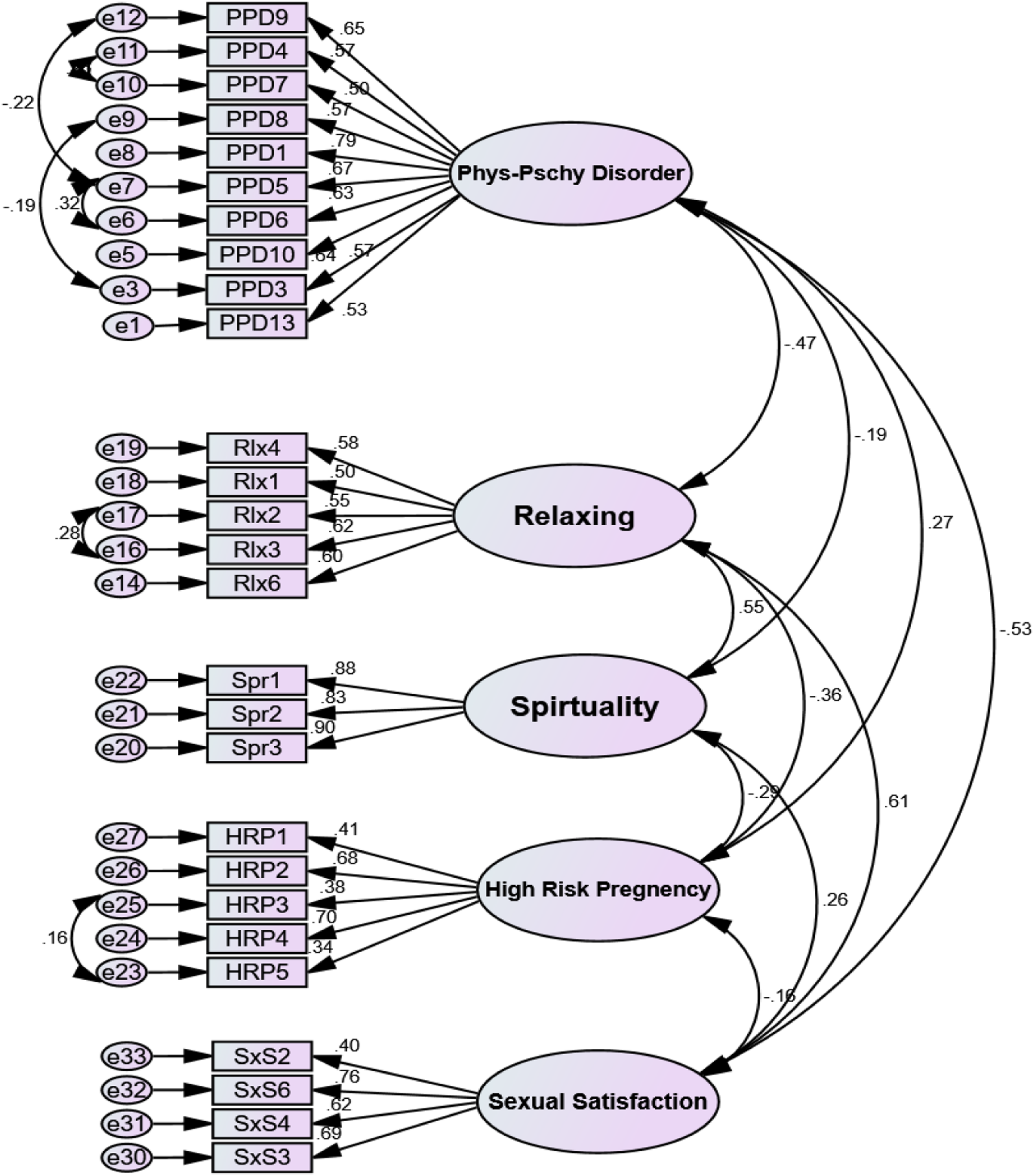
Sixth step: Reliability assessment
The internal consistency of the scale was found to be acceptable based on Cronbach's alpha, McDonald's omega, and AIC results for the five factors, which were all above 0.6, 0.7, and between 0.2 and 0.4, respectively. The scale was also found to be reliable based on CR and maximum H (Max H) reliability results in Supplemental Tables 2 and 3.
The reliability of the scale was strong based on the overall ICC of 0.878 (95% CI: 0.424–0.961) (Supplemental Table 4). The absolute reliability of the scale, based on SEM results, was found to be 4.88, indicating that the scale score changed by 4.88. MDC results indicated that MIC of the scale was responsive. Additionally, the ceiling and floor effects were evaluated for the entire tool and each of the factors. The results showed that the items were free from these effects, indicating that the scale had interpretability (Supplemental Table 4). Also, scoring of scale is presented in Supplemental Table 5. Instruction of RHASLE scoring showed as supplemental Table 6.
