
Abstract
Background
Systemic lupus erythematosus (SLE) patients are prone to frequent emergency department (ED) visits. This study explores the epidemiology and outcomes of ED visits by patients with SLE utilizing the Nationwide Emergency Department Sample (NEDS).
Methods
Using NEDS (2019), SLE ED visits identified using ICD-10 codes (M32. xx) were compared with non-SLE ED visits in terms of demographic and clinical features and primary diagnoses associated with the ED visits. Factors associated with inpatient admission were analyzed using logistic regression. Variations in ED visits by age and race were assessed.
Results
We identified 414,139 (0.35%) ED visits for adults ≥ 18 years with SLE. ED visits with SLE comprised more women, Black patients, ages 31–50 years, Medicare as the primary payer, and had higher comorbidity burden. A greater proportion of Black and Hispanic SLE patients who visited the ED were in the youngest age category of 18–30 years (around 20%) compared to White patients (less than 10%). Non-White patients had higher Medicaid utilization (27%–32% vs 19% in White patients). Comorbidity patterns varied based on race, with more White patients having higher rates of hyperlipidemia and ischemic heart disease (IHD) and more Black patients having chronic kidney disease (CKD), hypertension, and heart failure. Categorizing by race, SLE/connective tissue disease (CTD) and infection were the most prevalent primary ED diagnosis in non-White and White patients, respectively. Age ≥ 65 years, male sex, and comorbidities were linked to a higher risk of admission. Black race (OR 0.86, p = .01) and lowest income quartile (OR 0.78, p = .003) had lower odds of inpatient admission.
Conclusion
Infection and SLE/CTD were among the top diagnoses associated with ED visits and inpatient admission. Despite comprising a significant proportion of SLE ED visits, Black patients had lower odds of admission. While the higher prevalence of older age groups, hyperlipidemia, and IHD among White patients may partly explain the disparate results, and further study is needed to understand the role of other factors including reliance on the ED for routine care compared among Black patients, differences in insurance coverage, and potential socioeconomic biases among healthcare providers.
Background
Autoimmune rheumatic diseases are chronic conditions that often lead to multi-organ involvement, often requiring emergency department (ED) utilization and inpatient care. Patients with systemic lupus erythematosus (SLE) may be particularly prone to ED visits due to a complex disease course, flares, complications from medication, and treatment non-adherence. Prior studies have demonstrated higher ED use among SLE patients with Medicaid coverage, higher disease activity, higher comorbidity burden, and treatment non-adherence.1–5 Similarly, higher SLE disease severity, chronic pain, depression or a preceding psychiatric diagnosis, and cardiovascular complications are associated with recurrent ED utilization.6,7 On the other hand, older age was associated with a lower risk of frequent ED use in SLE.2,6 Only a few studies worldwide have investigated the reasons for ED visits in SLE.4,8–10 These studies identified diverse infections as the most common diagnoses associated with ED visits, more so than active SLE-related manifestations or disease flares.8,9 Another study that examined SLE patients who repeatedly visited the ED identified pain as the main reason for these persistently frequent ED visits (defined as at least three times in a year for two out of 4 years of the study period). 10 A considerable portion of ED visits results in patients being treated and discharged from the ED, which is referred to as "treat-and-release" ED visits. This pattern of ED visits may suggest inadequate or inaccessible primary or preventative healthcare services within the community or lack of health insurance coverage. 11 Many of the studies that have studied the reasons, factors, and outcomes associated with ED use in SLE have been limited by the use of data from a single-institution and small sample sizes. Studies of SLE patients conducted in the recent years utilizing larger sample sizes may offer valuable insights into this area. Therefore, this study aims to explore the epidemiology and outcomes of ED visits in SLE utilizing the Nationwide Emergency Department Sample (NEDS), the largest all-payer ED database in the United States.
Patients and methods
Data source and patient selection
The U.S. NEDS database for year 2019 was used to identify patients ≥ 18 years who visited the ED. NEDS is the largest publicly available all-payer ED database in the United States and is a part of the Healthcare Cost and Utilization Project (HCUP). It contains discharge information from about 20% stratified sample of the hospital-owned EDs in the United States. Unweighted, NEDS-2019 contains data on 33.1 million ED visits across 989 sampled hospital-owned EDs in the United States, which approximates to 143 million ED visits after applying discharge weight provided by HCUP to calculate national estimates and represents about 83.9% of U.S. ED visits. The NEDS is constructed using the HCUP State Emergency Department Databases (SEDD) and the State Inpatient Databases (SID). The SEDD captures discharge information on ED visits that do not result in an admission and the SID contains discharge information on patients initially seen in the ED and then admitted to the same hospital. 12 This study was performed in concordance with the formal HCUP data use agreement and was exempt from requiring institutional review board approval as NEDs data is de-identified.
ED visits with diagnosis of SLE were identified using the presence of ≥ 1 of the International Classification of Disease (ICD)-10 codes M32.xx (M32.1x, M32.8, and M32.9, excluding the code M32.0 for drug-induced SLE). The ED visits with SLE were compared to ED visits for patients without any of the above diagnosis codes for SLE. At least one count of any SLE diagnosis code in the electronic health records (EHR) data has been reported to have positive predictive values (PPV) of approximately 71%–74%.13,14
Exploratory variables and outcomes
The variables studied included baseline demographic characteristics (age, sex, race/ethnicity, primary payer, and income), and clinical comorbidities (chronic kidney disease (CKD), overweight and obesity, hyperlipidemia (HLD), hypertension (HTN), diabetes mellitus (DM), ischemic heart disease (IHD), cerebrovascular disease (CVD), peripheral vascular disease (PVD), heart failure (HF), venous thromboembolic diseases (VTE), and mood disorders) (Supplementary Table S1). SLE visits were categorized by age (18–30, 31–50, 51–64, and ≥ 65 years) and race (White, Black, Hispanic, and other races). In HCUP, “the variable RACE contains a uniform coding for race and ethnicity. If the data source supplied information on race and ethnicity as separate data elements (RACE_X and HISPANIC_X, respectively), ethnicity takes precedence over race in setting the HCUP uniform values. For example, a patient who is Hispanic and Black is assigned to the category of Hispanic (RACE = 3 based on information included in HISPANIC_X).” 15 For income, the HCUP categorical variable ZIPINC_QRTL provides a quartile classification of the estimated median household income derived from ZIP Code-demographic data obtained from Claritas, and indicated by values 1 to 4, for poorest to wealthiest populations. Because these estimates are updated annually, the value ranges for the ZIPINC_QRTL categories vary by year. 16