Specifically, the ceiling effect for the whole instrument was 14.53%, while the floor effect was 12.25%. The percentages of the factors were as follows: physical-psychological disorder (44.3% and 13.63%), relaxing feeling (9.75% and 10.1%), spirituality (12.94% and 9.51%), high-risk pregnancies (7.32% and 4.88%), and sexual satisfaction (10.23% and 4.3%).
Discussion
The article describes the development and evaluation of RHASLE, a tool specifically designed to assess reproductive health in women with lupus. The RHASLE consists of 27 items and 5 factors (Supplemental Table 5), including physical-psychological disorder, relaxing feeling, spirituality, high-risk pregnancy, and sexual satisfaction. The tool was found to be valid and reliable, with high internal consistency, stability, responsiveness, and interpretability. That was able to get approval of Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN) checklist. 25
The physical-psychological disorder factor, which consisted of 10 items, had the largest percentage of total variance and was the most important factor in explaining the concept of reproductive health in women with lupus. The relaxing feeling factor, which contained five items, was the second most important factor. The article concludes that the RHASLE is a valuable resource for healthcare professionals and researchers working in the field of lupus and reproductive health.
The article highlights that the third factor of the RHASLE, spirituality, was found to be the most important factor in explaining the concept of reproductive health in women with lupus, with the highest percentage of total variance (37.41).
The article explains that the fourth factor of the RHASLE, high-risk pregnancy, contained five items and accounted for 13.54% of the total variance. The inter-item correlation was good, with a Cronbach's alpha and MacDonald's omega of 0.65 and 0.7, respectively.
The fifth factor of the RHASLE, sexual satisfaction, consisted of four items and accounted for 10.38% of the total variance, and had a good inter-item correlation. The weight of the items within this factor ranged from 2.36 to 4.33.
The article discusses the development of RHASLE, a self-report tool designed to address the gap in addressing reproductive health beyond the physical aspects of lupus disease in clinics and hospitals. The scale included a rating system and unique item weights obtained through psychometric testing. This approach has not been utilized in other available scales in this field, and it highlights the importance of considering cultural, social, and religious backgrounds in assessing reproductive health in women with lupus.
The items and factors of RHASLE compared to the sexual quality of life-female (SQOL-F) which was validated by Maasoumi et al 26 (with four domains: 1. Psychosexual Feelings, 2. Sexual and Relationship Satisfaction, 3. Self-Worthlessness, and 4. Sexual Repression) in Iran. The PPD and some items of Rlx of RHASLE completely covered the items of one, three, and four domains of SQOL-F. The SxS factor items of RHASLE covered all items of second domain of SQOL-F. But RHASLE had the additional factors of high-risk pregnancy, spirituality, and some items of Rlx that can be achieved with exercise, walking, and family support. Thus, RHASLE more comprehensively covered all aspects of reproductive and sexual health of women with SLE.
The literature review on reproductive health scales for patients with lupus found a lack of disease-specific tools. Instead, general quality of life and self-reported questionnaires were used to assess overall health and sexual status in lupus patients, which may not be sensitive to the unique conditions and experiences of women with lupus. The Lupus Quality of Life (QoL) scale was identified as the best scale for patients with lupus. When comparing the Lupus QoL with RHASLE, it was found that the RHASLE addressed fertility problems unique to women with lupus and had a stronger emphasis on spirituality, which was found to be the biggest source of support for women with lupus in dealing with disease crises. The review also highlighted studies that did not follow established principles for scale development and used non-standardized scales. The RHASLE also had good internal consistency and was found to be acceptable for use in assessing reproductive health in women with lupus.
Strengths and limitations
One of the major limitations of the present study is the potential concern regarding the generalizability of the findings, as the samples were selected from Iranian populations. Therefore, the scale should be tested in other cultures to ensure its validity and reliability in different populations. Additionally, the scale developed in this study was a self-report type, which had inherent weaknesses and limitations.
Conclusion
The article highlights that this is the only scale development study that focuses on this women reproductive and sexual health. The scale can be used to measure and aim at reducing or controlling the complications of lupus as well as it can also be used to train medical, nursing, and midwifery students who are the primary caregivers of women's reproductive health.
Supplemental Material
Supplemental Material - Development and psychometric properties of the Reproductive Health Assessment in Systemic Lupus Erythematosus: Mixed-Methods study
Supplemental Material for Development and psychometric properties of the Reproductive Health Assessment in Systemic Lupus Erythematosus: Mixed-Methods study by Zahra Behboodi Moghadam, Armin Zareiyan, Seyedeh Tahereh Faezi, and Elham Rezaei in Lupus.
Footnotes
Acknowledgments
The authors would like to thanks Lupus Association, and the Rheumatology Center of Shariati hospital in Tehran, Clinical Research Development Unit, Talegani Hospital, Tabriz University of Medical Sciences, Tabriz, Iran for kind supports.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tehran University of Medical Sciences.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.