The primary objective was to examine the demographic characteristics and clinical comorbidities linked to ED visits with SLE, compared to those without SLE. Additionally, we sought to explore other pertinent secondary outcomes, including characterization of ED visits with SLE by age and race/ethnicity, the top ten most frequently encountered primary diagnoses for both ED visits and inpatient admissions in SLE, as well as patient-related factors contributing to inpatient admission among SLE ED visits. The primary diagnoses were identified using the Clinical Classifications Software Refined (CCSR), which are developed by HCUP and aggregate multiple ICD-10 diagnosis codes into clinical meaningful categories. 17
Statistical analysis
The baseline demographic features and clinical comorbidities were compared between ED visits with without SLE. The top ten primary diagnoses were compared for the following groups: (a) ED visits with and without SLE and (b) SLE ED visits with and without inpatient admission from the ED. To study inpatient admission, the SLE ED visits were categorized into two groups: those admitted versus those released from the ED, after excluding SLE patients who died in the ED. A multivariable logistic regression model was used to calculate the odds ratio (OR) of association of different baseline demographic features and clinical comorbidities to inpatient admission in SLE ED visits.
Secondarily, we also examined how the demographic characteristics, clinical comorbidities, and main reasons for emergency department visits varied among SLE patients of different racial and ethnic groups.
U.S. national estimates from the representative sample discharges were calculated using the discharge weights (discwt) for the observations provided by the NEDS. Costs for inpatient stays were calculated using the HCUP Cost-to-Charge Ratios for Inpatient Files. Continuous variables were presented as mean [standard error of mean (SEM)] and categorical variables as counts and percentages. Pearson chi squared tests were used to compare categorical variables and t-tests to compare continuous variables among groups; a p-value of 0.05 was considered as statistically significant. Statistical software STATA v13 was used for analysis. 18
Results
Demographic and clinical characteristics
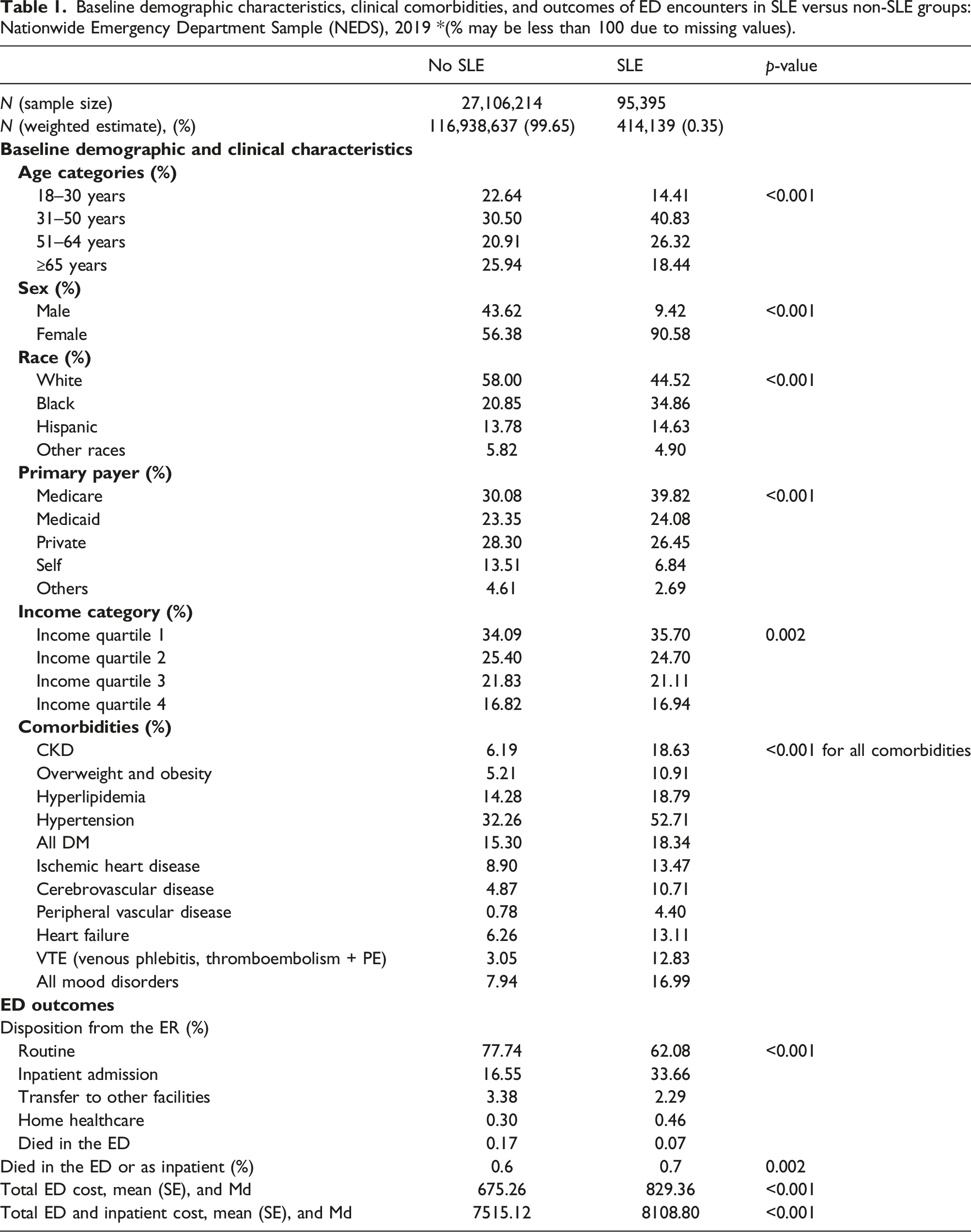
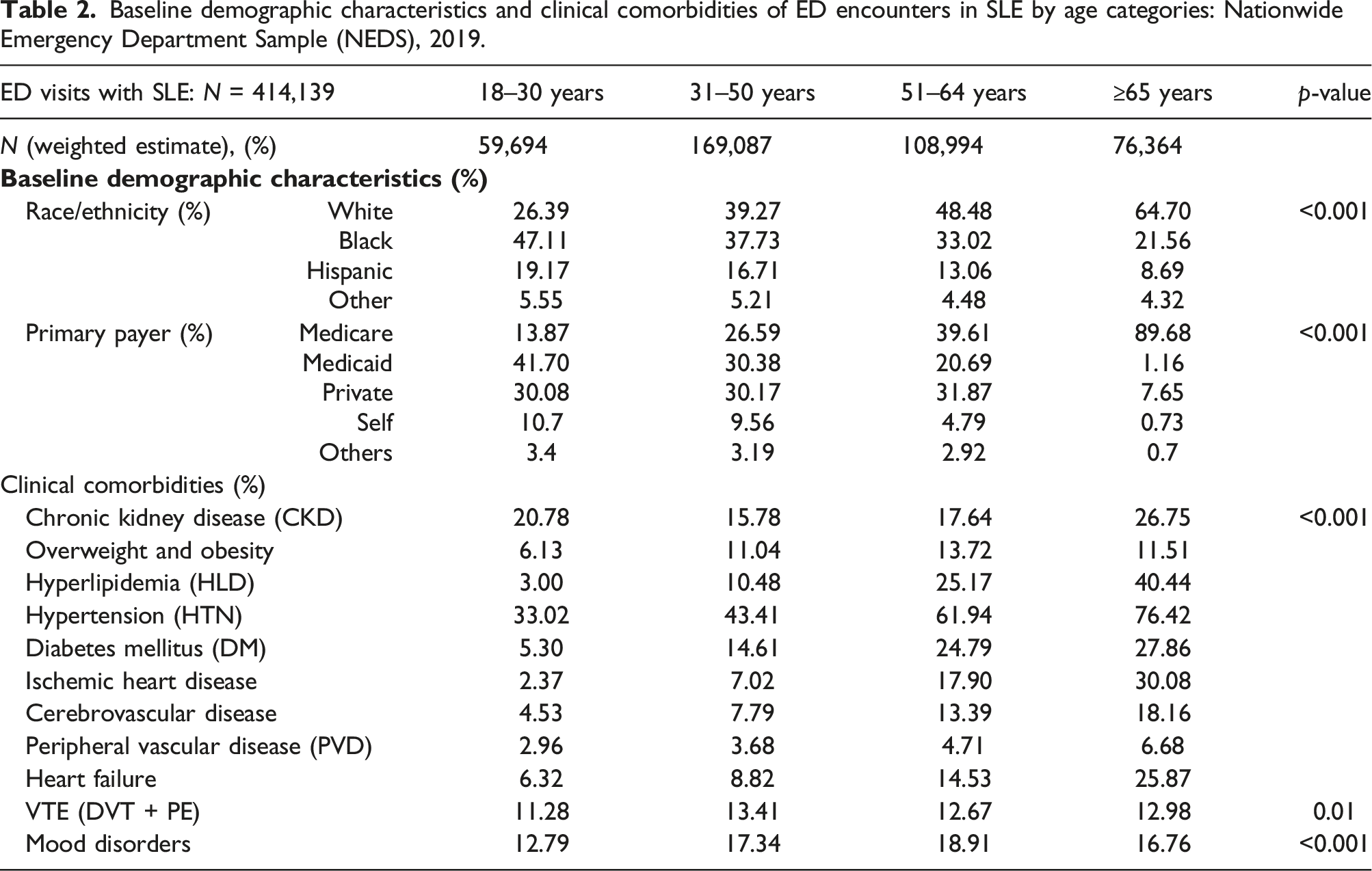
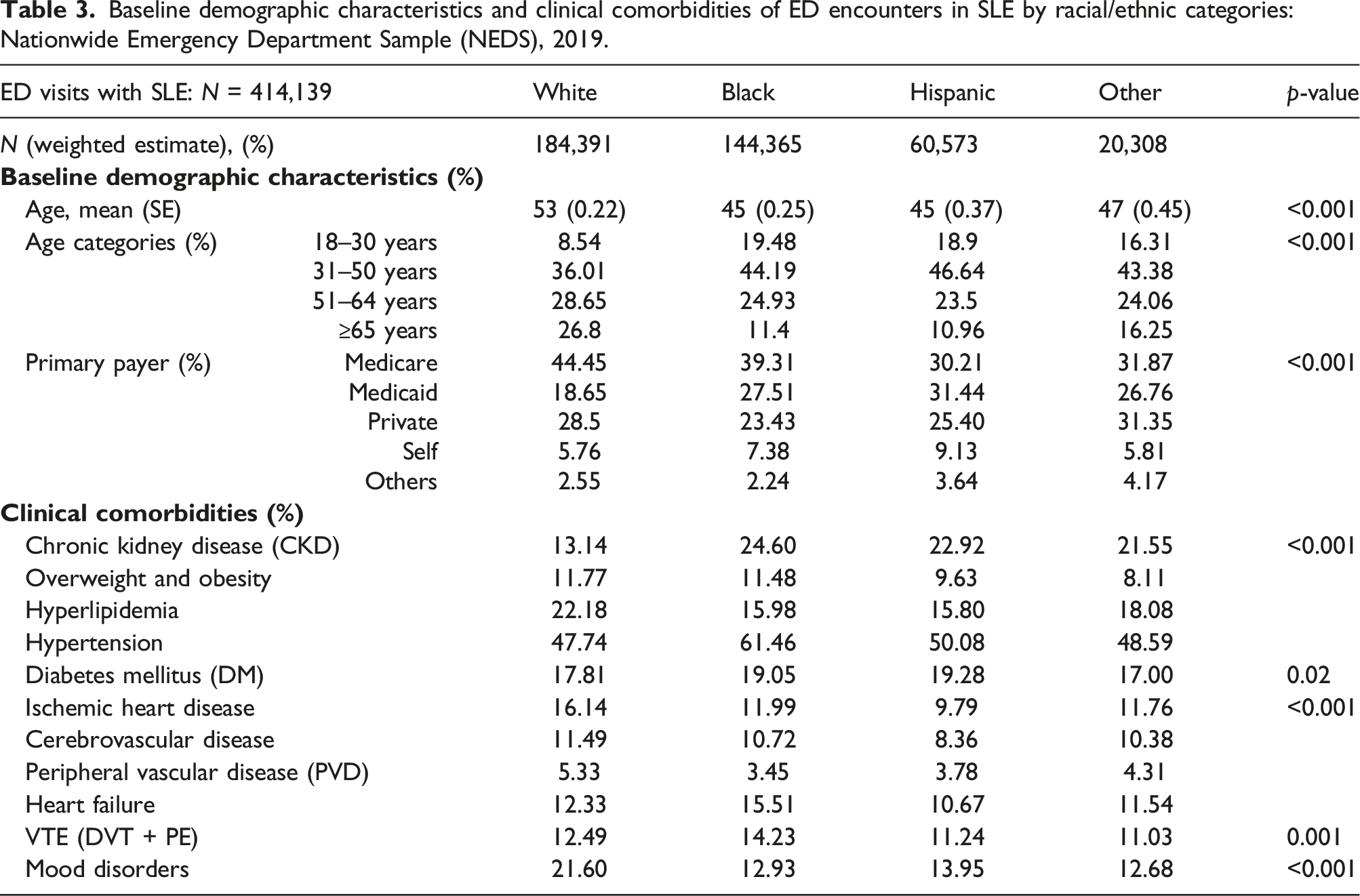
i. ED visits in individuals with and without SLE: Of 116,938,637 ED visits for adults ≥ 18 years in 2019, 414,139 (0.35%) had a diagnosis of SLE. ED visits with SLE as compared to those without SLE comprised of higher proportion of women (91% vs 56%), patients of Black race (35% vs 21%), patients aged 31–50 years old (41% versus 31%), and those with Medicare as the primary payer (40% vs 30%), p < .001. All the studied clinical comorbidities were significantly higher in SLE compared to non-SLE group. The most prevalent comorbidities in SLE ED visits were HTN (53%) and CKD (19%) (Table 1). PVD (6-fold), VTE (4-fold), and CKD (3-fold) were notably higher in ED visits with SLE compared to those without. Obesity, CVD, HF, and mood disorders were approximately twice as common in the SLE ED visits as compared to those without (Table 1). ii. SLE ED visits by age categories: About 50% of ED visits with SLE among the youngest adults aged 18–30 years comprised of patients of Black race, whereas majority (65%) of ED visits among older adults ≥ 65 years consisted of White patients. Public insurance was the primary payer across all age groups, with Medicaid primarily covering most visits for those aged 18–30 years (∼ 42%) and 31–50 years (∼30%). Older SLE adults ≥ 65 years had higher comorbidities, such as CKD, HLD, HTN, and DM, as well as cardiovascular diseases (IHD, CVD, PVD, and HF), but even the ED visits among youngest SLE adults aged 18–30 years exhibited a substantial comorbidity burden with approximately 21% having CKD, 33% with HTN, 11% with VTE, and 13% with mood disorders (Table 2). iii. SLE ED visits by race/ethnicity: In ED visits with SLE, non-White patients were on average younger (mean age 45 years for Black and Hispanic, and 47 for other race categories) compared to White patients (mean age 53 years). The highest proportion of ED visits for SLE occurred among patients aged 31–50 years across all racial/ethnic groups. However, a greater proportion of Black and Hispanic SLE patients who visited the ED were in the youngest age category of 18–30 years (around 20%) compared to White patients (less than 10%). Although Medicare was the predominant primary payer for SLE ED visits, Medicaid was more commonly used as the primary payer for SLE ED visits among non-White patients (27%–32%) compared to White patients (19%) (Supplementary Table S2). Comorbidities varied across racial categories, with White patients having higher rates of HLD (22% vs 16%–18%), IHD (16% versus 10%–12%), and mood disorders (22% versus 13%–14%) than non-White patients, while non-White patients had higher rates of CKD than White patients (22%–25% versus 13%). Hypertension (62%) was the most prevalent comorbidity among SLE ED visits in Black patients, which was higher than in other racial/ethnic groups. Similarly, heart failure as a comorbidity was higher among Black patients presenting to the ED (16%) compared to other racial categories (Table 3). Baseline demographic characteristics, clinical comorbidities, and outcomes of ED encounters in SLE versus non-SLE groups: Nationwide Emergency Department Sample (NEDS), 2019 *(% may be less than 100 due to missing values). Baseline demographic characteristics and clinical comorbidities of ED encounters in SLE by age categories: Nationwide Emergency Department Sample (NEDS), 2019. Baseline demographic characteristics and clinical comorbidities of ED encounters in SLE by racial/ethnic categories: Nationwide Emergency Department Sample (NEDS), 2019.
Top ten primary diagnoses
i. ED visits in individuals with and without SLE: Pain-related visits (non-specific chest pain, abdominal pain, and musculoskeletal pain) were among the top ten reasons for ED visits in both SLE and non-SLE groups. Other top diagnoses for SLE ED visits, identified as primary CCSR codes associated with these ED visits, were SLE/connective tissue disease (CTD) (6%) and infections such as sepsis (4%), urinary tract infection (UTI, 3%), pneumonia (2%), and skin and soft tissue infection (SSTI, 2%). The SLE/CTD diagnosis was identified using the CCSR code “MUS024,” which incorporates a broad range of diagnosis including SLE and other autoimmune rheumatic and connective tissue diseases, and likely represent ED visits related to increased symptoms of underlying SLE.
In contrast, injury, sprains/strains, and infections [UTI 3%, SSTI 2%, and upper respiratory tract infection (URTI) 2%] were other major diagnoses for ED visits in individuals without SLE (Supplementary Figure S1). ii. ED visits in individuals with SLE who were admitted versus discharged from the ED: For SLE ED visits who were admitted from the ED, the top primary diagnoses included infections [sepsis (11%), pneumonia (4%), UTI (2%), and SSTI (2%)], SLE/CTD (6%), and heart failure (3%). For SLE ED visits who were released from the ED, the top primary diagnoses included pain-related visits, SLE/CTD, injury, and infections such as UTI and SSTI (Supplementary Figure S2). iii. SLE ED visits by age categories: The most common primary diagnosis for ED visits of younger adults aged 18–30 years with SLE was SLE/CTD, whereas sepsis was the most frequent primary diagnosis for older adults aged ≥ 65 years. Pain-related, pregnancy-related, and infections such as sepsis, UTI, URTI, and SSTI were among the major ED diagnoses for younger age groups (18–30 and 31–50 years). Heart failure and arrhythmias, which were among the top 10 diagnoses for adults aged ≥ 65 years, were not present in the top 10 for younger age categories (Supplementary Figure S3). iv. SLE ED visits by race/ethnicity: Categorizing by race, the primary ED diagnosis of SLE/CTD was more common in Black (8.61%), Hispanic (6.70%), and other races (8.24%) than in White patients (2.99%). CKD was among the top 10 primary diagnosis in ED visits for Black (2.12%) and Hispanic (2.44%) SLE patients. Conversely, among White patients, top ten primary ED diagnoses exhibited higher rates of infection than in other groups [12.34% (sepsis 4.30%, UTI 3.43%, SSTI 2.51%, and pneumonia 2.10%)] compared to other groups [Black 5.77%, Hispanic 9.61%, and other races 7.72%] (Supplementary Figure S4).
Factors associated with inpatient admission among SLE ED visits
ED visits with SLE had double the rate of inpatient admission (34%, 139,416/414,139) compared to ED visits without SLE (17%). For ED visits with SLE, age ≥ 65 years (reference: 18–30 years; OR 1.52, 1.37–1.69, p < .001), male sex (reference: women, OR 1.30, 1.20–1.41, p < .001), and Hispanic and “other” race categories (reference: White, OR 1.19, 1.02–1.39, p = .03 and OR 1.42, 1.23–1.63, p < .001) had higher odds of inpatient admission from the ED. Conversely, Black race (reference: White, OR 0.86, 0.77–0.96, p = .01) and lowest income quartile (reference: highest income quartile, OR 0.78, 0.66–0.92, p = .003) were associated with lower odds of inpatient admission from the ED (Table 2).
Most of the comorbidities studied were associated with higher odds of inpatient admission in the adjusted analysis. The comorbidities with the highest odds for inpatient admission from the ED included CKD (OR 2.80, 2.59–3.02), overweight/obesity (OR 2.68, 2.41–2.99), PVD (OR 2.23, 1.97–2.52), and mood disorders (OR 1.98, 1.80–2.18), p < .001 (Figure 1). Multivariable analysis of baseline demographic characteristics and clinical comorbidities associated with inpatient admission after ED visit in patients with SLE: Nationwide Emergency Department Sample (NEDS), 2019 *OR adjusted for age, sex, race, primary payer, income quartile, and baseline clinical comorbidities).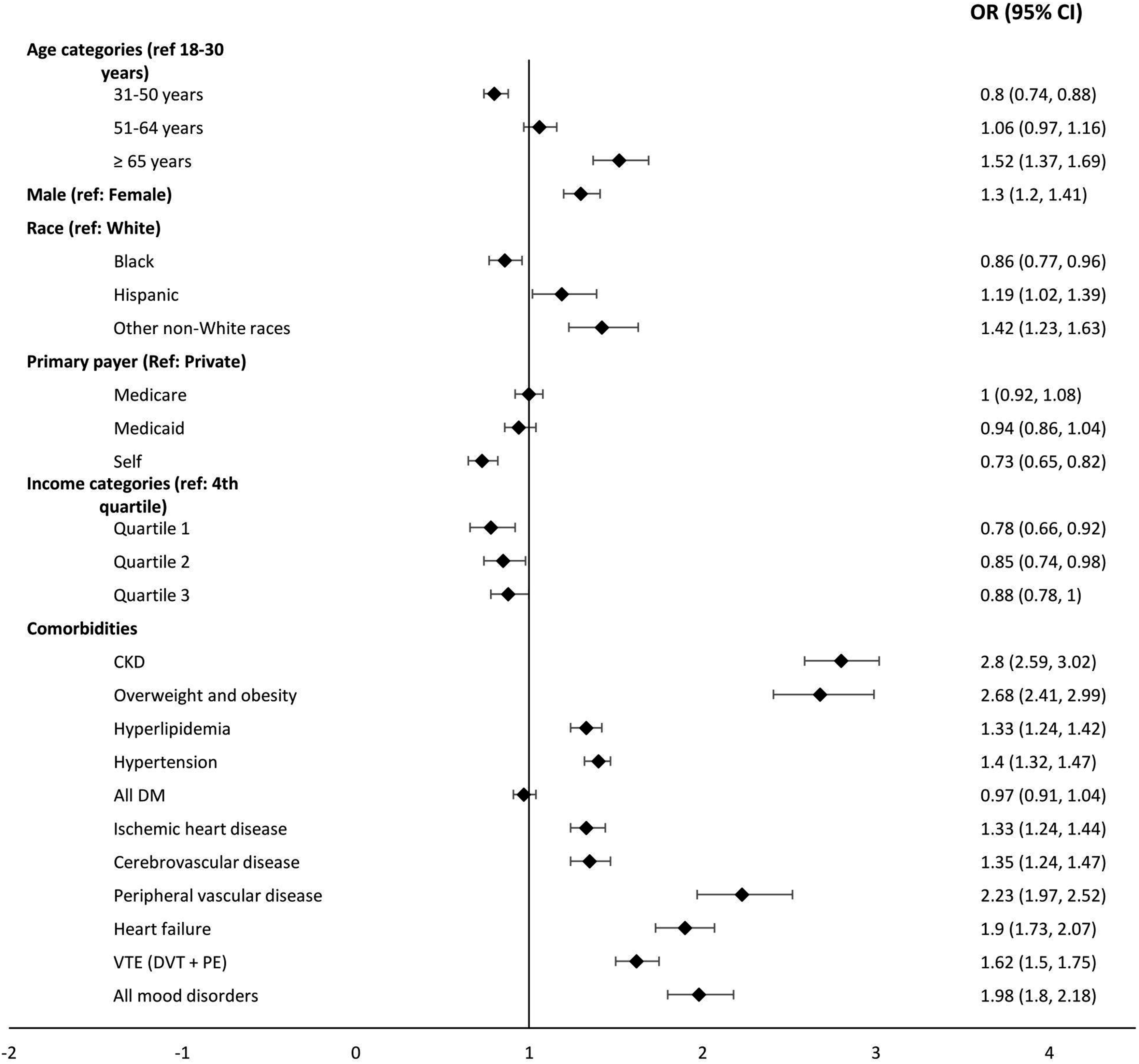
Discussion
In this work, we show that compared to non-SLE visits, ED visits with SLE had significantly higher proportions of women, Black patients, patients aged 31–50 years, and Medicare beneficiaries, as well as a higher comorbidity burden. Non-White patients with SLE who visited the ED were more likely to utilize Medicaid as the primary payer compared to White patients. Almost half of the SLE ED visits in 18–30 age group were of Black race/ethnicity and had Medicaid as the primary payer. Compared to SLE patients of other racial/ethnic groups, Black patients had the highest rates of CKD, HTN, and heart failure. Although pain-related visits were among the top ten primary diagnoses associated with ED visits in both SLE and non-SLE groups, other major diagnoses for ED visits associated with SLE were SLE/CTD and infections such as sepsis, UTI, pneumonia, and SSTI. The most common primary diagnosis for ED visits among the 18–30-year age group with SLE was SLE/CTD, while in older patients ≥ 65 years, sepsis was the most frequent primary diagnosis. SLE patients were twice as likely to require hospitalization compared to non-SLE patients following ED visits. For SLE-related ED visits that resulted in hospitalization, the top primary diagnoses included infections, SLE/CTD, and heart failure. The odds of inpatient admission were higher for those aged ≥ 65 years, male patients, patients belonging to Hispanic and “other” race categories, and those with comorbidities, while patients of Black race and lowest income quartile had lower odds of admission.
The SLE group's demographics in our study (aged 31–50 years, women, Black, and publicly funded insurance) represent the typical demographic of lupus patients.2,6,10 SLE patients had a substantially higher comorbidity burden compared to non-SLE ED visits, with double the rates of obesity, heart failure, CVD, and mood disorders and more than triple the rates of CKD, PVD, and VTE compared to non-SLE ED visits. Previous research has shown 3-fold greater likelihood of experiencing multimorbidity and substantial multimorbidity in SLE patients compared to the general population. 19 About 2/3rd of SLE ED visits had publicly funded insurance, likely related to a higher incidence of end-stage renal disease in this population. In our study, CKD had the strongest association with inpatient admission among comorbidities in SLE patients. This finding is consistent with previous reports indicating that SLE patients with renal involvement have higher rates of acute care utilization and incur greater medical costs.2,3,6,8,10 Other comorbidities in SLE including cardiovascular disease and psychiatric disorders have also been linked to increased utilization of acute care, such as ED visits and hospitalization.4,6,8,10 The higher inpatient admission among men and older adults ≥ 65 years with SLE are likely related to more severe disease manifestations in men 20 and a higher comorbidity burden in older patients, 4 as was also noted in our study.
A notable finding from our study is that Black patients and the patients belonging to the lowest income quartile who made up a significant portion of the SLE ED visits were significantly less likely to be admitted for inpatient care compared to White patients and patients of highest income quartile, respectively. This finding is intriguing and warrants further investigation to understand the underlying factors contributing to this disparity given that Black and low-income patients have been shown to have more severe SLE disease manifestations, damage accrual, and mortality in SLE.21–24 In our study, we found that ED visits by Black SLE patients were associated with a higher proportion of Medicaid coverage and significantly higher rates of CKD and HTN when compared to White patients. However, we also observed that several other comorbidities such as HLD, IHD, and mood disorders were more common in White patients with SLE visiting the ED than in Black patients.
Additionally, previous research has shown that low-income and Black patients are more likely to have frequent ED use and potentially preventable hospitalizations, particularly for pain-related complaints.10,25,26 Patients with SLE with frequently utilized the ED for pain were more also likely to be non-critically ill. 10 This results might suggest that these patients may be relying on the ED for more routine care needs due to lack of access to a primary care physician or an urgent care facility. However, it is possible that cognitive and socioeconomic biases on the part of healthcare providers play a role in these statistics, resulting in lower rates of inpatient admissions for Black patients as compared to White patients. Additionally, it is plausible that the ED physicians may not possess comprehensive knowledge of the overall impact and severity of SLE based on racial categories, resulting in varying decisions regarding hospital admission. While this has not been examined specifically in SLE ED visits, a study of the general population found that Black patients received lower triage scores, had a lower rate of inpatient admission from ED, and higher ED and in-hospital mortality as compared to White patients. Hispanic and Asian patients, on the other hand, had an equal or higher likelihood of being admitted. 27
Although the exact cause for ED visits could not be ascertained due to the inherent limitation of the database used, and the reasons for ED visits were assumed based on the primary discharge diagnoses associated with the ED visits, the major primary diagnoses for ED visits found in this study were similar to those previously reported in the literature.4,8–10 Infection was identified as one of the most common reasons for both ED visits and hospitalizations in lupus patients. Earlier research has also indicated that infections make up approximately 1/3rd of ED visits and are the leading causes of hospitalization and mortality in individuals with SLE.8,28 In our study, we found that only about 6% of the SLE ED visits had the primary diagnosis of SLE/CTD likely representing ED visits related to increased symptoms of underlying SLE, and this percentage was slightly higher among young adults aged 18–30 years (13.17%) compared to older SLE patients and among Black patients (8.61%) compared to White patients (2.99%). Previous studies have reported 8.9%–18.3% of ED visits being related to SLE disease activity or flares.8,9 However, the database's nature prevents conclusive determination of whether alternate primary diagnoses, like "heart failure" or "abdominal pain," were unrelated to SLE. A major advantage of NEDS-2019 is the large sample size and national representation of about 83.9% of U.S. ED visits. Additionally, it provides information on a wide range of sociodemographic data such as age, race/ethnicity, primary payer, median household income, and pertinent hospital characteristics, along with ED outcomes such as charge and dispositions, enabling the investigation of the epidemiology of ED visits. However, there are several limitations to our study. While there are validated algorithms for identifying SLE from the provided codes using EHR data, these codes have not been specifically validated for SLE diagnoses coded during ED visits. Additionally, since NEDS contains encounter-level and not individual patient-level data, patients who visited the ED multiple times in a year may contribute to more than one observation in the random sample. Consequently, the dataset cannot distinguish between frequent and infrequent ED visits. Furthermore, lack of information on outpatient/ambulatory data including duration of the disease and associated comorbidities, disease activity, or medication usage in relation to ED use restricts clinical interpretation. 12
From this study, it appears that SLE patients presenting to the ED are more likely to be women, younger in age, and Black, and have publicly funded insurance as well as a higher comorbidity burden than patients without SLE. Pain-related, SLE/CTD, and infections were the most common diagnoses for ED visits with SLE, while infections, SLE/CTD, and heart failure were the top primary diagnoses for SLE patients admitted from the ED. SLE ED visits were twice as likely to result in admission than non-SLE ED visits, and age ≥ 65 years, male sex, and comorbidities were linked to higher risk of admission. Managing comorbidities in the outpatient setting may help decrease the need for ED and inpatient care in SLE. Conversely, Black patients and those in the lowest income quartile were less likely to be admitted, despite accounting for a significant portion of ED visits associated with SLE. Discriminating determinants appear to be younger age, higher Medicaid use, CKD, HTN, and heart failure amongst Black SLE patients, and higher prevalence of older age groups, hyperlipidemia, and IHD among White patients, which may partly explain the disparate admission rates. Further research using different datasets is needed to confirm these findings, and to assess whether these discriminating factors are also observed in other studies. Additionally, a more comprehensive exploration into disparities in ED utilization and outcome patterns based on sociodemographic and disease-related attributes is essential to better understand the role of different factors including variation in disease activity and severity, reliance on the ED for routine care, disparities in insurance coverage, and potential socioeconomic biases among healthcare providers that could elucidate the disparities identified in this study. Such efforts will aim to facilitate implementation of effective to improve health equity and outcomes for all patients.
Supplemental Material
Epidemiology and outcomes of emergency department visits in systemic lupus erythematosus: Insights from the nationwide emergency department sample (NEDS)
Supplemental Material for Epidemiology and outcomes of emergency department visits in systemic lupus erythematosus: Insights from the nationwide emergency department sample (NEDS)
Footnotes
Author contributions
The primary author (RD) is funded by a research training grant from NIH/NIAMS (T32AR064194).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.